Infection Prevention and Control Carbapenemase Producing Enterobacteriaceae (CPE)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Infection Prevention and Control
Carbapenemase Producing
Enterobacteriaceae (CPE)
IPCT CPE Policy V4 May 2018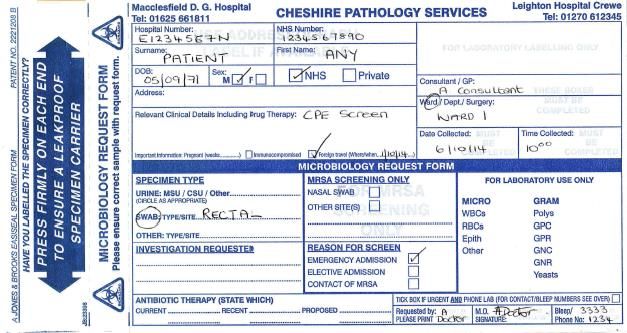
Policy Title:
Carbapenemase Producing Enterobacteriaceae (CPE)
Executive This policy details the micro-organisms capable of producing carbapenemase,
Summary: how they are identified, managed and spread within the hospital setting.
Supersedes: Carbapenemase Producing Enterobacteriaceae (CPE) V2 February 2016
Description of Updated to reflect National Guidelines
Amendment(s):
This policy will impact on: Clinical Staff
Financial Implications: Laboratory screening costs
Policy Area: Infection Prevention Document ECT002985
and Control Trust Wide Reference:
Version V4 Effective Date: July 2018
Number:
Issued By: Infection Prevention Review Date: May 2021
and Control
Author: Abigail Paterson Impact Assessment May 2018
Associate Specialist Date:
Practitioner Infection
Prevention and Control
APPROVAL RECORD
Committees / Group Date
Consultation: Infection Control Committee 19th July 2018
Approved by Director: Director of Infection Prevention & 19th July 2018
Control / Director of Nursing and
Quality
Ratified by: Infection Control Committee 19th July 2018
Received for Directorate SQS
information:
IPCT VRE Policy V4 July2018 Page 2
Table of Contents
44
1. Introduction 4
2. Purpose 4
3. Responsibilities 4
4. Processes and Procedures 5
5. 5. Monitoring Compliance with the Document 11
6. References 12
7. Communication
7. Appendices Page 11
Appendix 1 – CPE patient information leaflet Page 12
13
Appendix 2 – Screening for Carbapenemase producing 15
Enterobacteriaceae (CPE)
Appendix 3 – Carbapenemase producing 16
Enterobacteriaceae (CPE) pathway
Appendix 4 – Carbapenemase-producing 17
Enterobacteriaceae (CPE) screening flowchart
Appendix 5 – Carbapenemase-producing 18
Enterobacteriaceae (CPE) contact screening flowchart
Appendix 6 – Mattress Integrity check 19
IPCT VRE Policy V4 July2018 Page 3
1. Introduction Enterobacteriaceae such as Klebsiella spp and Escherichia coli, are a family of bacteria that live in the gut of humans and animals. They are opportunistic bacteria capable of causing a variety of infections including urinary tract, intra-abdominal and bloodstream infections (PHE, 2018). There are strains of Enterobacteriaceae that can produce Carbapenemase, an enzyme capable of destroying carbapenem antibiotics. Carbapenems are a valuable family of antibiotics normally reserved for serious infections caused by drug-resistant Gram-negative bacteria (including Enterobacteriaceae). They include meropenem, ertapenem, imipenem and doripenem. The presence of carbapenemase makes the Enterobacteriaceae resistant to multiple antimicrobials and therefore infections caused by CPE (Carbapenemase producing Enterobacteriaceae), limiting treatment options. Antibiotic resistance is a major public health concern highlighted by the Chief Medical Officers report (DH, 2011) where the incidence of CPE in the UK is discussed. Public Health England (PHE, 2013 & 2015) also issued guidance to acute Trusts & none acute settings to advise on the detection and management of CPE. This guidance has been used as an evidence base to develop this policy. Section 4.1 of this policy includes a table which identifies countries and UK regions with a high prevalence of CPE 2. Purpose This policy aims to promote awareness of CPE and enable early identification, screening and isolation of high risk patients; which are all essential steps in the control of drug resistant organisms (Damani, 2012). The guidance within promotes correct management of affected patients and aims to improve patient safety by limiting the spread of CPE locally, to contribute towards the global effort to minimise CPE transmission. 3. Responsibilities The Chief Executive has ultimate responsibility for the implementation and monitoring of the policies in use in the Trust. This responsibility may be delegated. The Director of Nursing, Performance and Quality/ Director of Infection Prevention and Control (DIPC) will take the lead responsibility for the development and implementation of this policy with support of the Head of Nursing Infection Prevention and Control and the Infection Prevention and Control Doctor. In addition as the DIPC they will oversee the implementation of the policy and challenge poor practice. Providing assurance to the board that systems and process are in place to ensure compliance with agreed standards. The Infection Prevention and Control Team (IPCT) will have responsibility for: -ensuring the CPE policy is implemented and monitored across the trust IPCT VRE Policy V4 July2018 Page 4

-ensuring the policy is updated to reflect any changes to the national or local guidelines
-providing education and support to clinical staff
-providing education and advice on the management of CPE patients within the organisation
-referring to the Consultant Microbiologist / Infection Control Doctor where appropriate.
All Employees are responsible for ensuring standards of Infection Prevention and Control
are maintained in line with trust policies and procedures. Infection Prevention and Control
training and standards will be monitored via the appraisal process
Matrons / Ward Senior Sister / Departmental Managers are responsible for ensuring
that all staff:
-are aware of, and adhere to, this policy
-are aware of their roles and responsibilities with regard to reducing healthcare associated
infections (HCAIs)
-are aware of patients considered high risk for CPE colonisation / infection
-carry out CPE screens for high risk patients as specified in this policy
-isolate all suspected / confirmed CPE patients promptly
-demonstrate appropriate and effective infection control practices
-alert the Infection Prevention and Control Team of suspected / confirmed CPE patients
-inform the patient of their CPE status
-communicate patient’s status on discharge / transfer to receiving organisations (as
appropriate).
4. Processes and Procedures
1. What are Carbapenemase producing Enterobacteriaceae?
Enterobacteriaceae are a large family of Gram negative bacteria that usually live
harmlessly in the guts of humans and animals, as per the images below.
Species include:
Escherichia coli
Klebsiella spp
Enterobacter spp
Carbapenemases are enzymes made by some strains of the bacteria which allow them to
destroy carbapenem antibiotics and so the bacteria are said to be resistant to these
antibiotics
IPCT VRE Policy V4 July2018 Page 5In the UK in there has been an increase in incidence of infection and colonisation of
multidrug resistant carbapenemase producing organisms. UK regions / areas where
problems have been noted include:
London
North West- particularly Manchester
Countries and regions with a high prevalence of CPE are documented in the following table.
Bangladesh North Africa
The Balkans Malta
China Middle East
Cyprus Pakistan
Greece South East Asia
India South / Central America
Ireland Turkey
Israel Taiwan
Italy USA
Japan
2. Which patients are at a high risk of CPE and requiring screening?
All high risk / suspected CPE positive patients must be CPE screened. They must be
admitted into an isolation room, preferably with en-suite facilities.
Admission to augmented Admission to general Patient screen required /
care ITU, CCU, Neonatal wards: isolation required
unit:
A known or recently A known or recently Repeat screen not required
laboratory confirmed CPE laboratory confirmed CPE isolation required
case (these patients will not case (these patients will not
need rescreening but will need rescreening but will
need isolating) need isolating)
A direct patient transfer from A direct patient transfer from CPE Screen Required
any UK hospital any UK hospital isolation required
A direct patient transfer from A direct patient transfer from CPE Screen Required
any hospital abroad any hospital abroad isolation required
A medical tourist from a A medical tourist from a CPE Screen Required
hospital abroad hospital abroad isolation required
A patient that has a history of A known or recently CPE Screen Required
hospitalisation in the last 12 laboratory confirmed CPE isolation required
months in the UK or abroad case (these patients will not
need rescreening but will
need isolating)
A close contact of a known CPE Screen Required-
CPE positive case e.g. living discuss with infection control
in the same house, sharing a isolation required
sleeping place i.e. room or
hospital bay
3. What is the difference between colonisation and infection?
Colonisation Infection
The presence of Carbapenemase-producing Carbapenemase-producing
IPCT VRE Policy V4 July2018 Page 6Colonisation Infection
Enterobacteriaceae (CPE) living harmlessly Enterobacteriaceae (CPE) can cause serious
on the skin or within the human infections, including urinary tract infections,
gastrointestinal tract and causing no signs or intra-abdominal infections, blood stream
symptoms of infection. A carrier is colonised infections (bacteremia) and hospital-acquired
with Carbapenemase-producing pneumonias. Patients with infections caused
Enterobacteriaceae (CPE). by Carbapenemase-producing
Enterobacteriaceae (CPE) require treatment.
4. How is CPE transmitted?
Carbapenemase-producing Enterobacteriaceae (CPE) can be spread person to person by
faecal contamination of the hands, transferred from an environmental source or
contaminated equipment.
5. What is the screening process for CPE?
Following identification of a high risk / suspected CPE positive patient they must be CPE
screened.
Informed consent must be gained from the patient wherever possible. If a patient
declines the screen, document this in the patients’ medical notes and consider taking a
stool specimen. Document on the pathology form why a stool sample has to be sent
CPE information must be given to the patient or relatives (see Appendix 1 )
Gloves and aprons must be worn when obtaining the CPE screen
A rectal swab must be obtained using a dry transwab. The cotton tip of the transwab
should be inserted just inside the rectum gently and rotated to come into contact with
faeces (see Appendix 2 for screening advice).
Additional swabs must be taken from any wounds (surgical wounds, ulcers, lesions) or
device related sites (cannula, tracheostomy, PEG, drains or lines)
Send swabs to the laboratory labelled for CPE testing – include any relevant clinical
details.
A stool sample will be accepted if a rectal swab is deemed inappropriate e.g., patients
with a stoma, paediatrics. Please label the stool sample for CPE testing and provide
details of why a stool sample has been sent instead of a rectal swab.
Screens must be taken on day 0 e.g. day of admission, day 2 (48 hours after the 1st
screen) and day 4 (48 hours after the 2nd screen). If any of the screens return CPE
positive, cease screening. See Appendix 4.
Follow and complete the “CPE Care Pathway” using Appendix 3.
6. What actions do I take if the screens return negative?
If all three CPE screens return as negative, the patient can be moved out of isolation (unless
there is another reason for isolation) and classed as CPE negative.
7. What actions do I take if the screen returns positive?
Advise the patient (and relatives if appropriate) of the positive result and provide a patient
information leaflet and Public Health England CPE card, if not already done so. Establish if
the patient has an infection or is colonised.
Isolate in a side room (preferably en- Isolation sign placed on outside of isolation
suite) room door
The door to the room must be kept closed. If
this is not possible, document the reason
why in the patients notes.
The patient must remain in isolation for
IPCT VRE Policy V4 July2018 Page 7the duration of their hospital stay.
Hand decontamination Hands must be decontaminated after contact
with the patient, equipment and before
leaving the room. Follow the WHO ‘5
moments for hand hygiene’.
Hand sanitiser or liquid soap and water can
be used.
Encourage patients to clean their hands
before meals and after using the toilet /
commode.
Visitors must be advised regarding hand
hygiene
PPE Aprons and gloves must be worn for clinical
care and when in contact with the patients
environment e.g. when changing bed linen.
Yellow aprons must be worn.
Decontaminate hands after removing PPE
with liquid soap and water.
Visitors are not required to wear PPE unless
they are participating in personal care,
however must comply with hand hygiene
Mask / eye protection Not required unless CPE is isolated in a
patient’s sputum. In these circumstances a
surgical facemask must be worn for aerosol
generating procedures only such as:
intubation, invasive suction, deep chest
physiotherapy
Linen Linen must be changed daily and disposed
of in a red alginate bag and then into a white
linen bag.
Used linen must be disposed of promptly.
Linen bags must not be placed on the floor
of the isolation room- this reduces the
potential for further environmental
contamination.
Toilet facilities Where possible admit patients with CPE into
an en-suite room.
If this is not possible a dedicated commode
must be provided and cleaned after each
use using a sporicidal agent e.g. clinell
sporicidal wipes (red packet).
If a patient is required to use the bathroom
on the ward, try to dedicate this bathroom for
their use only. If the bathroom cannot be
dedicated, the bathroom requires cleaning
after each use using Tristel.
The bathroom must be cleaned twice daily.
Equipment If possible, equipment must be dedicated for
IPCT VRE Policy V4 July2018 Page 8the patient. If this is not possible, any shared
equipment must be decontaminated after
use using a sporicidal product e.g. Tristel
before leaving the isolation room.
Waste Disposal Clinical waste to be placed into an orange
bag.
Crockery and cutlery Patients can use crockery and cutlery from
the main kitchen, no special precautions
required.
Documentation An alert must be placed electronically on
Extramed by ward staff or IPCT
An alert sticker must be placed on the
patient’s notes and the alert card at the front
of the notes completed.
Monitor patient bowel habit on a stool chart.
Ensure patient has an information leaflet and
Public Health England CPE card.
The ward is responsible for informing the
patients GP of their CPE status.
Gut decolonisation is not recommended as there is a concern this may contribute to longer
term resistance. Skin decolonisation is not recommended as the bacteria generally colonise
the gut rather than the skin. No antibiotic treatment is required for CPE colonisation.
If a patient is to be transferred to another hospital or care home, the receiving
organisation must be notified of the patient’s CPE status prior to transfer by the
transferring clinical area / department.
8. Do contacts require screening?
If a patient returns positive for CPE and has spent 24 hours or more in a main hospital bay,
the patients contacts in the bay must be CPE screened.
Contacts must be screened weekly for a total for 4 weeks (whilst an inpatient). See
appendix 5.
Contacts only need to be screened whilst they remain an inpatient.
Only begin contact screening once the positive index case has been isolated / left the
bay.
Cohort the contact patients together and close the bay to admissions.
The contact bay must remain closed until all CPE screen results have returned or
until the contact patients have been isolated. The decision to reopen the bay must be
discussed with IPCT / out of hours Consultant Microbiologist.
The IPCT can provide guidance on contact tracing and screening.
The above precautions must be followed for contact patients.
Screening of household contacts and healthcare staff is NOT required.
IPCT VRE Policy V4 July2018 Page 99. Are there any restrictions on visitors?
There are no restrictions placed on visitors. However, if the patient gives consent to discuss
their diagnosis with family / carers / visitors, advise immunocompromised patients to avoid
visiting if appropriate.
All visitors must be advised to practice scrupulous hand hygiene with liquid soap and water
prior to leaving the room.
Advise visitors undertaking multiple hospital visits to visit the affected patient last. Visitors /
care takers taking part in care activities must be provided with PPE, shown how to apply and
remove it and the correct waste streams to dispose PPE into.
10. What actions must be taken for the transfer of patients within the hospital/ access to
services?
Transfer to a different ward within the Patients with CPE must only be moved to a
trust different ward if there is a clinical need for a
different speciality.
This may be reviewed by the bed management team
and IPCT if the trust is experiencing organisational
pressures and ward moves are required to facilitate
patient flow through the organisation.
Access to services e.g. therapy, theatre, Treatments and procedures must not be
radiology delayed however, where possible, planned at
the end of the day / list (without
compromising clinical treatment).
Multi-disciplinary team members MDT members should visit patients last on
requiring access to a patient with their list wherever possible.
confirmed / suspected / contact of CPE Access to communal areas is acceptable
unless the patient is symptomatic of infection
or has diarrhoea.
Hospital porters Porters are not required to wear PPE when
transferring patients within the trust.
Portering staff must practice good hand
hygiene after transferring a patient.
11. What actions should be taken on discharge?
Type of clean Post Infection Clean
Steam and Tristel
Curtain change
Including dedicated bathroom if appropriate
Disposable equipment All disposable equipment to be disposed of
including unused dressings, ointments,
tapes, wipes etc.
Clinical equipment To be cleaned with sporicidal agent e.g.
Tristel by clinical staff.
Mattress and pillows Pillows must be disposed of
The mattress must be assessed as safe to
re-use (see appendix 6)
Hired mattresses must be returned to the
company for cleaning and decontamination
IPCT VRE Policy V4 July2018 Page 10Please note: There is no reason for non-acute settings to refuse admission or
readmission of service users on the grounds they are colonised with CPE (PHE,
2015).
Patients can return to their own home without any special measures.
If a patient is being discharged to another healthcare facility / community services the
clinical area caring for the patient is responsible for informing the receiving organisation of
the patient’s CPE status prior to transfer, to allow them time to organise appropriate
facilities.
Ambulance staff must be informed of the patient’s CPE status to enable them to make
appropriate preparations. CPE positive patients should undergo a risk assessment in
order to determine the requirement for a separate ambulance.
12. What actions are required for community care?
While the level of risk for infected or colonised individuals is lower than that in acute
settings, if the levels of hygiene in the care setting are inadequate, resistant bacteria may
spread amongst individuals who congregate together e.g. in a care home. This may
increase the risk of the spread of infection within the care setting (PHE, 2015).
Healthcare staff must maintain strict IPC standard precautions e.g. hand hygiene to
prevent spread within the persons home or to other clientele on their case list.
Where possible CPE positive patients should be seen at the end of the list / day.
Patients should not be prevented from attending communal rehabilitation sessions.
If a patient is diagnosed CPE positive during an inpatient stay at a healthcare
organisation other than East Cheshire NHS Trust , please inform the IPC team on 01625
661597. This will enable alerts to be placed in the patient’s medical records and
preparations to occur to facilitate their potential admission at a point in the future.
13. What actions are required on the patient’s death?
Precautions taken when performing last offices for the deceased person are the same as
in life. This use of “Danger of infection” stickers and body bags are unnecessary.
Mortuary and undertaking staff should abide to standard infection control precautions as
appropriate for their role.
5. Monitoring Compliance with the Document
The infection prevention and control team will review and investigate incidents reported
relating to this policy.
IPCT VRE Policy V4 July2018 Page 116. References Legislation, Guidance and References Damani N (2012) - Manual of Infection Prevention and Control, 3rd Edition. Oxford: Oxford University Press Chief Medical Officer (2011) - Annual Report of the Chief Medical Officer Infections and the rise of antimicrobial resistance Vol 2. DH: London. Available at: http://media.dh.gov.uk/network/357/files/2013/03/CMO-Annual-Report-Volume-2-20111.pdf Last accessed 16.05.2018 Public Health England (2013) - Acute Trust toolkit for the early detection, management and control of carbapenemase-producing Enterobacteria. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/329227/Acute _trust_toolkit_for_the_early_detection.pdf . Last accessed 16.05.018 Public Health England (2015) - Toolkit for managing carbapenemase-producing Enterobacteria in none acute and community settings. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/439801/CPE- Non-AcuteToolkit_CORE.pdf Last accessed 16.05.2018 IPCT VRE Policy V4 July2018 Page 12
Appendix 1 CPE Patient Information Leaflet What are Carbapenemase-producing Enterobacteriaceae? Enterobacteriaceae are bacteria that usually live harmlessly in the gut of humans. This is called ‘colonisation’ (a person is said to be a ‘carrier’). However, if the bacteria get into the wrong place, such as the bladder or bloodstream they can cause infection. Carbapenems are one of the most powerful types of antibiotics. Carbapenemases are enzymes (chemicals), made by some strains of these bacteria, which allow them to destroy carbapenem antibiotics and so the bacteria are said to be resistant to the antibiotics. Why does carbapenem resistance matter? Carbapenem antibiotics can only be given in hospital directly into the bloodstream. Until now, doctors have relied on them to successfully treat certain ‘difficult’ infections when other antibiotics have failed to do so. In a hospital, where there are many vulnerable patients, spread of resistant bacteria can cause problems. Does carriage of carbapenemase-producing Enterobacteriaceae need to be treated? If a person is a carrier of carbapenemase-producing Enterobacteriaceae (sometimes called CPE), they do not need to be treated. However, if the bacteria have caused an infection then antibiotics will be required. How do people ‘pick up’ carbapenemase-producing Enterobacteriaceae? Do ask your doctor or nurse to explain this to you in more detail. As mentioned above, sometimes this bacteria can be found, living harmlessly, in the gut of humans and so it can be difficult to say when or where it is picked up. However, there is an increased chance of picking up these bacteria if you have been a patient in a hospital abroad or in a UK hospital that has had patients carrying the bacteria, or if you have been in contact with a carrier elsewhere. How will I be cared for whilst in hospital if I am found to be positive? You will be accommodated in a single room with toilet facilities whilst in hospital. You may be asked to provide a number of samples, depending on your length of stay, to check if you are still carrying the bacteria. These will probably be taken on a weekly basis. The samples might include a number of swabs from certain areas, such as where the tube for your drip (if you have one) enters the skin, a rectal swab i.e. a sample taken by inserting a swab briefly just inside your rectum (bottom), and / or a faecal sample. You will normally be informed of the results within two to three days. How can the spread of carbapenemase-producing Enterobacteriaceae be prevented? By accommodating people in a single room this helps to prevent the spread of the bacteria. Healthcare workers will wash their hands regularly. They will use gloves and aprons when caring for you. The most important measure for people to take is to wash hands well with soap and water, especially after going to the toilet. Avoid touching medical devices (if you have any) such as a urinary catheter tube and intravenous drip, particularly at the point where it is inserted into the body or skin. Visitors will be asked to wash their hands on entering and leaving the room and may be asked to wear an apron. What about when I go home? Whilst there is a chance that you may still be a carrier when you go home quite often this will go away with time. No special measures or treatment are required; any infection will have been treated prior to your discharge. You should carry on as normal, maintaining good hand hygiene. If you have any concerns you may wish to contact your GP for advice. IPCT VRE Policy V4 July2018 Page 13
Before you leave hospital, ask the doctor or nurse to give you a letter or card advising that you have had an infection or been / are colonised with carbapenemase-producing Enterobacteriaceae. This will be useful for the future and it is important that you make health care staff aware of it. Should you or a member of your household be admitted to hospital, you should let the hospital staff know that you are, or have been a carrier and show them the letter / card. Where can I find more information? If you would like any further information please speak to a member of your care staff, who may also contact the Infection Prevention and Control Team for you. Websites are another source of information: Public Health England http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/CarbapenemResistance/ NHS Choices http://www.nhs.uk/news/2014/03March/Pages/Antibiotic-resistance-toolkit-launched.aspx Useful contact: East Cheshire NHS Trust Infection Prevention and Control team 01625 661597 IPCT VRE Policy V4 July2018 Page 14
Appendix 2 – Screening for Carbapenemase-producing Enterobacteriaceae (CPE)
Rectal specimens to be taken on day 0, 2 & 4 (3 swabs over 5 days), additional swabs to
include wounds or devices. If any screens return CPE positive, cease swabbing
Specimen type:
Rectal screen (preferred sample type)
Stool sample (if patient declines or is unable to provide a rectal screen). Document on
pathology card reason for stool specimen.
TRANSWAB charcoal swab
Performing a rectal screen:
Explain the procedure to the patient to gain their
consent. Ensure the patient’s privacy & dignity while
performing the procedure
Decontaminate hands using liquid soap and water.
Confirm patient details on the pathology request card
with the patient, or against patient’s ID band.
Put on non-sterile examination gloves and plastic
apron to collect specimen.
Insert the dry charcoal swab into the rectum
approximately 2.5 cm (for adults) beyond the anal sphincter
and very gently rotate to obtain faecal flora.
Ensure that the tip of the swab is well covered in
faecal material.
Remove apron and gloves.
Decontaminate hands using liquid soap and water.
Dispose of PPE / equipment into appropriate waste
stream
Label specimens correctly and organise transport to
laboratory.
Complete pathology request form:
A minimum of 3 patient identifiers must be
evident on the pathology form e.g. patient’s
name, Hosp. No, NHS No, DOB etc.
Document rationale for CPE request e.g.
CPE screen, CPE contact screen
Rectum
IPCT VRE Policy V4 July2018 Page 15Appendix 3 –
Carbapenemase Producing Enterobacteriaceae
CPE Care Pathway
If a patient admitted to any augmented care area or meets any of the below criteria please
isolate and screen the patient for CPE.
Criteria Tick Date
Is the patient a known or recently laboratory confirmed CPE case (these
patients will not need re screening but will need isolating with full Infection
Control precautions)
Is the patient a direct transfer from a UK hospital?
Is the patient a direct transfer from a hospital abroad?
Has the patient been a medical tourist abroad in the last 12 months?
Does the patient have a history of hospitalisation in any care setting in a
UK hospital in the last 12 months?
Does the patient have a history of an augmented care admission in the last
12 months abroad?
Has the patient been identified as a contact of a CPE positive case?
Infection Control Precaution Checklist during screening Initial Date
Has the patient / relative / carer been given a CPE leaflet?
Has the patient been isolated with the door closed if safe to do so?
Have dedicated toilet facilities been arranged for the patient if applicable?
Has the patient been placed on a stool chart?
Has advice been given to patient /carer / visitors regarding hand hygiene?
Is PPE accessible outside the isolation room?
Is the isolation room clutter free?
Are the patient’s notes and charts being kept outside of the isolation room?
Infection Control Precaution Checklist following positive result Initial Date
Has the patient / relative / carer been given a CPE card?
Has Infection Control signage been placed on the isolation room door?
Has a twice daily “Infection Clean” of the room been requested from the
Trust cleaning provider (Ext 1999)
Is the nursing equipment being cleaned twice daily by ward staff using a
sporicidal agent e.g. Tristel / chlorine releasing agent?
Has an alert sticker been placed on the medical notes and annotated CPE
Has an electronic alert been placed on CRIS
Please complete screening flowchart on the following page
IPCT VRE Policy V4 July2018 Page 16Appendix 4
Patient Identifier Label
CPE SCREENING FLOWCHART
Date of 1st CPE screen Sites screened Results
If any of the screening results return positive the If the 1st CPE screen is negative
patient will need to be isolated throughout their please repeat the screen 48
entire admission. hours after the first:
Please discuss results with medics to determine
whether the patient is colonised or has an
infection. If an infection is suspected please
discuss treatment with Consultant Microbiologist
Date of 2nd CPE screen Sites screened Results
If any of the screening results return positive the
patient will need to be isolated throughout their If the 2nd CPE screen is negative
entire admission. please repeat the screen 48
Please discuss results with medics to determine hours after the first:
whether the patient is colonised or has an
infection. If an infection is suspected please
discuss treatment with Consultant Microbiologist
Date of 3rd CPE screen Sites screened Results
If any of the screening results return positive the
patient will need to be isolated throughout their If all 3 CPE screens are negative
entire admission. patient can be classed as CPE
Please discuss results with medics to determine Negative and removed from
whether the patient is colonised or has an isolation
infection. If an infection is suspected please
discuss treatment with Consultant Microbiologist
IPCT VRE Policy V4 July2018 Page 17Patient Identifier label
Appendix 5 Carbapenemase-producing Enterobacteriaceae (CPE) Contact Screening flowchart
Date of 1st CPE screen Sites screened Results
If any of the screen results positive the patient will If the 1st CPE screen is negative
need to be isolated throughout their entire admission. please repeat the screen 1 week
Please discuss results with medics to determine after the first
whether the patient is colonised or has an infection. If
an infection is suspected please discuss treatment with
Consultant Microbiologist
Date of 2nd CPE screen Sites screened Results
If any of the screen results positive the patient will
need to be isolated throughout their entire admission. If the 2nd CPE screen is
Please discuss results with medics to determine negative please repeat the
whether the patient is colonised or has an infection. If screen 1 week after the
an infection is suspected please discuss treatment with second
Consultant Microbiologist
Date of 3rd CPE screen Sites screened Results
If any of the screen results positive the patient will
need to be isolated throughout their entire admission.
Please discuss results with medics to determine If the 3rd CPE screen is
whether the patient is colonised or has an infection. If negative please repeat the
an infection is suspected please discuss treatment with screen 1 week after the third
Consultant Microbiologist
Date of 4th CPE screen Sites screened Results
If any of the screen results positive the patient will
If the 4th CPE screen is
need to be isolated throughout their entire admission.
negative patient can be
Please discuss results with medics to determine
classed as CPE negative
whether the patient is colonised or has an infection. If
and requires no further
an infection is suspected please discuss treatment with
screening
Consultant Microbiologist
IPCT VRE Policy V4 July2018 Page 18Appendix 6 –
Mattress integrity check - Water penetration test instructions
1. Wear appropriate PPE (gloves and aprons)
2. Inspect the mattress for any visible signs of damage to mattress integrity, if noted
inform the nurse in charge as a replacement mattress must be sought and the
damaged mattress disposed of.
3. Unzip the mattress and inspect inner mattress for signs of soiling. If there are any
stains / decolouration to the underside of the cover remove the mattress from
circulation and inform nurse in charge so that a replacement mattress can be sought
and the damaged mattress disposed of.
4. If soiling not evident, proceed with water leak test:
Place a sheet of absorbent tissue between the top surface of the mattress and
the cover in the area where the patients “bottom” would normally be.
Re-Zip the mattress cover
Using the fist, indent the mattress over the area where the tissue is located to
form a shallow well and pour approximately 30 mls of tap water into the well.
Agitate the area with the fist for one to two minutes
Mop up the water with disposable paper towels and discard as domestic waste.
Undo zip and inspect tissue for water spots.
If the absorbent tissue is wet, then the integrity of the mattress has been
breached and the mattress must be replaced.
If no water is evident the mattress can be used by further patients
The mattress should be removed from use and the mattress cover replaced if it is
found to fail the above test or if it is visibly damaged.
IPCT VRE Policy V4 July2018 Page 19You can also read

















































