Enhancement of Nab-Paclitaxel Antitumor Activity through Addition of Multitargeting Antiangiogenic Agents in Experimental Pancreatic Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Molecular
Cancer
Small Molecule Therapeutics Therapeutics
Enhancement of Nab-Paclitaxel Antitumor Activity through
Addition of Multitargeting Antiangiogenic Agents in
Experimental Pancreatic Cancer
Niranjan Awasthi1,4, Changhua Zhang4,5, Anna M. Schwarz4, Stefan Hinz4,
Margaret A. Schwarz2, and Roderich E. Schwarz1,3,4
Abstract
Nanoparticle albumin–bound paclitaxel (nab-paclitaxel, NPT) has recently shown efficacy in pancreatic
ductal adenocarcinoma (PDAC). Targeting tumor angiogenesis is a sensible combination therapeutic strategy
for cancer, including PDAC. We tested the hypothesis that NPT response in PDAC can be enhanced by the
mechanistically different antiangiogenic agents bevacizumab (Bev) or sunitinib (Su), despite its inherently
increased tumor penetration and drug delivery. Compared with controls (19 days), median animal survival
was increased after NPT therapy (32 days, a 68% increase, P ¼ 0.0008); other regimens with enhanced survival
were NPTþBev (38 days, a 100% increase, P ¼ 0.0004), NPTþSu (37 days, a 95% increase, P ¼ 0.0004), and
NPTþBevþSu (49 days, a 158% increase, P ¼ 0.0001) but not bevacizumab, sunitinib, or BevþSu therapy.
Relative to controls (100 22.8), percentage net local tumor growth was 28.2 23.4 with NPT, 55.6 18 (Bev),
38.8 30.2 (Su), 11 7.2 (BevþSu), 32.8 29.2 (NPTþBev), 6.6 10.4 (NPTþSu), and 13.8 12.5
(NPTþBevþSu). Therapeutic effects on intratumoral proliferation, apoptosis, microvessel density, and stromal
density corresponded with tumor growth inhibition data. In AsPC-1 PDAC cells, NPT IC50 was reduced >6-fold
by the addition of sunitinib (IC25) but not by bevacizumab. In human umbilical vein endothelial cells (HUVEC),
NPT IC50 (82 nmol/L) was decreased to 41 nmol/L by bevacizumab and to 63 nmol/L by sunitinib. In
fibroblast WI-38 cells, NPT IC50 (7.2 mmol/L) was decreased to 7.8 nmol/L by sunitinib, but not by
bevacizumab. These findings suggest that the effects of one of the most active cytotoxic agents against
PDAC, NPT, can be enhanced with antiangiogenic agents, which clinically could relate to greater responses
and improved antitumor results. Mol Cancer Ther; 13(5); 1032–43. 2014 AACR.
Introduction not able to benefit from primary tumor resection. There-
Pancreatic ductal adenocarcinoma (PDAC) has the fore, much attention has been focused toward systemic
worst survival rate of all solid tumors. Despite recent treatment options for PDAC for possible definitive or
advancements in surgical procedures and availability of perioperative therapy benefits.
novel and more effective antineoplastic combination strat- Single agent gemcitabine has been a standard of care in
egies, the 5-year survival rate for PDAC overall remains advanced PDAC since 1997 after producing a response
less than 5% (1). Because of the lack of ability for early rate of 5% and a median survival of 5.7 months in a pivotal
detection of pancreatic cancer, most patients present with randomized trial (2). Currently, several clinical studies are
metastatic or locally advanced disease, and are therefore exploring gemcitabine-based combinations, either in con-
junction with other cytotoxic agents or targeting biologics,
to develop more effective and less-toxic regimens for
Authors' Affiliations: Departments of 1Surgery and 2Pediatrics; 3Indiana patients with PDAC.
University Health Goshen Center for Cancer Care, Indiana University Taxanes such as docetaxel and paclitaxel are mitotic
School of Medicine, South Bend, Indiana; 4Division of Surgical Oncology,
Department of Surgery, The University of Texas Southwestern Medical inhibitors that showed promising antitumor activities in
Center, Dallas, Texas; and 5Department of Gastrointestinopancreatic Sur- solid tumors (3, 4). These taxanes had limited clinical
gery, The First Affiliated Hospital of Sun Yat-Sen University, Guangzhou,
Guangdong, China
activity against PDAC (5, 6). Nanoparticle albumin–
bound paclitaxel (nab-paclitaxel, NPT) is a water-soluble,
Note: Supplementary data for this article are available at Molecular Cancer
Therapeutics Online (http://mct.aacrjournals.org/).
cremophor-free, albumin-bound 130-nm particle formu-
lation of paclitaxel. NPT is approved for the treatment of
Corresponding Author: Roderich E. Schwarz, Indiana University Health
Goshen Center for Cancer Care, Indiana University School of Medicine, 200 metastatic breast cancer based on its superior activity
High Park Avenue, Goshen, IN 46526. Phone: 574-364-2892; Fax: 574- compared with solvent-based paclitaxel (7). NPT initially
364-2480; E-mail: rschwarz@iuhealth.org was developed to avoid toxicity associated with the sol-
doi: 10.1158/1535-7163.MCT-13-0361 vent cremophor required to solubilize paclitaxel. Preclin-
2014 American Association for Cancer Research. ical and clinical data have demonstrated superior efficacy
1032 Mol Cancer Ther; 13(5) May 2014
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.
Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Nab-Paclitaxel Combinations with Antiangiogenic Agents
and safety of NPT over solvent-based paclitaxel (7, 8). A both supplemented with 10% FBS. HUVECs were grown
recent phase III clinical trial in patients with metastatic in EndoGRO-LS medium containing endothelial cell
adenocarcinoma of the pancreas showed a median sur- growth supplements (Millipore Corporation).
vival of 8.5 months in patients treated with NPT plus
gemcitabine compared with 6.7 months in the gemcita- Cell viability assay
bine-alone group (9). Recent experiments in our labora- Assays were performed in 96-well plates using the
tory demonstrated superior antitumor activity of NPT colorimetric WST-1 reagent as previously described (23).
compared with docetaxel or gemcitabine, providing a Briefly, cells were plated in a 96-well plate and treated with
strong rationale for evaluating NPT as first-line chemo- NPT, bevacizumab, and sunitinib. After a 72-hour incu-
therapy or as a backbone of combination regimens with bation, 10 mL WST-1 reagent was added in each well, and
potential biologic targeting or antiangiogenic agents in absorbance at 450 nm was measured after 2 hours using a
patients with pancreatic cancer (10). microplate reader. Drug sensitivity curves and IC50 values
Angiogenesis, an essential process for tumor growth were calculated using GraphPad Prism 6.0 software
and metastasis, is a well-established target for cancer (GraphPad Software).
therapy, including PDAC. Antiangiogenic agents includ-
ing bevacizumab (Bev), a monoclonal antibody against Western blot analysis
VEGF (11, 12), the COX inhibitor celecoxib (13), the EGF Subconfluent monolayers of cells were treated with
receptor inhibitor erlotinib (14), and various receptor NPT (10 mmol/L), bevacizumab (1 mg/mL), or sunitinib
tyrosine kinase (RTK) inhibitors (15) have been studied (10 mmol/L) and lysed after 16 hours. Tumor tissue lysates
in combination therapy in PDAC models. Sunitinib is a were prepared as previously described (24). Briefly,
multikinase inhibitor of several tumorigenic RTKs, tumor tissues were immediately snap frozen in liquid
including VEGF receptors (type 1 and 2), platelet-derived nitrogen and stored at 80 C. These samples were
growth factor (PDGF) receptors (a and b), c-KIT, FLT3, crushed in liquid nitrogen using a sterilized mortar,
and RET (16, 17). Sunitinib is currently approved for the resuspended in lysis buffer, and extracts were sonicated.
treatment of advanced renal cell carcinoma and imatinib- Proteins in supernatants were separated by SDS-PAGE
resistant gastrointestinal stromal tumors (18). VEGF and transferred to PVDF (polyvinylidene difluoride)
receptor and PDGF receptors are overexpressed and have membranes (Bio-Rad). Membranes were incubated over-
been correlated with poor prognosis in human PDAC (19, night at 4 C with the following antibodies: phospho-stath-
20). Sunitinib has been shown to have antitumor efficacy min (Ser38), cleaved PARP-1 (Cell Signaling Technology),
in experimental PDAC (21, 22). These findings suggest a-tubulin and GAPDH (glyceraldehyde-3-phosphate
that the multifactorial nature of pancreatic cancer may dehydrogenase; both from Sigma). The membranes were
be more effectively approached through treatment of mul- then incubated with the corresponding horseradish per-
tiple molecular targets, and thus provide a strong rationale oxidase (HRP)–conjugated secondary antibodies (Pierce
for studying the therapeutic potential of antiangiogenic Biotechnology). Enhanced chemiluminescence reagent
agents in combination with an effective cytotoxic agent. (ECL; PerkinElmer) was used to detect specific bands,
The present study evaluated combination treatment ben- which were then quantitated by densitometry.
efits of NPT with the multitargeting combination of the
antiangiogenic agents bevacizumab and sunitinib for Animal survival analysis
potentially enhanced PDAC clinical applications. Animal experiments were performed according to the
guidelines and approved Institutional Animal Care and
Materials and Methods Use Committee protocols of the University of Texas
Materials Southwestern Medical Center (Dallas, TX; animal proto-
NPT was obtained from Abraxis BioScience, bevacizu- col number 2012-0081) and the Indiana University School
mab was purchased from Genentech, and sunitinib was of Medicine (South Bend, IN; animal protocol number 16-
purchased from LC Laboratories, Inc. The cell prolifera- 023). Animal survival studies were performed using 6- to
tion reagent WST-1 was purchased from Roche Diagnos- 8-week-old female nonobese diabetic/severe combined
tics Corporation. immunodeficient (NOD/SCID) mice (25). The mice were
intraperitoneally injected with AsPC-1 (0.75 106) cells.
Cell culture Two weeks later, the animals were randomly grouped
The human pancreatic cancer cell lines AsPC-1 and (n ¼ 6 to 8 per group) and treated intraperitoneally with
Panc-1, the human umbilical vein endothelial cells PBS (control), NPT (10 mg/kg, twice weekly), bevacizu-
(HUVEC), and the human fibroblast cell line WI-38 were mab (10 mg per mouse, twice weekly), or sunitinib (20
all purchased from the American Type Culture Collection mg/kg, 5-times weekly) for 2 weeks. NPT, bevacizumab,
(ATCC). Cells were initially grown and multiple aliquots and sunitinib doses were selected on the basis of previous
were cryopreserved. All the cell lines were used within 6 studies in the literature (26–28). Mice were euthanized
months after resuscitation. AsPC-1cells were grown in when moribund according to predefined criteria includ-
RPMI-1640 medium; Panc-1 and WI-38 cells were grown ing rapid weight loss or gain (>15%), tumor size, lethargy,
in Dulbecco’s Modified Eagle Medium (DMEM; Sigma), inability to remain upright, and lack of strength. Animal
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1033
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.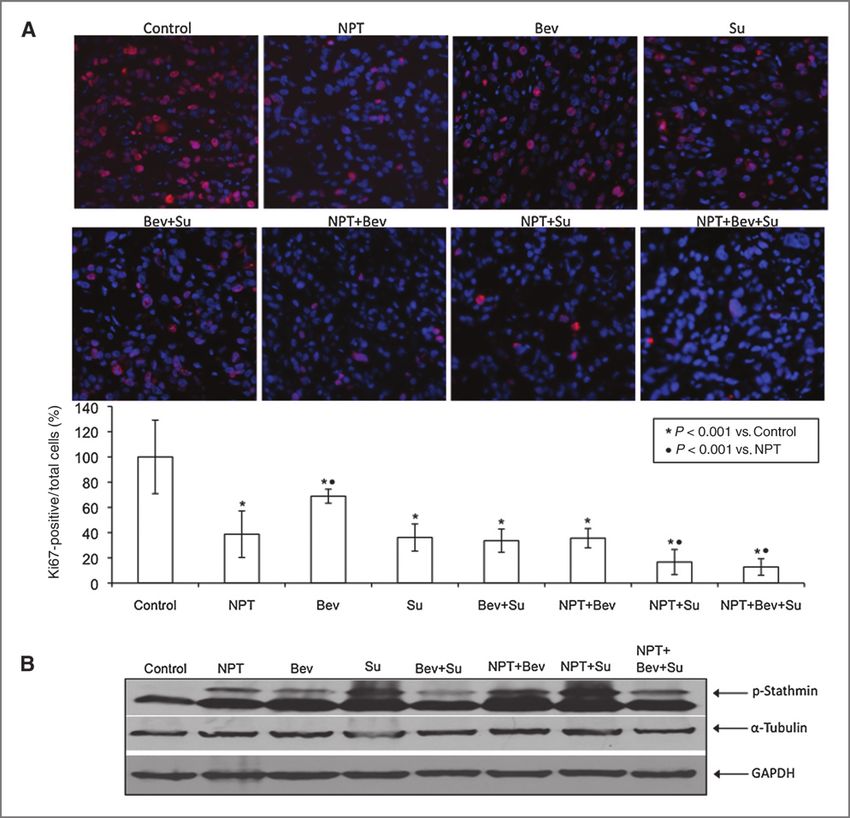
Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Awasthi et al.
survival was evaluated from the first day of treatment Student t test using GraphPad Prism 6.0 software (Graph-
until death. Pad Software) for individual group comparison. Statistical
analysis for in vivo tumor growth studies was performed
Tumor implantation and in vivo tumor growth by one-way ANOVA for multiple-group comparison and
experiment the Student t test for the individual-group comparison.
Female athymic nu/nu mice (ages 4–6 weeks) were Survival study statistics were evaluated using log-rank
used to establish a subcutaneous xenograft model as group comparison (GraphPad Prism 6.0). Values of P < 0.05
previously described (29). Mice were injected with were considered to represent statistically significant group
AsPC-1 cells (0.75 106) or Panc-1 cells (10 106), differences.
randomly grouped (n ¼ 6 to 8 per group), and intraper-
itoneal therapy started after 2 weeks with PBS (control), Results
NPT (10 mg/kg, twice weekly), bevacizumab (10 mg per Effects of NPT, bevacizumab, and sunitinib on animal
mouse, twice weekly), and sunitinib (20 mg/kg, 5-times survival
weekly). The tumor size was measured twice weekly Animal survival benefit was evaluated using an intra-
and tumor volume (V) was calculated by using the formula peritoneal PDAC murine xenograft model in NOD/SCID
[V ¼ 1/2 (L (W)2], where L ¼ length and W ¼ width. After mice after 2 weeks of therapy. The median animal survival
completion of treatment, the animals were euthanized, was 19 days in the control group and was significantly
tumors were removed, weighed, dissected, and processed improved by single agent NPT (32 days, a 68% increase
for histologic or immunohistochemical analysis. compared with control, P ¼ 0.0008), modestly improved
by sunitinib (24 days, P ¼ 0.045), but without any
Immunohistochemical analysis improvement with bevacizumab therapy (21 days, P ¼
Tumor tissues fixed in 4% paraformaldehyde were em- 0.18). Median survival after the combination of bevacizu-
bedded in paraffin. Intratumoral proliferative activity was mab with sunitinib (22 days, P ¼ 0.157) was also not better
measured by using Ki67 nuclear antigen staining as per than the control group. Combination of NPT with bev-
manufacturer’s protocol (Abcam). Briefly, tissue sections acizumab enhanced animal survival to 38 days (a 100%
(5 mm) were deparaffinized and rehydrated followed by increase compared with controls, P ¼ 0.0004 versus con-
heat-mediated antigen retrieval using citrate buffer. The trol, P ¼ 0.0005 versus bevacizumab, P ¼ 0.03 versus NPT),
tissue sections were incubated with CAS blocking buffer whereas the combination of NPT with sunitinib extended
followed by 1-hour incubation with Ki67 antibody (1:200) animal survival to 37 days (a 95% increase compared with
and a 40-minute incubation with Cy3 (1:200) secondary controls, P ¼ 0.0004 versus control, P ¼ 0.008 versus
antibody. Slides were mounted with DAPI (40 ,6-diamidino- sunitinib, P ¼ 0.17 versus NPT). Importantly, the combi-
2-phenylindole)-containing mounting solution (Invitro- nation of NPT with both antiangiogenic agents bevacizu-
gen). Proliferative activity was evaluated by calculating mab and sunitinib demonstrated the greatest observed
Ki67-positive cells from five different high-power fields survival benefit with a median survival of 49 days (a 158%
(HPF) in a blinded manner. Intratumoral apoptosis was increase compared with controls, P ¼ 0.0001 versus con-
analyzed by staining tissue sections with "Apoptag Apo- trol, P < 0.001 versus monotherapy groups; Fig. 1). No
ptosis Detection Kit" according to the manufacturer’s (Milli- significant change in mouse body weight was observed
pore) instructions. Intratumoral microvessel density (MVD) during 2-week therapy in all groups, indicating that there
was evaluated by incubating tissue sections with PECAM-1 was no significant drug-related toxicity even in the triple
(1:100) antibody (BD Pharmingen) overnight at 4 C follow- combination therapy group (Supplementary Fig. S1A).
ed by a 40-minute incubation with Cy3 secondary antibody.
Slides were mounted with DAPI-containing mounting NPT, bevacizumab, and sunitinib therapy effects on
solution. PECAM-1–positive vessels were calculated within local tumor growth
a microscopic HPF in a blinded manner. Intratumoral stro- Therapy effects on local tumor growth were evaluated
mal density was evaluated by incubating tissue sections in AsPC-1 subcutaneous tumor xenografts in athymic nu/
with a smooth muscle actin (a-SMA) or collagen I (1:200) nu mice. Treatment of AsPC-1 tumor-bearing mice with
antibody overnight at 4 C followed by a 40-minute incu- all three agents, either alone or in combination, caused an
bation with Cy3-conjugated secondary antibody. Slides inhibition in local tumor growth. Evaluation of tumor
were mounted with DAPI-containing mounting solution. volume during a treatment period of 3 weeks revealed
Fluorescence microscopy was used to detect fluorescent that the combination therapy groups BevþSu, NPTþSu,
signals using IX81 Olympus microscope and images were and NPTþBevþSu were more effective in inhibiting local
captured with a Hamamatsu Orca digital camera (Hama- tumor growth (Fig. 2A). However, some inhibition of local
matsu Corporation) with a DSU spinning confocal unit tumor growth in vivo was observed after all treatments;
using Slidebook software (Intelligent Imaging Innovations). compared with controls (100 22.8), percentage net local
tumor growth was 28.2 23.4 with NPT, 55.6 18 (Bev),
Statistical analysis 38.8 30.2 (Su), 11 7.2 (BevþSu), 32.8 29.2 (NPTþBev),
In vitro cell proliferation data are expressed as mean 6.6 10.4 (NPTþSu), and 13.8 12.5 (NPTþBevþSu; Fig.
SD. Statistical significance was analyzed by the two-tailed 2B). There was no significant change in mouse body
1034 Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.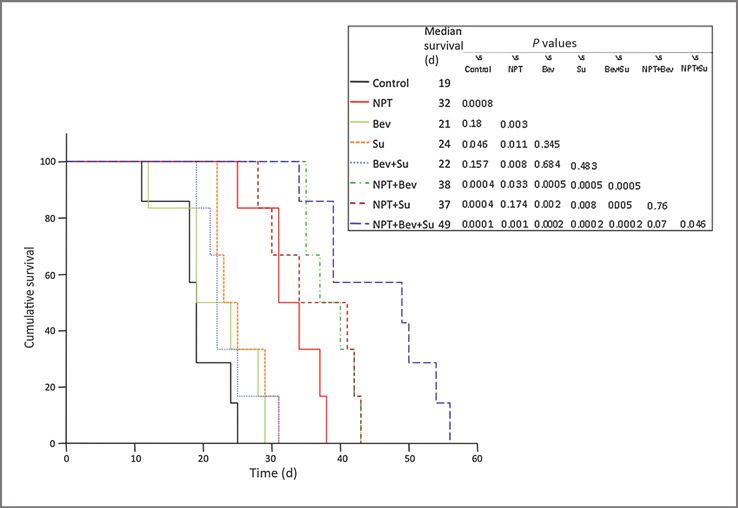
Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Nab-Paclitaxel Combinations with Antiangiogenic Agents
Figure 1. Animal survival evaluation
after treatment with NPT,
bevacizumab, or sunitinib. AsPC-1
tumor-bearing NOD/SCID mice
were treated for 2 weeks with NPT
(10 mg/kg, twice weekly),
bevacizumab (10 mg per mouse,
twice weekly), or sunitinib (20 mg/
kg, 5-times weekly), either alone or
in combination. The curve
represents animal survival time
from the start of therapy. Statistical
group differences in survival time
were calculated using log-rank
testing (GraphPad Prism 6.0).
weight during the experiment (Supplementary Fig. S1B). decreased in the NPT (39% 18%), bevacizumab (69%
The tumor weight measurement at completion of therapy 6%), sunitinib (36% 11%), BevþSu (34% 9%),
was very comparable to the final day tumor volume data NPTþBev (36% 8%), NPTþSu (17% 10%), and
(Supplementary Fig. S2). We also evaluated NPT, beva- NPTþBevþSu (13% 6%) therapy groups (Fig. 3A).
cizumab, and sunitinib treatment effects on local tumor The mechanism of cell proliferation inhibition was
growth in Panc-1 subcutaneous xenografts in athymic nu/ further investigated by analyzing the expression of phos-
nu mice and observed a similar pattern as seen in AsPC-1 pho-stathmin and a-tubulin, proteins regulating micro-
xenografts with all three agents inhibiting tumor growth. tubule dynamics. Immunoblot analysis of tumor lysates
Compared with the percentage net local tumor growth in from the subcutaneous xenografts revealed that NPT and
controls (100 46), the most effective groups showed a sunitinib increased the expression of phospho-stathmin,
net gain of only 4.3% 24% (BevþSu), or a net reduction an inactive form of stathmin, but no change in tubulin
of 11.2% 23% (NPTþSu) and 12.4% 28% expression. Bevacizumab also caused a small increase in
(NPTþBevþSu; Supplementary Fig. S3). Overall, group phospho-stathmin expression but no change in tubulin
differences were highly statistically significant as deter- expression (Fig. 3B and Supplementary Fig. S4).
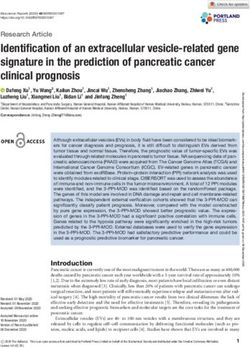
mined by one-way ANOVA (P < 0.0001). TUNEL staining was performed to analyze the effects of
NPT, bevacizumab, and sunitinib on intratumoral apo-
Intratumoral mechanisms of antitumor effects ptosis. Apoptotic index calculated by TUNEL-positive
The mechanisms of antitumor activities of NPT, bev- cells over total cells per HPF revealed that sunitinib was
acizumab, and sunitinib, either alone or in combination, more effective in inducing apoptosis followed by NPT and
were investigated by immunohistologic and immunoblot bevacizumab monotherapy. Combinations of NPT with
analyses of tumor tissues obtained from AsPC-1 subcu- bevacizumab or sunitinib were also effective but not
taneous xenografts of athymic nude mice after 3 weeks of significantly better than sunitinib alone (Fig. 4). Mean
therapy. apoptotic index in different treatment groups was as
Ki67 staining to analyze intratumoral proliferative follows: 0.02 0.01 (control), 0.07 0.02 (NPT), 0.04
activity demonstrated that NPT and sunitinib monother- 0.01 (Bev), 0.14 0.05 (Su), 0.18 0.03 (BevþSu), 0.11
apy were more effective in inhibiting intratumoral cell 0.05 (NPTþBev), 0.19 0.04 (NPTþSu), and 0.21 0.05
proliferation than bevacizumab alone. Compared with (NPTþBevþSu; Fig. 4).
single-agent treatments, the combination treatment The effects of NPT and antiangiogenic agents, bevaci-
groups NPTþSu (P < 0.0005) and NPTþBevþSu (P < zumab and sunitinib, on tumor vasculature was assessed
0.0001) were more effective, but the differences were not by PECAM-1 staining of tumor tissue sections. All three
statistically significant compared with the BevþSu or agents caused a reduction in MVD, sunitinib being the
NPTþBev groups. Compared with controls (100%), the most effective. The combination treatment group
intratumoral proliferative index, measured by calculating NPTþBevþSu showed some additive effects on decreas-
Ki67-positive cells over total number of cells per HPF, was ing microvessel counts, but these were not significantly
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1035
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Awasthi et al.
Figure 2. NPT, bevacizumab, and
sunitinib effects on growth of
established local PDAC tumors.
Nude mice were subcutaneously
injected with AsPC-1 cells and
therapy was started after 2 weeks.
A, relative tumor growth is
calculated by dividing the tumor
volume at any time by the tumor
volume at the start of treatment. B,
net tumor growth was calculated
by subtracting tumor volume on the
first treatment day from that on the
final day. Data are representative of
mean values SD from 6 to 8 mice
per group. , P < 0.05 versus
controls.
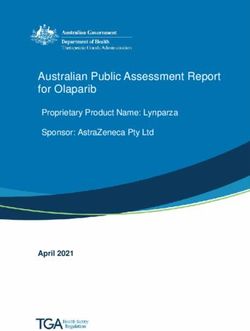
lower than after sunitinib alone (Fig. 5). Mean microvessel Effects on in vitro cell proliferation and related
counts per HPF were as follows: 21 4 (control), 12.9 2 protein expression
(NPT), 14.4 3.2 (Bev), 7 1 (Su), 9.3 1.5 (BevþSu), 10.9 To delineate the antitumor mechanism of the addition of
1.7 (NPTþBev), 6.5 2.1 (NPTþSu), and 3.8 1.7 bevacizumab and sunitinib to NPT on various cellular
(NPTþBevþSu; Fig. 5). MVD in the setting of NPT therapy lineage components present within the tumor microenvi-
was only significantly reduced by the addition of suniti- ronment, in vitro cell viability assays were performed using
nib, but not after bevacizumab. WST-1 reagent in the representative PDAC AsPC-1 cells,
The effects of NPT and antiangiogenic agents on HUVEC endothelial cells, and WI-38 fibroblast cells. In
tumor stroma were examined by fluorescent immuno- AsPC-1, NPT IC50 5.1 mmol/L was reduced more than 6
histochemical staining of stromal marker proteins col- fold by addition of an IC25 dose of sunitinib, but no signif-
lagen I and a-SMA. Relative to control, collagen I pixel icant effect was observed by bevacizumab addition at an
intensity was decreased in treatment groups by (in IC25 dose (Fig. 6A). In HUVEC, the NPT IC50 of 82 nmol/L
percentage) 66.6 14 (NPT), 31.2 10.2 (Bev), 54.1 was decreased to 41 nmol/L by bevacizumab and to 63
6.2 (Su), 70.6 8.7 (BevþSu), 71.9 6.3 (NPTþBev), 81.1 nmol/L by sunitinib. In WI-38 cells, the NPT IC50 of 7.2
1.7 (NPTþSu), and 83.2 2.6 (NPTþBevþSu; Sup- mmol/L was decreased to 7.8 nmol/L by sunitinib, whereas
plementary Fig. S5). Pixel intensity of a-SMA expres- no significant decrease was observed after bevacizumab
sion was also significantly decreased by NPT (68%, P < addition (Fig. 6A). The underlying mechanisms were fur-
0.0003) but less affected by bevacizumab and sunitinib; ther evaluated by analyzing the effects of these treatments
combination treatment groups were not significantly on the expression of phospho-stathmin, a-tubulin, and the
different from the NPT monotherapy group (Supple- apoptosis marker protein cleaved PARP-1. NPT treatment
mentary Fig. S6). caused a significant increase in phospho-stathmin and
1036 Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Nab-Paclitaxel Combinations with Antiangiogenic Agents
Figure 3. Intratumoral proliferative activity analysis after NPT, bevacizumab, or sunitinib therapy. AsPC-1 tumor-bearing athymic nude mice were treated for
3 weeks and tumors were dissected and processed for immunohistochemical analysis. A, tumor tissue sections were stained with Ki67 antibody and slides were
photographed under a fluorescent microscope. Ki67-positive cells were counted in five different HPFs. B, expression of phospho-stathmin and a-tubulin proteins
in tumor lysates. The intensity of bands was quantitated by densitometry. Data are representative of three independent experiments with similar results.
cleaved PARP-1 in all the three cell types. NPT decreased therapeutic options are the major contributors in the
a-tubulin expression in AsPC-1 cells but not in HUVEC or generally dismal prognosis of patients with pancreatic
WI-38 cells. Sunitinib treatment caused an increase in cancer. The modest effectiveness of gemcitabine, the dom-
cleaved PARP-1 protein but no change in phospho-stathmin inant chemotherapeutic agent used in PDAC, raises the
or a-tubulin expression. Bevacizumab treatment had no need for novel therapeutic strategies to be explored and
effect on phospho-stathmin, a-tubulin, or cleaved PARP-1 the underlying mechanisms of resistance to systemic
protein expressions in all the three cell types (Fig. 6B). treatments to be elucidated.
PDAC is characterized by the formation of a dense
Discussion stroma that not only plays an important role in cancer
Late-stage diagnosis, early and aggressive local inva- development, progression, invasion, and metastasis, but
sion and metastatic progression, and lack of effective also provides a mechanical barrier for the optimal
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1037
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Awasthi et al.
Figure 4. Intratumoral apoptotic activity measurement after NPT, bevacizumab, or sunitinib therapy. AsPC-1 tumor-bearing athymic nude mice were
treated for 3 weeks and tumors were dissected and processed for immunohistochemical analysis. Apoptotic activity was measured by staining tumor tissue
sections with TUNEL procedure and photographed under a fluorescent microscope. TUNEL-positive apoptotic cells were counted in five different HPFs.
The data are expressed as the mean SD.
delivery of chemotherapy (30). NPT has recently been and targeted therapy (32, 33). Therefore, the evaluation of
proposed to disrupt the PDAC stromal architecture, caus- combination treatment benefits of NPT with antiangio-
ing increased perfusion and delivery of gemcitabine, and genic agents seems logical and plausible in advanced and
as a result leading to higher antitumor responses in a NPT metastatic cancers. Because angiogenesis is critical for
and gemcitabine combination, as observed in the recent primary and metastatic PDAC progression, antiangio-
clinical PDAC trial (31). Recent studies in our laboratory genic treatment is a conceptually promising therapeutic
have shown that NPT is the most effective single cytotoxic strategy based on its potential for synergistic interaction
agent when compared with gemcitabine or docetaxel in with other antitumor agents, limited toxicity, and
experimental PDAC (10). In addition, in a breast cancer enhanced antitumor effects (34). However, resistance to
model, NPT has also been proposed to improve primary angiogenic inhibitors in the primary tumor and induction
tumor oxygenation by inhibiting the formation of novel of metastasis are two possibly major challenges for anti-
microvessel and by disrupting established microvessel, angiogenic therapy (35). In renal cell cancer, sunitinib has
thus improving the antitumor response of radiotherapy been shown to decrease local tumor growth but to also
1038 Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Nab-Paclitaxel Combinations with Antiangiogenic Agents
Figure 5. Tumor vasculature analysis after NPT, bevacizumab, or sunitinib therapy. AsPC-1 tumor-bearing athymic nude mice were treated for 3 weeks
and tumors were dissected and processed for immunohistochemical analysis. Tumor vascular was analyzed by staining tumor tissue sections with
PECAM-1 antibody and photographed under a fluorescent microscope. PECAM-positive microvessels were counted in five different HPFs. The data are
expressed as the mean SD.
increase VEGF expression and metastatic burden at the extended by the single target antiangiogenic agent bev-
same time, resulting in no survival benefit (36, 37). Also, in acizumab or the multitargeting antiangiogenic agent suni-
vivo antitumor activities of sunitinib have been shown to tinib to similar extent. Importantly, the maximum surviv-
depend not only upon its antiangiogenic activities, but al benefit was achieved when NPT was combined with
also upon its direct impact on tumor cells and stromal both bevacizumab and sunitinib. Advantages in combin-
components (16, 17, 38). The scope of the present study ing NPT with bevacizumab and sunitinib might be
was to evaluate the treatment benefits and underlying explained by previous studies showing that sunitinib
mechanism of NPT combinations with bevacizumab or inhibits signaling pathways involved in bevacizumab
sunitinib in experimental PDAC. resistance (36). These finding clearly support the impor-
Animal survival studies in an intraperitoneal murine tance of blocking multiple pathways by using mechanis-
xenograft model, which itself is well representative of the tically different antiangiogenic agents combined with
progression pattern of PDAC (39), revealed that NPT effective chemotherapy regimen for PDAC treatment.
significantly improved animal survival that was further Previous studies in our laboratory have shown that in
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1039
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Awasthi et al.
Figure 6. NPT, bevacizumab, and sunitinib effects on in vitro cell proliferation and related protein expression. A, cells were seeded into 96-well plates and
treated with different concentrations of NPT with or without IC25 dose of bevacizumab or sunitinib. After 72 hours of incubation, WST-1 reagent (10 mL)
was added and absorbance was measured at 450 nm that is proportional to the viable cells in each well. Data are the mean SD of triplicate determinations.
Drug sensitivity curves and IC50 values were calculated using GraphPad Prism 6.0 software. B, antiproliferative effects of NPT, bevacizumab, and
sunitinib correlate with increased phospho-stathmin and cleaved PARP-1 expression. Subconfluent cell monolayers were treated with NPT (10 mmol/L),
bevacizumab (1 mg/mL), or sunitinib (10 mmol/L), either alone or in combination for 16 hours. Total cell extracts were analyzed by immunoblotting for
p-stathmin, cleaved PARP-1, a-tubulin, GAPDH, and actin proteins. Data are representative of two independent experiments with similar results.
experimental PDAC, gemcitabine response can be imp- metastatic progression and is generally more easily affect-
roved by addition of one or more antiangiogenic agents ed by antiangiogenic agents (42).
(22, 29, 39–41). The current study thus extends this general Ki67 nuclear antigen staining is a prognostic marker in
notion for comparable combinations with the antimitotic metastatic pancreatic cancer (43). Decreased Ki67 staining
agent NPT, giving support to a rationale for using poly- by NPT and sunitinib, either alone or in combination
mechanistic antiangiogenic therapy independent from groups, indicate its role as biomarker for enhanced com-
the underlying cytotoxic agent’s mechanism. In addition, bination therapy efficacy. High resistance of PDAC to
this strategy seems to function even in the setting of conventional therapies is attributed to its resistance to
enhanced intratumoral delivery, a characteristic for NPT apoptosis (44). The greater apoptosis-inducing activity of
over other unbound taxanes. sunitinib compared with NPT or bevacizumab indicates
Subcutaneous murine xenograft studies revealed that that the contribution made by sunitinib in combination
NPT inhibited local tumor growth, but in contrast with the therapy are likely in part apoptotic pathway driven; this
survival experiment, single agent bevacizumab and suni- would explain the propensity of sunitinib to enhance NPT
tinib were also effective. This difference in effectiveness of effects more than those of bevacizumab. High PECAM-1
antiangiogenic agents in two different models can be staining, a well-established marker of MVD/angiogene-
attributed to the fact that the subcutaneous model lacks sis, in control tumor tissues confirmed an abnormal
1040 Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Nab-Paclitaxel Combinations with Antiangiogenic Agents
hypervascularity of PDAC. A decrease in MVD indicating represented in Fig. 3B, there was no significant change in
antiangiogenic effects was observed by all therapies via a-tubulin expression in tumor lysates, probably due to the
NPT, bevacizumab, and sunitinib; this effect was more presence of multiple nonepithelial cell types within the
pronounced in combination therapy groups. Further- samples derived from tumor tissues. In all the three cell
more, NPT decreased the tumor stromal density markers, types, sunitinib increased cleaved PARP-1 expression,
collagen I and a-SMA, that corroborate with previously whereas bevacizumab had no effect, again supporting
published report that NPT disrupts stromal architecture aspects of the multitargeting nature of sunitinib. The in
(31). NPT-containing combination therapy groups were vitro expression pattern of cleaved PARP-1 by NPT, bev-
also effective in decreasing collagen I and a-SMA con- acizumab, and sunitinib in all three cell types was very
tent. Overall, all these tissue-based analyses showed comparable with the in vivo apoptosis data indicating that
differential effects of NPT, bevacizumab, and sunitinib, cleaved PARP-1 is a good marker for therapeutic activity
but in general correlate with in vivo combination ther- in this setting.
apy effects, and could therefore be considered as clinical In summary, the present study demonstrates that
biomarkers of treatment efficacy for these combinations. although NPT already has strong antitumor activity as
Of course, all markers are mere surrogates for the actual a single agent, this is significantly enhanced by combina-
events taken place within the tumor tissue during treat- tion with the antiangiogenic agents bevacizumab and
ment, but the aggregate impression is that there is a sunitinib. Although the exact mechanism for the enhance-
considerable activity by NPT against stromal (vascular ment of NPT activity by bevacizumab or sunitinib remains
and fibroblastic) targets within the PDAC microenvi- unclear, it could be attributed to a decrease in angiogen-
ronment that can still be enhanced through the anti- esis, reduction of desmoplastic stroma formation, inc-
angiogenic agents used. reased delivery of NPT to tumor, and greater efficacy in
During further evaluation of the mechanism of action of growth inhibition of multiple cell types within the tumor
NPT combination with bevacizumab and sunitinib, in vitro microenvironment (49). These results strongly support a
cell viability studies revealed that NPT inhibited prolifer- rationale for combining polymechanistic, multitargeting
ation of the PDAC cell line AsPC-1. This cell line is very antiangiogenic agents with effective systemic therapy
aggressive and highly resistant to gemcitibine, which we such as NPT for clinical PDAC treatment.
consider useful for an experimental therapeutic approach
to PDAC (39). As expected, the addition of bevacizumab Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
had no meaningful effect on AsPC-1 proliferation, where-
as sunitinib addition effectively decreased the NPT IC50,
Authors' Contributions
supporting the notion that sunitinib has indeed direct Conception and design: N. Awasthi, R.E. Schwarz
antiepithelial effects in addition to its antiangiogenic prop- Development of methodology: N. Awasthi, R.E. Schwarz
erties (22). Targeting endothelial cells and fibroblast for Acquisition of data (provided animals, acquired and managed patients,
provided facilities, etc.): N. Awasthi, C. Zhang, A.M. Schwarz, S. Hinz,
solid tumor treatment has been shown to be a potentially M.A. Schwarz, R.E. Schwarz
effective strategy (45, 46). Furthermore, NPT inhibited Analysis and interpretation of data (e.g., statistical analysis, biostatis-
tics, computational analysis): N. Awasthi, C. Zhang, R.E. Schwarz
representative endothelial cells and fibroblast prolifera- Writing, review, and/or revision of the manuscript: N. Awasthi, S. Hinz,
tion, suggesting that its effect is not limited to epithelial R.E. Schwarz
cells but may well extend to tumor vasculature and stro- Administrative, technical, or material support (i.e., reporting or orga-
nizing data, constructing databases): C. Zhang, M.A. Schwarz, R.E.
mal architecture. In HUVECs, NPT effects were further Schwarz
improved by bevacizumab and sunitinib, but in WI-38 Study supervision: R.E. Schwarz
fibroblasts NPT effects were only enhanced by sunitinib
and not by bevacizumab. Stathmin, an important micro- Grant Support
tubule dynamics regulatory protein, is overexpressed in This work was financially supported in part by the Division of Surgical
Oncology, Department of Surgery, Simmons Comprehensive Cancer Cen-
several cancers (47). Antimicrotubule activities of taxanes ter, Hamon Center for Therapeutic Oncology Research, The University of
have shown to be correlated with phosphorylation and Texas Southwestern Medical Center funds (to R.E. Schwarz); and
thus inactivation of stathmin, decrease in tubulin, and 5R01HL114977 grant and the Lilly Endowment, Inc. Physician Scientist
Initiative (to M.A. Schwarz).
increase in apoptosis (48). In the present study, NPT The costs of publication of this article were defrayed in part by the
induced phospho-stathmin and cleaved PARP-1 in all payment of page charges. This article must therefore be hereby marked
three cell-types. NPT decreased a-tubulin only in AsPC- advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate
this fact.
1 but not in HUVECs or WI-38 cells, indicating that this is a
cell line–specific phenomenon, and not an essential com- Received May 8, 2013; revised January 29, 2014; accepted February 18,
ponent for an antiproliferative effect of NPT. Also, as 2014; published OnlineFirst March 7, 2014.
References
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer 2. Burris HA III, Moore MJ, Andersen J, Green MR, Rothenberg ML,
J Clin 2013;63:11–30. Modiano MR, et al. Improvements in survival and clinical benefit with
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1041
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Awasthi et al.
gemcitabine as first-line therapy for patients with advanced pancreas pancreatic cancer, and its relationship to angiogenesis. Eur J Cancer
cancer: a randomized trial. J Clin Oncol 1997;15:2403–13. 1998;34:1439–47.
3. Montero A, Fossella F, Hortobagyi G, Valero V. Docetaxel for treatment 20. Korc M. Pancreatic cancer-associated stroma production. Am J Surg
of solid tumours: a systematic review of clinical data. Lancet Oncol 2007;194:S84–6.
2005;6:229–39. 21. Tran Cao HS, Bouvet M, Kaushal S, Keleman A, Romney E, Kim G, et al.
4. Marupudi NI, Han JE, Li KW, Renard VM, Tyler BM, Brem H. Paclitaxel: Metronomic gemcitabine in combination with sunitinib inhibits multi-
a review of adverse toxicities and novel delivery strategies. Expert Opin site metastasis and increases survival in an orthotopic model of
Drug Saf 2007;6:609–21. pancreatic cancer. Mol Cancer Ther 2010;9:2068–78.
5. Rougier P, Adenis A, Ducreux M, de Forni M, Bonneterre J, Dembak M, 22. Awasthi N, Zhang C, Ruan W, Schwarz MA, Schwarz RE. Evaluation of
et al. A phase II study: docetaxel as first-line chemotherapy for poly-mechanistic antiangiogenic combinations to enhance cytotoxic
advanced pancreatic adenocarcinoma. Eur J Cancer 2000;36: therapy response in pancreatic cancer. PLoS ONE 2012;7:e38477.
1016–25. 23. Awasthi N, Schwarz MA, Verma V, Cappiello C, Schwarz RE. Endo-
6. Whitehead RP, Jacobson J, Brown TD, Taylor SA, Weiss GR, Macdo- thelial monocyte activating polypeptide II interferes with VEGF-
nald JS. Phase II trial of paclitaxel and granulocyte colony-stimulating induced proangiogenic signaling. Lab Invest 2009;89:38–46.
factor in patients with pancreatic carcinoma: a Southwest Oncology 24. Awasthi N, Zhang C, Ruan W, Schwarz MA, Schwarz RE. BMS-
Group study. J Clin Oncol 1997;15:2414–9. 754807, a small-molecule inhibitor of insulin-like growth factor-1
7. Gradishar WJ, Tjulandin S, Davidson N, Shaw H, Desai N, Bhar P, et al. receptor/insulin receptor, enhances gemcitabine response in pancre-
Phase III trial of nanoparticle albumin-bound paclitaxel compared with atic cancer. Mol Cancer Ther 2012;11:2644–53.
polyethylated castor oil-based paclitaxel in women with breast cancer. 25. Schwarz RE, McCarty TM, Peralta EA, Diamond DJ, Ellenhorn JD. An
J Clin Oncol 2005;23:7794–803. orthotopic in vivo model of human pancreatic cancer. Surgery
8. Desai N, Trieu V, Yao Z, Louie L, Ci S, Yang A, et al. Increased antitumor 1999;126:562–7.
activity, intratumor paclitaxel concentrations, and endothelial cell 26. Osgood RJ, Skipper J, Jiang P, Zimmerman S, Shepard HM, Maneval
transport of cremophor-free, albumin-bound paclitaxel, ABI-007, DC, Thompson CB, , et al. Pegylated recombinant human hyaluron-
compared with cremophor-based paclitaxel. Clin Cancer Res 2006; idase PH20 (PEGPH20) enhances nab-paclitaxel efficacy in BxPC-3
12:1317–24. human pancreatic cancer xenografts [abstract]. In: Proceedings of the
9. Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. 103rd Annual Meeting of the American Association for Cancer
Increased survival in pancreatic cancer with nab-paclitaxel plus gem- Research; 2012 Mar 31–Apr 4; Chicago, IL. Philadelphia (PA): AACR;
citabine. N Engl J Med 2013;369:1691–703. Cancer Res 2012;72(8 Suppl):Abstract nr 5635.
10. Awasthi N, Zhang C, Schwarz AM, Hinz S, Wang C, Williams NS, et al. 27. Zhang L, Smith KM, Chong AL, Stempak D, Yeger H, Marrano P, et al.
Comparative benefits of Nab-paclitaxel over gemcitabine or polysor- In vivo antitumor and antimetastatic activity of sunitinib in preclinical
bate-based docetaxel in experimental pancreatic cancer. Carcinogen- neuroblastoma mouse model. Neoplasia 2009;11:426–35.
esis 2013;34:2361–9. 28. von Baumgarten L, Brucker D, Tirniceru A, Kienast Y, Grau S, Burgold
11. Ko AH, Dito E, Schillinger B, Venook AP, Xu Z, Bergsland EK, et al. A S, et al. Bevacizumab has differential and dose-dependent effects
phase II study evaluating bevacizumab in combination with fixed-dose on glioma blood vessels and tumor cells. Clin Cancer Res 2011;
rate gemcitabine and low-dose cisplatin for metastatic pancreatic 17:6192–205.
cancer: is an anti-VEGF strategy still applicable? Invest New Drugs 29. Awasthi N, Schwarz MA, Schwarz RE. Enhancing cytotoxic agent
2008;26:463–71. activity in experimental pancreatic cancer through EMAP II combina-
12. Kindler HL, Niedzwiecki D, Hollis D, Sutherland S, Schrag D, Hurwitz H, tion therapy. Cancer Chemother Pharmacol 2011;68:571–82.
et al. Gemcitabine plus bevacizumab compared with gemcitabine plus 30. Mahadevan D, Von Hoff DD. Tumor-stroma interactions in pancreatic
placebo in patients with advanced pancreatic cancer: phase III trial of ductal adenocarcinoma. Mol Cancer Ther 2007;6:1186–97.
the Cancer and Leukemia Group B (CALGB 80303). J Clin Oncol 31. Von Hoff DD, Ramanathan RK, Borad MJ, Laheru DA, Smith LS, Wood
2010;28:3617–22. TE, et al. Gemcitabine plus nab-paclitaxel is an active regimen in
13. Dragovich T, Burris H III, Loehrer P, Von Hoff DD, Chow S, Stratton S, patients with advanced pancreatic cancer: a phase I/II trial. J Clin
et al. Gemcitabine plus celecoxib in patients with advanced or met- Oncol 2011;29:4548–54.
astatic pancreatic adenocarcinoma: results of a phase II trial. Am J Clin 32. Watkins G, Martin TA, Bryce R, Mansel RE, Jiang WG. Gamma-
Oncol 2008;31:157–62. Linolenic acid regulates the expression and secretion of SPARC in
14. Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. human cancer cells. Prostaglandins Leukot Essent Fatty Acids 2005;
Erlotinib plus gemcitabine compared with gemcitabine alone in 72:273–8.
patients with advanced pancreatic cancer: a phase III trial of the 33. Volk LD, Flister MJ, Bivens CM, Stutzman A, Desai N, Trieu V, et al.
National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol Nab-paclitaxel efficacy in the orthotopic model of human breast
2007;25:1960–6. cancer is significantly enhanced by concurrent anti-vascular endothe-
15. Assifi MM, Hines OJ. Anti-angiogenic agents in pancreatic cancer: a lial growth factor A therapy. Neoplasia 2008;10:613–23.
review. Anticancer Agents Med Chem 2011;11:464–9. 34. Konno H, Tanaka T, Matsuda I, Kanai T, Maruo Y, Nishino N, et al.
16. Abrams TJ, Lee LB, Murray LJ, Pryer NK, Cherrington JM. SU11248 Comparison of the inhibitory effect of the angiogenesis inhibitor, TNP-
inhibits KIT and platelet-derived growth factor receptor beta in pre- 470, and mitomycin C on the growth and liver metastasis of human
clinical models of human small cell lung cancer. Mol Cancer Ther colon cancer. Int J Cancer 1995;61:268–71.
2003;2:471–8. 35. Ebos JM, Kerbel RS. Antiangiogenic therapy: impact on invasion,
17. Mendel DB, Laird AD, Xin X, Louie SG, Christensen JG, Li G, et al. In disease progression, and metastasis. Nat Rev Clin Oncol 2011;8:
vivo antitumor activity of SU11248, a novel tyrosine kinase inhibitor 210–21.
targeting vascular endothelial growth factor and platelet-derived 36. Rini BI, Michaelson MD, Rosenberg JE, Bukowski RM, Sosman JA,
growth factor receptors: determination of a pharmacokinetic/pharma- Stadler WM, et al. Antitumor activity and biomarker analysis of sunitinib
codynamic relationship. Clin Cancer Res 2003;9:327–37. in patients with bevacizumab-refractory metastatic renal cell carcino-
18. Motzer RJ, Michaelson MD, Redman BG, Hudes GR, Wilding G, Figlin ma. J Clin Oncol 2008;26:3743–8.
RA, et al. Activity of SU11248, a multitargeted inhibitor of vascular 37. Ebos JM, Lee CR, Cruz-Munoz W, Bjarnason GA, Christensen JG,
endothelial growth factor receptor and platelet-derived growth factor Kerbel RS. Accelerated metastasis after short-term treatment with a
receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol potent inhibitor of tumor angiogenesis. Cancer Cell 2009;15:232–9.
2006;24:16–24. 38. Seandel M, Shia J, Linkov I, Maki RG, Antonescu CR, Dupont J. The
19. Fujimoto K, Hosotani R, Wada M, Lee JU, Koshiba T, Miyamoto Y, et al. activity of sunitinib against gastrointestinal stromal tumor seems to be
Expression of two angiogenic factors, vascular endothelial growth distinct from its antiangiogenic effects. Clin Cancer Res 2006;12:
factor and platelet-derived endothelial cell growth factor in human 6203–4.
1042 Mol Cancer Ther; 13(5) May 2014 Molecular Cancer Therapeutics
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Nab-Paclitaxel Combinations with Antiangiogenic Agents
39. Schwarz RE, Awasthi N, Konduri S, Cafasso D, Schwarz MA. EMAP II- metastatic pancreatic and midgut neuroendocrine neoplasms. Br J
based antiangiogenic-antiendothelial in vivo combination therapy of Cancer 2013;108:1838–45.
pancreatic cancer. Ann Surg Oncol 2010;17:1442–52. 44. Westphal S, Kalthoff H. Apoptosis: targets in pancreatic cancer. Mol
40. Awasthi N, Yen PL, Schwarz MA, Schwarz RE. The efficacy of a novel, Cancer 2003;2:6.
dual PI3K/mTOR inhibitor NVP-BEZ235 to enhance chemotherapy 45. Hayes AJ, Li LY, Lippman ME. Anti-vascular therapy: a new approach
and antiangiogenic response in pancreatic cancer. J Cell Biochem to cancer treatment. West J Med 2000;172:39–42.
2012;113:784–91. 46. Kalluri R, Zeisberg M. Fibroblasts in cancer. Nat Rev Cancer 2006;
41. Awasthi N, Zhang C, Hinz S, Schwarz MA, Schwarz RE. Enhancing 6:392–401.
sorafenib-mediated sensitization to gemcitabine in experimental 47. Bieche I, Lachkar S, Becette V, Cifuentes-Diaz C, Sobel A, Lidereau R,
pancreatic cancer through EMAP II. J Exp Clin Cancer Res 2013; et al. Overexpression of the stathmin gene in a subset of human breast
32:12. cancer. Br J Cancer 1998;78:701–9.
42. Fidler IJ. Critical factors in the biology of human cancer metastasis: 48. Li Y, Li X, Hussain M, Sarkar FH. Regulation of microtubule, apoptosis,
twenty-eighth G.H.A. Clowes memorial award lecture. Cancer Res and cell cycle-related genes by taxotere in prostate cancer cells
1990;50:6130–8. analyzed by microarray. Neoplasia 2004;6:158–67.
43. Khan MS, Luong TV, Watkins J, Toumpanakis C, Caplin ME, Meyer T. A 49. Jain RK, Duda DG, Clark JW, Loeffler JS. Lessons from phase III clinical
comparison of Ki-67 and mitotic count as prognostic markers for trials on anti-VEGF therapy for cancer. Nat Clin Pract Oncol 2006;3:24–40.
www.aacrjournals.org Mol Cancer Ther; 13(5) May 2014 1043
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.Published OnlineFirst March 7, 2014; DOI: 10.1158/1535-7163.MCT-13-0361
Enhancement of Nab-Paclitaxel Antitumor Activity through Addition
of Multitargeting Antiangiogenic Agents in Experimental Pancreatic
Cancer
Niranjan Awasthi, Changhua Zhang, Anna M. Schwarz, et al.
Mol Cancer Ther 2014;13:1032-1043. Published OnlineFirst March 7, 2014.
Updated version Access the most recent version of this article at:
doi:10.1158/1535-7163.MCT-13-0361
Supplementary Access the most recent supplemental material at:
Material http://mct.aacrjournals.org/content/suppl/2014/03/11/1535-7163.MCT-13-0361.DC1
Cited articles This article cites 48 articles, 17 of which you can access for free at:
http://mct.aacrjournals.org/content/13/5/1032.full#ref-list-1
Citing articles This article has been cited by 2 HighWire-hosted articles. Access the articles at:
http://mct.aacrjournals.org/content/13/5/1032.full#related-urls
E-mail alerts Sign up to receive free email-alerts related to this article or journal.
Reprints and To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Subscriptions pubs@aacr.org.
Permissions To request permission to re-use all or part of this article, use this link
http://mct.aacrjournals.org/content/13/5/1032.
Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
Rightslink site.
Downloaded from mct.aacrjournals.org on January 10, 2021. © 2014 American Association for Cancer Research.You can also read