Complications in the Use of the Halo Fixation Device
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
R e p r i n t e d w i t h p e r m i s s i o n from The Journal of Bone and Joint Surgery, V o l u m e 6 8 - A , N o . 3,
March, 1986, pp. 3 2 0 - 3 2 5 .
Complications in the Use of the Halo
Fixation Device*
Steven R. Garfin, M.D.
Michael J . Botte, M.D.
Robert L. Waters, M.D.
Vernon L. Nickel, M.D.
S i n c e its i n t r o d u c t i o n in 1959 by P e r r y Although other authors have reported
1 5
a n d N i c k e l , the h a l o fixation d e v i c e h a s c o m p l i c a t i o n s in their p a t i e n t s , n o prior
b e c o m e the m o s t c o m m o n m e a n s u s e d to report h a s c o n c e n t r a t e d specifically on the
i m m o b i l i z e t h e u n s t a b l e cervical s p i n e . A l c o m p l i c a t i o n s that m a y b e a s s o c i a t e d w i t h
t h o u g h it w a s initially d e s i g n e d to be u s e d u s e o f the h a l o fixation d e v i c e . T h e pur
after s u r g e r y o n p a t i e n t s p a r a l y z e d b y p o p o s e o f this s t u d y is to e v a l u a t e the p r o b
liomyelitis, its c u r r e n t u s e is primarily r e l e m s that w e h a v e o b s e r v e d .
lated to spinal t r a u m a o r r e c o n s t r u c t i v e
p r o c e d u r e s o n the cervical s p i n e . T h e a d
v a n t a g e s i n c l u d e early m o b i l i z a t i o n o f t h e MATERIALS A N D
p a t i e n t a n d a v o i d a n c e of the c o m p l i c a t i o n s
a s s o c i a t e d w i t h p r o l o n g e d b e d rest, p s y METHODS
c h o l o g i c a l b e n e f i t s to the p a t i e n t in t e r m s T h e m e d i c a l r e c o r d s from the U n i v e r s i t y
of b e i n g a b l e to w a l k or m o r e fully partici of California at S a n D i e g o a n d affiliated
p a t e in the rehabilitation p r o g r a m , a n d a h o s p i t a l s a n d the R a n c h o L o s A m i g o s
s h o r t e r h o s p i t a l stay. C o m p a r e d with c o n M e d i c a l C e n t e r , D o w n e y , California, o f all
v e n t i o n a l o r t h o s e s , t h e h a l o v e s t or h a l o p a t i e n t s w i t h a d i a g n o s i s of fracture, dislo
b o d y j a c k e t offers m o r e rigid i m m o b i l i z a c a t i o n , or instability o f the cervical s p i n e
tion of t h e cervical s p i n e , the ability to that o c c u r r e d d u r i n g the p e r i o d from 1973
m o r e p r e c i s e l y p o s i t i o n the n e c k to obtain to 1983 w e r e r e v i e w e d . R e q u i r e m e n t s for
or m a i n t a i n cervical a l i g n m e n t , a n d less in i n c l u s i o n in t h e s t u d y i n c l u d e d : (1) a h i s
terference with mandibular motion and tory o f c o n t i n u o u s t r e a t m e n t with a halo
1 7 1 2 1 4 1 7
e a t i n g . , - , - H o w e v e r , t h e majority o f d e v i c e for a m i n i m u m of t w o w e e k s , (2)
t h e r e v i e w s in the literature c o n c e r n i n g the availability o f the hospital chart a n d radio
h a l o h a v e c o n c e n t r a t e d o n its e a s e o f a p g r a p h s , a n d (3) a m i n i m u m f o l l o w - u p o f
plication, the t o l e r a n c e o f t h e d e v i c e by the t h r e e m o n t h s after the h a l o w a s r e m o v e d .
patient, t h e d e g r e e o f i m m o b i l i z a t i o n o b E m p h a s i s w a s p l a c e d o n identifying s p e
t a i n e d , a n d its s u c c e s s in m a i n t a i n i n g r e cific c o m p l i c a t i o n s that resulted from the
d u c t i o n a n d a c h i e v i n g h e a l i n g after a frac p l a c e m e n t a n d u s e o f the h a l o d e v i c e .
3 6 1 0
ture or a r t h r o d e s i s . , - , 1 2 - 1 4 , 1 6 - 2 0 T h e s e i n c l u d e d infection at p i n sites,
l o o s e n i n g of pins, radiating pain o r n u m b
ness around pins, pain with mastication,
l o c a l i z e d d i s c o m f o r t a b o u t a pin, residual
scars left by p i n s , a n d p r e s s u r e s o r e s b e
n e a t h t h e v e s t or c a s t .
T h e c h a r t s o f 5 1 2 p a t i e n t s w e r e re
v i e w e d . D u e to lost c h a r t s or r a d i o g r a p h s ,
i n c o m p l e t e r e c o r d s , or p a t i e n t s m o v i n g or
b e i n g t r a n s f e r r e d to o t h e r facilities, o n l y
179 c h a r t s w e r e c o n s i d e r e d to h a v e a d e
q u a t e d o c u m e n t a t i o n to b e i n c l u d e d in t h e
study. E i g h t y - s e v e n of t h e s e p a t i e n t s w e r e
from t h e R a n c h o L o s A m i g o s M e d i c a l C e n
ter a n d 92 w e r e from t h e U n i v e r s i t y o f
California at S a n D i e g o M e d i c a l C e n t e r
a n d affiliated h o s p i t a l s . F i f t y - n i n e o f the
179 p a t i e n t s w e r e c o n t a c t e d b y t e l e p h o n e
a n d a s k e d to s u b j e c t i v e l y e v a l u a t e their
pin-site scars a n d to classify t h e m a s
e i t h e r m i n i m u m , m o d e r a t e , or s e v e r e . A
m i n i m u m scar w a s defined to the patient as
Table I.
b e i n g u n n o t i c e a b l e o r b a r e l y p e r c e p t i b l e by
*Fifty-nine patients evaluated.
close e x a m i n a t i o n . A m o d e r a t e s c a r w a s **One hundred and one patients evaluated.
d e f i n e d as n o t i c e a b l e , b u t s h a l l o w a n d n o t
disfiguring. A s e v e r e s c a r w a s c o n s i d e r e d
a s disfiguring, d e e p , a n d a s s o c i a t e d with RESULTS
p a t i e n t dissatisfaction. (Table I)
T h e s e 5 9 p a t i e n t s w e r e also q u e s t i o n e d
a s to w h e t h e r t h e y h a d h a d pain at the pin Pin-Loosening
sites w h i l e t h e h a l o w a s in p l a c e . T h e i r r e L o o s e n i n g w a s c o n s i d e r e d to b e p r e s e n t
plies w e r e p l a c e d in four c a t e g o r i e s : n o w h e n a pin c o u l d b e freely t w i s t e d b y the
d i s c o m f o r t ; m i n i m u m discomfort, w h i c h e x a m i n e r w i t h o u t r e s i s t a n c e , o r t h e tip of
w a s tolerable; m o d e r a t e discomfort, pain t h e p i n w a s visible at t h e e d g e of t h e skin,
ful at t i m e s ; a n d s e v e r e , p r o l o n g e d dis rather than being secured against the
comfort. skull. L o o s e n i n g o f o n e or m o r e p i n s o c
O n e h u n d r e d a n d forty-three p a t i e n t s c u r r e d in 6 4 p a t i e n t s ( 3 6 % ) . A total o f 716
were male and 36 were female. T h e pa p i n s (four p e r p a t i e n t ) h a d b e e n u s e d , of
tients' a g e s r a n g e d from 2 to 9 0 y e a r s , w i t h w h i c h 1 8 0 ( 2 5 % ) b e c a m e l o o s e . A l o o s e pin
a m e a n of 2 8 . 3 y e a r s . T h e l e n g t h of w a s t r e a t e d b y e i t h e r r e m o v i n g t h e pin a n d
f o l l o w - u p r a n g e d from t h r e e m o n t h s to ten p l a c i n g a n e w p i n into a n e w site (75 p i n s )
y e a r s after r e m o v a l o f t h e h a l o . T h e m o s t or t i g h t e n i n g t h e e x i s t i n g l o o s e pin in situ
c o m m o n c a u s e of cervical s p i n e i n j u r y w a s (105 p i n s ) . O f t h e 7 5 p i n s for w h i c h t h e site
a motor-vehicle accident ( 4 7 % ) , followed w a s c h a n g e d , 5 5 r e m a i n e d t i g h t , 13
in f r e q u e n c y b y a diving injury, fall, loosened again, and seven b e c a m e as
motorcycle accident, or other trauma. s o c i a t e d w i t h infection. O f t h e 1 0 5 p i n s
T w e l v e p a t i e n t s h a d a c o n g e n i t a l defect of that w e r e t i g h t e n e d in situ, 8 8 r e m a i n e d
t h e cervical s p i n e . tight, t e n r e l o o s e n e d , a n d s e v e n b e c a m e
Fifty-four p a t i e n t s ( 3 0 % ) h a d n o n e u r o a s s o c i a t e d w i t h infection.
logical i m p a i r m e n t , 53 ( 3 0 % ) h a d quadriparesis, a n d F 61o r (t h3 -4t %
h r)e w
e e rpee r cqeunatd r iof
p l etghiec . l o o s e p i n s
Eleven patients ( 6 % ) had an isolated w e r e d i a g n o s e d d u r i n g t h e first m o n t h
n e r v e - r o o t injury. after application a n d 4 2 % , d u r i n g the s e c
o n d . Fifty-three p e r c e n t o f the p i n s that
Figure 1.
Lateral
radiograph of the
skull of a
nineteen year old
man in whom
osteomyelitis
developed
(arrow) from a
halo pin-site
infection. A
craniotomy was
required to drain
the resulting
subdural abscess.
b e c a m e l o o s e w e r e l o c a t e d anteriorly. F o u r l o c a t i o n . T h i r t y - o n e o f t h e s e p i n sites
of t h e six p a t i e n t s in w h o m t h e h a l o b e s h o w e d n o further e v i d e n c e o f infection
c a m e completely dislodged gave a history after t h e c h a n g e , b u t t w o b e c a m e infected
of falling o r s u s t a i n i n g a direct b l o w to t h e a s e c o n d t i m e . N i n e of the t e n p i n - s i t e in
h a l o . In t h e o t h e r t w o , t h e d i s l o d g e m e n t fections that w e r e treated w i t h s y s t e m i c
w a s n o t e d w h e n t h e p a t i e n t a r o s e in t h e antibiotics, without c h a n g i n g the pin,
morning. healed. Eleven patients required removal
of t h e h a l o d e v i c e b e c a u s e of m u l t i p l e
p i n - s i t e i n f e c t i o n s . S e v e n of t h e s e i n f e c
t i o n s h e a l e d , b u t four h a d p e r s i s t e n t ,
Pin-Site Infection c h r o n i c d r a i n a g e from t h e p i n s i t e s . N i n e
Thirty-five p a t i e n t s ( 2 0 % ) h a d an infec t e e n p e r c e n t of t h e i n f e c t e d pin sites w e r e
tion at o n e or m o r e pin s i t e s . S i x t y - s e v e n d e t e c t e d d u r i n g t h e first m o n t h ; 4 4 % ,
p i n s ( 9 % ) w e r e i n v o l v e d . P i n - s i t e infection d u r i n g t h e s e c o n d m o n t h ; a n d 1 9 % , dur
w a s d i a g n o s e d b y e i t h e r a p o s i t i v e culture i n g t h e third m o n t h . Sixty p e r c e n t o f t h e
o r s u r r o u n d i n g cellulitis. T h e r e w e r e 2 6 infections were observed around the ante
superficial i n f e c t i o n s a n d ten d e e p infec rior p i n s . T h r e e o f t h e 3 5 p a t i e n t s in w h o m
tions. T h e deep infections included three a pin-site infection developed were treated
c a s e s of o s t e o m y e l i t i s ( o n e r e s u l t i n g in a with intravenous antibiotics, and eleven
s u b d u r a l a b s c e s s ) (Figure 1) a n d t w o c a s e s w e r e g i v e n oral a n t i b i o t i c s . S u r g i c a l d e
of septicemia. b r i d e m e n t w a s r e q u i r e d in t h r e e p a t i e n t s
T h e t r e a t m e n t of t h e infected pin sites with a pin-tract infection, including one
varied. Thirty-three pins were changed c r a n i o t o m y for d r a i n a g e of a s u b d u r a l ab
a n d a n e w pin w a s p l a c e d at a different scess.
Figure 2. Lateral radiograph of the skull of a seventy year old man, showing penetration of a halo pin
through the inner table of the skull.
Pin Penetration plaster cast or a p r e f a b r i c a t e d vest. Fifteen
s o r e s d e v e l o p e d u n d e r 8 3 c a s t s a n d five,
A halo pin penetrated through the inner
u n d e r 96 prefabricated vests. T h e sores
table of the skull in a 7 2 - y e a r - o l d m a n with
w e r e l o c a t e d o n t h e t r u n k , u s u a l l y in t h e
a type-II fracture of the odontoid process
r e g i o n o f t h e s c a p u l a or s t e r n u m . O f t h e 2 0
(Figure 2 ) . N i n e w e e k s after application of
patients, 11 w e r e completely quadriplegic,
t h e h a l o , t h e p a t i e n t fell o n t o t h e left side.
six w e r e i n c o m m p l e t e l y q u a d r i p l e g i c , t w o
H e felt m i n o r p a i n a r o u n d t h e a n t e r i o r left
w e r e n e u r o l o g i c a l l y intact, a n d o n e p a t i e n t
pin, a n d a r a d i o g r a p h s h o w e d that t h e pin
h a d a h e a d injury w i t h i m p a i r e d m e n t a l
h a d p e n e t r a t e d t h r o u g h t h e i n n e r table o f
status. Four patients had the halo r e m o v e d
t h e skull. W h e n t h e pin w a s r e m o v e d , a
to aid in t h e t r e a t m e n t o f the p r e s s u r e s o r e .
small a m o u n t o f c e r e b r o s p i n a l fluid w a s
O n e p a t i e n t r e q u i r e d d e b r i d e m e n t only,
noted. T h e patient w a s hospitalized and
o n e h a d a s p l i t - t h i c k n e s s skin graft, a n d
treated with antibiotics and elevation of
o n e h a d a transfer o f a local skin flap. All
t h e h e a d , a n d a n e w p i n w a s p l a c e d in a
subsequently healed.
different site. T h e original pin site h e a l e d
uneventfully, and no detectable neurologi
cal s e q u e l a e from the pin p e n e t r a t i o n w e r e Nerve Injury
noted. N o other patient had penetration of Injury to t h e supraorbital or s u p r a t r o
t h e pin t h r o u g h t h e i n n e r table. c h l e a r n e r v e o c c u r r e d in t h r e e p a t i e n t s .
T h e s e p a t i e n t s all h a d t h e a n t e r i o r p i n
Pressure Sores placed above the medial one-third of the
Twenty patients ( 1 1 % ) had the de eyebrow. The complication was mani
v e l o p m e n t of pressure sores under a halo fested b y s e v e r e pain a n d p a r e s t h e s i a s in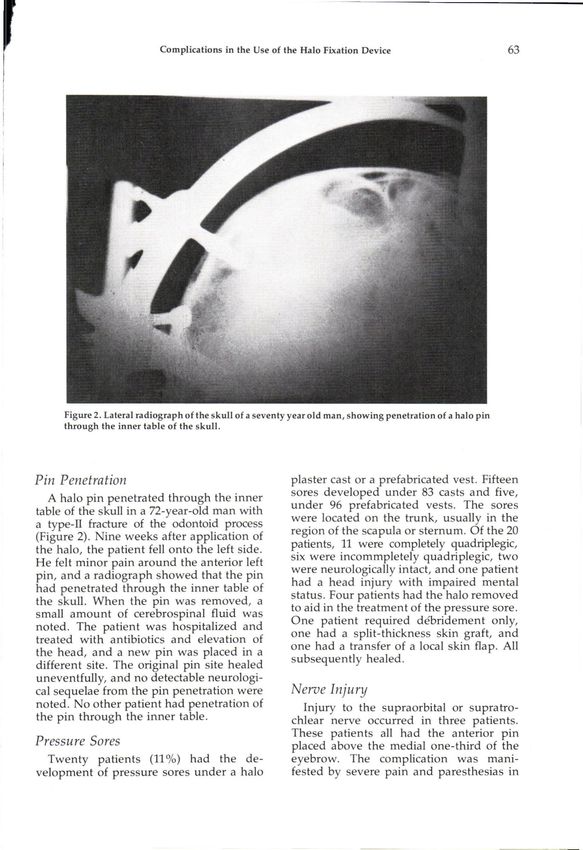
t h e r e g i o n o f t h e f o r e h e a d a n d scalp a b o v e pain had caused severe discomfort. T w e n
t h e a n t e r i o r h a l o pin. All of t h e s e p a t i e n t s ty-two patients ( 2 2 % ) reported moderate
o b t a i n e d relief after t h e p i n w a s r e m o v e d d i s c o m f o r t ; 23 ( 2 3 % ) , slight d i s c o m f o r t ;
a n d the a p p l i c a t i o n site w a s c h a n g e d to a a n d 3 8 ( 3 8 % ) r e p o r t e d n o pin d i s c o m f o r t .
slightly m o r e lateral p o s i t i o n . O n e p a t i e n t T w o p a t i e n t s c o m p l a i n e d o f pain at the
h a d p e r s i s t e n t p a r e s t h e s i a s for six w e e k s , a n t e r i o r pin sites w h i l e e a t i n g o r l a u g h i n g .
w h i c h t h e n gradually r e s o l v e d . In b o t h o f t h e s e p a t i e n t s t h e a n t e r i o r p i n s
w e r e l o c a t e d in t h e t e m p o r a l fossa, b e h i n d
Pin-Site Bleeding t h e t e m p o r a l h a i r l i n e . P l a c i n g n e w pins
m o r e anteriorly, o v e r t h e e y e b r o w s , a n d
T w o p a t i e n t s h a d s u s t a i n e d b l e e d i n g at
r e m o v i n g t h e e x i s t i n g p i n s led to i m m e d i
all four o f t h e p i n sites w h i l e r e c e i v i n g
ate relief of t h e s y m p t o m s .
h e p a r i n for the t r e a t m e n t o f t h r o m b o p h l e
bitis. In b o t h p a t i e n t s , t h e b l e e d i n g s u b
s i d e d after t h e h e p a r i n d o s a g e w a s d e
c r e a s e d . N o n e o f t h e s e pin sites b e c a m e
DISCUSSION
infected. W e h a v e identified s o m e o f t h e m a j o r
p r o b l e m a r e a s that are directly r e l a t e d to
Dysphagia t h e h a l o i m m o b i l i z a t i o n d e v i c e u s e d for
T h r e e p a t i e n t s r e q u i r e d r e a d j u s t m e n t of stabilization o f the cervical s p i n e . T h e
t h e p o s i t i o n o f t h e h e a d in the h a l o b e largest percentage of complications were
c a u s e o f d y s p h a g i a . In all t h r e e , t h e cervi r e l a t e d to l o o s e n i n g a n d infection. At Rancho
cal s p i n e initially w a s i m m o b i l i z e d in h y - routinely been tightened rather than
p e r e x t e n s i o n . R e p o s i t i o n i n g o f the n e c k to changed. N o obvious negative conse
less e x t e n s i o n w a s p e r f o r m e d w i t h o u t l o s s q u e n c e s h a v e b e e n o b s e r v e d from t h i s
of r e d u c t i o n of t h e cervical s p i n e fracture- p r a c t i c e . W e h a v e n o t e d , in the laboratory,
d i s l o c a t i o n for w h i c h t h e h a l o h a d b e e n that in c a d a v e r skulls that h a v e h a d halo
a p p l i e d a n d r e s u l t e d in i m m e d i a t e i m p i n s a p p l i e d e x p e r i m e n t a l l y at t h e r e c o m
p r o v e m e n t in t h e a b i l i t y t o e a t a n d mended six-inch-pound (0.69-newton-me-
swallow. ter) a p p l i c a t i o n t o r q u e t h e o u t e r c o r t e x o f
t h e skull is o n l y partially p e n e t r a t e d b y t h e
Pin Scars h a l o p i n s . T h e r e is a solid m a r g i n o f corti
cal b o n e to allow safe r e t i g h t e n i n g . W e
Fifty-nine patients were contacted by h a v e c o n c l u d e d , t h e r e f o r e , that it is safe to
t e l e p h o n e a n d a s k e d to c o m m e n t o n t h e t i g h t e n l o o s e n e d p i n s , a s s u m i n g that s o m e
appearance of the pin scars. Five patients r e s i s t a n c e is m e t d u r i n g that p r o c e d u r e .
s t a t e d that t h e y h a d o b t r u s i v e , s e v e r e scars S i n c e l o o s e n i n g is often a f o r e r u n n e r o f in
a n d w e r e dissatisfied w i t h t h e a p p e a r a n c e . fection, its e l i m i n a t i o n o r early c o r r e c t i o n
S e v e n t e e n p a t i e n t s felt that t h e y h a d m o d is b e n e f i c i a l in t h e p r e v e n t i o n of p i n - t r a c t
e r a t e , n o t i c e a b l e s c a r s , b u t that t h e y c o u l d i n f e c t i o n s a n d their s e q u e l a e . If n o r e s i s
tolerate t h e m . T h i r t y - s e v e n p a t i e n t s r e t a n c e is n o t e d after a few t u r n s of t h e pin,
p o r t e d m i n i m u m or n o scars a n d h a d n o t h e p i n s h o u l d be r e m o v e d , a n d a n e w o n e
c o m p l a i n t s . O n e p a t i e n t , a 2 1 y e a r old s h o u l d b e p l a c e d in a different site.
black w o m a n , had the d e v e l o p m e n t o f
k e l o i d s at b o t h a n t e r i o r p i n sites; the k e
If infection at a pin site d o e s d e v e l o p , it
loids w e r e treated s u c c e s s f u l l y b y surgical
s e e m s p r u d e n t to a d m i n i s t e r s y s t e m i c anti
revision.
biotics a n d initiate early local w o u n d c a r e . If
d r a i n a g e , cellulitis, or o t h e r s i g n s o f i n f e c
Pin Discomfort tion d o n o t i m p r o v e , t h e site of the pin
E v a l u a t i o n o f pin d i s c o m f o r t w h i l e in t h e s h o u l d be c h a n g e d a n d m o r e a g g r e s s i v e
halo was m a d e either by telephone contact local, a n d p e r h a p s p a r e n t e r a l , anti-biotic
(59 p a t i e n t s ) o r from s t a t e m e n t s i n c l u d e d t r e a t m e n t s h o u l d b e i n s t i t u t e d . Certainly,
in t h e m e d i c a l r e c o r d s (42 p a t i e n t s ) . S e v e n t h e p r e v e n t i o n o f infection w o u l d be pref
t e e n ( 1 7 % ) o f t h e p a t i e n t s s t a t e d that t h e e r a b l e , a n d p i n - s i t e - c a r e t e c h n i q u e s , in-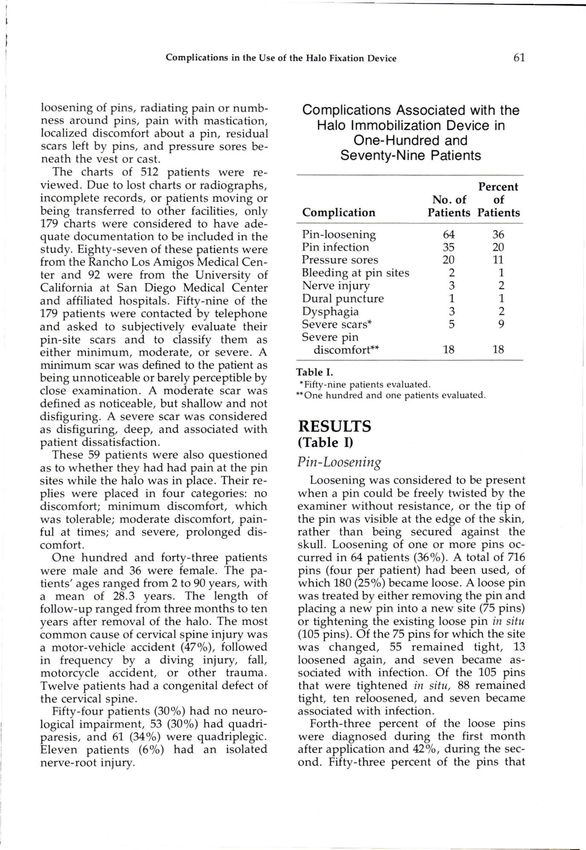
c l u d i n g c l e a n i n g t h e pin sites w i t h B e t a - c o r d injury s h o u l d b e c o n s i d e r e d w h e n
dine (providone-iodine) or hydrogen pe p o s s i b l e . A l t h o u g h t h i s m a y lead to an e n
r o x i d e e v e r y o t h e r day, s h o u l d be per tirely different set o f c o m p l i c a t i o n s , p r e s
f o r m e d in t h e hospital a n d t a u g h t to t h e s u r e s o r e s in p a t i e n t s w i t h a spinal c o r d
p a t i e n t b e f o r e d i s c h a r g e from the h o s p i t a l . injury can b e d e v a s t a t i n g . T h e r e f o r e , if
M o r e frequent c l e a n s i n g is n o t desirable p o s s i b l e , w e n o w r e c o m m e n d early i n t e r
a n d m a y l e a d to a l o w - g r a d e infection nal fixation a n d fusion of t h e cervical
c a u s e d b y c o n s t a n t m a n i p u l a t i o n o f the s p i n e , p a r t i c u l a r l y in e l d e r l y p a t i e n t s ,
w o u n d site. W e d o n o t k n o w w h y the an q u a d r i p l e g i c s , a n d q u a d r i p a r e t i c s , to eli
terior p i n s are m o r e apt to b e c o m e infected. m i n a t e the n e e d for the h a l o a n d r e p l a c e
T h e literature on t h e u s e of the h a l o d e it w i t h a m o r e l i m i t e d i m m o b i l i z a t i o n d e
vice h a s p a i d little a t t e n t i o n to t h e p r o b vice w h i c h hopefully can b e c o n f i n e d to
l e m s o f l o o s e n i n g or infection of t h e h a l o pressure-sensitive areas.
pins, although these complications have P r o l o n g e d b l e e d i n g at pin sites o c c u r r e d
3 8 9 1 4
been described. , , , F o u r o f the e l e v e n in t w o p a t i e n t s w h o h a d b e e n r e c e i v i n g
p a t i e n t s w i t h a n injury o f t h e cervical s p i n e h e p a r i n for t h r o m b o p h l e b i t i s . N e i t h e r o f
w h o s e c a s e s w e r e r e p o r t e d by T h o m p s o n t h e s e p a t i e n t s r e s p o n d e d to p a c k i n g or
h a d l o o s e n i n g o f t h e p i n s , a n d o n e h a d an d r e s s i n g o f t h e p i n sites, b u t t h e b l e e d i n g
infection. N i c k e l , et al. r e p o r t e d o n 2 0 4 pa c e a s e d after a d e c r e a s e in t h e d o s a g e o f
t i e n t s w h o h a d b e e n treated w i t h t h e h a l o h e p a r i n . T h i s possibility m u s t b e c o n s i d
1 2
d e v i c e . All o f the p a t i e n t s w h o h a d b e e n e r e d in t h o s e p a t i e n t s w h o requireanticoagula
in a h a l o for m o r e t h a n t w o m o n t h s h a d vice.
l o o s e n i n g of s o m e of the p i n s . M o s t pa
t i e n t s r e q u i r e d at l e a s t o n e c h a n g e in pin T h r e e p a t i e n t s in t h i s series s u s t a i n e d an
site. M a n y p a t i e n t s also h a d i n f l a m m a t i o n a p p a r e n t c o m p r e s s i o n o f t h e supraorbital
or infection in at l e a s t o n e pin site that r e 9
or s u p r a t r o c h l e a r n e r v e . T h e s e n e r v e s exit
q u i r e d a c h a n g e in t h e site. In t w o p a t i e n t s o v e r the m e d i a l o n e - t h i r d o f t h e orbit, a n d
the halo dislodged, and three patients had i n v o l v e m e n t o c c u r s b e c a u s e of too m e d i a l
o s t e o m y e l i t i s o f t h e skull. O t h e r a u t h o r s a p l a c e m e n t of the a n t e r i o r p i n s . If the a n
1 3 8
h a v e listed t h e s a m e c o m p l i c a t i o n s . , , 5 , , terior p i n s are p l a c e d o v e r t h e m i d d l e por
9, 12, 16, 17, 21 T h e s e f i n d i n g s , a l t h o u g h inci tion of t h e orbit, or slightly lateral, this
d e n t a l to t h e m a j o r e m p h a s i s of t h e s e complication should not occur.
o t h e r r e p o r t s , are c o n s i s t e n t w i t h o u r s . N i n e percent of the patients in this series
P r e s s u r e s o r e s u n d e r t h e h a l o cast o r w e r e m a r k e d l y dissatisfied w i t h the s c a r s .
v e s t h a v e also b e e n r e p o r t e d p r e v i o u s In g e n e r a l , m o s t of t h e p a t i e n t s felt that t h e
9 1 7 , 2 1
ly.1, , In o u r s e r i e s , 1 1 % of t h e p a t i e n t s scars were acceptable or were a necessary
h a d p r e s s u r e s o r e s . T h e majority o f p a o u t c o m e of t h e t r e a t m e n t o f t h e s p i n e in
t i e n t s w i t h this p r o b l e m w e r e q u a d r i p l e jury. T h e o l d e r p a t i e n t s a n d t h e m o r e s e
gics w h o l a c k e d s e n s a t i o n in t h e area o f v e r e l y i n j u r e d p a t i e n t s w e r e less likely to
the skin breakdown. This problem decreased express concern about the presence of re
m a r k e d l y in o u r p a t i e n t s as a w a r e n e s s o f sidual h a l o - p i n scars. In t h e majority o f p a
t h i s c o m p l i c a t i o n h e i g h t e n e d , a n d early tients t h e r e w a s o n l y a small residual
p r o p h y l a c t i c m e d i c a l a n d n u r s i n g care w a s dimple.
initiated. O n l y five p a t i e n t s h a d p r e s s u r e S o m e authors have reported no compli
s o r e s in t h e last four y e a r s o f this r e v i e w . A cations with the use of the halo d e v i c e . 4
h a l o c a s t is n o w u s e d less frequently, a H o w e v e r , w e h a v e f o u n d t h e overall c o m
p r e f a b r i c a t e d or m o l d e d v e s t b e i n g p r e plication rate to b e relatively h i g h . L o o s
ferred. T h e s e a l l o w e a s i e r i n s p e c t i o n o f t h e e n i n g a n d i n f e c t i o n are particularly c o m
skin, p e r h a p s m o r e u n i f o r m p r e s s u r e dis m o n a n d i m p l y that further b a s i c r e s e a r c h
tribution, a n d b e t t e r p a d d i n g . B e c a u s e o f in h a l o - p i n d e s i g n a n d a p p l i c a t i o n is
t h e p r o b l e m of p r e s s u r e s o r e s a n d their ef n e e d e d . T o d a t e , o n l y c h a n g e s in the suprastructure o
fect o n rehabilitation a n d h e a l t h , early sur s i n c e its first d e s c r i p t i o n b y P e r r y a n d
gical stabilization of p a t i e n t s w i t h a spinal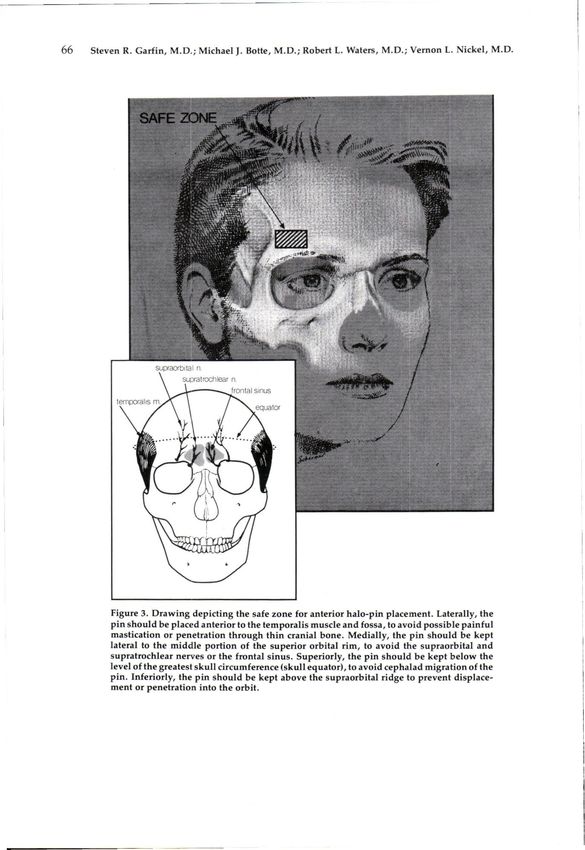
Figure 3. Drawing depicting the safe zone for anterior halo-pin placement. Laterally, the pin should be placed anterior to the temporalis muscle and fossa, to avoid possible painful mastication or penetration through thin cranial bone. Medially, the pin should be kept lateral to the middle portion of the superior orbital rim, to avoid the supraorbital and supratrochlear nerves or the frontal sinus. Superiorly, the pin should be kept below the level of the greatest skull circumference (skull equator), to avoid cephalad migration of the pin. Inferiorly, the pin should be kept above the supraorbital ridge to prevent displace ment or penetration into the orbit.
1 5
N i c k e l in 1 9 5 9 . T h e high-profile d e s i g n Care and awareness should be exercised
h a s b e e n m o d i f i e d to l o w e r t h e u p r i g h t s , in a p p l y i n g a h a l o j a c k e t or cast in t h e
in s o m e c a s e s four u p r i g h t s or aninterdigitating q u a d r i p l e g i c r ap tact hi eent t s y to
s t e mavoid
h a v e r eppr el as cs u
e dr e t h e
t w o high-fixation p a r t s , a n d m a t e r i a l s s o r e s . A l t h o u g h the h a l o is a v e r y useful
h a v e b e e n altered. H o w e v e r , t h e b a s i c i m m o b i l i z i n g d e v i c e to a p p l y initially to
r i n g - a n d - p i n d e s i g n , a s well as t h e r e c t h e p a t i e n t w i t h a spinal c o r d injury, c o n
o m m e n d a t i o n s for application, h a v e n o t sideration s h o u l d b e g i v e n to early surgical
b e e n a l t e r e d . T h e s e c o n c e p t s , also, h a v e stabilization w i t h internal fixation, t h u s
n e v e r b e e n r i g o r o u s l y scientifically tested a v o i d i n g t h e risk o f p r e s s u r e s o r e s u n d e r
1 1
or c h a l l e n g e d . O u r r e v i e w is t h e initial t h e vest or cast.
s t e p in a n e v a l u a t i o n o f t h e h a l o , a n d it B y following t h e s e r e c o m m e n d a t i o n s ,
d o e s d e l i n e a t e a r e a s in n e e d of further in w e t h i n k that t h e risks o f e m p l o y i n g t h e
v e s t i g a t i o n . W e w o u l d like to e m p h a s i z e , h a l o cervical i m m o b i l i z e r m a y b e m i n i
h o w e v e r , that n o p e r m a n e n t s e r i o u s s e m i z e d , a l t h o u g h n o t c o m p l e t e l y elimi
q u e l a e from t h e s e c o m p l i c a t i o n s o c c u r r e d nated.
despite the documentation of problem
areas.
* No benefits in any form have been received or will
be received from a commercial party related directly
Based on our experience, we recom or indirectly to the subject of this article. Funds were
m e n d that t h e following strict g u i d e l i n e s received in total or partial support of the research or
b e f o l l o w e d w h e n a p p l y i n g a n d treating clinical study presented in this article. The funding
sources were University of California at San Diego
a d u l t p a t i e n t s in a h a l o o r t h o s i s . T h e initial
Academic Senate Grant RH70-M and the Orthope
a p p l i c a t i o n t o r q u e in placing t h e p i n s in dic Research and Education Fund.
a d u l t s s h o u l d b e at least six to eight i n c h -
p o u n d s ( 0 . 6 9 to 1.12 n e w t o n - m e t e r s ) . W e REFERENCES
r o u t i n e l y t i g h t e n the p i n s 2 4 to 48 h o u r s ]
Cooper, P.R., K.R. Maravilla, F.H. Sklar,
after t h e h a l o is first a p p l i e d . Local pin care
S.F. Moody, and W.K. Clark, "Halo Immobili
s h o u l d b e s t a n d a r d i z e d , b u t n o t o v e r l y ag
zation of Cervical Spine Fractures, Indications
g r e s s i v e or d i s r u p t i v e to the pin site. If a and Results," J. Neurosurg., 50, 1979. pp. 6 0 3 -
pin is n o t e d to b e l o o s e , an a t t e m p t at r e - 610.
tightening to the original application 2
Garfin, S.R., M.J. Botte, R . S . Centeno, and
torque should be performed, assuming V.L. Nickel, "Osteology of the Skull as it Af
that r e s i s t a n c e is m e t d u r i n g this p r o c e fects Halo Pin Placement," Spine, 10, 1985, pp.
d u r e . T h e p i n site s h o u l d b e c h a n g e d a n d a 696-698.
3
n e w p i n s h o u l d b e u s e d if o s s e o u s e n Garrett, A.L., Jacquelin Perry, and V.L.
g a g e m e n t d o e s n o t o c c u r after a few c o m Nickel, "Stabilization of the Collapsing Spine,"
J. Bone and Joint Surg., 43-A, June, 1961, pp.
plete t u r n s . If infection or d r a i n a g e is s e e n ,
474-484.
c u l t u r e s s h o u l d b e g r o w n a n d t h e anti
4Houtkin, Sol, and D.B. Levine, "The Halo
biotic s e n s i t i v i t y o f t h e o r g a n i s m s h o u l d b e Yoke, A Simplified Device for Attachment of
d e t e r m i n e d . If t h e p a t i e n t ' s r e s p o n s e to the Halo to a Body Cast," J. Bone and Joint Surg.,
t h e a n t i b i o t i c s is n o t rapid, a c h a n g e in t h e 54-A, June, 1972, pp. 8 8 1 - 8 8 3 .
p i n site s h o u l d b e c o n s i d e r e d . A n t e r i o r 5
Kalamchi, Ali, A.C.M.C. Yau, J.P. O'Brien,
p i n s s h o u l d b e p l a c e d s u p e r i o r to t h e m i d and A.R. Hodgson, "Halo-Pelvic Distraction
dle or lateral o n e - t h i r d of t h e orbit, b e l o w Apparatus, An Analysis of One Hundred and
t h e g r e a t e s t c i r c u m f e r e n c e of t h e c r a n i u m , Fifty Consecutive Patients," J. Bone and Joint
to m i n i m i z e t h e risk o f l o o s e n i n g ,dislodgment, Surg., 58-A, December,
a n d n e 1976,
r v e dpp. a m a1119-1125.
ge. Also, the
6
pin s h o u l d n o t b e p l a c e d o v e r t h e t e m p o r a l Kleinfeld, F., "Zur Behandlung von Fraktu-
ren der Halswirbelsaule mit dem Halo-Fixa-
fossa or in t h e t e m p o r a l i s m u s c l e . T h e c r a
teur-externe," Unfallheilkunde, 84, 1981, pp.
nial c o r t e x is thin in that area, a n d pentration of the temporalis muscle may cause
2
161-167.
pain d u r i n g m a s t i c a t i o n (Figure 3 ) . 7
Koch, R.A., and V.L. Nickel, "The Halo
Vest, An Evaluation of Motion and Forces
across the Neck," Spine, 3, 1978, pp. 103-107.
8
Kopits, S.E., and M.H. Steingass, "Experi 16
Pieron, A.P., and W.R. Welply, "Halo Trac
ence with the 'Halo Cast' in Small Children," tion," J. Bone and Joint Surg., 52-B(l), 1970, pp.
Surg. Clin. North America, 50, 1970, pp. 9 3 5 - 9 4 3 . 119-123.
9
Kostuik, J.P., "Indications for the Use of the 17
Prolo, D.J., J . B . Runnels, and R.M. Jame
Halo Immobilization," Clin. Orthop., 154, 1981, son, "The Injured Cervical Spine, Immediate
pp. 4 6 - 5 0 . and Lont-Term Immobilization with the Halo,"
10Muller, I., O Varmuzkova, O. Vlach, and P. J. Am. Med. Assn., 224, 1973, pp. 591-594.
Messner, "Halo, Another Method of Treatment 18
S n e d d e n , M.H. and Frank Giammattei,
and Care for Cervical Spine Injuries," Acta. "Pitfalls in Halo Application and Manage
Chir. Orthop. Traumat., Cechoslovaka, 46, 1979, ment," Scientific Exhibit at the Annual Meeting
pp. 161-166. of The American Academy of Orthopaedic Sur
11
Nickel, V.L., Personal communication. geons, Anaheim, California, March 1 0 - 1 5 ,
12
Nickel, V.L., Jacquelin Perry, Alice Garrett, 1983.
and Malcolm Heppenstall, "The Halo, A Spinal 19Thompson, Harral, "Halo Traction Ap
Skeletal Traction Fixation Device," J. Bone and paratus, A Method of External Splinting of the
Joint Surg., 50-A, October, 1968, pp. 1400-1409. Cervical Spine after Surgery," J. Bone and Joint
13Nickel, V.L., Jacquelin Perry, A.L. Garrett, Surg., 44-B(3), 1962, pp. 6 5 5 - 6 6 1 .
and R. Snelson, "Application of the Halo," 20
W h i t e , R., "Halo Traction Apparatus," In
Orthop. and Prosthet. Appliance J., 14, 1960, pp. Proceedings of the Australian Orthopaedic As-
31-35. socation, J. Bone and Joint Surg., 48-B(3), 1966,
14
Perry, Jacquelin, "The Halo, in Spinal Ab p. 592.
normalities, Practical Factors and Avoidance of 21
Zwerling, M.T., and R.S. Riggins, "Use of
Complications," Orthop. Clin. North America, 3, the Halo Apparatus in Acute Injuries of the
1972, pp. 69 - 8 0 . Cervical Spine," Surg. Gynec. and Obstet., 138,
15
Perry, Jacquelin, and V.L. Nickel, "Total 1974, pp. 189-193.
Cervical-Spine Fusion for Neck Paralysis," J.
Bone and Joint Surg., 41-A, January, 1959, pp.
37-59.You can also read

















































