How to Treat WOUND INFECTION - Prevention and treatment Richard Everts - ACC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

How to Treat
WOUND INFECTION
Prevention and treatment
Richard Everts
Online reading and accredited assessment available Free Access Code
www.howtotreat.co.nz/infection infection
COMPLETE YOUR FREE EDUCATION MODULE ONLINE
➤Go to www.howtotreat.co.nz/infection and use How much do you
the access code given on the cover of this reprint. already know?
Try this quiz
1. Topical antiseptic agents are
1 CR 1 HR 1.5 PT more likely than topical antibiotics
to cause allergic reactions.
True/False
2. Saline is preferred over tap
EARN CPD CREDITS WITH ELEARNING water for cleansing and irrigation
of acute traumatic wounds.
True/False
Reading How to Treat is an approved 3. Very severe pain is a common
1 CR individually planned learning activity recognised feature of necrotising infection.
True/False
by the RNZCGP for CPD purposes (1 credit).
4. Isolation of Pseudomonas
aeruginosa from a chronic ulcer
or wound usually indicates
The College of Nurses Aotearoa (NZ) endorses
a need for systemic antibiotic
1 HR the article for 1 professional development hour therapy, such as ciprofloxacin.
(CNA016). True/False
Answers on page 10
The Pharmaceutical Society of
1.5 PT
New Zealand allocates 0.75 ENHANCE
group 1 points if you read this article,
or up to 1.5 ENHANCE group 2 points
if you read this article and successfully complete the online ELearning
assessment. (Accreditation number PT16/6; expires 16/11/2018.)
Simply complete the online quiz-based assessment
at www.howtotreat.co.nz/infection
ELearning is a service provided by The Health Media, provider of
independent news and education to the primary care community in
New Zealand. The Health Media is the publisher of New Zealand Doctor,
Pharmacy Today, the Healthcare Handbook (an approved pharmacy
audit text) and the everybody patient sheets.
© The Health Media Ltd, 2017
+HOW TO TREAT
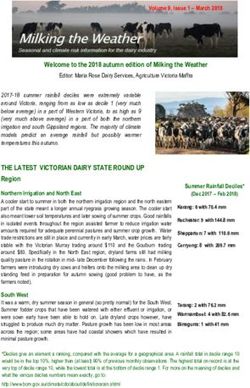
Wound infection:
Prevention and treatment
Wound infection following traumatic injury or minor surgery is inconvenient,
painful and can lead to failure or delay in wound healing and poor cosmetic outcomes.
It can also cause systemic infection requiring urgent intervention. This article
reviews the preventive and treatment approaches to this problem,
the burden of which all primary healthcare professionals can help reduce
T
housands of bacteria live normal In some cases, wound infection is very This article with how to prevent, recognise and treat
ly on every square centimetre of severe, causing necrotising cellulitis or was written by infections in chronic ulcers and wounds.
your skin. If the skin barrier is dis fasciitis; spread into local bone, tendon Richard Everts, Practising evidence-based medicine
rupted as a consequence of trauma, sur or joint tissues; systemic disease (eg, infectious in the field of wound care is a challenge
gery or disease, these bacteria may in shock); or metastatic spread to the spine disease given that much of the evidence is weak
vade and cause a symptomatic infection. or other distant sites. specialist and or equivocal. This leaves the subject
Micro-organisms from the environment Wound infections increase the cost of microbiologist, prone to “expert” opinions and product
(eg, soil, water) or from a mucosal surface care and antibiotic consumption. In the Nelson Bays promotion. This article sets out to provide
(eg, following a bite) may also contamin last five years, the Accident Compen Primary Health clear information and useful recommen
ate a skin wound. sation Corporation (ACC) in New Zea dations for primary care healthcare staff
The incidence of wound infection land has accepted more than 32,000 new and others in New Zealand.
ranges from 2 to 17.5 per cent after trau claims for infections related to trauma.
ma and from 1 to 1.5 per cent after minor For all of these reasons, it is important Topical antiseptics: advantages
dermatological surgical procedures. that doctors, nurses and pharmacists over topical antibiotics
Infections are inconvenient and pain know how to prevent and treat infections Antimicrobial medication and products,
ful, and lead to failure or delay in wound in traumatic wounds, burns and minor both topical and systemic, play an im
healing and poor cosmetic outcomes. surgical wounds. This article also deals portant role in preventing and treating
www.howtotreat.co.nz/infection HOW TO TREAT 3
→WOUND INFECTION
wound infections. anisms and a narrower spectrum of The broad spectrum of activity, mini
Topical antiseptic agents generally antimicrobial activity. They suffer from mal risk of resistance or cross-resistance
have multiple mechanisms of action resistance and sometimes lead to cross- and low risk of allergic reactions give
and a broad spectrum of antimicrobial resistance, and cause allergic reactions topical antiseptic agents short-term
activity, and uncommonly suffer from more frequently than antiseptic agents. and long-term advantages over topical
resistance or cause allergic reactions, but But, many are safe enough for systemic antibiotics in wound care, and this is
are too toxic for systemic use in humans. use in humans. reflected in the recommendations in
Topical antiseptic agents include Mupirocin, for example, is an antibi this article. Almost all of the topical anti
high-concentration ethanol, hydrogen otic active against Staphylococcus aureus septic agents discussed are available over
peroxide (eg, Crystaderm), iodine, chlor and beta-haemolytic streptococci. the counter and in public hospitals in
-hexidine (± cetrimide, eg, Savlon), Mupirocin resistance rates in S. aureus New Zealand.
sodium hypochlorite (bleach), super- have increased to over 60 per cent in some In view of the worsening global crisis
oxidizing solutions (eg, Microdacyn), places overseas, and to over 20 per cent with antibiotic-resistant bacteria, top
polyhexanide (with betaine, eg, Pronto in New Zealand in 2000, after nine years ical antibiotic use should be avoided in
san), acetic acid (vinegar), benzalkonium of over-the-counter availability. Since wound care. Oral and intravenous anti
(eg, Bepanthen), chloroxylenol (eg, restricting access to mupirocin in New biotic agents have an important but
Dettol), honey and silver. Bacteria have Zealand to prescription-only, in 2001, limited role for prophylaxis and treatment
not developed resistance to iodine, silver the S. aureus resistance rate has fallen of wound infection.
or polyhexanide, for example, despite Topical to less than 8 per cent. Mupirocin or
over 50 years of use. antiseptic fusidic acid resistance sometimes devel
In contrast, topical antibiotic agents – ops in S. aureus even during the course Practice point 1
agents generally
such as mupirocin (eg, Bactroban), fusidic of treatment with those agents. Antiseptics vs antibiotics
have multiple
acid (eg, Foban), gramicidin (eg, Sofradex, Another example of a topical antibiot Topical antiseptic agents are
mechanisms
Viaderm KC, Kenacomb), clindamycin, ic is neomycin, an aminoglycoside agent preferred over topical antibiotic
of action agents because they are broader
neomycin (eg, Pimafucort, Viaderm similar to gentamicin and tobramy
KC, Kenacomb, Neosporin, “triple anti- and a broad cin: neomycin causes allergic reactions in their spectrum of activity,
biotic cream”), framycetin (eg, Sofradex), spectrum of in up to 13 per cent of patients (com practically unaffected by anti
ciprofloxacin, clioquinol (eg, Locorten- antimicrobial pared with iodine at
+HOW TO TREAT
Are antiseptic agents safe
to put on a wound?
N
umerous animal and human iodine) cause less human cytotoxicity component) have additional anti-biofilm
studies undertaken since the than others (hydrogen peroxide, povidone- activity, which may be an advantage when
1960s show topical antiseptic iodine) at bactericidal concentrations. treating chronic ulcers and wounds.
agents have beneficial effects in acute Moreover, the in vivo applicability of Polyhexanide, cadexomer iodine prod
and chronic wound care. The popularity of these in vitro cytotoxicity studies has ucts and sustained-release silver dressings
antiseptic agents was seen to decline af been challenged because, in the labora have long-lasting activity, which reduces
ter in vitro studies published in the 1990s tory, the fibroblasts and keratinocytes the need for frequent dressing changes.
and 2000s showed that these agents dam are grown without the usual vascular Sustained-release silver products are more
age fibroblast and keratinocyte cell types support and proteinaceous environ- effective and safer than older silver for
in laboratory models. ment, and because most comparative mulations such as silver nitrate or silver
Since then, however, a number of clinical trials show no impairment of sulfadiazine; similarly, cadexomer iodine
studies have shown that, at lower con wound healing in the antiseptic arms. is more effective for treating chronic ul
centrations, antiseptic agents cause less cers and wounds than povidone-iodine.
human cytotoxicity. Potentially important differences Super-oxidizing solutions, like
Further, certain topical antiseptic between antiseptic agents Microdacyn, have performed better than
agents (super-oxidizing solutions, poly In addition to human cytotoxicity, there povidone-iodine and other comparators
hexanide, diluted sodium hypochlor are other potentially important differ in a number of clinical trials.
ite, chlorhexidine, silver and cadexomer ences between antiseptic agents. Some Most of the topical antiseptic agents
gram-negative bacilli are resistant to can occasionally cause local irritation or lo
chlorhexidine and benzalkonium, and cal or systemic allergic reactions, but these
Practice point 2 recent strains of S. aureus (especially Local adverse effects are less common than
Modern antiseptic agents MRSA, methicillin-resistant S. aureus; irritation with topical antibiotic agents and rarely
Most modern antiseptic agents including in New Zealand) are resistant or local or occur with super-oxidizing solutions.
are safe to put in a wound. Super- to chlorhexidine, cetrimide or benzal systemic Sodium hypochlorite (bleach) requires
oxidizing solutions, polyhexanide, konium, which potentially limits the use dilution (Table 1), which is a hassle, but
allergic
dilute bleach, chlorhexidine of these agents in the future. it is an effective and cheap antiseptic
(± cetrimide), sustained-release silver, In contrast, there is no resistance in
reactions...
agent and, therefore, a good option in
cadexomer iodine, povidone-iodine clinically important bacteria to super- rarely occur low-resource situations.
and honey are generally effective and oxidizing solutions, polyhexanide, sodi with super- Choosing an antiseptic agent from the
safe in wound care (see later sections um hypochlorite, silver, iodine, hydro oxidizing range of options described in this arti
for details and recommendations). gen peroxide or honey. Super-oxidizing solutions cle comes down to individual preference,
solutions and Prontosan (the betaine availability and cost.
Table 1 Sodium hypochlorite* dilution recommendations for use as a wound or skin antiseptic
Undiluted original Volume of bleach to add 2,3
bleach product1
To 500ml water To 1L water To 15L bucket To 30L water (a full-sized
bath with 10cm water)
Budget brand – Regular 1ml 2ml 35ml 70ml
(21.5g/L, 2.15%) (¼ teaspoon) (½ teaspoon) (2 tablespoons) (5 tablespoons)
Clor-o-gene 1.5ml 24ml 48ml
0.75ml
(31.5g/L, 3.15%) (¼ teaspoon) (5 teaspoons) (3 tablespoons)
Homebrand – Regular 0.6ml 1.2ml 18ml 35ml
(42g/L, 4.2%) (⅛ teaspoon) (¼ teaspoon) (3½ teaspoons) (2½ tablespoons)
Janola – Premium 0.6ml 1.2ml 18ml 35ml
(42g/L, 4.2%) (⅛ teaspoon) (¼ teaspoon) (3½ teaspoons) (2½ tablespoons)
* Bleach. 1. Use regular, not perfumed, bleach. 2. Based on a target concentration of 0.05g/L (0.005%), but up to five times more concentrated (0.25g/L,
0.025%) may be more effective and is still likely to be safe. 3. Add double the volume of bleach to the water if the bleach product is near its expiry date,
as sodium hypochlorite weakens with time to approximately half of its original strength by the expiry date
www.howtotreat.co.nz/infection HOW TO TREAT 5
→WOUND INFECTION
Preventing infection in
acute traumatic wounds
T
he risk of wound infection after recommended, including: may be effective, but is not well stud
trauma ranges from 2 to 17.5 per • manual removal of large foreign bodies ied. Honey-containing products may be
cent. Significant risk factors for • use of moist gauze or gentle scrubbing effective, but one brand of honey dress
infection are highlighted in Panel 1. with a brush to remove small pieces of ing did not improve outcomes in a small
foreign material randomised trial of patients with acute
Wound cleansing and • use of a scalpel, scissors or curette to minor traumatic wounds.
debridement remove necrotic, devitalised or macerat This author recommends the routine
Wound cleansing and debridement aim to ed tissue use of topical antiseptic agents in patients
remove foreign bodies, non-viable matter • irrigation with fluid (tap water and with acute traumatic wounds, especially
(exudates, slough, eschar) and contami saline have equal outcomes). those with extra risk factors for infection.
nating bacteria. The theoretical benefits Using pressure to cleanse or irrigate a These agents may be applied at the time
of cleansing and debridement are that wound may not be important, based of initial cleansing and subsequent dress
the remaining tissue is well vascularised on a recent, large randomised trial in ing changes. Different antiseptic products
and devitalised tissue that might support over 2500 patients with open fractures, are used in different ways – liquids may be
microbial growth and prevent access to Topical in which there was no difference in applied to the wound by irrigation, spray
leukocytes is removed. antiseptic outcomes between high-pressure, low- or soaked gauze; gels and creams may be
Wound infection risk is higher when agents...may pressure and very low-pressure irrigation. applied to the wound before or after clo
there is contamination with foreign ma be applied sure; and antiseptic-containing dressings
terial, such as wood or soil, and especially Topical antiseptic agents placed on the wound.
at the time
clay. Although a Cochrane review in 2012 in acute trauma
(CD003861.pub3) failed to find strong
of initial Experimental animal studies (mostly with Dressings for acute wounds
evidence that cleansing wounds per se cleansing and povidone-iodine) show either no effect Dressings provide numerous theoret
increases healing or reduces infection, subsequent or a reduction in wound bacterial count ical advantages in the management of
many studies show a benefit from wound dressing or clinical infection rate with the use of acute wounds, including the mainten
irrigation. Prompt cleansing and irri changes topical antiseptic agents. ance of a moist environment, removal of
gation of traumatic wounds are widely Human trials show reduced (most tri exudates and slough, thermal insulation
als) or little to no change in infection rates and reduction of further trauma. Dres
after acute traumatic skin break with top sings probably reduce the risk of wound
Panel 1 ical antiseptic or antibiotic treatment, infection.
Significant risk factors for infection compared with control; the reduction in The choice, frequency of change and
after acute trauma infection rate ranges from 10 to 70 per duration of dressing use are beyond the
cent. For example, a randomised trial of scope of this article but, for an acute
ucertain host factors: advanced age, obesity, diabetes and a triple-antibiotic gel or povidone-iodine traumatic wound, the dressing should
immune compromise, such as that due to chemotherapy cream for school children with accid- ideally protect against further trauma,
or high-dose steroids ental skin injuries reduced the infection have some capacity for absorption of dis
uwound location – this probably relates to arterial supply, rate from 12.5 per cent (placebo) to 1.6 charging fluid and blood, and be shower-
venous or lymphatic stasis and degree of contamination: the per cent (“triple-antibiotic” gel) or 3 per proof (eg, an “island” or foam dressing).
highest risk is on the distal limbs cent (povidone-iodine). The higher the risk of infection in the
uwound type and devitalised tissue: burst lacerations, crush There should be less concern about the wound (see above), the more frequently
injuries, large wounds human cytotoxicity seen in vitro with the dressing should be removed and the
uwound contamination: bites, faecal flora, soil, foreign bodies some antiseptic agents when these agents wound checked.
udelayed wound closure (possibly) are used in acute traumatic wounds,
especially those with healthy underlying General measures in
tissue and a reasonable blood supply. managing acute wounds
Although most of the studies of anti The control of hyperglycaemia in pa-
Panel 2 septic agents in acute traumatic wounds tients with diabetes may aid healing
Wounds generally requiring involved povidone-iodine, it is likely and prevent wound infection. Clinicians
prophylactic systemic antibiotics other topical antiseptic agents would should follow up-to-date guidelines for
also prevent infections in these patients. tetanus prevention, such as those in the
ucrush injuries Based on their broad spectrum of activ New Zealand Immunisation Handbook
ubites or oral wounds ity, evidence of clinical efficacy in various (Ministry of Health, 2014).
uwounds with gross contamination with soil or wood wound care situations and low risk of
uwounds to the feet or legs in the patient with lymphoedema toxicity, super-oxidizing solutions, poly Prophylactic systemic
or diabetes hexanide, dilute bleach (in low-resource antibiotics for acute wounds
udeep injuries (involving tendon, cartilage, joint or situations), chlorhexidine (± cetrimide), Some acute wounds are considered at
open fracture) cadexomer iodine, povidone-iodine, such high risk of infection that systemic
uwounds in patients with immune compromise (eg, poorly hydrogen peroxide and sustained-release antibiotics are given at the time of injury
controlled diabetes or immune-suppressive medication) silver are likely to be effective and reason
ably safe. Benzalkonium (Bepanthen) Continued on page 7
6 HOW TO TREAT www.howtotreat.co.nz/infection
+HOW TO TREAT
Preventing infection after
minor surgical procedures
C
ompared with traumatic topical antibiotic treatment will likely Topical antibiotic
wounds, the risk of infection result in more allergic or other adverse prophylaxis after
following an elective, minor, reactions than infections prevented. minor surgery
clean surgical procedure is low – general Moreover, widespread use of topical an will promote
ly less than 1.5 per cent. In these patients, tibiotic prophylaxis after minor surgical resistance
preoperative skin disinfection and post procedures will promote resistance and
operative dressings are probably effective cross-resistance.
in preventing infection. Although there has been no compara
Studies in patients undergoing major tive trial of a topical antiseptic agent in
surgical procedures show that a combi this situation, it is likely these agents are
nation of alcohol plus chlorhexidine or as effective as the antibiotics studied, but
alcohol plus iodine is most effective for without as high a risk of adverse reaction
preoperative skin disinfection. The com and without promoting antibiotic resist
mon practice of applying a topical anti ance. Therefore, if doctors or nurses wish
microbial agent once or more after a to use an antimicrobial agent or product
minor dermatological surgical proce to reduce the risk of infection after a
dure has also proven to reduce the risk of minor dermatological procedure, they
infection. should use an antiseptic agent. Practice point 4
A meta-analysis of four randomised Based on their broad spectrum of Preventing infection after minor
controlled trials of antimicrobial agents activity, evidence of clinical efficacy in surgical procedures
versus controls, including study pop various other wound care situations and 1. Preoperatively disinfect skin with a combination product
ulations totalling over 4000 patients, low risk of cytotoxicity, super-oxidized including alcohol plus either chlorhexidine or iodine.
showed that applying bacitracin, chlo solutions, polyhexanide, chlorhexidine 2. Use an intraoperative or postoperative antiseptic (not
ramphenicol, mupirocin or gentamicin (± cetrimide), slow-release silver, cadex antibiotic) agent – eg, super-oxidizing wound care solution or
postoperatively significantly reduced omer iodine, povidone-iodine and hy hydrogel, polyhexanide liquid or gel, chlorhexidine
the infection risk, with a pooled odds drogen peroxide are likely to be effective (± cetrimide), hydrogen peroxide, sustained-release silver,
ratio of 0.71 (J Dermatol Treat 2015; and safe. cadexomer iodine, povidone-iodine or honey.
26[2]:151–58). Honey dressings have shown mixed 3. Apply a protective, absorbent, shower-proof dressing
In these minor surgical cases, the success in comparative trials of post (eg, an “island” dressing).
baseline risk of infection is so low that operative wounds.
Continued from page 6 between injury and presentation in
creases the risk of contamination and Practice point 3
to prevent infection. Experimental ani infection in most studies, so it is com Preventing infection in acute traumatic wounds
mal studies show prophylactic antibiotics mon practice to delay closing the wound 1. Cleanse and debride all wounds to remove foreign
reduce acute wound infection, and hu when the patient presents a long time bodies, soil and non-viable tissue.
man clinical trials show prophylactic after the injury. 2. Topical antiseptic agents probably reduce infection risk
antibiotics reduce acute wound infection A 2013 Cochrane review on this topic and may be used in all acute traumatic wounds, at the time
in high-risk situations. (CD008574.pub3) concludes there are of initial injury and subsequent dressing changes. Avoid
Prophylactic systemic antibiotics are no proper comparative trials to answer topical antibiotic agents.
not indicated in low-risk, simple wounds the question of immediate versus a. Topical antiseptic options include super-oxidizing
but are generally indicated in more delayed closure for patients presenting wound care solution or hydrogel, polyhexanide liquid or
high-risk wounds (Panel 2). some time after injury. gel, dilute bleach (in low-resource situations, see Table 1
Amoxicillin+clavulanate, cefalexin, A general recommendation from for dilution instructions), chlorhexidine (± cetrimide), hydrogen
clindamycin and doxycycline are common other reviews and experts is that the peroxide, sustained-release silver, cadexomer iodine and
antibiotic choices, the latter two especial higher the risk of contamination, the povidone-iodine. Benzalkonium and honey may also be
ly in patients at high risk of MRSA colo better it is to delay closure, irrigate and effective.
nisation (see later section on treatment). debride the wound, apply a dressing, 3. Apply a protective, absorbent, shower-proof dressing
Prophylactic treatment usually continues consider antibiotic prophylaxis and (eg, “island” or foam dressing) or an absorbent pad.
for three to five days after a traumatic re-evaluate two to five days later. 4. Provide tetanus prevention, if appropriate.
injury, or longer if a bony fracture is Low-risk wounds (eg, scalp, face) can 5. Provide antibiotic prophylaxis (eg, amoxicillin+clavulanate
contaminated. generally be closed up to 24 hours after for three to five days) for wounds at highest risk of infection
the person sustains the injury, and high- (eg, large crush injuries; bites; gross contamination with soil;
Delayed wound closure risk wounds (eg, hands, diabetic feet, wounds in feet or legs with lymphoedema or diabetes; deep
Closing (suturing) an infected wound heavily contaminated, crush injuries, injuries involving tendon, cartilage, joint or open fracture;
or a highly contaminated wound may bites) can generally be closed up to 10 immune-compromised patients).
cause more harm than good. A delay hours after injury.
www.howtotreat.co.nz/infection HOW TO TREAT 7
→WOUND INFECTION
Preventing infection
after minor burns
B
acterial infection is a common requires frequent and painful dress
complication of burns, especial ing changes and may lead to antibiotic Practice point 5
ly large or deep burns. In addition resistance and allergic reactions. Silver Preventing infection
to cleansing and debridement of necrot nitrate has also been associated with after minor burns
ic skin and eschar, topical antimicrobial impaired healing. These older silver 1. Cleanse and debride burn
agents are recommended for patients products have been superseded by wounds to remove non-viable tissue
with burns that compromise the skin sustained-release silver dressings, which and eschar.
integrity. improve outcomes compared with 2. Topical antiseptic agents probably
There is no consensus on which anti standard care in comparative trials. reduce infection risk and aid healing
microbial agent should be used, but top Older silver A Co chrane rev ie w o f hone y in burns in which there is loss of skin
ical antiseptic agents have advantag (CD005083.pub4) reports that honey integrity. Options include sustained-
products
es over antibiotic agents in terms of the dressings heal burn wounds faster than release silver products, honey,
risk of adverse reaction or resistance.
have been other treatments. There are some data, super-oxidizing wound care solution
Silver sulfadiazine, for example, which superseded albeit limited, to support the use of or hydrogel, cadexomer iodine or
includes a sulphur-group antibiotic, has by sustained- chlorhexidine, super-oxidizing solutions dilute bleach (in low-resource
been the most common antimicrobial release silver or dilute bleach in burns care. MEBO, a situations; see Table 1 for dilutions).
agent used in burns for decades but has dressings popular Chinese herbal dressing, has not 3. Apply an appropriate dressing.
been associated with delay in healing, performed well in comparative trials.
Recognising and treating
infection in acute wounds
I
R EVERTS
nfection in an acute wound usual
ly presents with local pain, swelling,
redness or exudate, and sometimes
with regional lymphangitis or lymphad
enitis, systemic malaise, fever, abnormal
vital signs or raised C-reactive protein.
Wound swabs are not indicated in every
case but are most likely to give useful in
formation when the patient has high
risk factors for MRSA (eg, recently known
as MRSA-positive or household contact
MRSA-positive), is failing antibiotic Post-traumatic
treatment or has frank pus draining. wound with
Incision and drainage of any substan surrounding
tial collection of pus is essential. Systemic cellulitis
antibiotic treatment is generally neces
sary if invasive infection has spread
beyond the wound. For mild-to-moderate diate transfer to an acute surgical team; trauma, such as a skin laceration, abra
infections treated in the community, the features of a necrotising infection are sion or bruising. Clear documentation
recommendations for antibiotic choice presented in Panel 3. A GP may adminis of the time, circumstances and sequence
are provided in Table 2. ter intravenous amoxicillin+clavulanate of the traumatic event, signs of physical
More severe wound infections may re or ceftriaxone before the patient is taken injury, and the time of onset and
quire intravenous antibiotics and surgical by the ambulance to hospital if necrotis description of the infection will assist
assessment, and some complex wounds ing infection or severe sepsis is suspected. ACC to assess the claim. It would help
require – during or after infection treat Consider lodging an ACC claim for in to document any other factors that might
ment – negative pressure wound thera fection following a traumatic wound. have contributed to the infection, such
py (NPWT), also known as VAC (vacu This claim should clearly define the trau as previous skin or wound infections,
um-assisted closure). Necrotising fasciitis matic event (not just a minor every chronic skin conditions (eg, eczema,
and necrotising cellulitis are surgical and day twist, strain or friction) and docu psoriasis), lymphoedema at the site of
medical emergencies and require imme ment the objective physical evidence of infection or diabetes.
8 HOW TO TREAT www.howtotreat.co.nz/infection+HOW TO TREAT
Diagnosing infection in
chronic ulcers and wounds
I
nfection in chronic ulcers and wounds pain, discharge, a stinky odour and delay debris and exudate, and debrided to re
is difficult to define. Patients present in healing. These gram-negative bacteria move any necrotic tissue or eschar. Then
anywhere along a spectrum from and anaerobes most often colonise ulcers moisten the swab, especially if the ulcer or
simple, harmless colonisation to frank and chronic wounds without any clinical wound is dry, and twirl the tip of the swab
invasive disease, such as cellulitis, un impact. for a few seconds with pressure over the
derlying joint or bone involvement, or The culture results from a swab sam ulcer or wound bed.
septic shock. Diagnosis at either end of ple of the ulcer or wound also correlate The presence of white cells on micros
this spectrum (no infection or infection) with invasive infection, but not exactly. copy and a predominant pathogen on
may be easy. The middle of the spectrum, Whether or not to take a swab and how culture in the laboratory report sug-
however, is more difficult, especially if to interpret the result both require some gest an infection. S. aureus and beta-
there is underlying arterial insufficiency thought. haemolytic streptococci are premier
causing pain, or venous disease causing If clinical infection is not suspected, the soft-tissue pathogens and are most likely
stasis dermatitis. swab result will very likely be misleading, to be associated with invasive infection;
The further along this spectrum to so it is best not to take it in the first place. they represent causative pathogens.
wards invasive disease, the more likely it Even if clinical infection is suspected, the
is the patient presents with pain, swelling, swab result should not change your man
redness or exudate, regional lymphangitis agement if the patient is responding to Panel 3
or lymphadenitis, systemic malaise, fever, empiric antibiotic treatment targeting Clues to necrotising infection
abnormal vital signs or raised C-reactive S. aureus and beta-haemolytic strepto
protein. cocci. A swab is more likely to give useful usevere pain and tenderness, sometimes out of proportion
At the invasive disease end of the spec information when the patient has high to the appearance
trum, the most likely causative organ risk factors for MRSA, is failing antibiotic urapid spread of signs
isms are S. aureus and beta-haemolytic treatment or has frank pus draining. ublackish, haemorrhagic blisters, skin necrosis, a dusky
streptococci. In the middle of the spec When taking a swab for culture from colour, sometimes a sticky discharge, sometimes numbness
trum, heavy colonisation with gram-neg a chronic skin ulcer or wound, it is com ushock, confusion, respiratory dysfunction, acute kidney
ative bacteria (eg, Escherichia coli, Klebsiella monly recommended the infected site is injury, lactic acidosis and other signs of severe sepsis and
spp., Acinetobacter spp. or Pseudomonas aer- first cleaned by wiping or irrigating with multiorgan failure
uginosa) or anaerobes may contribute to sterile water or saline to clear away any
Table 2 Oral antibiotic choices for mild-to-moderately infected wounds1,2
Infection type Antibiotic choices
Infected post-traumatic wounds3 AMOXICILLIN+CLAVULANATE po 625mg tds
uMild penicillin allergy: cefalexin po 500mg qid and metronidazole po 600mg bd
uSevere penicillin allergy: ciprofloxacin po 500mg bd and clindamycin po 450mg tds
Infected penetrating injury through a shoe CIPROFLOXACIN po 500mg bd
Infected injury associated with exposure CIPROFLOXACIN po 500mg bd and CLINDAMYCIN po 450mg tds
to fresh or salt water
Infected bite or clenched-fist injury AMOXICILLIN+CLAVULANATE po 625mg tds
uPenicillin allergy: metronidazole po 600mg bd and either doxycycline po 100mg bd or trimethoprim+
sulfamethoxazole po 960mg bd
Surgical site infections – limb or upper body3 FLUCLOXACILLIN po 1000mg qid
uMild penicillin allergy: cefalexin po 500mg qid
uSevere penicillin allergy: clindamycin po 450mg tds
Surgical site infections – abdomen or pelvis3 AMOXICILLIN+CLAVULANATE po 625mg tds
uPenicillin allergy: trimethoprim+sulfamethoxazole po 960mg bd and metronidazole po 600mg bd
bd, twice daily; po, orally; qid, four times a day; tds, three times a day. 1. Based on guidelines written by the South Island Hospital Antimicrobial Guidelines
Group: New Zealand, 2016. 2. Duration of treatment is five to 10 days, depending on severity, drainage and response. 3. Cover MRSA if known to be recent-
ly MRSA-positive or failing beta-lactam therapy despite adequate surgical management. Oral antibiotic choices for MRSA include clindamycin, doxycycline,
trimethoprim+sulfamethoxazole or macrolides.
www.howtotreat.co.nz/infection HOW TO TREAT 9→WOUND INFECTION
Enteric gram-negative bacilli (like E. agents, is beyond the scope of this article. The strongest positive results are for ca
coli or Klebsiella spp.), Acinetobacter sp., P. If invasive infection is suspected, an dexomer iodine (at least 12 randomised
aeruginosa and anaerobes are less likely empiric systemic antibiotic agent such as comparative trials) and super-oxidizing
to be associated with invasive infection amoxicillin+clavulanate is likely to cov solutions (at least 13 comparative tri
but may contribute to patient symptoms er the usual pathogens (see Table 2 for als). Prontosan (polyhexanide plus be
and failure to heal. For example, only about common doses). If there is a mild penicil taine) improves healing (at least three
one in seven patients with P. aeruginosa lin allergy then use both a cephalospor comparative trials) and hydrogen perox
isolated on a wound swab has an inva in and metronidazole. If the patient has ide improves surrogate outcome measures
sive infection due to these bacteria that a severe penicillin allergy or any cepha (at least four randomised comparative
requires systemic antibiotic treatment. losporin allergy, use both ciprofloxacin trials) in chronic ulcers and wounds.
Common skin flora such as coagulase- and clindamycin. Subsequent antibiot Limited evidence indicates that sus
negative staphylococci, alpha-haemolytic ic choice can be guided by the results of tained-release silver dressings improve
streptococci and diphtheroids are usually culture, provided the sample was outcomes in chronic wounds.
harmless colonisers. correctly taken and the result is correctly In contrast, a Cochrane review in
interpreted (see above). 2014 (CD003557.pub5) reported no good
Managing infected or Topical antiseptic agents have been evidence of benefit with the use of pov
heavily colonised chronic shown to reduce the bacterial load on idone-iodine, chlorhexidine, mupirocin
ulcers and wounds and below the surface of chronic ulcers or honey in chronic ulcers or wounds. n
A key tactic in managing any chronic ul and wounds, and to improve clinical
cer or wound – whether it is infected or signs of infection. Although many stud
not – is to correct the underlying cause ies are of poor design and the results Practice point 6
of the failure to heal, such as arterial dis are somewhat conflicting, randomised Managing infected or heavily
ease, pressure, venous or lymphatic stasis, trials show, overall, that some topical colonised chronic ulcers
oedema, vasculitis or nutritional defic antiseptic agents improve chronic and wounds
iency. This often requires referral to a vas ulcer and wound healing. 1. Treat invasive infection
cular surgical clinic or wound-care nurse (eg, cellulitis) with systemic antibiotic
R GRECH
specialist in your region. agents (eg, amoxicillin+clavulanate,
A key tactic in managing
Another key tactic in managing a or cefalexin and metronidazole,
any chronic ulcer or
chronic ulcer or wound is to optimise the or ciprofloxacin and clindamycin).
wound is to address the
local healing environment – a topic that 2. Treat heavily colonised ulcers and
underlying cause
wound-care nurses are expert in. Healing wounds with topical antiseptic agents.
is likely to be enhanced by debriding ne a. Options include cadexomer
crotic, devitalised tissue and eschar, wash iodine paste, ointment or sheets;
ing away slough, correct moisture balance super-oxidizing wound care solution
and appropriate dressings. The choice of or hydrogel; and polyhexanide
dressing, other than the use of antiseptic (with betaine; Prontosan) liquid or gel.
Sustained-release silver dressings
and dilute bleach (in low-resource
Further situations; see Table 1 for dilutions)
may also be effective.
information 3. Cleanse and debride to remove
necrotic and non-viable tissue,
eschar and slough.
Reference 4. Treat reversible underlying
Arnold B, Chambers S, Everts R, causes of the chronic ulcer or wound
Gardiner S, Metcalf S, Ussher J on (eg, pressure, venous stasis).
behalf of the South Island Hospital
Antimicrobial Guidelines Group.
South Island Hospital Antimicrobial
Guidelines, 2016. Published by
Canterbury District Health Board.
Quiz answers
Estimated date of publishing: 1. False 2. False 3. True 4. True
March 2017
Conflict of interest statement This publication has been reprinted by the Accident Compensation Corporation to
Dr Everts receives no personal provide an update on the prevention and treatment of wound infection. The content
benefit such as payment or sponsor is entirely independent and based on published studies and the author’s opinion.
ship from any manufacturer or Accident Compensation Corporation,Treatment Injury Prevention Team,
distributor of antiseptic agents. Justice Centre, 19 Aitken Street, Wellington.
This article has been reprinted from New Zealand Doctor newspaper,
Acknowledgement
23 November 2016 and Pharmacy Today, February 2017. The views
Thanks to Melanie Terry and Sue
expressed are not necessarily those of the publisher or sponsor.
Rossiter (district nurses), Andrew
McGlashen (pharmacist) and David Produced by The Health Media, publisher of New Zealand Doctor
Dixon (GP) for their advice on the and Pharmacy Today, PO Box 31905, Milford, Auckland 0741.
manuscript for this article. Ph (09) 488 4286, Fax (09) 912 9257 © The Health Media (NZ) Ltd, 2016.
10 HOW TO TREAT www.howtotreat.co.nz/infectionGAIN CME
POINTS is
Take action to Complete th
online mod
ule
prevent infection
Wound infections are common but some practical steps can help reduce the incidence and severity.
Expand your knowledge of wound infections by completing our online learning module. It’s quick, accessible
from any device and contributes points to your professional development.
Start your online module now at www.howtotreat.co.nz/infection
NZDYou can also read