Itching for Answers Etiology of pruritus and the approach to the work up of the itchy patient - Massachusetts General Hospital ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Itching for Answers
Etiology of pruritus and the approach to
the work up of the itchy patient
Sarina B. Elmariah, MD, PhD
Director, MGH Itch and
Neurocutaneous Disorders Clinic
Massachusetts General Hospital
Harvard Medical School
www.mghcme.org
Disclosures
I have the following relevant financial relationship
with a commercial interest to disclose:
• Sanofi/Regeneron
• RAPT Therapeutics
• Menlo Therapeutics
• Trevi Therapeutics
www.mghcme.org
PART I: PRURITUS & EPIDEMIOLOGY
www.mghcme.org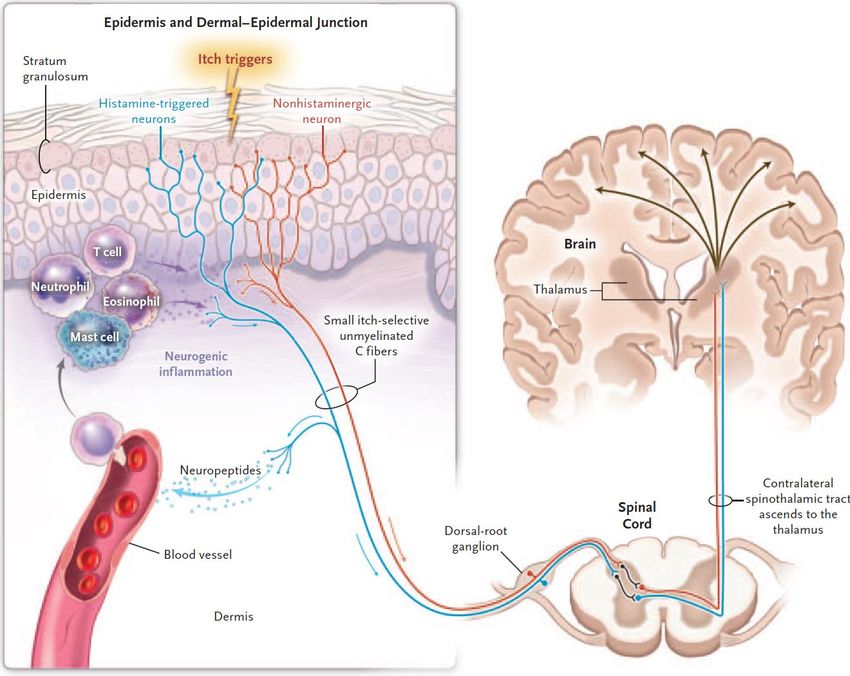
Itch
• Pruritus is defined as “an unpleasant sensation that
elicits the desire to scratch.” Samuel Hafenreffer, 1660
• Dysesthesia is an unpleasant, abnormal sensation that
may manifest as burning, prickling, tingling, stinging or
crawling.
• ACUTE itch < 6 weeks and CHRONIC itch > 6 weeks
• Not just one disease – there are countless causes!
www.mghcme.org
Itch Epidemiology
• Chronic itch has been estimated to affect 15-25% of the global
population
– A cross-sectional study (n = 11,730) found ~16% German workers had
chronic itch.
– A cross-sectional study (n = ~19,000 adults) found 8% of the Norwegian
general population had chronic itch.
• Higher in specific populations such as advanced age elderly, ESRD, ESLD,
HIV, inflammatory skin disease patients, where prevalence may reach
up to ~40%
• Women and men experience itch differently
– Women are more likely than men to experience stinging, warmth, or pain
with itch.
– Men are more likely to experience itch due to a primary rash or systemic
disease than women.
Stander S et al, Dermatology. 2010;221(3):229.
Dalgard F et al, J Investig Dermatol Symp Proc. 2004;9(2):120
Stander S et al., Br J Dermatol. 2013 Jun;168(6):1273-80
www.mghcme.org
Is itch really that bad?
• Chronic itch is associated with reduced quality
of life.
– Depression/anxiety
– Loss of sleep
– Loss of work productivity and economic hardship
– Impaired sexual function
– Social isolation and deterioration of interpersonal
relationships
Lavery MJ et al, Acta Derm Venereol 2017; 97: 513–515.
www.mghcme.org
14.1% 5.7%
21.4% 12.3%
15.7% 18.8% 7.6%
9.1%
33.0% 24.9%
Dalgard FJ et al, JID 2020; 140: 568–573.
www.mghcme.org
PART II: ETIOLOGY AND
CLASSIFICATION OF PRURITUS
www.mghcme.org
Basic itch pathway
Yosipovitch and Bernhard, NEJM. 2013 Apr 25; 368 (17):1625.
www.mghcme.org
Two-tier Itch Classification System
Unknown diagnosis Known diagnosis
(Anatomic classification)
• Group I: Itch on
inflamed skin • Dermatologic
• Group II: Itch on • Systemic
uninflamed skin • Neurologic
• Group III: Itch with • Psychogenic
severe, chronic
secondary scratch • Mixed
lesions
International Study for the Forum for Itch
Stander S et al, Acta Derm Venereol. 2007;87(4):291
Twycross et al., Q J Med 2003; 96: 7.
www.mghcme.orgItch DDx
Cutaneous/pruritoceptive Neuropathic/neurogenic Systemic
• Inflammatory dz • BRP • Renal
• AD • Notalgia/meralgia • CKD stage IV
• Psoriasis paresthetica • RCC
• Lichen planus
• Postherpetic Itch • Liver
• CTCL
• Xerosis • Multiple sclerosis/GBS • PBC/PSC
• Allergic or irritant contact • Post-viral syndromes • Cholestasis
dermatitis • Spinal trauma/disc • Hep C Cirrhosis
• Pityriasis rosea herniation • Cholestasis of Pregnancy
• PRP • CVA • Hematopoietic/PNP
• Bullous pemphigoid
• Small Fiber Neuropathy • Polycythemia vera
• Linear IgA
• Dermatitis Herpetiformis • Drugs (e.g. opiates) • Essential thrombocytosis
• Urticaria, mast cell activation • Iron-deficiency anemia
• Polymorphous light eruption Psychogenic • Systemic mastocytosis
• Infectious • Delusions of parasitosis • Vit B12 deficiency
• Fungal: Dermatophyte/candida • Skin picking • Lymphoma/Leukemia
• Infestation: Scabies, pediculosis • Depression/Anxiety • Multiple myeloma
• Parasites: Onchocerciasis +
• Eating disorders with rapid weight • Solid tumors
parasites
• Viral : HIV, HSV, VZV, Hep C loss • Metabolic/Endocrine
• Syphilis • Hyper/hypothyroidism
• Autoimmune dz Genetic • Hyperparathyroidism
• Dermatomyositis • Ichthyoses (Netherton, • Carcinoid
• Sjogren’s Sjogren-Larsson, etc) • Diabetes, pre-diabetes
• Scleroderma • Porphyrias (PCT, EPP) • Wilson’s
• SLE • Large congenital nevi • Progesterone dermatitis
• Graft versus Host disease
• Allergy
• Neoplastic Other • Mast cell activation
• Mycoses Fungoides • Drugs/medications syndrome
• Non-melanoma skin cancer • Pregnancy, progesterone
www.mghcme.orgPART III: DIAGNOSTIC APPROACH
FOR ITCHY PATIENTS
www.mghcme.orgThe Purpose of Diagnosis
• To identify the primary cause of itch and
design an effective treatment plan for
the patient.
• To identify important co-morbidities that
could impact overall patient well-being.
www.mghcme.orgApproach to Diagnosis
• History
• Physical examination
• Review of systems
• Trial of treatment
• Diagnostic testing - when to order labs,
imaging or refer
www.mghcme.orgKey elements of history
• Skin changes
– Do you see a rash before the itch, or do you see skin changes only after
you scratch?
• Distribution
– Localized vs generalized
– Special sites: scalp, eyelids, groin, acral sites
• New exposures/environments
– New medications or change in formulations of pre-existing medications?
– New pets?
– Recent move or travel?
– Renovations or water damage?
• Triggers/alleviators
– Water (cold, hot)?
• Co-morbid disease
– Diabetes, thyroid disorders, malignancy, liver or renal disease,
psychiatric disease?
www.mghcme.orgKey elements of examination:
PRIMARY OR SECONDARY??
Primary Secondary
• Diffuse or non-geometric • Localized or widespread,
patterns of erythema but limited to areas
• Pink-red or violaceous
• Includes areas where patient patient can reach
cannot reach
• Linear or geometric
• Papules/plaques,
vesicles/bullae, non- • Excoriations, erosions
linear erosions • Hyperpigmentation or
• Induration or edema lichenification
• Scale
www.mghcme.orgItch DDx
Cutaneous/pruritoceptive Neuropathic/neurogenic Systemic
• Inflammatory dz • BRP • Renal
• AD • Notalgia/meralgia • CKD stage IV
• Psoriasis paresthetica • RCC
• Lichen planus
• Postherpetic Itch • Liver
• CTCL
• Xerosis • Multiple sclerosis/GBS • PBC/PSC
• Allergic or irritant contact • Post-viral syndromes • Cholestasis
dermatitis • Spinal trauma/disc • Hep C Cirrhosis
• Pityriasis rosea herniation • Cholestasis of Pregnancy
• PRP • CVA • Hematopoietic/PNP
• Bullous pemphigoid
• Small Fiber Neuropathy • Polycythemia vera
• Linear IgA
• Dermatitis Herpetiformis • Drugs (e.g. opiates) • Essential thrombocytosis
• Urticaria, mast cell activation • Iron-deficiency anemia
• Polymorphous light eruption Psychogenic • Systemic mastocytosis
• Infectious • Delusions of parasitosis • Vit B12 deficiency
• Fungal: Dermatophyte/candida • Skin picking • Lymphoma/Leukemia
• Infestation: Scabies, pediculosis • Depression/Anxiety • Multiple myeloma
• Parasites: Onchocerciasis +
• Eating disorders with rapid weight • Solid tumors
parasites
• Viral : HIV, HSV, VZV, Hep C loss • Metabolic/Endocrine
• Syphilis • Hyper/hypothyroidism
• Autoimmune dz Genetic • Hyperparathyroidism
• Dermatomyositis • Ichthyoses (Netherton, • Carcinoid
• Sjogren’s Sjogren-Larsson, etc) • Diabetes, pre-diabetes
• Scleroderma • Porphyrias (PCT, EPP) • Wilson’s
• SLE • Large congenital nevi • Progesterone dermatitis
• Graft versus Host disease
• Allergy
• Neoplastic Other • Mast cell activation
• Mycoses Fungoides • Drugs/medications syndrome
• Non-melanoma skin cancer • Pregnancy, progesterone
www.mghcme.orgPrimary skin changes
Exfoliative scale Thick adherent scale
xerosis or eczematous process psoriasis
Images from UpToDate or
DermNetNZ.org
www.mghcme.orgPrimary skin changes
Papules, vesicles Patches, fissures, crust
eczematous dermatitis (atopic)
Image from DermNetNZ.org
www.mghcme.orgPrimary skin changes
Vesicles, crust Tense bullae, erosions
bullous tinea bullous pemphigoid
Image from VisualDx & UpToDate
www.mghcme.orgPrimary + Secondary skin changes
Eczematous
plaques +
lichenification
eczematous dermatitis (atopic)
Image from UpToDate
www.mghcme.orgPrimary skin changes
Papules, vesicles Burrows
scabies
Images from DermNetNz.org
www.mghcme.orgSecondary skin changes
Excoriated
nodules without
surrounding
erythema
Prurigo nodularis
Image from VisualDx and UpToDate
www.mghcme.orgSecondary skin changes
Hyperpigmented
nodules and
linear plaques
without
surrounding
erythema
Uremic pruritus
Image from DermNetNz.org
www.mghcme.orgSecondary skin changes
Geometric,
lichenified
plaque
without
surrounding
erythema
Lichen simplex chronicus Image from VisualDx & UpToDate
www.mghcme.orgItch DDx
Cutaneous/pruritoceptive Neuropathic/neurogenic Systemic
• Inflammatory dz • BRP • Renal
• AD • Notalgia/meralgia • CKD stage IV
• Psoriasis paresthetica • RCC
• Lichen planus
• Postherpetic Itch • Liver
• CTCL
• Xerosis • Multiple sclerosis/GBS • PBC/PSC
• Allergic or irritant contact • Post-viral syndromes • Cholestasis
dermatitis • Spinal trauma/disc • Hep C Cirrhosis
• Pityriasis rosea herniation • Cholestasis of Pregnancy
• PRP • CVA • Hematopoietic/PNP
• Bullous pemphigoid
• Small Fiber Neuropathy • Polycythemia vera
• Linear IgA
• Dermatitis Herpetiformis • Drugs (e.g. opiates) • Essential thrombocytosis
• Urticaria, mast cell activation • Iron-deficiency anemia
• Polymorphous light eruption Psychogenic • Systemic mastocytosis
• Infectious • Delusions of parasitosis • Vit B12 deficiency
• Fungal: Dermatophyte/candida • Skin picking • Lymphoma/Leukemia
• Infestation: Scabies, pediculosis • Depression/Anxiety • Multiple myeloma
• Parasites: Onchocerciasis +
• Eating disorders with rapid weight • Solid tumors
parasites
• Viral : HIV, HSV, VZV, Hep C loss • Metabolic/Endocrine
• Syphilis • Hyper/hypothyroidism
• Autoimmune dz Genetic • Hyperparathyroidism
• Dermatomyositis • Ichthyoses (Netherton, • Carcinoid
• Sjogren’s Sjogren-Larsson, etc) • Diabetes, pre-diabetes
• Scleroderma • Porphyrias (PCT, EPP) • Wilson’s
• SLE • Large congenital nevi • Progesterone dermatitis
• Graft versus Host disease
• Allergy
• Neoplastic Other • Mast cell activation
• Mycoses Fungoides • Drugs/medications syndrome
• Non-melanoma skin cancer • Pregnancy, progesterone
www.mghcme.orgDiagnostic algorithm
Image from UpToDate
www.mghcme.orgDiagnostic algorithm
Image from UpToDate
www.mghcme.orgKey elements of ROS
• ? Neuropathy
– Burning, tingling Diabetes
– Change in sweating distribution Vit B12 deficiency
– Muscle weakness – distal vs proximal
• ? Systemic disease
– Fevers, night sweats, weight loss Malignancy
– Abdominal pain Cholestatic disease
– Change in bowel or urinary habits Renal disease
• ? Connective tissue disease Sjogren’s
– Dry mouth/dry eyes?
– Arthritis or myalgias?
Scleroderma
Dermatomyositis
SLE
www.mghcme.orgTrial of treatment
• If no red flags on ROS, a trial of treatment for 1-2
months is reasonable.
• If you suspect:
– DRY SKIN ……………heavy emollients, humidifier use
– HIVES ………………...long-acting H1 anti-histamines
– INFLAMMATORY/ECZEMATOUS DERMATITIS
………………..…….topical steroids or prednisone taper
– SCABIES……………..permethrin >>> ivermectin
– TINEA…………………anti-fungals
– DRUG REACTION or CONTACT DERMATITIS ……..drug
discontinuation or allergen avoidance +/- topical steroids
www.mghcme.orgWhen & What to Screen
• If the patient has a primary rash:
– Trial of treatment with topical steroids, anti-infectious agents, emollients
– If patient fails topical therapy, refer to Dermatology
– Consider the following studies: CBC with differential, LDH (if generalized
itch or erythema), stool O+P (if travel or itchy pets), HIV (if folliculitis), RPR
(if risk factors), ANA
• If the patient has no rash, + ROS, or fails treatment trial:
– CBC with differential, iron studies, SPEP
– LFTs, LDH, BUN/Cr
– Bullous pemphigoid Ag IgGs (pre-urticarial stage)
– Consider: Hgb A1c, TSH, HIV, Hep C, RPR, ANA (if ROS+ or risk factors)
– CXR or age-appropriate malignancy screening
– Consider referral to: Hematology/Oncology (if ROS+ F/S/wt changes),
Allergy and/or Dermatology(refractory hives or flushing), Rheumatology (if
ROS+ arthritis, multi-organ sx), Psychiatry, other specialties as indicated
www.mghcme.orgWhat happens at the dermatologist
• Skin biopsy
– Hematoxylin and eosin staining (standard)
– Direct immunofluorescence staining (if autoimmune
condition is suspected)
– Intra-epidermal nerve fiber (IENF) staining
• Patch testing or photo-patch testing
• More extensive laboratory work up for autoimmune,
infectious or malignant causes of itch
www.mghcme.orgPART IV: DISEASE-SPECIFIC
CONSIDERATIONS
www.mghcme.orgParaneoplastic itch
Comorbid diagnoses:
• Skin exam for
cancer or other
paraneoplastic
findings
• Lymph node exam
• Routine age-
appropriate
malignancy
screening should
be up to date
Larson, et al, 2020, JAAD 81(5): 1198-1201.
www.mghcme.orgMast cell related itch
Comorbid diagnoses:
• GI: IBS, GERD, celiac, eos.
esophagitis, food
intolerance
• Neuro: migraines,
fibromyalgia, chronic
fatigue, POTS
• GU/Gyn: cystitis,
infertility, dysmenorrhea
• Psych: anxiety,
depression, insomnia
• Pulm: asthma, bronchitis
www.mghcme.orgDiagnostic studies in mast cell disease
• Samples should be refrigerated and centrifuged if possible for accuracy
• A word of caution about serum tryptase
• Elevated serum tryptase baseline suggests mastocytosis
• In mast cell activation syndrome (MCAS), tryptase levels are only detectable within 1-4 hours of episode.
Random testing is less helpful!
• Other tests to consider: (*Most sensitive in dx of MCAS)
• Serum chromogranin A
• Plasma prostaglandin D2, histamine, and heparin*
• Random and 24 hr urinary
• Prostaglandin D2*
• Histamine metabolites: N-methyl histamine & 1-methyl-4-imidazole acetic acid
– Moderate specificity for MCAS, but may be influenced by diet
• Leukotriene E4
– Useful to guide use of leukotriene inhibitor therapy Zenker N, Afrin LB. Blood (2015) 126 (23): 5174
Vysniauskaite M et al., PLoS ONE 2015;10(4):e0124912
• 11-β-Prostaglandin F2α* Zblewski D et al., Blood 2014;124(21):3204
Ravi A et al., J Allergy Clin Immunol Pract 2014;2(6):775
www.mghcme.orgSmall fiber polyneuropathy
• Peripheral never disorder affecting primarily small diameter
somatic fibers and/or autonomic fibers.
• Unmyelinated C fibers and thinly-myelinated Ad fibers
• Numerous medical conditions may underlie symptoms (metabolic,
infectious, autoimmune, etc)
• Questionnaire to SFPN patients (41 pts)
• Burning 77.5%
• Pain 72.5%
• Numbness 67%
• Itch 68.3%
• Most frequently affected back and distal limbs
• Worse at night
• Exacerbated by xerosis, sweating, hot temperatures, stress, fatigue
• Relieved by cold water
Brenaut et al., JAAD 2015 Feb; 72(2): 328-32
www.mghcme.orgDiagnostic evaluation of SFPN
• High clinical suspicion
• Typically affects hands and/or feet, but can affect face, trunk and arms first
• +/- Autonomic sx including dry eyes, dry mouth, orthostasis, constipation, urinary
incontinence, altered sweating
• Commonly lacks a primary inflammatory eruption
• Flushing can be seen Normal
• Can manifest as a change in previous dermatitis
• Hyper- or hypopigmentation, atrophy or xerosis (due to sudomotor loss)
• Intraepidermal nerve fiber (IENF) density
• 3mm punch biopsy from distal leg (10 cm above lateral malleolus)
• Sensitivity (78-92%) and specificity (65%-90%) SFPN
•Conclusions
• Itch has an impact on quality of life and is often a
diagnostic clue to other comorbid disease.
• Think broadly! When itch is severe, it’s usually
not just dry skin.
• A thorough physical exam and review of systems
is key when figuring out etiology of itch.
• MGH Itch and Neurocutaneous Disorders Clinic is
available to help!
www.mghcme.orgThank you!
www.mghcme.orgYou can also read