Epidemiology of hospitalized patients April through June 2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical AND Health Affairs
COVID-19 IN MINNESOTA
Epidemiology of hospitalized patients
April through June 2020
BY ERICA BYE, MPH; KATHRYN COMO-SABETTI, MPH; RICHARD DANILA, PHD, MPH; CARMEN BERNU, MPH; AND
RUTH LYNFIELD, MD
Severe acute respiratory syndrome was male, in his 70s, and had recently re- travel; however, testing at the time was
coronavirus-2 (SARS-CoV-2) was first identified turned from a cruise. Initial cases in Min- restricted to certain international travelers
in December 2019 in China. Subsequently, nesota were associated with international as per the U.S. Centers for Disease Control
millions of coronavirus disease 2019 (COVID-
19) cases have been identified worldwide.
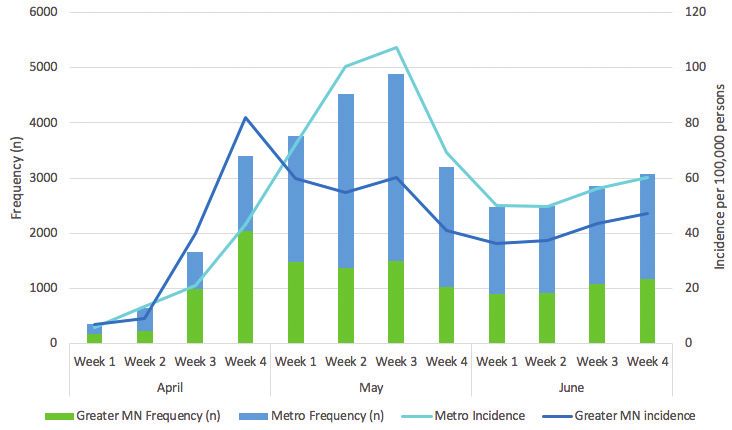
FIGURE 1
The Minnesota Department of Health
(MDH) implemented statewide surveillance Case Counts and Rate of Hospitalized COVID-19 Cases by
for laboratory-confirmed, hospitalized Week of Admission and Region, April 1 - June 30, 2020
COVID-19 cases as a part of the Centers for
Disease Control and Prevention Emerging
Infections Program Network. A total of 3,817
laboratory-confirmed cases of COVID-19
were hospitalized between April 1 and June
30, 2020. Ten percent of COVID-19 cases
in Minnesota were hospitalized, with an
incidence of 63 hospitalized cases per 100,000
population. Among 3,751 cases (94%) with
medical record review, median age was 59
years, 78% had >1 comorbidity, 63% had >2
comorbidities, 30% required admission to
an intensive care unit, and 13% died. Racial
and ethnic minorities were over-represented
and more than 80% of cases were from the
Minneapolis-St. Paul metropolitan area.
COVID-19 hospitalizations in Minnesota were FIGURE 2
similar to reports from other parts of the
Non-Hospitalized COVID-19 Cases by Week of Specimen
United States in spring 2020, with disparate
Collection and Region, April 1 – June 30, 2020
populations affected and high rates of ICU
admission and in-hospital death.
Introduction
Severe acute respiratory syndrome coro-
navirus-2 (SARS-CoV-2) was initially
identified in Wuhan, China, in Decem-
ber 2019. From the initial identification
through August 1, 2020, 17 million cases
of COVID-19 and 675,000 deaths were
reported globally1; the United States was
the largest contributor, with more than 4.5
million cases and 152,000 deaths.
The first laboratory-confirmed case of
COVID-19 in a Minnesota resident was
identified on March 6, 2020. The patient
SEPTEMBER/OCTOBER 2020 | MINNESOTA MEDICINE | 33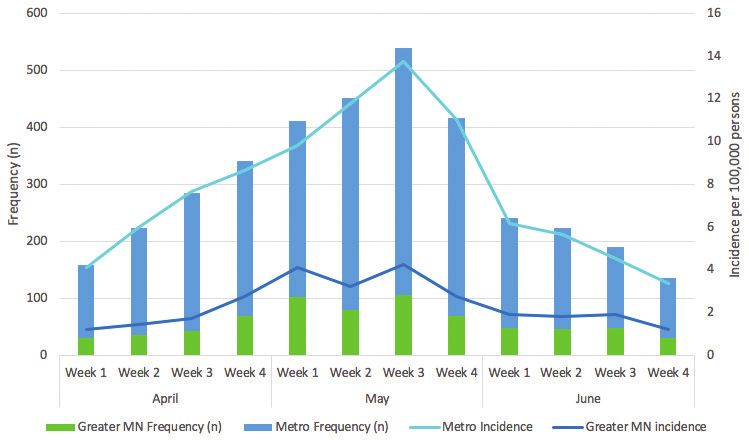
Clinical AND Health Affairs
TABLE 1
and Prevention (CDC) criteria. As testing
Demographic and clinical characteristics of cases hospitalized became more widely available in Minne-
with COVID-19, April 1–June 30, 2020
sota and testing criteria broadened, cases
METROPOLITAN GREATER P-VALUE TOTAL associated with community transmission
AREA* MINNESOTA N (%) and outbreaks in congregate and other set-
N (%) N (%) tings were detected. Minnesota COVID-
TOTAL n = 2,877 n = 694 n = 3,571 19 cases increased to over 55,000 cases
Age in years (median, IQR) 60, 45 – 74 57, 42 - 69Clinical AND Health Affairs
include Minnesota residents throughout ethnicity. Variables were included in mul- fied with an admission date from April 1
the state using COVID-NET methods. tivariate analysis when the p-value was < through June 30, 2020. After excluding
Medical record reviews were conducted 0.05. Multivariate analysis was conducted 246 patients where chart abstractions had
by trained surveillance officers using a using PROC LOGISTIC and PROC GEN- not yet been completed, 3,571 (94%) were
standardized case report form and proto- MOD controlling for age and presence of included in this analysis (97% chart review
col. Data collected included demographic an underlying condition. Case data were completion for seven-county metropolitan
(age, sex, race, and ethnicity) and clinical analyzed using SAS version 9.4 software area residents, and 83% completion for
variables (symptoms at time of admission, (SAS Institute Inc., Cary, NC, USA). charts of greater Minnesota residents).
presence of underlying medical conditions, Data were collected as part of routine Two thousand eight hundred seventy-
admission to an intensive care unit [ICU], public health surveillance and not subject seven (81%) cases resided in the metro-
laboratory testing, treatment, imaging, and to Institutional Review Board approval. politan area, and 694 (19%) were greater
discharge diagnoses and disposition). Minnesota residents. Overall incidence for
Cases with an admission date from Results hospitalizations was 63 cases per 100,000
April 1 through June 30, 2020 were in- A total of 37,192 laboratory-confirmed persons. Admissions peaked in the middle
cluded in this analysis. Analysis included cases were identified with a specimen col- of May and had a steady downward trend
a descriptive review of demographics, lection date from April 1 through June 30, into June for both residents of the metro-
underlying conditions, and outcome (e.g., 2020. Overall, case incidence for labora- politan area and greater Minnesota (Figure
ICU admission, in-patient mortality). tory-confirmed cases was 677 per 100,000 1), while non-hospitalized cases saw a
Multivariate models included age groups persons. Ninety percent (33,375) of cases steady increase throughout June (Figure
(50 years (Table 1). The
Clinical characteristics of cases hospitalized with COVID-19, median age for hospitalized cases was sig-
April 1–June 30, 2020 nificantly older than the median age of 38
METROPOLITAN GREATER P-VALUE TOTAL years (IQR 25-55 years) for overall cases
AREA* MINNESOTA (pClinical AND Health Affairs proportion of cases admitted from a facil- (51%), obesity defined as having a body toms at admission. Eleven percent (396) ity was greater among metropolitan cases mass index (BMI) ≥ 30 (35%), and dia- of cases had no documented symptoms compared to greater Minnesota cases (30% betes mellitus (32%) were the most com- at admission, 202 of which were pregnant vs 16%, p
Clinical AND Health Affairs those that did not need respiratory sup- in-hospital mortality after controlling for years. However, those older than 75 years port (median age: 62 years, IQR: 51–73 age and sex (OR: 3.58, 95% CI: 2.06–6.29, may have patient directives in place re- years vs median age: 59 years, IQR: 43–75 p
Clinical AND Health Affairs
sion was not widely recognized and testing in rates and case demographic, clinical and Rates and Characteristics of Patients Hospitalized with
Laboratory-Confirmed Coronavirus Disease 2019 - COVID-
was targeted at patients with recognized outcome characteristics. These data can NET, 14 States. Morbidity and Mortality Weekly Report.
COVID-19 symptoms. Retrospective as- help inform targeted education and pre- 2020; 69 (15):458-464.
certainment of this information is ongoing vention measures. MM 4. Guan Wj, Ni ZY, Hu Y, et al. Clinical Characteristics of
Coronavirus Disease 2019 in China. New England Journal
but not included in this analysis. Cases of Medicine. 2020; 382(18):1708-1720.
All authors are with the Minnesota Department of
residing in the metropolitan area were Health: Erica Bye, MPH, epidemiologist; Kathryn 5. Kim L, Garg S, O’Halloran A, et al. Risk Factors for
Como-Sabetti, MPH, supervisor of the Emerging Intensive Care Unit Admission and In-hospital Mortality
more likely to have a medical record re- among Hospitalized Adults Identified through the
Infections Unit; Richard Danila, PhD, MPH,
view completed than cases in greater Min- epidemiology program manager; Carmen Bernu, U.S. Coronavirus Disease 2019 (COVID-19)-Associated
Hospitalizations Surveillance Network (COVID-NET).
nesota. Therefore, data presented may not MPH, epidemiologist; and Ruth Lynfield, MD, state
Clinical Infectious Diseases. 2020; https://doi.org/10.1093/
epidemiologist.
represent characteristics of all hospitalized cid/ciaa1012.
Acknowledgments 6. Guan WJ, Liang WH, Zhao Y, et al. Comorbidity and
cases in greater Minnesota for this time Austin Bell, Kayla Bilski, Emma Contestabile, Kristen Its Impact on 1590 patients with COVID-19 in China: A
period. Ehresmann, Hannah Friedlander, Claire Henrichsen, Nationwide Analysis. European Respiratory Journal. 2020;
We observed certain characteristics Emily Holodnick, Melissa McMahon, Lisa Nguyen, 2000547.
Katherine Schleiss, Samantha Siebman, Maureen 7. Zheng Z, Peng F, Xu B, et al. Risk Factors of Critical &
that were associated with poorer out- Sullivan, Kristin Sweet, Minnesota Department Mortal COVID-19 Cases: A Systematic Literature Review
come among patients hospitalized with of Health. Mary G. Bernton, Hennepin County and Meta-analysis. Journal of Infection 2020; 81(2): e16-
Medical Center e25.
COVID-19, including older age and pres- 8. Petrilli CM, Jones SA, Yang Y, et al. Factors Associated
ence of comorbidities. Specific racial and with Hospital Admission and Critical Illness among 5279
R E F E R E N C E S people with Coronavirus Disease 2019 in New York City:
ethnic groups were also at higher risk for Prospective Cohort Study. BMJ. 2020; 369:m1966.
ICU admission and in-patient death even 1. Johns Hopkins Coronavirus Resource Center. COVID- 9. Centers for Disease Control and Prevention COVID-19
after controlling for sex and age. These 19 Map Johns Hopkins University and Medicine (2020, Response Team. Severe Outcomes Among Patients with
August 1) Retrieved from: https://gisanddata.maps.arcgis. Coronavirus Disease 2019 (COVID-19) United States,
finding highlight the need for preven- com/apps/opsdashboard/index.html#/bda7594740fd- February 12 – March 16, 2020. Morbidity and Mortality
tive measures, especially to protect those 40299423467b48e9ecf6 Accessed August 1, 2020 Weekly Reports. March 27, 2020; 69(12):343-346.
2. Minnesota Department of Health. (2020, August 1)
populations most vulnerable to COVID- Retrieved from: https://www.health.state.mn.us/diseases/
19. Ongoing surveillance of hospitalized coronavirus/situation.html
COVID-19 cases is needed monitor trends 3. Garg S, Kim L, Whitaker M, et al. Hospitalization
38 | MINNESOTA MEDICINE | SEPTEMBER/OCTOBER 2020You can also read

















































