How can informal caregivers in cancer and palliative care be supported? An updated systematic literature review of interventions and their ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review
Palliative Medicine
26(1) 7–22
How can informal caregivers in cancer and Ó The Author(s) 2011
Reprints and permissions:
palliative care be supported? An updated sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/0269216311409613
pmj.sagepub.com
systematic literature review of
interventions and their effectiveness
Richard Harding King’s College London, School of Medicine, Cicely Saunders Institute, Department of Palliative Care, Policy and Rehabilitation, UK
Sally List Countess Mountbatten Hospice, UK
Eleni Epiphaniou King’s College London, School of Medicine, Cicely Saunders Institute, Department of Palliative Care, Policy and Rehabilitation, UK
Hannah Jones King’s College London, School of Medicine, Cicely Saunders Institute, Department of Palliative Care, Policy and Rehabilitation, UK
Abstract
Introduction: Informal caregivers needs in cancer/advanced disease are largely unmet. The science of carer interven-
tion evaluation is methodologically challenging, and the evidence historically weak.
Objective: This systematic review updates an earlier effectiveness review to determine both the effectiveness of
subsequently published intervention studies, and the current state of science.
Method: The evidence was identified and appraised using a comprehensive search strategy. Articles were searched from
2001 to 2010 using the following electronic databases: Medline, PsychINFO and CINAHL. Inclusion criteria were studies
reporting intervention data for informal adult caregivers of a patient with a diagnosis of cancer or receiving palliative care.
The design and evidence rigour were assessed using the Jadad Rating Scale, and the Quality Rating Scale.
Results: 33 studies met inclusion criteria. From the original review, an encouraging increase was identified in the number
of evaluations (from 8 to 33), in carer-specific interventions (from 6 to 17) and in the robustness of the study design (an
increase from 2 to 12 studies with before/after measures, comparison groups and prospective data).
Conclusions: The evidence suggests a rapid increase in the number of robust intervention studies. However, the range
of models remains narrow in relation to caregivers’ needs and preferences.
Keywords
Cancer, caregivers, carers, palliative, systematic review
health or disabled populations) is that only a relatively
Introduction brief window of opportunity is available in which to
Studies have highlighted that informally caring for a learn new methods of coping, to put these methods into
relative or friend with cancer or advanced incurable practice, and to achieve an improvement in outcome.
disease can be associated with many problems, including Further, professionals must be careful to enhance
sleeplessness, general deterioration in health, exhaus- (rather than dismantle) existing coping strategies
tion1,2 and anxiety/depression.3 There have been consis- during the limited period of advanced disease, and be
tent calls for well-conducted intervention studies to mindful that while caregivers are helping the patient to
identify effective ways to support caregivers of patients prepare for dying, they are also trying to prepare them-
with cancer or those receiving palliative care.4,5 selves for the eventual death of their relative.6
However, the challenge of improving outcomes for Further methodological challenges to efficacy studies
caregivers in cancer and palliative care (compared to, are posed for those who attempt to undertake trials in
for example, informal care of the elderly, in mental populations with advancing disease. Even those who
Corresponding author:
Richard Harding, King’s College London, School of Medicine, Cicely Saunders Institute, Department of Palliative Care, Policy and Rehabilitation,
Bessemer Road, London SE5 9PJ, UK
Email: richard.harding@kcl.ac.uk
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 20128 Palliative Medicine 26(1)
succeed in conducting trials have concluded that it may Medline, CINAHL and PsychINFO databases were
not be possible to improve outcomes for informal searched from 2001 to the week of 1 July 2010.
carers in palliative care.7 Nevertheless, supportive and
palliative care aim to improve outcomes for family
Inclusion criteria
members and other caregivers, and guidance, such as
that of the National Institute for Health and Clinical Studies evaluating any type of intervention that explic-
Excellence (NICE), identifies the need to better sup- itly aimed to improve outcome(s) for current caregivers
port caregivers through delivery of evidence-based (i.e. unpaid informal providers of practical, physical or
interventions.8 emotional care) published in peer-reviewed journals,
The public health imperative to deliver effective and not included in the original review, were included.
interventions is great. During the last two weeks of Studies were required to be one of the following
life, both patients and carers identify anxiety in the designs: randomized controlled trial (RCT); prospec-
nearest carer as one of their biggest problems, and tive study; study with a concurrent mixed-methods
the needs of the family may exceed those of the design; qualitative post-intervention data; observa-
patient.9,10 Optimum home care for patients depends tional study with pre- and post-test measures.
on adequate care for the caregivers to sustain them in The study population for inclusion was adult infor-
their role.11 Despite a clear preference for home death, mal caregivers of adult patients with cancer or receiving
it is predicted that fewer than one in 10 will die at home palliative care. The final inclusion criterion was that
by 2030.12 A meta-analysis of the available evidence papers were published in the English language. Case
demonstrated that achieving home death is associated studies were excluded from the review, as were papers
with the availability of family support13 to the dying reporting models of intervention with no evaluation
patient. data. Bereavement interventions were also excluded.
Systematic reviews of evidence allow clinicians to
keep up-to-date with best practice, and are useful in
drafting (and delivering) clinical practice guidelines14
Study selection
and policy. A previous systematic review of carer out- The titles and abstracts of all the identified papers gen-
comes under cancer and palliative care was conducted erated from the search strategy were analysed and
in 2001 as ‘it was not yet clear how to meet assessed assessed against the eligibility criteria. Full versions of
need’.4 That review identified six interventions targeted the papers considered for inclusion were retrieved in
at caregivers that had evaluated their outcomes, order to make a final decision. Any papers that were
and concluded that ‘There was a lack of outcome eval- not clearly for inclusion or exclusion were reviewed by
uation designs, small sample sizes and a reliance on inter- SL, HJ and EE and adjudicated by RH.
vention descriptions and formative evaluations...The
current evidence contributes more to understanding fea-
sibility and acceptability than to effectiveness.
Analysis
Practitioners and evaluators must prioritize the further Data were extracted using common forms previously
development of intervention studies’. reported for systematic reviewing.15 Variables included
In order to appraise progress in methods, innovation paper reference (including country and year), interven-
in designing and delivering intervention, and the state tion model, palliative/cancer palliative or cancer
of science and evidence over the ensuing nine years, this population, intervention target population (i.e. solely
present study aimed to update the original review. caregivers or caregivers plus patients), study design,
intended intervention outcome, sample size, findings,
evidence grade (as applied in the previous review) and
Methods
study quality score.
Studies were identified using a systematic search of elec- Data were organized by intervention type, and the
tronic databases, with additional hand-searching of rel- evidence appraised according to the study quality. The
evant journals and reference lists of published papers. quality of the studies was assessed using two quality
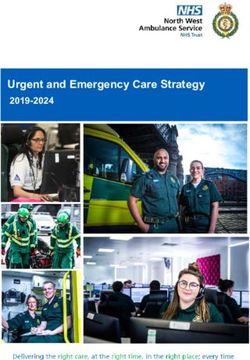
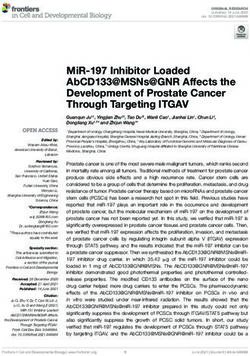
assessment tools. These were the Jadad scoring check-
list for randomized trials16 and the study design quality
Database search strategy rating system of the Clinical Guidance Outcomes
Keywords used for the search were the union of ‘carer*’ Group17 (the latter used in the original review) (see
and ‘caregiver*’ intersected with the union of ‘cancer’, Figures 1 and 2).
‘palliative’, ‘end of life’ and ‘terminal*’. These search The data were considered for suitability for meta-
terms were those of the original review,4 apart from the analysis (e.g. study quality, and heterogeneity of the
inclusion of the additional search term ‘end of life’. intervention, aims, sample and outcome tools).
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012Harding et al. 9
eQuestion Yes No
1. Was the study described as randomised? 1 0
2. Was the randomisation scheme described and appropriate? 1 0
3. Was the study described as double-blind? 1 0
4. Was the method of double blinding appropriate? (Were both the patient and the assessor
1 0
appropriately blinded?)
5. Was there a description of dropouts and withdrawals? 1 0
Figure 1. Jadad score.16 The maximum score is 5.
Grade I (Strong evidence)
RCTs or review of RCTS
IA Calculation of sample size and accurate standard definition
of appropriate outcome variables
IB Accurate and standard definition of appropriate outcome
variables
IC Neither of the above
Grade II (Fairly strong evidence)
Prospective study with a comparison group (non-randomized controlled
trial, good observational study or retrospective study that controls
effectively for confounding variables).
IIA Calculation of sample size and accurate, standard definition
of appropriate outcome variables and adjustment for the
effects of important confounding variables
IIB One or more of the above
Grade III (Weaker evidence)
Retrospective or observational studies
IIIA Comparison group, calculation of sample size, accurate and standard definition of
appropriate outcome variables
IIIB Two or more of the above
IIIC None of these
Grade IV (Weak evidence)
Cross-sectional study, Delphi exercise, consensus of experts
Figure 2. Evidence of Grading of Recommendations Assessment, Development and Evaluation (GRADE) grading criteria for review
of carer intervention studies.17 RCT: randomized controlled trial.
Results At the end of this process, 33 studies were included
in this review.
Literature search
A total of 10,817 citations were identified by the
search strategy in Medline, 810 in CINAHL and 1137
Origin of studies and populations
in PsychINFO. Following de-duplication, 33 were The reported data were collected in the following
retained following scrutiny against the inclusion crite- regions: USA n ¼ 11, Australia n ¼ 7, UK n ¼ 6,
ria. Hand-searching and the analysis of reference lists Canada n ¼ 4, Sweden n ¼ 2 and one each from
of reviews identified one further eligible study meeting Israel, Japan and South Africa. Concerning the
the inclusion criteria. One article could not be found research populations, the most interventions were in
despite attempting to contact the author (a qualitative cancer palliative care (n ¼ 15), with the remaining
evaluation of music therapy). equally conducted in palliative care (n ¼ 9) and
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 201210 Palliative Medicine 26(1)
cancer care (n ¼ 9). In terms of the target group for the Information and training interventions (n ¼ 3). The
intervention, 17 were targeted solely at carers and the fourth category of models, interventions that aimed
remaining 16 for both patients and carers. to deliver training and information, consisted of three
studies. The evaluation designs were one RCT,34 one
before and after single-group design35 and one retrospec-
Intervention models
tive study.36 The trial findings34 found that the Question
This review identified six intervention types. The Prompt List significantly increased the number of ques-
retained studies are reported in Table 1.7,18–48 tions that caregivers asked during medical consultations.
One-to-one psychological models (n ¼ 8). Eight Respite interventions (n ¼ 1). The fifth intervention
interventions were reported that were identified as model category was respite.
one-to-one and psychological. Of these, two were eval- Only one study47 reported this model, and used a
uated using an experimental RCT design,7,18 one using post-intervention structured (non-quantitative) inter-
an experimental design but no information on treat- view design.
ment allocation,19 three using single-group before/
after quantitative designs20–22 and two using post- Group interventions (n ¼ 10). The sixth category was
intervention qualitative methods.23,24 for group interventions, of which there were nine papers.
The RCT by Hudson et al.18 consisted of a psycho- Of these, two were ‘pure’ RCT evaluation designs,37–40
educational coping intervention delivered to carers by two were observational quasi-experimental designs,39,40
palliative nurses and aimed to increase the perceived three were before–after single-group designs,21,41,42 one
competence, rewards and preparedness and decrease was a single quantitative post-intervention43 and two
carers’ distress. The second RCT,7 in which 271 carers were qualitative post-intervention.44,45
received the intervention, involved weekly visits or tele- The first trial38 found significant improvements for
phone calls to the carer by a carer advisor and aimed to caregiver QoL, patients’ symptoms and caregiver task
increase support for depressed carers. Despite multiple burden. The trial that aimed to improve caregiver out-
endpoints in both studies, the only significant treatment comes through a group training intervention for
effect was in the Hudson study with respect to positive patients found no effect for caregivers.37
rewards of caring. Both studies were of high quality.
Physical interventions. The final category was of a
Psychological interventions for patient/carer dyads single paper that reported a yoga intervention using a
(n ¼ 4). For this intervention model, four intervention post-intervention survey.
studies emerged: three RCTs and one qualitative study.
Results from Northouse et al.,25 with 235 couples,
revealed improved quality of life (QoL), less uncer-
Discussion
tainty, higher self-efficacy and better communication Our systematic review has identified a significant
between patients and carers. Allen et al.26 indicated pos- and encouraging growth in the number of intervention
itive results too, with carers reporting reduced caregiv- studies that aim to improve outcomes for informal care-
ing stress and moderate reduction of depression. givers in cancer and palliative care, and an improvement
However, Northouse et al.27 fail to show significant dif- in the study designs used. Comparing the original sys-
ferences between the intervention and control group on tematic review (which reviewed the period 1966–August
uncertainty, hopelessness and coping. Evidence for the 2001) with the current review (which reviewed the ensu-
quality of the method was moderate in Allen et al.26 and ing 9 years from 2001 to July 2010), we find the follow-
Northouse et al.,27 while Northouse et al.25 was graded ing: an increase from 18 to 33 studies that have
more highly. evaluated outcomes for carers; an increase from 6 to
17 studies that report evaluations of interventions tar-
Palliative care/hospice interventions (n ¼ 6). Six geted solely at the caregiver; and an increase from 2 to 12
interventions were reported that were models of hospice study designs that incorporate before/after measures,
and palliative care delivery that evaluated outcomes for prospective data collection and a comparison group.
carers. These were evaluated using one RCT,28 one There are a number of limitations in conducting
matched retrospective cohort,29 two before/after single- systematic reviews, including the focus on the English
group designs,30,31 one post-intervention single-group32 language, the publication bias away from negative trials
and one mixed-method cross-sectional survey with focus and publication in non-indexed journals. However, our
groups.33 search strategy attempted to minimize these biases.
The single high-evidence grade study28 found no In drawing conclusions from this body of evidence,
effect on carer outcomes post-death. the model of intervention with the largest number of
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012Table 1. Data extraction tables: evidence of effectiveness of interventions for informal carers in cancer and palliative care
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
One-to-one/psychological interventions n ¼ 8 studies
Cameron et al., Single group prospec- Pall Ca C To enhance the problem-solving 58 carers of patients Small-scale project. 34 carers com- 0 III B
2004 Canada20 tive study abilities of carers, enhance confi- dying of cancer at pleted all aspects of the study.
Individual support dence of carers in their role and home 68% of carers – female, 73.5%
with 6/7 sessions decrease emotional distress carers married to patient. The
once a week for The Social Problem-Solving intervention resulted in
1.5 hours approx Inventory – Short Form, Profile improvements in emotional ten-
of Mood States, Caregiver sion (P ¼ 0.03), caring confidence
Assistance Scale and Caregiver (P ¼ 0.06), and positive problem-
Self-Sufficiency Scale solving orientation (P ¼ 0.06)
Hudson et al., 2009 Single group repeated Pall Ca C To evaluate the effectiveness of the 156 family carers Significant differences emerged 1 III B
Australia21 measures pro- psycho-educational intervention completed T1 between Time 1 and Time 2 on
An individual spective study for primary family carers of questionnaire. preparedness (P < 0.001),
psycho-educa- patients with advanced cancer to 62% of partici- rewards (P < 0.001), perceived
tional their preparedness, perceived pants completed competence (P < 0.001), and
intervention for competence, rewards and needs all 3 time periods information needs met
informal cancer Socio-demographic questionnaire, 70% women, spouse (P < 0.001)
carers delivered Carer Competence Scale, (59%) No significant differences emerged
over 3 weeks Preparedness for Caregiving between Time 2 and Time 3
in home palliative Scale, Family Inventory of Need, scores for all the four variables
care Rewards for Caregiving Scale,
program evaluation form
Hudson et al., 2005 RCT Pall Ca C The intervention would increase the 106 carers of a rela- No intervention effects were identi- 1 IA
Australia18 competence, rewards, levels of tive dying of fied concerning preparedness to
Psycho-educa- preparedness and decrease cancer at home. care, self-efficacy, competence
tional intervention anxiety Treatment n ¼ 54, and anxiety. However partici-
for family The Preparedness for Care giving control n ¼ 52. pants reported a significantly
caregivers of Scale, Caregiver Confidence more positive carer experience
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
patients dying of Scale, Rewards of Care giving than those who received stan-
cancer at home. Scale, HADS, Caregiver Self-Care dard care at both 5 weeks after
Self-Efficacy and Caregiver intervention and 8 weeks fol-
Problem-Solving Self-Efficacy lowing death of the patient
Milberg et al., 2005 Four tape recorded Pall Ca C To enhance the increased perception 22 carers of a relative The qualitative analysis resulted in 6 0 IIIC
Sweden24 focus groups of support and knowledge with advanced main categories: ‘reasons for
Clinical Nurse Qualitative analysis. Short question- cancer support group participation’,
Specialist (CNS) naire covering the role of the ‘group composition contributed
delivered, palliative care team and perceived to group cohesion’, ‘experience
individualized sup- support and sensitivity of group leader
portive was a catalyst’, ‘meaningful
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
intervention in dialogue helped to solve everyday
person problems’, ‘sense of cohesion
and by telephone increased effectiveness of the
over a 12-week group’, and ‘group sessions and
period post-session reflection increased
perception of inner strength’
The quantitative findings showed
participants wanted a support
group over a longer time period
Walsh and Face-to-face pilot Pall Ca C The intervention would decrease 14 carers of relatives Carers who completed the inter- 1 III C
Schmidt, 2003 study with pre- carers’ feelings of depression, diagnosed with vention experienced decreased
USA22 and post-test despair, and disorganization cancer; 5 carers depression, despair, and disorga-
A four-week tele- assessment of the Pre- and post-assessment package, completed study nization although the patient’s
phone interven- intervention including the Caregiver Burden before the patient condition deteriorated.
tion with Scale, Centre for Epidemiological died.
workbook Studies-Depression Instrument,
(Tele-Care II) for Inventory of Social Support and
carers of hospice the Hogan Grief Reactions
patients Checklist-End of Life
Walsh et al., 2007 RCT Pall Ca C The intervention would increase 271 carers of a rela- Mean scores in the intervention 3IA
UK7 support for distressed carers of tive with advanced group were lower at all time
A brief support patients with palliative care needs cancer entered points but these differences were
intervention General Health Questionnaire-28 the project. not significant. No difference
involving 6 weekly (GHQ-28), Eastern Cooperative Treatment ¼ 137 observed in secondary out-
visits or telephone Oncology Group (ECOG), control n ¼ 134 comes. Carers receiving the
calls to the carer Caregiver Strain Index, The At 4 weeks 16% intervention reported qualitative
by a carer advisor Caregiver Quality of Life Index- patients had died, benefit but study did not evi-
Cancer by 9 weeks 31% dence significant reduction in
(CQOLC) scale had died and by 12 psychological symptoms for
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
weeks 40% had carers with this intervention
died. Refusal rates
at each follow-up
point where the
patient remained
alive were 19%,
27% and 24%
respectively
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
Carter, 2006 USA19 A repeated measures Ca C To test the feasibility of The 30 cancer carers (15 The CASI is a feasible behavioural 0 II B
A brief cognitive- experimental Caregiver Sleep Intervention control & 15 intervention for cancer carers
behavioural inter- design (however (CASI) in improving the cancer intervention Intervention caregivers showed
vention that intervention & carer’s sleep quality, depressive group) more improvement in PSQI and
includes stimulus control group symptoms and quality of life. 63% female, 57% CES-D scores than controls. The
control, relaxa- allocation not The Actigraph Sleep Watch, Sleep spouses, 80% intervention appeared to
tion, cognitive described) Logs, Pittsburgh Sleep Quality Caucasian improve sleep quality and
therapy, and sleep Index (PSQI), Centre of depressive symptoms in the
hygiene elements. Epidemiological Studies- intervention group.
Depression Scale (CES-D), Improvements in quality of life
Caregiver Quality of Life-cancer scores were similar across
Scale (CQOLC) groups.
Ryan et al., 2008 Prospective, post- Ca C Macmillan’s support intervention for 81 carers received The project was well received by 0 IIIC
UK23 intervention quali- carers of patients with lung support from the carers as the MCP workers
Non-clinical com- tative case study cancer aimed to reduce carers’ MacMillan Carers offered information, useful con-
munity based design psychological morbidity, relieve Project (MCP), tacts, financial advice, practical
social support for burden and improve quality of life among them 20 and help and emotional support.
the carers of The Care Work Impact Appraisal carers were However some carers argued
patients with lung Questionnaire. interviewed that the MCP workers offered
cancer Semi-structured interviews for ‘old fashioned’ social work rather
Thematic Analysis than ‘care management’
Psychological interventions for patient/carer dyads n ¼ 4
Magill, 2009 Qualitative interviews Pall Ca P, C To evaluate the role of ‘preloss’ 7 bereaved cancer Descriptions of the meaning of the 0 IIIC
Canada46 of bereaved home home palliative care music ther- caregivers music by carers led to 4 themes:
Home-based palli- carers apy (for patients and carers) after ‘music is a conduit’, ‘music gets
ative care ‘preloss’ the death of the patient inside us’, ‘live music makes a
music therapy for difference’ and ‘music is love’.
patients and
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
carers
Northouse et al., RCT Ca P, C To examine whether a family-based 235 couples (112 At 4 months spouses in the inter- 51B
2007 USA25 intervention could improve intervention, 123 vention group reported signifi-
A family-based appraisal variables, QoL, coping control group) cantly better mental QoL
intervention for resources and symptom distress 84% of couples were (P < 0.05), better overall QoL
patients and their patients and their spouses during Caucasian, 65% of (P < 0.01), less negative appraisal
spouses consisting 3 phases of prostate cancer. patients were of caregiving (P < 0.01), less
of three 90- Medical Outcomes Study 12 item newly diagnosed, uncertainty about the illness
minute home (MOS SF-12), the general 14% in the bio- (P < 0.01) and less hopelessness
visits and two 30- Functional Assessment of Cancer chemical phase, (P < 0.05)
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
minute telephone Treatment (FACT-G), Appraisal 22% in the Higher self-efficacy at 4 and 12
sessions of Illness Scale, Appraisal of advanced stage months (P < 0.05) and better
Caregiving Scale, Brief Coping communication with patients at
Orientations to Problems all 3 assessments was also evi-
Experienced, Lewis Cancer Self- dent (P < 0.01), (P < 0.05),
Efficacy Scale, Lewis Mutuality (P < 0.01).
and Interpersonal Sensitivity
Scale, Omega Screening
Questionnaire (OSQ), Expanded
Prostate Cancer Index
Composite (EPIC)
Allen et al., 2008 RCT Pall Care C, P To decrease caregiving stress and 42 families entered The caregivers in the intervention 2IB
USA26 improve family communication the project. After group showed reduced caregiving
A family-based between caregivers and their 26% dropout: stress (P ¼ 0.034) and moderate
intervention con- patients by targeting meaning- Control n ¼ 14 reduction in depressive symp-
sisting of 3 home based coping dyads (patient toms and reported that their
visits Demographics, MMSE, Physical Self- with a life-limiting patients increased their social
Maintenance Scale and IADL illness and care- engagement (P ¼ 0.016). Patients
measures, Subjective well-being, giver) in the intervention group
ESAS: Edmonton Symptom Intervention ¼ 17 reported moderate improved
Assessment Scale- modified, dyads symptoms, reduced depressive
Additional symptom assessment, symptoms and increase sense of
Brief Multidimensional Measure religious meaning.
of Religion and Spirituality No changes were found in the care-
(BMMRS), Epidemiological giver’s estimates of symptoms.
Studies- Depression scale (CES-
D), Caregiver Stressor Scale -
revised, Project Evaluation
Survey
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
Northouse et al., RCT Ca C, P The intervention group will report 182 patient–family The family intervention showed a 3 IC
2005 USA27 more favourable psychological caregiver dyads; significant decrease in negative
Family-based outcomes 134 dyads (74%) appraisal of caregiving from
intervention for Appraisal of Illness Scale, Appraisal of completed 3 and 6 baseline to 3 months (P ¼ 0.004).
carers and Caregiving Scale, Mishel month follow-up. This change was not evident at
patients with Uncertainty in Illness Scale, Beck Intervention n ¼ six months.
recurrent breast Hopelessness Scale, Brief COPE, 69 dyads No differences between the
cancer delivered Control n ¼ 65 dyads control and intervention group
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
through a combi- the FACT scale version 3 and the on uncertainty, hopelessness,
nation of home SF-36 Survey coping and quality of life
visits and phone
calls.
Palliative care/hospice service n ¼ 6
Christakis and A matched retro- Pall Care C Spouses whose patients used hospice 195,533 elderly After adjustment for variables, an 0 II A
Iwashyna, 2003 spective cohort care would survive longer post couples odds ratio (OR) of 0.92 (95% CI:
USA29 study. Hospice bereavement 0.84–0.99) in favour of hospice
Analysis of Care use, n ¼ 30,383; Data from the Care after the Onset use occurs for widowed wives.
after the Onset of No hospice use, n of Serious Illness (COSI) data set Similarly, an OR of 0.95 (95% CI:
Serious Illness ¼ 30,383 drawn from Medicare claims 0.84–1.06) in favour of hospice
data to examine use occurs for widowed hus-
spouse mortality bands. This is only significant for
post bereavement women and the risk of death is
similar to that of other modifiable
risk factors in women.
Kirk and Collins, A single group Pall Care C, P Improved QoL following the intro- 24 patients, 17 after Statistically significant increase in 1 III C
2006 South pre- and post- duction of the hospital PCT 22.6% drop out FACT-Q percentage scores after
Africa30 evaluation of a FACT-G questionnaire introduction of HPCT
Evaluation of hos- hospital palliative (P < 0.001).
pital based pallia- care team Physical and functional wellbeing
tive care team scores were most improved; the
least improvement was seen in
social/family wellbeing.
Kusajima, 2009 A single group Pall Ca C, P Home palliative care would improve 55 family carers Reduced family anxiety about care at 0 IIIC
Japan31 pre- and family physical health, anxiety and home (p ¼ 0.002), however fre-
Evaluation of the post-evaluation sleep. quency of night time awakenings
transition to spe- Family health status and percep- for patient care increased
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
cialized home pal- tion of patient health status was (p < 0.001) and physical health
liative care for collected by qualitative interview. deteriorated (p ¼ 0.01)
patients and Families were asked to rate anxiety
families regarding care at home, fre-
quency of night-time awakening
for patient care, and physical
status in addition to perceptions
of patients’ physical and psycho-
logical status.
Grande et al., 2004 RCT Pall Care C, P HAH would increase quality of care 96 bereaved carers There was no evidence that HAH 3IA
UK28 for patient and so provide posi- Treatment n ¼ 78 had an impact on bereavement
Hospice at Home tive bereavement outcome for Control n ¼ 18 outcome. However perceptions
(HAH) service carers of inadequate terminal support
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
delivered by palli- Initial survey and letter to carers 6 and high symptom severity were
ative care nurses – months post-bereavement to associated with worse carer
input included participate in research interview bereavement response. Home
personal care for deaths were associated with
the patient, psy- better bereavement response
chological care for and better physical health post-
the carer and the bereavement than were inpatient
patient giving deaths.
information
McLaughlin et al., A single-group retro- Pall Care C, P To explore the bereaved caregivers’ 128 bereaved carers The bereaved caregivers were 0 III C
2007 UK32 spective study experience of the Hospice at returned the thankful for the Hospice at Home
Hospice at Home using a postal Home service delivered in one questionnaire – service. Areas highlighted for
service providing questionnaire region of the UK. 41% response rate improvement included the need
practical nursing The questionnaire used was designed for practical support, increased
care for the specifically for this study. awareness of the service and
patient and sup- bereavement support.
port and care for
the carer of the
patient
O’Connor, 2009 Survey and focus Pall Ca C, P Satisfaction with home care Survey: 300 carers High satisfaction with home care 0 III C
Australia33 group Focus group of bereaved and current (41.7% response (86.8%)
Evaluation of pri- carers, survey of carers receiving rate) Lack of continuity, Carers valued
vately provided care in previous 5 years Focus group: 7 patience and understanding from
palliative bereaved, 3 cur- staff but have poor knowledge
homecare rent carers and need to share their feelings.
Information and training n ¼ 3
Clayton et al., 2007 RCT Pall Ca C, P Provision of a QPL will influence 174 patients QPL carers asked 2.11 times more 3IA
Australia34 patients’/caregivers’ questions Treatment n ¼ 92, questions than controls (p ¼
Evaluation of and discussion topics during PC control n ¼ 82 0.0005) specifically with respect
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
Question Prompt consultations to lifestyle and quality of life (P ¼
List (QPL) booklet Coding of taped consultations; one 0.05), and end-of-life issues (p ¼
question from the CISQ; the 0.04). The total number of issues
SSAI; a specially designed ques- raised by caregivers was signifi-
tionnaire on information needs; cantly increased (p ¼ 0.08)
satisfaction Likert scales
Hendrix et al., Pre- and post follow- Ca C Confidence/self-efficacy in home care 20 carers of cancer Increased self-efficacy at post inter- 0 III C
2009 USA35 up study and symptom management patients vention (p ¼ 0.001) and at 1
Evaluation of indi- Caregiver Demographic week follow-up (p ¼ 0.01).
vidualized and Questionnaire, Cancer Caregiver
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
experiential train- Self-Efficacy (Confidence)
ing for cancer Questionnaire in Symptom
caregivers in Management (CCSE)
home care and
symptom manage-
ment of older pts
predicted to be
discharged to
home
Dobrof et al., 2006 A single-group, retro- Pall Care C Caregivers will benefit from social 169 caregivers There was a significant positive cor- 0 III C
USA36 spective assess- work interventions that focus relation between the number of
Evaluation of palli- ment of a support both on emotional impact and contacts and the number of pos-
ative care social program multiple resource issues itive results of social work inter-
work Specifically designed instrument ventions reported (p ¼ 0.0001).
interventions measuring caregiver characteris- This suggests that when care-
tics, social work interventions givers are engaged in services,
and the result of these caregivers’ abilities to cope and
interventions to acquire necessary resources
are enhanced.
Respite n ¼ 1
Barrett et al., 2009 Structured post- Pall Care C, P Respite care would improve carer 12 carers Carers showed satisfaction with care 0 IIIC
Australia47 intervention outcomes. and the opportunity for rest this
Implementation interviews A carer evaluation form evaluated gave. Carers perceived respite
and evaluation of the impact and perceptions of care providers to be competent.
an at-home pallia- carers of the service.
tive care respite
service.
Group
interventions n
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
¼ 10
McMillan et al., RCT Ca C, P Intervention would improve carer 329 patient–carer At the 30-day follow-up, the coping 5IB
2006 USA38 quality of life, carer burden, carer dyads skills intervention led to signifi-
A coping-skills burden due to tasks and carer Standard care n ¼ 109 cantly greater improvement in
training pro- mastery. dyads (60 at day caregiver QoL (P ¼ 0.03), burden
gramme for Caregiver Quality of Life Index, The 16, 40 at day 30) of patient symptoms (P < 0.001),
carers - with four Memorial Symptom Assessment Standard care plus and caregiving task burden (P ¼
components Scale, the Caregiver Demands support n ¼ 109 0.038). None of the groups
(COPE) Scale, the Brief COPE Scale and (47 at day 16, 32 showed significant change in
the General Caregiver Mastery at day 30) overall caregiving mastery, care-
Scale COPE intervention n giver mastery specific to caregiv-
¼ 111 (42 at day ing tasks, problem-focused or
16, 31 at day 30) emotion-focused coping.
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
Parsons and Ethnographic qualita- Pall Ca C, P Sharing and support 8 qualitative family Time to interact with staff, feeling 0 III C
Anderson, 2009 tive study Ethnography and qualitative inter- interviews supported through the gesture of
Canada45 views with patients to determine tea, sense of community and
Friday afternoon the meaning of Friday afternoon positive distraction, feel cared for
tea for patients tea
and families on a
palliative care unit
Cohen and Kuten, Quasi-experimental Ca C The CB intervention would reduce 104 carers (before Carers in the intervention group 1 II B
2006 Israel39 observational psychological distress þ increase drop out 143) scored significantly lower than
Cognitive study i.e. partici- psychological adjustment for Control n ¼ 52 the control group on the BSI and
Behavioural (CB) pants selected carers Intervention n ¼ 52 PAIS instruments, and reported
group interven- group Brief Symptom Inventory þ PAIS, the (drop out 27%) fewer sleep difficulties and higher
tion – 9 sessions Mini-Sleep Questionnaire þ the perceived support in the follow-
over 9 hours Multidimensional Scale of up measures. 30.8% of interven-
approx Perceived Social Support tion carers but only 3.9% of the
control carers had statistically
significant improvements in their
psychological distress. The inter-
vention lasted for 4 months after
intervention ended
Witkowski and A small-scale single- Pall Ca C, P Carer support provided – informa- 39 carers (48 before The intervention highlighted the 1 III C
Carlsson, 2004 group prospective tion, education and opportunity dropout) value of the group programme
Sweden43 study – with a to share experiences with other All subjects for carers with qualitative
A support-group phenomeno- carers answered five evidence.
programme of 5, graphic method Pilot study with 20 ranked most open-ended ques-
2-hour sessions. important topics for group pro- tions, and 12
gram. Questionnaire for carers completed semi-
and intervention staff to structured
complete interviews
Harding et al., 2004 A prospective, quasi- Pall Ca C To reduce anxiety, and increase psy- 73 carers of a relative There was a contradiction between 1 II A
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
UK40 experimental chological support and informa- with palliative care qualitative and quantitative data
A group work observational out- tion-giving and enhance short- needs may be result of pre-post mea-
intervention of a come study – term coping Control n ¼ 37 sure evaluation methods.
short-term closed involving qualita- Palliative Outcome Scale, Eastern Intervention ¼ 36 Attrition disallowed global mea-
group tive and quantita- Co-operative Oncology Group At baseline, post- sures from showing potential
tive methods Performance Scale, Zarit Burden intervention, and significant benefits, the qualitative
Inventory, Coping Responses follow-up, the data demonstrates that the pri-
Inventory, General Health intervention con- mary aims were met
Questionaire-12, State Anxiety dition consisted of
Scale Shortened Version 36, 24, and 15
carers,
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
respectively, and
the comparison
group included 37,
17, and 11 carers,
respectively
Kwak et al., 2007 Pre-post intervention Pall Care C Evaluating when the program can 2025 carers of a rela- The length of training significantly 1 II B
USA42 single group improve comfort with caregiving, tive during last increased the level of caregiver
Evaluating the sense of relationship closure, and years of life. comfort and closure experiences.
Caregiving at Life’s improve caregiver gain. Intervention n ¼ 926 Those who received an average
End (CGLE) pro- Comfort with Care giving Scale, completed pre- of 9.28 hours of training com-
gram A support- Caregiver Closure Scale and the and post-training pared to those who had an aver-
group programme Caregiver Satisfaction Scale questionnaires age of 5.26 hours had higher
of 9 modules levels of comfort and closure.
taking place over
approx 7.5 hours
Arnaert, 2010 Qualitative interviews Ca C Educate relatives of cancer patients 8 carers Benefits for carers included emo- 0 III C
Canada44 post-intervention how to communicate with the tional openness, shared experi-
Evaluating a ‘Skills medical system, inform them ences, mutual support and a
for Healing about nutrition and other com- sense of community
Retreat Weekend’ plementary therapies, provide
for carers. suggestions on how to manage
stress through relaxation and
yoga, inform them about support
group therapy and lectures on
alternative healing.
Qualitative interviews.
Hudson et al., 2008 Single-group repeated Pall Ca C To develop, deliver and evaluate a 74 people (56 females, Qualitative results: favourable feed- 1 III B
Australia41 measures pre- and group education programme 18 males) com- back with the majority of carers
A 3 week group post-study aimed to prepare cancer carers pleted Time 1 reporting that the programme
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
psycho-educa- for their role in supporting a questionnaires had a positive impact on their
tional intervention relative/friend receiving home- 44 people completed lives.
to prepare carers based palliative care all three time per- The intervention had a positive effect
for their role Demographic questionnaire, care- iods. 25% male, on the carers’ preparedness
giver competence scale, pre- 75% female (P < 0.001), competence
paredness for caregiving scale, (P < 0.01), rewards (P < 0.05) and
family inventory of need, rewards having needs met (P < 0.05) from
for caregiving scale, social sup- T1 to T2, which was maintained
port questionnaire, brief assess- at T3
ment scale for caregivers, life
orientation test, session evalua-
tion, programme evaluation,
semi-structured interviews
(continued)Table 1. Continued
Ca ¼ Cancer Pall
Ca ¼ Palliative
Cancer
Authors Country Evaluation Carers ¼ C Intended outcome þ Jadad Score
Intervention Design Patients ¼ P Measures Sample Results Evidence Grade
Hudson et al., 2009 Single group repeated Ca C To explore the utility and benefits of 20 informal family Following the family meeting, 0 II B
Australia21 measures pre- and using recently developed multi- carers of people between T1 and T2, carers were
Do family meet- post-study disciplinary clinical guidelines in with advanced less worried (P ¼ 0.001), the
ings reduce care 19 family meetings cancer (76% concerns arose less often (P ¼
needs of family Family Inventory of needs (FIN), women, 80% living 0.004) and the problem inter-
carers? pre-meeting questionnaires to with the patient, fered less with their lives (P ¼
assess the carer’s concerns; rate 59% spouse), 2 0.002)
their confidence. Short evalua- patients with The meeting had a positive effect
tion form after the meeting advanced cancer on having their needs met from
and 18 health T1 to T3 (P < 0.001)
professionals The meeting evaluation showed the
attended the carer’s positive attitude towards
meetings the meeting
Clark et al., 2006 RCT Ca P Evaluate how a patient-focused QoL Patients (n ¼ 103): 66 Although the intervention improved 1IB
USA37 intervention for cancer patients male, 37 female, the cancer patients’ overall QoL
An 8-session impacts the carer’s QoL and 17% had primary no overall between group differ-
structured multi- burden head and neck ences in the carers’ burden and
disciplinary inter- Linear Analog-self-assessment cancer, 15% lung QoL emerged
vention for cancer (LASA), Burden Interview cancer, 12% pri-
patients designed mary brain
to improve carer’s tumours.
burden and QoL Carers (n ¼ 83):
75% female, 86%
spouse.
Physical
intervention
n¼1
McDonald et al., A single-group post- Pall Care C, P Whether yoga sessions in the form 5 patients. The More than 90% of patients reported 1 III C
2006 UK48 treatment pilot of exercise, visualization and number of carers improved wellbeing and around
Evaluation of 12 evaluation relaxation would be beneficial was not specified 70% wanted more sessions.
week hospice Specially designed, simple survey of Following the success of the pilot
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012
yoga program patient views using Likert scales scheme the classes were
and yes/no responses. extended to the monthly support
Qualitative feedback. meeting for carers of day care
Carers not formally included in patients.
the study Carers participating reported they
experienced a marked reduction
in their stress levels; making them
feel relaxed and giving them a
general feeling of wellbeing.
CISQ: Clinical Information System Questionnaire, SSAI: BSI: PAIS: HADS: Hospital Anxiety and Depression Scale, RCT: randomized controlled trial, QoL: quality of live, MMSE: Mini Mental State Examination, IADL:
Instrumental Activities of Daily Living, PCT: primary care trustHarding et al. 21
(quasi)experimental evaluation data is the group inter- References
vention. This is the most commonly evaluated model 1. Barg FK, Pasacreta JV, Nuamah IF, Robinson KD,
of intervention, and has the largest number of Angeletti K, Yasko JM, et al. A description of a psychoe-
(quasi)experimental designs with 4 out of 10 studies. ducational intervention for family caregivers of cancer
Of these four, two reported some statistically significant patients. J Family Nurs 1998; 4: 394–413.
quantitative benefit for the intervention group over the 2. Ramirez A, Addington-Hall J and Richards M. ABC of
control. The next largest numbers of studies were one- palliative care. The carers. Br Med J 1998; 316: 208–211.
to-one psychological interventions (with three out of 3. Kinsella G, Cooper B, Picton C and Murtagh D. A
review of the measurement of caregiver and family
eight studies using (quasi) experimental methods, and
burden in palliative care. J Palliat Care 1998; 14: 37–45.
two of these finding a positive effect for the interven-
4. Harding R and Higginson IJ. What is the best way to
tion) and psychological interventions for patient/carer help caregivers in cancer and palliative care? A systematic
dyads (with three out of four using (quasi)experimental literature review of interventions and their effectiveness.
methods, and all three finding some positive effect). Palliat Med 2003; 17: 63–74.
In terms of outcomes, it is encouraging that the stud- 5. Hudson P. A conceptual model and key variables for
ies focus on a wide range of endpoints. This is to be guiding supportive interventions for family caregivers of
encouraged, as specificity of aims, intervention mecha- people receiving palliative care. Palliat Support Care
nisms and outcomes may be preferable over a ‘scatter- 2003; 1: 353–365.
gun’ approach that aims to improve too many outcomes 6. Steinhauser KE, Christakis NA, Clipp EC, McNeilly M,
within a fixed period of intervention. Further, it is essen- Grambow S, Parker J, et al. Preparing for the end of life:
preferences of patients, families, physicians, and other care
tial that some consensus is achieved in the selection of
providers. J Pain Symptom Manage 2001; 22: 727–737.
outcome measures to allow future meta-analysis.
7. Walsh K, Jones L, Tookman A, Mason C, McLoughlin J,
The timing of interventions and outcome measure- Blizard R, et al. Reducing emotional distress in people
ment also requires consideration – as palliative care is caring for patients receiving specialist palliative care.
often introduced late in the disease trajectory consider- Randomised trial. Br J Psychiatr 2007; 190: 142–147.
ation should be given to delivery outside of specialist 8. National Institute for Clinical Excellence (NICE).
palliative care services. In terms of measuring outcomes, ’Guidance on Cancer Services Improving Supportive and
it may be that follow-up post-intervention measurement Palliative Care for Adults with Cancer’, http://www.ni-
may miss the benefits that carers experience whilst in ce.org.uk/nicemedia/live/10893/28816/28816.pdf (2004).
receipt of targeted care, and therefore it may be advan- 9. Higginson I, Wade A and McCarthy M. Palliative care:
tageous and appropriate that measurement focuses on views of patients and their families. Br Med J 1990; 301:
277–281.
the ‘before–during’ period rather than the ‘before–after’.
10. Wingate AL and Lackey NR. A description of the needs
In terms of the populations in which studies were con-
of noninstitutionalized cancer patients and their primary
ducted, it is notable that almost none were from low- and care givers. Cancer Nurs 1989; 12: 216–225.
middle-income countries where the burden of terminal 11. Cull AM. Studying stress in care givers: art or science?. Br
illness is highest. Further, the needs of children and fam- J Cancer 1991; 64: 981–984.
ilies in paediatric palliative care merit specific study. 12. Gomes B and Higginson IJ. Where people die (1974–
With respect to analysis, the studies commonly reported 2030): past trends, future projections and implications
the persisting challenge of attrition on palliative care for care. Palliat Med 2008; 22: 33–41.
populations. In order to fully utilize the data points avail- 13. Gomes B and Higginson IJ. Factors influencing death at
able, longitudinal data analysis methods, such as multi- home in terminally ill patients with cancer: systematic
level models, should be advocated. review. Br Med J 2006; 332: 515–521. (Erratum appears
In conclusion, there has been an impressive increase in Br Med J 2006; 332: 1012).
in the number of targeted interventions for informal 14. Moher D, Liberati A, Tetzlaff J and Altman DG. Preferred
reporting items for systematic reviews and meta-analyses:
caregivers in cancer and palliative care. However, this
the PRISMA statement. Br Med J 2009; 339: b2535.
activity needs to continue to focus on mechanisms of 15. Gomes B, Harding R and Higginson IJ. Meeting existen-
intervention, tightly focused aims and outcomes, robust tial needs at the end of life: a systematic review of inter-
designs and a plurality of models and target popula- ventions. An Unpublished Systematic Review. King’s
tions/settings. College London, 2004.
16. Olivo SA, Macedo LG, Gadotti IC, Fuentes J, Stanton T
Funding and Magee DJ. Scales to assess the quality of randomized
This research received no specific grant from any funding controlled trials: a systematic review. Phys Ther 2008; 88:
agency in the public, commercial or not-for-profit sectors. 156–175.
17. Cancer Guidance Subgroup of the Clinical Guidance
Conflict of interest statement Outcomes Group. Improving outcomes in breast cancer -
None declared. the research evidence. Leeds: NHS Executive, 1996.
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 201222 Palliative Medicine 26(1)
18. Hudson PL, Aranda S and Hayman-White K. A psycho- trial of a prompt list to help advanced cancer patients and
educational intervention for family caregivers of patients their caregivers to ask questions about prognosis and
receiving palliative care: a randomized controlled trial. J end-of-life care. J Clin Oncol 2007; 25: 715–723.
Pain Symptom Manage 2005; 30: 329–341. 35. Hendrix CC, Abernethy A, Sloane R, Misuraca J and
19. Carter PA. A brief behavioral sleep intervention for Moore J. A pilot study on the influence of an individu-
family caregivers of persons with cancer. Cancer Nurs alized and experiential training on cancer caregiver’s self-
2006; 29: 95–103. efficacy in home care and symptom management. Home
20. Cameron JI, Shin JL, Williams D and Stewart DE. A Healthc Nurse 2009; 27: 271–278.
brief problem-solving intervention for family caregivers 36. Dobrof J, Ebenstein H, Dodd SJ and Epstein I.
to individuals with advanced cancer. J Psychosom Res Caregivers and professionals partnership caregiver
2004; 57: 137–143. resource center: assessing a hospital support program
21. Hudson P, Thomas T, Quinn K and Aranda S. Family for family caregivers. J Palliat Med 2006; 9: 196–205.
meetings in palliative care: are they effective?. Palliat Med 37. Clark MM, Rummans TA, Sloan JA, Jensen A, Atherton
2009; 23: 150–157. PJ, Frost MH, et al. Quality of life of caregivers of
22. Walsh SM and Schmidt LA. Telephone support for care- patients with advanced-stage cancer. Am J Hosp Palliat
givers of patients with cancer. Cancer Nurs 2003; 26: Care 2006; 23: 185–191.
448–453. 38. McMillan SC, Small BJ, Weitzner M, Schonwetter R,
23. Ryan PJ, Howell V, Jones J and Hardy EJ. Lung cancer, Tittle M, Moody L, et al. Impact of coping skills inter-
caring for the caregivers. A qualitative study of providing vention with family caregivers of hospice patients with
pro-active social support targeted to the carers of patients cancer: a randomized clinical trial. Cancer 2006; 106:
with lung cancer. Palliat Med 2008; 22: 233–238. 214–222.
24. Milberg A, Rydstrand K, Helander L and Friedrichsen 39. Cohen M and Kuten A. Cognitive-behavior group inter-
M. Participants’ experiences of a support group interven- vention for relatives of cancer patients: a controlled
tion for family members during ongoing palliative home study. J Psychosom Res 2006; 61: 187–196.
care. J Palliat Care 2005; 21: 277–284. 40. Harding R, Higginson IJ, Leam C, Donaldson N, Pearce
25. Northouse LL, Mood DW, Montie JE, Sandler HM, A, George R, et al. Evaluation of a short-term group
Forman JD, Hussain M, et al. Living with prostate intervention for informal carers of patients attending a
cancer: patients’ and spouses’ psychosocial status and home palliative care service. J Pain Symptom Manage
quality of life. J Clin Oncol 2007; 25: 4171–4177. 2004; 27: 396–408.
26. Allen RS, Hilgeman MM, Ege MA, Shuster Jr. JL and 41. Hudson P, Quinn K, Kristjanson L, Thomas T,
Burgio LD. Legacy activities as interventions approach- Braithwaite M, Fisher J, et al. Evaluation of a psycho-
ing the end of life. J Palliat Med 2008; 11: 1029–1038. educational group programme for family caregivers in
27. Northouse L, Kershaw T, Mood D and Schafenacker A. home-based palliative care. Palliat Med 2008; 22:
Effects of a family intervention on the quality of life of 270–280.
women with recurrent breast cancer and their family care- 42. Kwak J, Salmon JR, Acquaviva KD, Brandt K and Egan
givers. Psychooncology 2005; 14: 478–491. KA. Benefits of training family caregivers on experiences
28. Grande GE, Farquhar MC, Barclay SI and Todd CJ. of closure during end-of-life care. J Pain Symptom
Caregiver bereavement outcome: relationship with hos- Manage 2007; 33: 434–445.
pice at home, satisfaction with care, and home death. J 43. Witkowski A and Carlsson ME. Support group pro-
Palliat Care 2004; 20: 69–77. gramme for relatives of terminally ill cancer patients.
29. Christakis NA and Iwashyna TJ. The health impact of Support Care Canc 2004; 12: 168–175.
health care on families: a matched cohort study of hos- 44. Arnaert A, Gabos T, Ballenas V and Rutledge RD.
pice use by decedents and mortality outcomes in surviv- Contributions of a retreat weekend to the healing and
ing, widowed spouses. Soc Sci Med 2003; 57: 465–475. coping of cancer patients’ relatives. Qual Health Res
30. Kirk J and Collins K. Difference in quality of life of 2010; 20: 197–208.
referred hospital patients after hospital palliative care 45. Parsons S and Anderson C. The meaning of Friday after-
team intervention. S Afr Med J 2006; 96: 101–102. noon tea for informal caregivers on a palliative care unit.
31. Kusajima E, Kawa M, Miyashita M, Kazuma K and Int J Palliat Nurs 2009; 15: 74–78.
Okabe T. Prospective evaluation of transition to special- 46. Magill L. The meaning of the music: the role of music in
ized home palliative care in Japan. Am J Hosp Palliat palliative care music therapy as perceived by bereaved
Care 2009; 26: 172–179. caregivers of advanced cancer patients. Am J Hosp
32. McLaughlin D, Sullivan K and Hasson F. Hospice at Palliat Care 2009; 26: 33–39.
home service: the carer’s perspective. Support Care Canc 47. Barrett M, Wheatland B, Haselby P, Larson A,
2007; 15: 163–170. Kristjanson L and Whyatt D. Palliative respite services
33. O’Connor L, Gardner A, Millar L and Bennett P. using nursing staff reduces hospitalization of patients and
Absolutely fabulous–but are we? Carers’ perspectives on improves acceptance among carers. Int J Palliat Nurs
satisfaction with a palliative homecare service. Collegian 2009; 15: 389–395.
2009; 16: 201–209. 48. McDonald A, Burjan E and Martin S. Yoga for patients
34. Clayton JM, Butow PN, Tattersall MH, Devine RJ, and carers in a palliative day care setting. Int J Palliat
Simpson JM, Aggarwal G, et al. Randomized controlled Nurs 2006; 12: 519–523.
Downloaded from pmj.sagepub.com by SAGE Production (DO NOT CHANGE THE PASSWORD!) on January 11, 2012You can also read