May 2021 - Immunize Nevada
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
May 2021
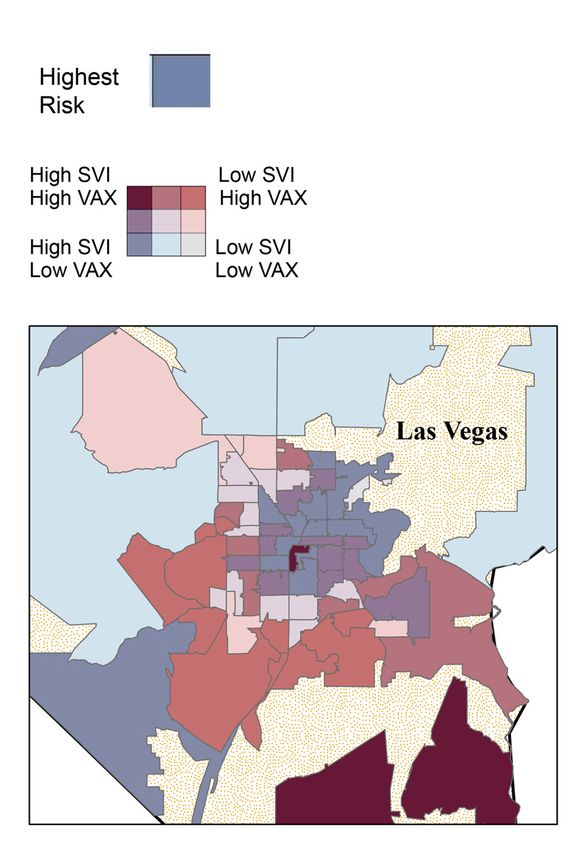
Table of Contents
Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Community-Engaged Outreach . . . . . . . . . . . . . . 5
Building a Communication Framework . . . . . . . . . . 8
Identify Your Target Population . . . . . . . . . . . . . . 9
Get to Know Your Target Audience . . . . . . . . . . . . 13
Tailoring Messages . . . . . . . . . . . . . . . . . . . . . 14
Vaccine Communication . . . . . . . . . . . . . . . . . . 15
Communication Considerations . . . . . . . . . . . . . . 16
Developing a Communication Plan . . . . . . . . . . . . 17
Vaccine Distribution Plan . . . . . . . . . . . . . . . . . . 18
Our Recommendations . . . . . . . . . . . . . . . . . . 20
References . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Appendix A . . . . . . . . . . . . . . . . . . . . . . . . . 22
Appendix B . . . . . . . . . . . . . . . . . . . . . . . . . 26
PAGE 2Overview
The COVID-19 pandemic has profoundly impacted the lives of all Nevadans, especially the
state’s most socially vulnerable communities. The morbidities and mortalities of COVID-19 reveal
a disproportionate impact by the virus and an amplification of existing social inequities. As the
COVID-19 vaccines were introduced to Nevada in mid-December 2020, the rollout revealed an
inequitable distribution throughout the state. In early February 2021, Governor Steve Sisolak
declared, “Equity and fairness requires an intentional effort to reach every community and not
create a situation where those who have been disproportionately impacted by this virus are left
behind — including the elderly and frontline workers.”
The widespread allocation and distribution of a safe and effective COVID-19 vaccine is the
foundation of establishing community immunity. In response to Governor Sisolak’s equity initiative,
along with President Biden’s National Strategy for the COVID-19 Response and Pandemic
Preparedness, Immunize Nevada and the Nevada Minority Health and Equity Coalition partnered
to form the Nevada Vaccine Equity Collaborative (NVEC). This collaborative includes public,
private, state, and community partners who are invested in the equitable distribution of the
COVID-19 vaccine.
NVEC STRATEGY:
• Develop a community-engaged outreach approach to reduce the impact of COVID-19 and
increase vaccine uptake
• Develop a comprehensive communication plan to meet the cultural and linguistic needs of
communities highly impacted by COVID-19
• Maximize and leverage community partnerships, resources and opportunities
• Assess the latest data and provide the state and health districts with recommendations on
how to equitably distribute the vaccine
This strategic plan is a living document and will be adjusted as Nevada responds to the
needs of its residents. Four ethical principles guided its creation:
• Maximize benefits and minimize harms
• Promote justice
• Mitigate health inequities
• Promote transparency
With these considerations at the forefront, Nevada’s vaccination plan is designed to mitigate
asmuch disease spread and death as possible, and requires that every person be considered and
treated as having equal dignity, worth, and value.
NVEC GOALS:
• Accelerate getting shots into arms and accines into the communities that need them most
• Create as many venues as needed for people to be vaccinated
• Focus on hard-to-reach and high-risk populations
• Drive equity throughout the vaccination campaign and broader pandemic response
PAGE 3THE FOLLOWING DOCUMENT
IS A GUIDE TO ACHIEVING
THE ABOVE STATED GOALS.
PAGE 4Community-Engaged Outreach
Engagement with the community of interest is an essential element of public health work.
Community engagement is defined as “...the process of working collaboratively with and through
groups of people affiliated by geographic proximity, special interest or similar situations to address
issues affecting the well-being of those people.” (Centers for Disease Control and Prevention
[CDC], 1997, p. 9). It involves careful planning and acknowledgment of the uniqueness of each
population, as well as inclusivity by creating strong and sustainable relationships within those
different communities. While we acknowledge that community involvement runs on a spectrum and
all relationships on this spectrum are important – considerations should be made towards building
community relationships that empower our communities and public health practice (Table 1).
Community-engaged outreach (CEO) is a departure from traditional outreach, where the primary
aim is to share information with the community about an issue, problem, opportunity, or decision.
TABLE 1: SPECTRUM OF COMMUNITY ENGAGEMENT
Increasing level of Community Involvement and Impact
INFORM CONSULT INVOLVE COLLABORATE EMPOWER
PUBLIC To provide To obtain To work directly To partner with To place final
PARTICIPATION the public public feedback with the public the public in each decisions in the
GOAL with balanced on analysis, throughout the aspect of the hands of the
and objective alternatives, and/ process to ensure decision, including public
information to help or decisions public concerns developing
them understand and aspirations alternatives and
the problem, are consistently identifying the
alternatives, understood and preferred solution
opportunities, considered
and/or solutions
PROMISE TO We will keep the We will keep the We will work We will look to We will implement
THE PUBLIC public informed public informed, with the public the public for what the public
listen to and to ensure that direct advice decides
acknowledge community and innovation
concerns and concerns and in formulating
aspirations, and aspirations are solutions and
provide feedback directly reflected incorporate
on how public in the alternatives your advice and
input influenced developed and recommendations
that decision provide feedback in to the decision
on how public to the maximum
input influenced extent possible
the decision
EXAMPLE Communicate Learn about Community Work closely Community
COVID-19 vaccine community partner meetings with community member is able
information to concerns and to discuss the partners to to make an
communities by barriers regarding COVID-19 build vaccine informed decision
using various the COVID-19 vaccine concerns confidence and about vaccination
channels such as vaccine by and barriers eliminate barriers because they
fact sheets, flyers, conducting focus within specific to vaccination were provided
or social media groups and communities and within their accurate
surveys possible solutions respective and relevant
communities information, and
barriers were
addressed
Note: Adapted from Community Engagement during the COVID-19 Pandemic and Beyond by M. Fedorowicz, O. Arena, and K. Burrowes,
2020, Urban Institute. Copyright 2020 by Urban Institute.
PAGE 5Therefore, CEO should be thought of as combination of both community engagement and
community outreach. It involves community partners having a seat at the table throughout
the entire decision-making process to ensure outreach will actively engage and appropriately
represent their respective communities. Successful community engaged outreach will result in
appropriate reflection of a community’s values, empowered decision-making, and a reduction in
inequities often seen in services.
V
DIVERSITY IS HAVING A SEAT AT THE TABLE,
INCLUSION IS HAVING A VOICE, AND
BELONGING IS HAVING THAT VOICE BE HEARD.
EQUITABLE CEO ENCOMPASSES (DONOVAN, 2014):
• Striving for community representation and inclusion of underrepresented groups
• Fostering equitable relationships by accounting for power differentials in
decision-making processes
• Increasing public understanding and support for an issue in culturally responsive ways
• Facilitating local, community-driven decisions that appropriately reflect community needs
• Building accountability and trust by building processes that are responsive to
feedback from community partners and by delivering what is promised
• Identifying shared community concerns, interests, and goals
• Creating strong, healthy, vibrant places to live, work, learn, and plan
• Creative problem-solving that accounts for the perspectives
and knowledge of community members
• Supporting existing community leaders and developing new community leaders
• Working with community members to identify community assets, skills, and resources
• Continuous reflection of how decisions impact diverse groups
• Establishing and maintaining feedback to ensure that outputs
center community needs and perspectives at every step
PAGE 6To guide the creation of our CEO approach, we have established a set of core values
and principles (Table 2).
TABLE 2: OUR CORE VALUES AND PRINCIPLES
VALUE PRINCIPLE(S)
EQUITY • share decision-making and initiative leadership as often as possible
• provision of varying levels of support—based on specific needs—to achieve
greater fairness of treatment and outcomes (Longley, 2020).
• treat participants with integrity and respect
INCLUSIVITY • the process of improving the terms on which individuals and groups take part
in the partnership—improving the ability, opportunity, and dignity of those,
who at an aggregate, social level, have historically been disempowered (The
World Bank, n.d.)
• creating a space in which communities feel valued and welcomed
DIVERSITY • engaging community members with different backgrounds, beliefs, and
experiences such as race/ethnicity, citizenship status, religious beliefs,
socioeconomic status, language, geographical origin, gender and/or
sexual orientation
• recognizing that these differences as assets to learning and innovation
CULTURAL HUMILITY • maintain awareness of power imbalances and biases, respect other’s values,
and do not set personal expectations to memorize all aspects of another
culture
• understand how personal biases may impact work
• a lifelong process of self-reflection and self-critique whereby the individual
not only learns about another’s culture, but one starts with an examination of
her or his own beliefs and cultural identities (Yeager & Bauer-Wu, 2013)
ACCOUNTABILITY • build processes that are responsive to feedback from community partners
• be willing to change and adapt throughout the process
TRANSPARENCY • communicate openly about motives, resources, power dynamics, and
decision-making processes
• acknowledge challenges and limitations and work openly to address these
and maintain the trust of our communities
SUSTAINABILITY • continually reflect, assess and communicate to maintain and deepen
relationships for long-term action
• allocate adequate resources to maintain relationships with communities over
the long-term
CAPACITY BUILDING • increase community involvement, impact, trust, and communication by
improving coordination, enhancing existing services, advocating for policy
change and learning through pilots
Note: Adapted from Race to Justice: Community Engagement Framework by the New York City Department of Health and Mental Hygiene, 2017.
PAGE 7Building a Communication Framework
ENGAGE PARTNERS
IDENTIFYING SITE LOCATION
Pods
• accessible
• trusted
Other
• providers
• pharmacies
• non-vaccine providers
ENGAGE ADDITIONAL PARTNERS
TO ADDRESS SITE NEEDS
• Churches, chambers, coalitions, consulates, etc.
• transportation partners
• voluneeer recruitment
• homebound/disabled
SCHEDULING A VACCINE
• simplify the process
• consider langague and technology literacy
COMMUNICATION REGARDING THE VACCINE
• address access
• address hesistancy
• timeliness
• consider literacy
• use of diverse methods
COORDINATE SITE ACTIVITIES
• local volunteers
• language needs
• from front door to vaccine
• volunteer training
PAGE 8Identify Your Target Population
Targeting intervention approaches to the most at risk supports the reduction of negative outcomes
due to COVID-19 among our most vulnerable communities — older adults, those with preexisting
conditions, racial and ethnic minorities, those with disabilities, and other vulnerable populations
(CDC, 2021).
The Centers for Disease Control and Prevention’s (CDC) Social Vulnerability Index (SVI) can serve
as a tool to identify at-risk communities before, during, and after disasters or emergency events
(CDC, 2015). The CDC SVI is used to create maps that identify communities with the greatest social
vulnerability. Resources can then be deployed to geographic locations once communities with the
highest social vulnerability are identified. The CDC SVI accounts for 15 social factors that are divided
into four themes (Figure 1). Each factor is ranked at the census tract level, then ranked as a theme,
and lastly ranked as a whole to give the overall vulnerability.
FIGURE 1: CDC SOCIAL VULNERABILITY INDEX
Below Poverty
Socioeconomic Unemployed
Status Income
VULNERABILITY
No High School Diploma
Aged 65 or Older
OVERALL
Household Composition Aged 17 or Younger
and Disability Older than Age 5 with a Disability
Single-Parent Households
Minority Status and Minority
Language Speak English “Less than Well”
Multi-Unit Structures
Mobile Homes
Housing and
Crowding
Transporation
No Vehicle
Group Quarters
Note: Reprinted from CDC SVI Documentation 2018 by Centers for Disease Control and Prevention (2020).
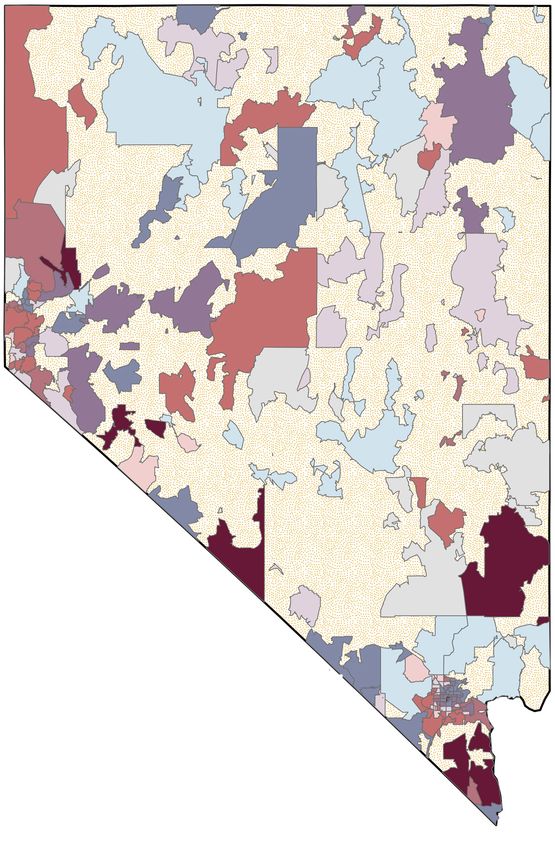
This strategic plan is guided by a modified version of the CDC SVI and provides data at the zip
code level. Our COVID-19 SVI uses the same 15 indicators as the CDC SVI, with the addition of
total numbers of new COVID-19 positive cases and total number of COVID-19 vaccinations by
zip code. The use of COVID-19 specific data provides deeper insight into which zip codes are a)
hit hardest by COVID-19 cases, and b) not receiving an equitable distribution of the COVID-19
vaccinations based on need. Due to data availability limitations, the data are analyzed at the zip
code level.
This analysis resulted in 10 zip codes in Clark County (89102, 89030, 89104, 89101, 89115,
89107, 89106, 89122, 89142) 4 zip codes in Washoe County (89431, 89502, 89512, 89503) and
1 zip code in Carson City (89706).
PAGE 9FIGURE 2: NEVADA ZIP CODE PRIORITIZATION MAP
N
Variable/Term Definition
Vaccination Coverage The estimated percentage of people who have received specific vaccines
County Nevada county name
Zip Code Zip code
SVI Category Social Vulnerability Index category
Low = 0 - 0.333
Moderate = 0.334 - 0.666
High = 0.667 - 1
Population Total population for zip code
COVID+ Cases (%) (# of COVID+ cases / population)*100
Initial Vaccine Coverage (%) (# of first doses / population)*100
Complete Vaccine Coverage (%) (# of completed vaccine series / population)*100
Completed = 2 doses received of Pfizer/Moderna OR 1 dose of Janssen
Vaccination rate towards herd 80 - Complete Vaccine Coverage
immunity (%)
https://www.cdc.gov/vaccines/vaxview/index.html
PAGE 10Vaccine Coverage
Vaccine Coverage
as of 05/02/2021
as of 05/02/2021
% Initial Vaccine
% Initial Vaccine
Coverage as of
Coverage as of
as of 5/4/2021
as of 5/4/2021
SVI Category
SVI Category
% Complete
% Complete
05/02/2021
05/02/2021
Population
Population
% COVID+
% COVID+
Zip Code
Zip Code
County
County
Carson City 89701 High 27193 9.45 39.81 28.35 Clark (cont’d) 89113 Moderate 32308 9.49 45.91 34.10
89706 High 19318 7.50 38.39 26.79 89117 Moderate 54590 8.73 45.43 33.99
89703 Moderate 9955 11.04 54.05 42.28 89123 Moderate 60679 8.05 39.29 29.52
Churchill 89406 High 24213 7.81 29.27 22.80 89124 Moderate 1362 2.72 19.97 15.93
Clark 89015 High 42387 7.33 33.04 25.18 89128 Moderate 35666 9.84 42.32 31.73
89018 High 4847 1.79 5.94 3.24 89129 Moderate 57116 8.00 36.47 27.71
89019 High 2158 5.10 25.25 19.79 89130 Moderate 34697 8.97 36.63 28.27
89025 High 1203 6.07 14.63 10.39 89134 Moderate 24363 6.19 64.66 53.13
89027 High 18446 5.06 41.41 35.28 89139 Moderate 40612 11.04 44.19 31.94
89029 High 8167 4.11 24.33 17.55 89143 Moderate 13265 8.49 32.81 24.91
89030 High 50417 15.37 24.38 15.50 89145 Moderate 25071 9.31 40.63 30.39
89032 High 44200 14.29 33.02 23.90 89148 Moderate 55553 9.65 44.53 32.18
89081 High 37480 10.68 30.71 22.43 89149 Moderate 39613 8.55 39.26 30.13
89101 High 42592 12.40 25.88 16.70 89166 Moderate 25245 8.73 34.55 26.01
89102 High 39449 9.86 29.08 19.83 89183 Moderate 42480 8.24 33.68 24.68
89103 High 53732 9.19 31.70 21.69 89002 Moderate 35881 6.60 35.09 27.76
89104 High 39443 13.84 34.35 22.99 89004 Low 326 3.37 55.83 45.09
89106 High 26480 11.47 25.89 17.42 89012 Low 36512 6.22 45.37 36.23
89107 High 38936 13.53 37.67 24.48 89021 Low 3534 5.04 21.51 15.93
89108 High 73991 11.24 28.94 20.18 89039 Low 149 2.68 55.03 46.98
89109 High 7859 10.80 77.03 41.71 89044 Low 22558 7.41 62.86 51.96
89110 High 71489 15.62 31.48 21.34 89052 Low 55096 7.34 54.80 43.83
89115 High 63084 12.38 21.66 13.66 89054 Low 57 7.02 57.89 42.11
89118 High 21826 10.50 38.32 27.13 89085 Low 4156 7.34 35.54 27.53
89119 High 52378 9.43 28.59 19.00 89131 Low 50564 8.04 35.83 27.99
89120 High 24813 10.41 38.54 28.32 89135 Low 28192 7.85 58.91 46.43
89121 High 63190 11.74 35.72 24.88 89138 Low 17952 8.43 57.59 44.74
89122 High 49600 11.86 37.63 27.28 89141 Low 35169 9.11 44.43 33.34
89142 High 34671 15.46 34.32 23.31 89144 Low 19881 7.23 47.38 36.33
89146 High 18695 12.07 38.06 26.57 89161 Low 136 14.71 95.59 74.26
89147 High 55865 9.69 40.37 29.28 89178 Low 40808 8.93 40.26 29.68
89156 High 29764 12.76 27.69 18.90 89179 Low 7449 14.08 61.43 45.91
89169 High 21822 9.43 28.74 19.00 89191 Low 581 1.55 10.15 8.61
89005 Moderate 15840 5.94 42.83 33.50 Douglas 89410 Moderate 11191 5.67 43.16 33.53
89007 Moderate 1479 5.61 14.87 11.70 89413 Moderate 725 2.07 33.10 27.17
89011 Moderate 28229 10.30 47.28 36.15 89460 Moderate 13570 4.72 36.32 28.39
89014 Moderate 39430 8.82 39.75 30.06 89705 Moderate 5307 4.90 40.06 30.17
89031 Moderate 67750 11.00 34.87 25.79 89411 Low 643 9.80 132.50 111.82
89040 Moderate 3886 3.09 22.16 16.98 89423 Low 10283 5.09 51.45 41.99
89046 Moderate 357 5.88 47.90 37.25 89448 Low 1712 4.67 56.13 44.80
89074 Moderate 50353 7.54 45.92 36.32 89449 Low 3094 3.14 34.74 26.89
89084 Moderate 27773 9.13 44.80 34.93 Elko 89825 High 1289 0.70 16.83 14.90
89086 Moderate 6404 10.35 26.01 19.13 89832 High 1312 0.84 28.73 25.46
PAGE 11Vaccine Coverage
Vaccine Coverage
as of 05/02/2021
as of 05/02/2021
% Initial Vaccine
% Initial Vaccine
Coverage as of
Coverage as of
as of 5/4/2021
as of 5/4/2021
SVI Category
SVI Category
% Complete
% Complete
05/02/2021
05/02/2021
Population
Population
% COVID+
% COVID+
Zip Code
Zip Code
County
County
Elko (cont’d) 89833 Moderate 137 1.46 35.77 31.39 Mineral (cont’d) 89049 Moderate 2286 5.51 27.73 21.30
89834 Moderate 152 2.63 11.18 9.21 Nye 89003 Moderate 820 3.17 34.76 31.59
89835 Moderate 1626 1.35 28.66 23.06 89061 Moderate 6160 6.62 37.37 29.79
89883 Moderate 4381 9.40 24.93 19.33 89045 Low 1951 1.28 13.58 10.56
89801 Moderate 26669 7.00 21.96 17.98 89409 Low 109 2.75 51.38 44.04
89822 Moderate 2160 3.80 14.31 10.88 Pershing 89419 High 5549 7.17 31.97 19.68
89823 Low 124 2.42 32.26 27.42 89418 Low 306 2.29 15.69 12.75
89815 Low 14177 5.92 20.35 17.18 Storey 89440 Low 864 7.41 49.54 36.92
89828 Low 363 5.79 37.19 33.33 Washoe 89424 High 209 10.53 91.87 76.08
89830 Low 208 0.48 12.02 8.17 89431 High 39042 10.54 34.37 20.06
89831 Low 11 63.64 72.73 63.64 89433 High 21875 9.95 30.47 16.72
Esmeralda 89010 High 514 4.28 21.98 14.79 89501 High 3961 7.78 42.77 26.00
89013 High 305 8.20 46.23 35.08 89502 High 45294 10.48 36.60 21.71
89047 Low 142 2.11 19.01 13.38 89506 High 43566 8.86 34.89 21.07
Eureka 89316 Low 1218 2.63 26.03 24.06 89512 High 26222 15.50 36.13 20.68
89821 Low 462 2.16 17.75 13.42 89434 Moderate 25575 9.56 45.51 30.37
Humboldt 89421 High 496 11.90 8.47 5.85 89442 Moderate 1076 4.55 39.68 30.30
89445 High 16387 6.42 25.46 20.71 89508 Moderate 13206 5.84 31.52 21.60
89425 Moderate 312 1.60 32.05 24.68 89509 Moderate 35793 6.26 50.58 36.16
89426 Moderate 174 2.30 40.80 28.74 89510 Moderate 1454 10.04 60.80 44.98
89438 Low 91 1.10 16.48 12.09 89503 Moderate 28867 7.82 42.50 27.75
89414 Low 154 1.95 43.51 33.12 89523 Moderate 34363 7.24 50.17 35.57
Lander 89820 High 5436 7.63 23.75 19.81 89402 Low 16 56.25 731.25
89310 Low 292 2.74 48.97 45.21 89405 Low 134 0.75 8.21 6.72
Lincoln 89008 High 1009 2.68 35.38 32.31 89412 Low 114 14.91 107.02 78.95
89042 Moderate 1247 3.37 18.28 15.88 89436 Low 43826 8.30 46.81 33.12
89043 Moderate 1478 1.76 23.27 20.77 89439 Low 1284 6.85 77.10 57.17
89017 Low 83 10.84 100.00 72.29 89441 Low 12435 8.11 45.39 33.53
89001 Low 1363 2.49 22.60 18.20 89450 Low 60 1178.33
Lyon 89429 High 7715 3.24 24.46 18.20 89451 Low 8777 3.25 38.19 24.66
89447 High 7834 3.42 35.12 28.20 89511 Low 26443 8.46 61.26 45.82
89403 Moderate 15531 5.51 38.05 28.39 89519 Low 8766 6.00 60.87 47.66
89408 Moderate 20439 6.00 29.20 19.57 89521 Low 33381 8.47 55.45 39.27
89444 Moderate 2949 1.87 34.45 28.72 89704 Low 3828 4.57 49.01 37.90
89428 Low 158 3.80 60.13 51.90 White Pine 89301 High 8141 3.54 27.85 23.36
89430 Low 308 6.17 63.96 52.27 89314 Moderate 313 0.64 26.84 21.73
Mineral 89415 High 3043 9.83 45.65 40.72 89317 Moderate 268 4.10 45.90 42.16
89427 High 1162 7.83 3.18 2.32 89311 Low 124 4.03 108.87 106.45
89420 Low 55 1.82 27.27 21.82 89318 Low 990 3.13 32.22 29.49
89422 Low 182 1.65 32.42 29.67 89319 Low 132 6.06 91.67 83.33
89020 High 1435 4.04 22.37 18.19 NOTE: Some zip codes exceed 100% vaccination may be due to zip
89048 High 21784 5.24 27.69 21.65 codes applied to where the shot was administered rather a person’s
89060 High 9473 7.61 28.03 21.57 place of residence.
PAGE 12Get to Know Your Target Audience
When getting to know the target audience, several factors must be accounted for including:
geographic, demographic, psychographic, and behavioral information. Getting to know these
factors will guide the creation and delivery of messaging to the target audience.
TABLE 3: SOCIAL FACTORS TO CONSIDER ABOUT THE TARGET AUDIENCE
GEOGRAPHIC FACTORS
VARIABLE EXAMPLE(S)
City Las Vegas, Reno, Elko
Zip code 89110, 89115, 89106
Population density Under 5,000; 5,000-20,000; 50,000-100,000
DEMOGRAPHIC FACTORS
VARIABLE EXAMPLE(S)
Age 16-24, 25-34, 35-44, 45-54, 55-64, 65 and over
Gender Male, Female, Transgender (MTF), Transgender (FTM), Gender fluid/non-binary
African American/Black, American Indian/Alaska Native, Asian, White, Hispanic/
Race or ethnicity
Latinx, Native Hawaiian/Pacific Islander, Other
Family size 1-2, 3-4, 5 or more
Under $10,000, $10,000-20,000; $20,000-30,000; $30,000-50,000; $50,000-
Income
100,000; $100,000-250,000; over $250,000
Employment Status Employed, Unemployed
Grade school or less, Some high school, High school graduate, Some college,
Education
College graduate
Religion Catholic, Protestant, Jewish, Muslim, Hindu, other
PSYCHOGRAPHIC FACTORS
VARIABLE EXAMPLE(S)
Lower lower, Upper lower, Working class, Middle class, Upper middle, Lower upper,
Social class
Upper upper
Lifestyle Achievers, Strivers, Strugglers
Personality Compulsive, Outgoing, Authoritarian, Ambitious
BEHAVIORAL FACTORS
VARIABLE EXAMPLE(S)
Benefits Safety, Economy, Convenience, Speed
Readiness stage Unaware, aware, informed, interested, desirous, intending to vaccinate
Attitude towards vaccination Enthusiastic, Positive, Indifferent, Negative, Hostile
Note: Adapted from Social Marketing: Behavior Change for Social Good by N. Lee and P. Kotler, 2020, SAGE Publishing.
PAGE 13Tailoring Messages
Community engagement is the most effective strategy to authentically learn about the audience and
how to tailor messaging to them effectively. Engaging with the community provides firsthand insight
into common concerns or barriers that exist. It also helps develop a better understanding of how to
create messaging that is relevant and accurately represents the target audience.
Our top priority is to create culturally and linguistically appropriate messaging. To do so, we have
established four key goals that guide the creation of culturally engaged content (Table 4).
TABLE 4: GOALS FOR CULTURALLY ENGAGED MEDIA
REPRESENTATION Develop content that accurately and realistically represents the target population
through colors, symbols, photographs, graphics, etc.
RELEVANCE Develop content that matches the needs, concerns, beliefs, and attitudes of the
target population
LANGUAGE Develop content in the language(s) commonly used within the target population(s)
which also considers accessibility, literacy level, and colloquial language
VARIETY Develop content for multiple mediums including print, mailers, TV, radio
commercials, and social media to account for the digital divide and limited access
to internet among low-income and minority populations
To create culturally engaged outreach, we will practice cultural humility by:
• Engaging with our community partners to gather input and feedback about the representation,
relevance, language and variety of the content being produced;
• Practicing flexibility and possess the ability to adjust the direction of content based on the
feedback given by the community;
• Regularly assessing our work to ensure content is culturally engaged;
• Clearly communicating changes and/or discrepancies with all team members.
PAGE 14Vaccine Communication
An equitable communication plan must include both vaccine access and vaccine hesitancy to be
effective.
Based on this, we identified five key messaging themes to address when developing
messaging about the COVID-19 vaccine:
• Disease Spread, Safety, & Prevention
• Vaccine Safety & Efficacy
• Vaccine Prioritization & Distribution
• Vaccine Purpose, Need, and Location
• Similarities and Differences between COVID-19 and Influenza
Although many of the concerns surrounding the COVID-19 vaccines overlap among the different
target populations, it will ultimately be ineffective to create a single, universal message to share
among each group. The messages need to be prioritized and tailored to each community to
ensure it is relevant and resonate with the target population. Messaging can vary based on
communication goals, audiences, and available resources.
The framework allows for more specific and relevant messaging based on our five key messaging
themes and three key audience mindsets. The framework presented below is flexible and will allow
for pivoting as new vaccine developments and distribution plans emerge.
TABLE 5: COMMUNICATION FRAMEWORK
OVERARCHING GOAL
Increase vaccine uptake among Nevada’s most socially vulnerable communities by working with trusted community
partners and conducting community engaged outreach
OVERARCHING CONCERNS
Vaccine Access Vaccine Hesitancy
KEY MESSAGING THEMES
Disease Spread, Vaccine Vaccine Prioritization Vaccine Purpose, Similarities and
Safety & Prevention Safety & Efficacy & Distribution Need, and Location Differences between
COVID-19 and
Influenza
KEY AUDIENCE MINDSETS
READY & WILLING UNSURE & NEEDS INFORMATION SKEPTICAL & CRITICAL
Provide clear information about Build vaccine confidence Build trust
vaccine eligibility
Inform about vaccination Provide clear information about the Build vaccine confidence
expectations (i.e., what to expect the importance of vaccination
day of, potential side effects)
Provide clear information about Address physical vaccination barriers Be consistent and transparent
vaccine eligibility with information about the vaccine
Educate about preventative Acknowledge concerns and hesitancies by Minimize misinformation
measures after vaccination providing timely, transparent, and science-
based information
PAGE 15Communication Considerations
TRUSTED MESSENGERS
Identify trusted messengers to deliver vaccine information and the call to action. This includes
identifying trusted community influencers from within each specified socially vulnerable
community, including faith leaders, community organizers, or local business owners.
UNIQUE HESITANCY ISSUES
Information regarding the community’s hesitancies can be collected with the help of a community
influencer. In partnership, create messaging that addresses the vaccine access issues and other
barriers.
After addressing vaccine hesitancies and identifying access barriers, these partnerships drive the
planning of local community clinics or PODs. This model can also be implemented in the future to
address vaccine hesitancy towards the flu vaccine or children’s school aged vaccinations.
Nevada Vaccine Equity Collaborative Example: Informational flyers and how-to’s for creating
an appointment in English and Spanish. Translating educational content to a school grade level for
broad understanding of the vaccine information. Placing vaccine information and digital resources
at bus shelters.
TIMELINESS
Timeliness of communication is important as clinic locations are changing constantly along with
mobile units being addded to the distribution strategy. Type of vaccine available at a given clinic
is also relvant for those ages 16-17 years old (af of April1, 20201, only Pfizer is approved for that
age group).
Communicating to socially vulnerable communities is crucial. They will experience difficulty
creating vaccine appointments with lack of technology and internet access, they may lack
transportation to a vaccine appointment, and could be potentially left out of the vaccination
process. Creating community vaccine clinics using the community-engaged outreach model, in
partnership with community influencers will address the aforementioned challenges.
Address vaccine access
Address vaccine issues i.e. location,
Vaccine Pod
hesistancy concerns transportation,
ability to sign up
PAGE 16Developing a Communication Plan
A successful communication plan must account for diverse stakeholders and their varying
capabilities and access to different platforms. Stakeholders should use a variety of
communication methods and channels to best reach their community members. Online platforms
are capable of sharing information quickly, but often exclude socially vulnerable populations
such as the elderly, individuals with low income, immigrants, and individuals with low-English
proficiency. A part of developing the communication framework is to take into consideration which
dissemination channels are best suited for each key audience.
TABLE 6: TOOLS FOR COMMUNICATION
NON-DIGITAL TOOLS
Non-digital communication methods are a great way to engage with the elderly, people with limited access to the internet,
and people with limited computer literacy.
A phone tree is a system to activate a group of people by phone. It is a great way to effectively
PHONE CALLS AND
and efficiently spread a brief message to a large number of people. This method is most effective
PHONE TREES
with brief messaging, such as notifying individuals about a meeting or last-minute change.
Mailers are postcards and flyers that include information that are sent directly to people.
It is an effective way to reach an audience and raise awareness when digital formats are
MAILERS
unavailable. This strategy can also be used to encourage community participation such as a
completing a survey or attending an event.
Both television and radio can be used to broadly share a developed message through
BROADCAST MEDIA commercials. However, it is important to consider the tone and specific content, as well as the
primary listening audience.
Flyers and brochures are still an effective way of sharing information to communities,
PRINT MATERIALS
especially among those who do not have access to digital formats.
Use existing community-based newsletters to share information. Existing community networks
NEWSLETTERS
and connections can provide a more authentic community response and engagement.
Billboards target users that use various modes of transportation. Level of community
BILLBOARDS
engagement depends on the amount of traffic that passes by daily.
Directly engage with a community by attending in-person events such as tabling at a
IN-PERSON EVENTS
community resource fair, handing-out information at a drive-thru event, or engaging in
conversation at a townhall meeting. These are great ways to inform, consult, and involve
the community.
DIGITAL TOOLS
Digital dissemination methods offer a way to share information quickly without having community members leave the
comfort of their home.
Facebook, Instagram, Twitter, LinkedIn, and TikTok are platforms that can be used to
SOCIAL MEDIA informally engage with the community. Social media platforms can be used to inform, consult,
and involve the community.
WEBSITE Websites can be used to share online brochures, flyers, and toolkits with community members.
Host a webinar or virtual townhall to engage the community in a deeper conversation. These
WEBINAR OR
events can help educate the community, provide feedback about a proposed plan, and
TOWNHALL
provide key insight about common community concerns.
Share information with the community through email. Similar to a non-digital newsletter, use
EMAIL AND DIGITAL
existing community-based Listervs to distribute content. Existing networks and connections
NEWSLETTER
can provide a more authentic community response and engagement with the material.
Text messaging and messaging apps, such as Whatsapp, can be used to broadly share
TEXT MESSAGING
information within a community.
Videos are an effective way to raise awareness and to engage with the community. Videos
VIDEOS
can be shared by all digital methods and should be simple and easy to digest.
PAGE 17Vaccination Distribution Plan
PROMOTE EQUITABLE ACCESS TO VACCINATION
To inform COVID-19 vaccination outreach efforts at the programmatic and provider levels,
jurisdictions need to know where community members are located. Jurisdictions should create
visual maps of these populations, to assist in COVID-19 vaccination clinic planning, especially for
satellite, temporary, or off-site clinics. To ensure equitable access to vaccination services among
priority populations and identify areas where additional providers might be needed, jurisdictions
could also use mapping tools to identify areas with health disparities.
THE ROLE OF MAPPING
Maps of critical populations (using an index such as the COVID-19 Vulnerability Index) should
then be overlaid with maps of enrolled providers by provider type and populations served by
these providers. Jurisdictions might also want to consider encouraging and supporting healthcare
personnel who are existing trusted sources and work in areas serving these priority population
groups to enroll as vaccination providers.
Nevada Vaccine Equity Collaborative Example: Vaccine Locator. Making it prominent on the
landing page of NV Covid Fighter. Being updated with age information so 16 and 17 year olds
know where to receive the Pfizer vaccine. Data from the state is being collected to identify which
zip codes were most impacted by COVID-19 guiding where resources should be placed. Working
with local healthcare providers from BIPOC communities to build confidence and trust for the
vaccine.
Several factors should be considered when selecting a vaccination site for a population.
Some considerations are listed below:
• Populations with limited mobility, including those who might be homebound or have other
access issues, on-site vaccination is essential.
• Options for non-traditional clinic sites and hours, sites are coordinated with other community
services, subsidized and/or accessible transportation.
• Training and scheduling providers or staff - who represent the community and speak the
appropriate languages - to administer vaccine.
• Working with trusted or racially concordant providers or staff to refer individuals to vaccination
provider sites
• Connect vaccination providers with places of worship, community organizations, recreation
programs, food banks/pantries, schools and colleges/universities, grocery stores, salons/
barbershops/beauticians, major employers, and other key community institutions to
set up temporary and/or mobile COVID-19 vaccination provider sites, especially in high-
disparity communities.
• Connect local health departments, community health centers, and/or trusted healthcare
organizations, including pharmacies, with communities through mobile COVID-19 vaccination
clinics in communities facing disparities to increase the number, range, and diversity of
opportunities for vaccination.
• Build partnerships with healthcare providers to increase provider understanding of the
populations of interest and interventions to increase vaccination rates for these populations.
PAGE 18Nevada Vaccine Equity Collaborative Example: Working with pharmacy and health district
partners to set up pop-up clinics. Taking vaccine to those who need it. Working with trusted
community partners to create pop-up clinics. Working with partners that understand and have
established trust with the population being vaccinated, for example NV Homeless Alliance and
Catholic Charities. Identifying vaccinators that look like the community they are vaccinating.
BALANCING VACCINE SUPPLY, ACCESS, EQUITY, AND DEMAND
Jurisdictions must strike a balance between vaccine supply, access, and demand. Ensuring
access includes having vaccination sites near public transportation.
If there is low uptake, which can manifest as low coverage, jurisdictions will need to quickly
understand the reasons and address them before vaccine wastage occurs. When demand is
found to be low, jurisdictions are encouraged to work with community groups and community
leaders to understand and address any population concerns.
Nevada Vaccine Equity Collaborative Example: Collecting input from community partners for each
identified vulnerable group. Allowing them to guide the clinic planning process. Introducing the
resources we have available and how they can be used the partner agency.
FEDERAL RETAIL PHARMACY PARTNERSHIP STRATEGY
Federal pharmacy partners begin ordering vaccine directly from the federal government for
distribution to broad population groups. Pharmacy providers will also be required to report
CDC-defined vaccine administration data elements to jurisdiction immunization information
systems (IISs)
Nevada Vaccine Equity Collaborative Example: All pharmacies added to vaccine locator.
Ages being added to identify Pfizer for ages 16+. Vaccine locator will be updated regularly to
reflect updated Pfizer providers
SCHEDULING A VACCINE
To ensure access to vaccine appointments, provide a phone line to answer questions and/or
schedule over the phone. Consider preferred language and technology availability, and have
volunteers available to assist with the process if needed.
Nevada Vaccine Equity Collaborative Example: The statewide helpline is available in multiple
languages, 7 days, week, 7:00 am to 8:00 pm. Call center staff are available to assist with making
appointments.
PAGE 19Our Recommendations
Community-engaged outreach involves making sure that community partners have a seat at
the table and that they have a voice throughout the entire decision-making process to ensure
outreach will actively engage and appropriately represent their respective communities. CEO
is an effective way to create culturally and linguistically relevant content. Successful CEO will
reflect the community’s values, empower community-level decision-making, and a reduce
inequities often seen in services.
To successfully implement community-engaged outreach, we have three key
recommendations:
1. Be inclusive. Community members need to have a seat at the table and a voice throughout
every step of the process. These members are able to indicate what barriers their communities
are facing when receiving information.
2. Be responsive. Community members are able to provide firsthand insight into the needs of their
community. It is critical to respond to their recommendations in order to maintain relevance.
3. Be timely. Timeliness is essential and it is not necessarily about speed. The delivery of
messaging should be well-timed and appropriate to the community’s current needs. For example,
in some communities, there is low awareness about COVID-19. So, delivering messages about
the importance of vaccinating should not precede messages that educate the community about
the COVID-19 virus and essential safety precautions. Likewise, timely dissemination to address
vaccine concerns and communicate the location of pod pop-ups is critical.
PAGE 20References
Centers for Disease Control and Prevention (1997). Principles of community engagement
(1st ed.). Atlanta (GA): CDC/ATSDR Committee on Community Engagement; 1997.
Centers for Disease Control and Prevention. (2015). Planning for an Emergency: Strategies for
Identifying and Engaging At-Risk Groups. Retrieved from https://www.cdc.gov/nceh/hsb/
disaster/atriskguidance.pdf
Centers for Disease Control and Prevention. (2020). CDC SVI Documentation 2018.
Retrieved from https://www.atsdr.cdc.gov/placeandhealth/svi/documentation/SVI_
documentation_2018.html
Centers for Disease Control and Prevention. (2021). People at Increased Risk. Retrieved from
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html
Donovan, M. E. (2014). Community Outreach and Engagement. University of New Hampshire
Cooperative Extension. Retrieved from https://extension.unh.edu/resources/files/
Resource004766_Rep6785.pdf
Fedorowicz, M., Arena, O., and Burrowes, K. (2020). Community Engagement during the
COVID-19 Pandemic and Beyond. Urban Institute. Retrieved from https://www.urban.org/
research/publication/community-engagement-during-covid-19-pandemic-and-beyond
Lee, N. & Kotler, P. (2020). Social Marketing: Behavior Change for Social Good [6th Edition]. SAGE
Publishing.
Longley, R. (2020, August 21). Equity vs. Equality: What is the Difference? ThoughtCo. Retrieved
from https://www.thoughtco.com/equity-vs-equality-4767021#:~:text=Equity%20refers%20
to%20the%20provision,fairness%20of%20treatment%20and%20outcomes.
New York City Department of Health and Mental Hygiene. (2017). Race to Justice: Community
Engagement Framework. NYC Health. Retrieved from https://www1.nyc.gov/assets/doh/
downloads/pdf/che/community-engagement-framework.pdf
Wang, H.L. (2018, November 6). Native Americans On Tribal Land Are ‘The Least Connected’
To High-Speed Internet. NPR. Retrieved from https://www.npr.org/2018/12/06/673364305/
native-americans-on-tribal-land-are-the-least-connected-to-high-speed-internet
The World Bank. (n.d.). Social Inclusion. Retrieved from https://www.worldbank.org/en/topic/
social-inclusion#:~:text=Social%20inclusion%20is%20the%20process,the%20basis%20
of%20their%20identity.
Yeager, K.A. & Bauer-Wu, S. (2013). Cultural humility: Essential foundation for clinical
researchers. Applied Nursing Research, 26(4), 251-256. doi: 10.1016/j.apnr.2013.06.008
PAGE 21Appendix A
Arriba Las Vegas & Puentes Community Clinic / Arriba Las Vegas y Puentes Clínica Comunitaria
April 10, 2021
Mater Academy East Las Vegas
3900 E. Bonanza Road, Las Vegas, NV 89110
9 am – 4 pm
BACKGROUND:
Access to the COVID-19 vaccine in southern Nevada began as a tiered system, otherwise
known as “lanes.” These lanes were ranked by age group and categories of certain employment/
occupation being at the top, such as frontline medical staff. The lanes widened over time,
allowing for more ages and occupations to be eligible for the COVID-19 vaccine. On April 5,
2021, the lane system was phased out and the COVID-19 vaccine was made widely available to
the general public, anyone above the age of 16 in Nevada.
Though appointment availability had increased in southern Nevada’s mass vaccination sites,
vaccination appointments being made by the Latinx/Hispanic populations did not show an
increase. Community partners, trusted and embedded within the Latinx/Hispanic community,
identified a number of issues that were creating barriers to vaccine access for Latinx/Hispanic
and Spanish speaking communities.
These barriers include, difficulty accessing the online appointment system due to a lack of
access to technology; lack of internet access; inability to operate digital devices; limited in-
language educational resources; and few to no resources for those with low reading or writing
proficiency. Additionally, a fear of exposing immigration status to the government is also a
significant deterrent.
For those attendees who created an appointment and showed up for their vaccine, some felt
apprehensive and turned down the opportunity when asked for a form of Nevada ID, a health
insurance card, or saw that the medical application included a section to include a social
security number.
After learning about these experiences, it became clear there was a need for culturally sensitive
COVID-19 vaccine outreach and clinics to serve hesitant, marginalized populations.
This led to the creation of a community clinic, organized with the help of various community
partners, directly addressing barriers to access. The goal of the clinic was to drive clinic
attendance, successfully administer COVID-19 vaccines, and connect participants with
resources such as food assistance and access to community support agencies.
This clinic eliminated appointment scheduling, the requirement to show a photo ID or give a
social security number, and questions about health insurance. The clinic was staffed by
Spanish speaking staff and volunteers who assisted attendees with medical screening forms,
the registration application, and answered questions regarding the vaccination process.
PAGE 22ORGANIZING PARTNERS: FOOD DISTRIBUTION PARTNER:
• Puentes • Culinary Academy of Las Vegas
• Arriba Las Vegas • Nevada Minority Health and Equity Coalition
• Nevada Vaccine Equity Collaborative
OUTREACH PARTNERS:
• Anthem VACCINATION PARTNERS:
• CARE Coalition • Immunize Nevada
• Health Plan of Nevada • Albertsons Pharmacy
• Liberty Dental • UNLV School of Medicine – Dr. Culley
• Nevada Health Centers
• Nevada Minority Health and Equity
Coalition
• Nevada Wheelchair Foundation
• UnitedHealthcare, D-SNP
• UNLV Community Clinic
• UNLV School of Public Health
PRE-EVENT PLANNING:
The goal of the community clinic was to ensure attendees felt safe, welcome, and able
to completes the process of receiving a COVID-19 vaccine in the language they felt most
comfortable with.
To accomplish the goal, we ensured each attendee had access to a Spanish speaking guide or a
Spanish speaking volunteer who could assist them at every step of the process.
It was important to establish line management in the planning phase to ensure that the clinic did
not exceed the capacity limits for the designated space at any given time. This was facilitated by
the use of an attendee counter at clinic registration.
It is important to note that event volunteers for these events may require training or guidance
before the event . In some situations, volunteers will need to meet the literacy needs of
participants, which may mean reading the questions aloud to the participant and helping them
complete the application form.
Planning events in southern Nevada must take the weather and high temperatures into
consideration. Waiting in line outside is not a tenable option.
DAY OF PLANNING:
Ensuring you have delineated roles and times for check in/check out for volunteers, as well as
provide them with refreshments and appropriate breaks.
BLISS REQUA-TRAUTZ, EXECUTIVE DIRECTOR
ARRIBA LAS VEGAS WORKERS CENTER
I think it’s important here to note the resources and relationships utilized to achieve these
results. We’ve talked about removing barriers to access, and some about relying on the trust
organizations build with the community, but we are also spending staff time and resources and
utilizing existing institutional infrastructure to get this level of turnout.
PAGE 23GUY GIRARDIN, PRESIDENT
PUENTES
A lot of organizations are very enthusiastic and want to serve, but these events don’t happen on
their own, both with respect to planning and execution. I’d caution anyone who relies on a “build it
and they will come” approach.
I’d also caution organizations to not underestimate the volunteer/staffing requirement. As came
out in our debriefing, we thought we could use more, and that was with having 50+ present.
EVENT PROMOTION AND MARKETING:
The event was promoted through the established audiences that Arriba Las Vegas, Puentes, and
Mater Academy regularly serve. Outreach was done within Mater Academy, notifying students and
their families of the event details and information regarding the COVID-19 vaccine.
As explained by Guy Girardin, President of Puentes, “To a very large extent, the numbers we
realized were due to Bliss’ and Mater Academy’s ability to reach out to the hundreds, if not
thousands, of contacts and personal relationships they have in the community, as well as the
outreach networks and capabilities we’ve all developed.” Again, advocate for the behind-the-
scenes work that must be done.
A pop-up clinic with no previous marketing or educational efforts may not be successful.
Attendees want to know who will attend these clinics, what the process will look like, what will be
asked of them, and what vaccine will be administered on the day of the clinic.
SUGGESTIONS FOR FUTURE CLINICS:
Be aware of event costs, both in money and time. Take into consideration the overhead for staff,
volunteer hours, total hours of vaccinators. It takes much organizing, planning, and community
outreach to ensure success of these events. This may require organizers to quantify payroll costs,
volunteers’ hours, and event space costs vs. space that is donated. Also ensure volunteers are
trained, culturally competent, informed about basic vaccine information, know how to fill out forms/
applications, and can assist those with low literacy levels in a sensitive and appropriate way.
Strategically locate your waiting zone. After receiving a COVID-19 vaccine, it is recommended the
patient wait 15 minutes after to ensure they are feeling well and have access to medical attention,
if needed. The 15-minute waiting period for this event happened indoors. Having a section outside
where the outreach vendors could have passed out materials and answered questions while the
patients sat for 15 minutes may have improved line flow.
Be aware of technical glitches. An event volunteer followed the GPS guidance of their mobile
device to the location of the event. The specific location where the event took place, Mater
Academy, has two locations located within a mile of one other. Some attendees arrived at the
second location where a line was forming to receive the vaccine. A volunteer guided those
attendees to the correct location that was up the street. A sign was made to hang on the door
of the second location. Review GPS technology beforehand to ensure participants are correctly
guided to the clinic site. On the marketing materials, consider including the nearest bus route
number and cross streets.
Prepare for unforeseen vaccine updates and procedures. Unfortunately, the day after this clinic,
PAGE 24news was released claiming the Janssen/Johnson & Johnson vaccine had led to a medical
complication in several women across the country. There was a lack of vaccine information
to follow up with the community partners and the clinic attendees. Vaccine partners can work
to ensure that all clinic organizers have access to trusted resources in case of an emergency
response situation.
CONCLUSION:
The high participation for the event is tied to two main points. The first is the outreach effort
that was made by the organizing partners. They are a trusted source to give out information
regarding the vaccine and are trusted messengers when advocating for getting vaccinated and
explaining its importance.
The second is ensuring participants knew they could engage with the event in their preferred
language, in this case Spanish. Participants were advised beforehand that no ID, health
insurance, or social security number would be required or inquired about.
RESULTS:
~470 vaccines were administered of the Janssen / Johnson & Johnson vaccine.
450, 30-pound boxes of groceries, and 300 prepared meals were distributed.
PAGE 25Appendix B
Creating an Accessible Vaccine Experience for People
with Disabilities and Older Adults
Federal law requires that all public spaces, such as public health buildings, convention centers,
fairgrounds, doctor’s offices, pharmacies, and other businesses comply with the Americans with
Disabilities Act (ADA) to protect people from discrimination based on their disabilities.
Vaccination clinics must comply with the ADA. Any entity operating a vaccine clinic should have
policies and procedures in place that include how it will serve people with disabilities, including
steps to provide reasonable accommodations, to communicate effectively with people with
disabilities, and a process for receiving and responding to ADA complaints.
Reasonable accommodation needs will vary from site to site, and for different individuals. Vaccine
clinics should consider that people who are needing to access vaccinations will have a wide range
of disabilities and many different access and accommodation needs. They may be deaf or hard
of hearing. They may experience blindness or low vision. They may have an intellectual disability
or cognitive impairment that impacts understanding of clinic process and procedures. They may
use a wheelchair or other mobility devices. They may experience low stamina or fatigue, mental
health conditions or behavioral support needs that may impact their ability to stand in line for long
periods of time. They may require personal supports or assistance from a caregiver or companion
throughout the process.
What is central to success is creating the opportunity for vaccine clinics to be physically and
programmatically accessible (including scheduling and transportation considerations.) Clinic
organizers should address communication and support needs, ensure volunteers and staff have
information or training related to assisting people with disabilities, and develop a process for
setting up vaccine appointments that meet the needs of people with disabilities and older adults.
In many areas of the country, setting up vaccine appointments has become a significant barrier
for people with disabilities and older adults, with inaccessible or confusing websites, complex
registration processes, QR codes or other technologies that assume participants have access
to a smart phone or broadband, and/or limited outreach to individuals who may not rely upon
electronic forms of communication. Making registration and scheduling as straightforward as
possible can improve access for everyone, not just people with disabilities and older adults.
Partnering with local disability and aging organizations is an effective approach that can
ensure better access to vaccinations for these important-to-serve individuals.
They can assist in understanding the needs of people with disabilities and older adults,
including vaccine site design and implementation decisions.
PAGE 26ACCESSIBILITY COMMUNICATION APPOINTMENTS
• Choose a centrally-located site • Offer readily-available staff • Allow for multiple scheduling
that is physically accessible (e.g. or volunteers to assist with options: phone, website, direct
level ground without slopes, zero- reading forms or documents assistance.
step, spacious), and that people for individuals who may require • Ensure that websites and apps
can reach by mass transit. assistance with seeing, reading, or are 508-compliant and accessible
• Coordinate with accessible comprehending. to people with various types
transportation providers to offer • Include American Sign Language of reasonable accommodation
low or no cost transportation to (ASL) Interpretation along with needs, including people using
vaccine sites for appointment. other language interpretation assistive technologies and
• Reserve adequate parking near available at the site. screen readers.
the entrance (in addition to • Offer staff or volunteers clear face • Minimize documentation and
accessible spaces) for people with coverings to assist people who identification requirements
disabilities and their supports, and depend on speechreading. to demonstrate eligibility.
offer a drop off zone that allows for • Provide clear and easy-to-read Communicate any expectations
minimal walking. external signage with photos/ prior to the appointment clearly
• Provide an accessible, clearly graphics indicating path to and simply.
marked “ADA/Accessible” accessible entrance/exits. • Allow for “group” scheduling –
entrance with assisters available, • Provide additional signage for example, people from the
allowing entrants to bypass waiting indicating elevator priority for same household or people with
in line (including people whose people with disabilities and older disabilities and older adults
disabilities may not be apparent). adults. with their caregivers or home
• Maintain pathways to and from the • Provide signage regarding wait health workers.
vaccine site and within the facility times, for example: your wait time • Support and engage existing
with clear, wide, level access (free is 15 minutes. community-based organizations
of snow, leaves, orange cones, or • Have a clear, publicly posted serving people with disabilities
other debris) for people who use policy recognizing that people with and/or older adults as partners
wheelchairs and other mobility disabilities have the option to bring to assist in outreach and
devices, avoiding steps and stairs. a support person with them at all implementation efforts, and to
• If doors do not include power stages of the process. identify solutions in collaboration
openers, leave doors propped to provide a more accessible
• Post clearly marked signage and
open or provide staff or volunteers experience for individuals with
information in plain language and
to open doors. disabilities and older adults.
translated to reflect the language
• Ensure elevator access is available needs of the community for people
and prioritized for people with seeking assistance to find help,
disabilities and older adults. and ensure an adequate number of
• Ensure that staff and volunteers trained “assisters” available.
have a basic understanding or • Post signage and/or graphics
access to information regarding clearly indicating the accessible
reasonable accommodations, path of travel outside and inside
including service animals. building for individuals who
• Modify mask requirements for use wheelchairs or other
those individuals whose disabilities mobility devices.
prevent them from wearing a
face covering and ensure staff/
volunteers understand this
accommodation.
• Offer a “quiet room” space for
individuals to wait in line, receive
vaccines, and for the post
vaccine observation period, for
those who cannot tolerate large,
noisy spaces.
• Have wheelchairs, including
bariatric chairs, available for
people who have mobility
disabilities or experience fatigue.
• Ensure staff/volunteers are trained
to accommodate individuals with
non-apparent disabilities.
• Have simple, plain-language
explanatory materials on hand.
• Have large print and Braille
versions of all written materials
available.
PAGE 27You can also read