Meeting of the North Carolina Child Fatality Task Force September 20, 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Meeting of the North Carolina Child Fatality Task Force September 20, 2021
Roll Call Attendance & Approval of Minutes Minutes from last meeting on 1-11-21 have been posted on the CFTF website, the link has been sent out and is also linked to on your agenda.
COVID-19 and Children
Elizabeth Cuervo Tilson, MD, MPH
State Health Director
Chief Medical Officer
Child Fatality Task Force
September 20, 2021
NC DHHS COVID – 19 Response
Four Key Metrics – All Quickly Rising
Daily Cases by Date Reported Positive Tests as a Percent of Total Tests
What Percentage of ED Visits this Season are for
Daily Number of People Currently Hospitalized COVID-like Illness Compared to Previous Seasons?
Source: https://covid19.ncdhhs.gov/dashboard
North Carolina Department of Health and Human Services 4
Case Rates Increasing Statewide https://covid.cdc.gov/covid-data-tracker/#county-view
Delta variant is the most common variant in NC Spreads easily because it's highly contagious North Carolina Department of Health and Human Services 6

Case Rates Declining, but
Children age 0-17 years have highest case rates for first time in pandemic
COVID Cases per 100K Population by Age Group and Report Date
Case Rates Highest for School Aged Children
High school and middle school highest among school aged children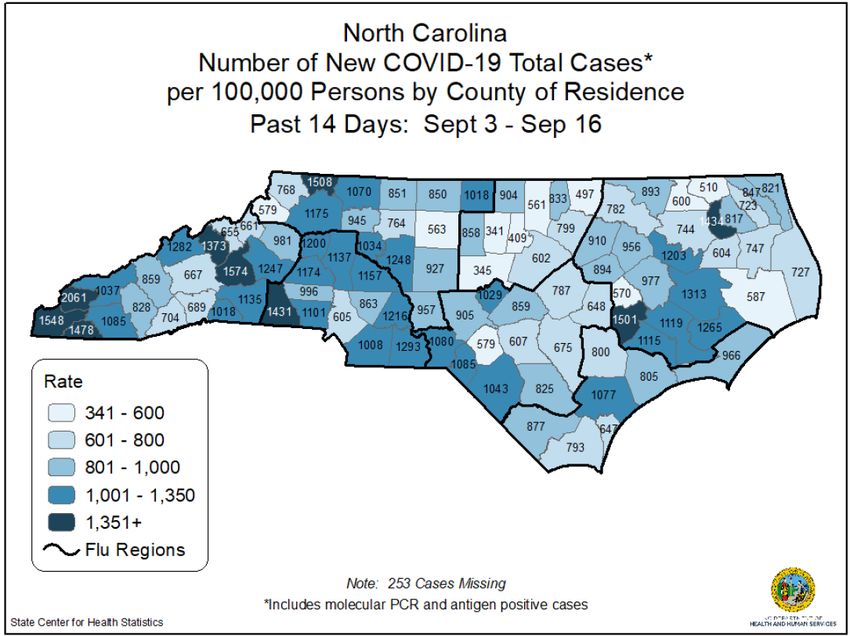
PCR Test Positivity Highest in Children
Test positivity rates have plateaued in recent weeks
across most age groups; remain highest for children.
Percent of ED Visits for CLI
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
9/26/2020
10/3/2020
Source: NC DETECT
Generated: 09/13/21
10/10/2020
10/17/2020
10/24/2020
10/31/2020
11/7/2020
11/14/2020
11/21/2020
11/28/2020
12/5/2020
12/12/2020
12/19/2020
12/26/2020
1/2/2021
1/9/2021
1/16/2021
1/23/2021
1/30/2021
0-18
2/6/2021
2/13/2021
2/20/2021
19-24
2/27/2021
3/6/2021
3/13/2021
25-44
3/20/2021
3/27/2021
Week Ending Date
4/3/2021
45-64
4/10/2021
4/17/2021
4/24/2021
65+
5/1/2021
5/8/2021
5/15/2021
5/22/2021
5/29/2021
6/5/2021
6/12/2021
Percent of NC ED Visits for COVID-Like-Illness (Not Flu) Within Each Age Group by Week
6/19/2021
6/26/2021
7/3/2021
7/10/2021
7/17/2021
7/24/2021
7/31/2021
8/7/2021
8/14/2021
8/21/2021
8/28/2021
9/4/2021
9/11/2021Pediatric Hospitalizations in Southeastern United States
https://covid.cdc.gov/covid-data-tracker/#new-hospital-admissionsMulti-System Inflammatory Syndrome in Children (MIS0C)
https://covid19.ncdhhs.gov/dashboard/cli-surveillance
North Carolina Department of Health and Human Services 12Children can transmit to others – including
adults at higher risk – Teachers, staff, family members
Record Number of Cases in K12 Clusters
Cases Linked with Any Educational Cluster K-12 Cluster Metrics
Child Care Camp K12 School College/University
800 Since June 2020, there have been 462 K-12
clusters
700
– 362 at public schools
600
– 100 at private schools
500
There are currently 192 active clusters
Cases
400
– 178 at public schools
300
– 14 at private schools
200
In total, there are 4,277 cases associated with
100 all K-12 clusters
0 – 3,387 cases among students
– 890 cases among staff
– 3,194 cases at public schools
Week of Illness Identification – 1,083 cases at private schoolsMULTI-LAYERED PROTECTION CAN GREATLY REDUCE RISK OF
SPREAD
14Vaccines are Working
People who are fully vaccinated are 3.96 times less likely to be get COVID-19 and
more than 13 times less likely to die from COVID-19.
Age-Adjusted Case and Mortality Rates in Vaccinated vs. Unvaccinated Populations
incomplete
Data in shaded area may be
Cases Deaths
incomplete
Data in shaded area may be
7
600
6
Attack Rate per 100,000
Death Rate per 100,000
5
400
4
3
200 2
1
0 0
Week End Date Week End Date
Age Adjusted Attack Rate in Unvaccinated Age Adjusted Attack Rate in Vaccinated Age Adjusted Death Rate in Vaccinated Age Adjusted Death Rate in Unvaccinated
Attack Rate Ratio (week ending 8/28): 3.96 Death Rate Ratio (week ending 8/28): 13.47VACCINATION STATUS BY AGE
0-12 years – 0%
Not currently eligible for
vaccination
https://covid19.ncdhhs.gov/dashboard/vaccinations 16North Carolina Department of Health and Human Services 17
Q&A
Science Brief: Transmission of SARS-CoV-2 in K-12 Schools and Early Care and Education Programs – Updated
NC DHHS COVID – 19 Response 27NC Department of Health and Human Services
Injury Surveillance Update
Child Fatality Task Force
Shana Geary, MPH
NC Division of Public Health
September 20, 2021
NCDHHS Division of Public Health| Safe States Annual Conf| September 10, 2020 19Outline
• Overall Child (ages 0-17) Injury Trends
• Child Injury Deaths and ED visits by injury type
• Motor vehicle traffic (MVT) injuries
• Firearm
• Self-inflicted/Suicide
• Unintentional medication/drug overdose
• Child maltreatment
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 20Overall Injury Trends NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 21
There were 319 child injury deaths in 2020*, a
15% increase from 2019 (n=277).
Note: 2020 data are provisional
Number of
Child Deaths 2019 2020*
45
40
35
30
25
20
15
10
5
0
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total Child Injury Deaths: 2019 n=277; 2020 n=319
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 22Child firearm deaths almost doubled in 2020*.
Motor vehicle traffic (MVT) deaths decreased.
2019 2020*
MVT - Unintentional 83 63
Firearm - Assault 36 64
Suffocation - Unintentional 35 34
Firearm - Self-Inflicted 15 31
Drowning - Unintentional 25 18
Suffocation - Self-Inflicted 18 21
Poisoning - Unintentional 8 15
Unspecified - Assault 10 8
Other 47 65
Total Child Injury Deaths: 2019 n=277; 2020 n=319
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 23NC experienced a 18% decrease in overall ED
visits between 2019 and 2020
There are known data quality gaps for May-June 2021 that are impacting
the shown trends. Interpret the data for these months with caution
Note: Provisional 2020 and 2021 data as of 9/13/2021, limited to NC residents
Weeks begin at 01/01 and end at 12/30 for 2019 and 12/29 for 2020
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 24There was a 31% decrease in injury ED visits
among children (0-17) between 2019-2020.
There are known data quality gaps for May-June 2021 that are impacting
the shown trends. Interpret the data for these months with caution
Total Child Injury ED Visits: 2019 n=191,531; 2020 n=132,937
Note: Provisional 2020 and 2021 data as of 9/13/2021, limited to NC residents ages 0-17
Weeks begin at 01/01 and end at 12/30 for 2019 and 12/29 for 2020
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 25The number of child injury ED visits decreased
across all injury categories in 2020.
2019 Child Injury ED Visits 2020* Child Injury ED Visits
Fall - Unintentional 40,292 26,427
MVT - Unintentional 17,518 12,457
Struck By/Against - Unintentional 18,902 10,062
Unspecified - Unintentional 16,530 9,621
Natural/Environmental - Unintentional 11,428 7,613
Cut/Pierce - Unintentional 5,998 4,891
Overexertion - Unintentional 6,084 3,370
Poisoning - Unintentional 3,149 2,667
Other 26,219 21,679
Total Child Injury ED Visits: 2019 n=191,531; 2020 n=132,937
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC DETECT ED Visit Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 26MVT Injuries NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 27
Child MVT Deaths decreased by 32% in 2020.
Most deaths were among children ages 15-17 and males.
Number of child MVT deaths by age and sex
2019 2020
41 42
40
38
32
23
17
14 14 13
10
7
0-4 5-9 10-14 15-17 Female Male
Total Child MVT Deaths: 2019 n=83; 2020 n=63
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 28Most MVT deaths were among white children.
The Hispanic MVT death rate increased in 2020.
Number of Child MVT Deaths Rate per 100,000
2019 2020* 5.0
42
NH White 29 4.0
26 Hispanic
NH Black 17 3.0 NH Black
10 NH White
Hispanic 13 2.0
2
NH Asian 1.0
1 0.0
NH AI/AN 4
2019 2020*
2
Unknown
Total Child MVT Deaths: 2019 n=83; 2020 n=63; NH – non-Hispanic
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 29The proportion of child MVT ED visits has
increased in 2021.
% of Child Injury
ED Visits 2019 2020* 2021*
18.0%
16.0%
14.0%
12.0%
10.0%
8.0%
6.0%
4.0%
2.0%
0.0%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total Child MVT Injury ED Visits: 2019 n=17,537; 2020 n=12,468
Note: 2020 Provisional Data as of 8/10/2020; Data limited to North Carolina residents ages 0-17
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 30Firearm Injuries NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 31
Child firearm deaths increased by 88% in 2020
Most deaths were homicides followed by suicides.
2019 Child Firearm Deaths 2020* Child Firearm Deaths
Assault 36 64
Self-Inflicted 15 31
Unintentional 4 9
Undetermined 1 1
Total Child Firearm Deaths: 2019 n=56; 2020 n=105
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 32The number of child firearm deaths among
ages 15-17 almost doubled in 2020.
Most deaths were among males.
Number of child firearm deaths by age and sex
2019 2020
86
66
47
34
25
19
14
8 6 9
4 4
0-4 5-9 10-14 15-17 Female Male
Total Child Firearm Deaths: 2019 n=56; 2020 n=105
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 33The number of firearm deaths tripled among NH
white children in 2020*. Rates increased the most
among NH Black children.
Number of child firearm deaths Rate of child firearm deaths per 100,000
2019 2020* 10.0
7 NH Black
Hispanic 10 8.0
14
White NH 42 6.0
33
Black NH 4.0
49 NH White
AI/AN NH
2 Hispanic
2.0
0
Asian NH 0.0
3
2019 2020*
0
Other NH
Total Child Firearm Deaths: 2019 n=56; 2020 n=105; NH – non-Hispanic
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 34The proportion of child firearm injury ED visits
increased by 89% between 2019 and 2020.
% of Child Injury
ED Visits 2019 2020* 2021*
0.6%
0.5%
0.4%
0.3%
0.2%
0.1%
0.0%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total Child Firearm Injury ED Visits: 2019 n=334; 2020 n=438
Note: 2020 Provisional Data as of 8/10/2020; Data limited to North Carolina residents ages 0-17
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 35Most child ED visits for firearm injuries
were unintentional.
Percentage of child firearm injury ED visits Percentage of 2020* child firearm
2019 2020* injury ED visits by age and sex
77% 0-4 7%
Unintentional
82% 5-9 6%
21% 10-14 19%
Assault
14%
15-17 68%
1%
Self-Inflicted
1%
Female 16%
2%
Undetermined
2% Male 83%
Total Child Firearm Injury ED Visits: 2019 n=334; 2020 n=438
Note: 2020 Provisional Data as of 8/10/2020; Data limited to North Carolina residents ages 0-17
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 36NC Firearm Injury Surveillance Through Emergency
Rooms (FASTER)
• NC one of 10 states funded for enhanced
surveillance of non-fatal firearm injuries.
• Goals of NC-FASTER:
1. Increase the timeliness of aggregate reporting of
ED visits for nonfatal firearm injuries.
2. Disseminate surveillance findings to key partners
working to prevent or respond to firearm injuries.
NCDHHS, Division | Suicide and Self-Inflicted Injury Update | 3/5/2021 37Suicide and
Self-Inflicted Injuries
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 38Child Suicide deaths increased by 53% in 2020.
Most deaths involved firearms followed by suffocation.
2019 Child Suicide Deaths 2020* Child Suicide Deaths
Firearm 15 31
Suffocation 18 20
Poisoning 1 3
Other 2 1
Total Child Suicide Deaths: 2019 n=36; 2020 n=55
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 39Most suicide deaths were among children
ages 15-17 and males.
Number of child firearm deaths by age and sex
2019 2020*
38
35
27
20 21
17
15
9
10-14 15-17 Female Male
Total Child Suicide Deaths: 2019 n=36; 2020 n=55
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 40The number of suicide deaths almost doubled
for NH white children in 2020*.
2019 Child Suicide Deaths 2020* Child Suicide Deaths
6 Hispanic 3
20 White NH 37
8 Black NH 9
2 AI/AN NH 1
Asian NH 4
Other NH 1
Total Child Suicide Deaths: 2019 n=36; 2020 n=55; NH – non-Hispanic
*2020 Provisional Data as of 9/1/2021; Data limited to North Carolina residents ages 0-17
Source: NC State Center for Health Statistics Death Certificate Data, 2019-2020
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 41The proportion of child self-inflicted injury ED
visits increased by 44% between 2019 and 2020.
% of Child Injury
ED Visits 2019 2020* 2021*
5.0%
4.0%
3.0%
2.0%
1.0%
0.0%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total Child Self-Inflicted Injury ED Visits: 2019 n=2,742; 2020 n=2,745
Note: 2020 Provisional Data as of 8/10/2020; Data limited to North Carolina residents ages 0-17
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 42Medication/Drug
Overdose
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 43The proportion of unintentional med/drug overdose
ED visits among children 15-17 increased by 43%
between 2019 and 2020.
% of Child Injury
ED Visits 2019 2020* 2021*
3.0%
2.5%
2.0%
1.5%
1.0%
0.5%
0.0%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Total Unintentional Med/Drug Overdose ED Visits: 2019 n=366; 2020
n=352
Note: 2020 Provisional Data as of 8/10/2020; Data limited to North Carolina residents ages 15-17
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 44Child Maltreatment NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 45
The proportion of child abuse/neglect* ED visits
increased by 24% between 2019 and 2020.
% of Child Injury
ED Visits 2019 2020* 2021*
2.5%
2.0%
1.5%
1.0%
0.5%
0.0%
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
*Total Child Abuse/Neglect ED Visits: 2019 n=1,968; 2020 n=1,698; includes suspected or confirmed abuse/neglect
Note: 2020 Provisional Data as of 8/10/2020; Data limited to North Carolina residents ages 0-17
Source: NC DETECT ED Visits, 2019-2021
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 46Questions?
Shana Geary
Shana.Geary@dhhs.nc.gov
Scott Proescholdbell
Scott.Proescholdbell@dhhs.nc.gov
www.injuryfreenc.ncdhhs.gov
NCDHHS, Division of Public Health | CFTF Injury Surveillance Update | September 20, 2021 47Review of 2021 CFTF Legislative Action Agenda Items and Legislative Update Karen McLeod, MSW Chair, Child Fatality Task Force
The recommendations addressed in the
bill involve agency action, changes in
law, new state funding to do the
following:
• Create a State Office of Child Fatality
Prevention to put state support for
Child Fatality • SB 703 addresses CFTF system all in one place to coordinate
and support local teams, data, and
recommendations whole CFP System.
Prevention • Sponsors are Sen. • Implement a centralized electronic
data and information system that
System Edwards, Sen. Bergin includes NC joining 45 other states in
a national electronic data system.
Strengthening • SB 703 is in the Senate • Reduce the volume of team reviews
to focus on certain categories most
Rules Committee and likely to yield prevention
has not received a opportunities.
hearing • Reduce the number and types of
teams performing fatality reviews by
combining the functions of the four
• Funding is not in House current types of teams into one local
or Senate budget team.
• Formalize Task Force functioning and
expand reporting by the Task Force.
• Appropriate funding to support this
restructuring and system work.A FEW DATA POINTS:
• From 2010 to 2019 (ten years),
460 child deaths in NC due to
firearm injury (age 17 and
Statewide • Addressed in HB 427;
sponsors are Rep.
younger)
• From 2016 to 2019 (five years),
Firearm Safe Hanig, Carter, C. Smith
437 hospitalizations & 1,246 ED
visits
Storage
• In NC, firearms are used in
• Passed House on a vote almost half of youth suicides
of 116 to 1 • More than 75% of guns used in
Awareness • HB 427 is included in
suicide attempts and
unintentional injuries of kids
Initiative the House version of
the budget; not
were stored in the home of the
victim, relative, or a friend
(national study)
included in Senate • Dramatic rise in gun purchases
version in 2020
• Appears to be significant rise in
firearm-related deaths to
children in 2020 (based on
provisional data; final 2020 data
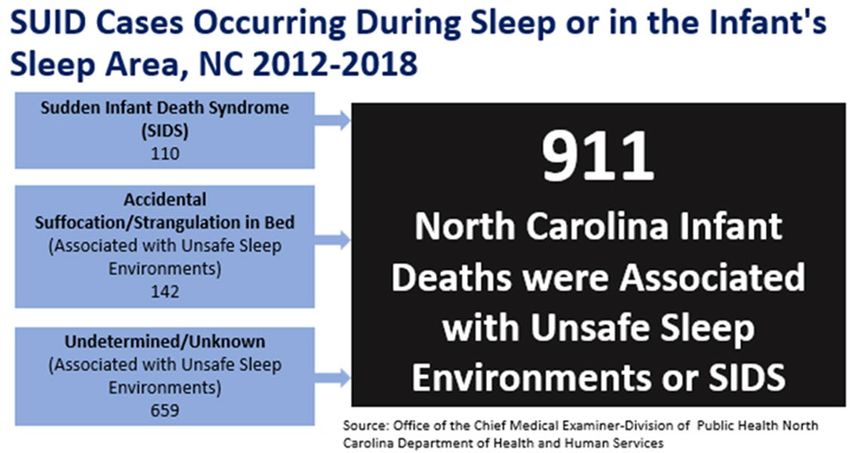
not yet available)Funding to Prevent Infant Deaths Associated
with Unsafe Sleep Environments
• SB 537 addressed this CFTF
recommendation for
additional $85K (current
funding is only $45K)
• Sponsors are Sen. Bergin,
Sen Krawiec
• SB 537 did not get a
hearing; funding is not
included in House or
Senate budgetCFTF recommendations were
for changes in law to make it
• HB 473 addresses CFTF more likely the law will be
recommendations; used in circumstances for
Strengthen sponsored by Rep.
which it was intended to
protect a newborn infant at
White, Rep. Bradford,
Infant Safe Rep. Riddell
risk of abandonment or harm
by making legislative changes
to accomplish the following:
Surrender • HB 473 passed the 1) remove “any adult” from
House unanimously and
Law is currently in Senate
those designated to accept a
surrendered infant;
Rules (no funding in this 2) provide information to a
bill) surrendering parent;
3) strengthen protection of a
• SB 535, nearly identical surrendering parent’s identity;
to HB 473, sponsored 4) incorporate steps to help
by Sen. Burgin, Sen. ensure the law is only applied
Krawiec; no hearing when criteria are met.Funding to
increase the
number of school
nurses, social
workers,
counselors,
psychologists to
move toward
nationally • Senate budget appropriates recurring funding for 115
recommended additional school psychologists
ratios • House budget includes $1.7 million to establish a school
psychologist grant program
• No recurring funding in either House or Senate budget
to increase number of school nurses, social workers,
counselorsLegislation that • No bill introduced.
would add child • Bill that relates to child abuse and neglect
abuse and reporting (not CFTF-related) is SB 693 which
became Session Law 2021-132 and requires:
neglect reporting
• DHHS to develop a plan to create and
requirements to implement a statewide child protective
topic list for services hotline
required mental • Public schools to provide students with
information and resources on child abuse
health training and neglect via a document provided to
for school students yearly and displays posted
throughout schools
personnelLegislation • HB 402 = SB 183 – bills do not expand the
use of ignition interlocks to all DWI offenders
that would as recommended by the CFTF but the bills
would require studying the issue of
require expanded use.
ignition • House sponsors: Faircloth, Stevens, Clampitt;
Senate sponsors: Britt, Sawyer, Daniel
interlocks for • S 183 passed the Senate and is now in House
Rules Committee after a favorable report
all DWI from Judiciary 1.
offenders • H 402 has passed the House and is currently
in the Senate Transportation Committee
after a favorable report from Judiciary.Tobacco
prevention • House budget provides funds from the
funding: NC settlement with Juul Labs, Inc to
DPH for tobacco and nicotine
$7 mil. for dependence prevention activities
youth and targeted at youth and young adults:
$13 million nonrecurring.
$3 mil. for • Not addressed in Senate budget.
Quitline
(endorse)Workplace supports: • S 633 = H 514 addressed pregnancy pregnancy and and lactation accommodations but did lactation not advance, did not make crossover accommodations; • H 875 addressed kin care and safe kin care and safe days leave but did not advance, did days leave not make crossover (endorse)
Highlights of two bills not related to CFTF agenda that impact child deaths & child well-being
Among its provisions:
Session Law 2021-110 (HB • Law allows an immunizing pharmacist to
96) related to pharmacist dispense, deliver, or administer self-
authorization for administered oral or transdermal
contraceptives pursuant to certain
dispensing, delivering, and requirements related to record keeping,
administering certain notification of patient’s provider, etc.
treatment and medications
• Immunizing pharmacist may also
administer to a patient any prescribed,
self-administered injectable medication.
• If pharmacist administers or dispenses a
hormonal contraceptive, the pharmacist
shall counsel the patient about
preventative care . . .Medicaid for
The Senate budget continues
12 months Medicaid coverage for pregnant
postpartum women for 12 months
postpartum.
The House budget does not
include this extension.CFTF Director’s Report
Kella Hatcher, JD
Executive Director, NC
Child Fatality Task ForceAt its core, CFTF work is about MAKING KIDS A PRIORITY
2021 CFTF Annual Report – access on home page of
CFTF website
Represent CFTF in more than a dozen stakeholder
groups/steering committees
Work to advance administrative items on CFTF Action
Highlights Agenda
Child Fatality Prevention System strengthening work
of ED
Activities Presentations, materials, and meetings to educate
about CFTF, CFP System, CFTF recommendations
Legislative education, monitoring, reporting
Media: press inquiries, press releases• Firearm safety/safe storage education and awareness and focus on
social drivers that relate to gun deaths
• Funding to increase numbers of school nurses, social workers,
counselors, psychologists
• Strengthen child abuse and neglect reporting education and
awareness and prioritize resources to strengthen CPS intake and
State Team 2021 assessment
• Expanded efforts to prevent sleep-related infant deaths including
recommendations expanded program funding and a statewide campaign
to be heard in • Support for community-based programs supporting families’ health
committees and well-being through addressing impacts of social determinants of
health
• Focus on upstream issues (ACES/screening/social determinants of
health) in mental health
• Support DPI efforts to implement statewide data system
• Funding for full toxicology in all medical examiner jurisdiction child
fatalities• Strengthen training on child abuse and
neglect awareness and reporting for health
care providers and law enforcement
• Child Passenger Safety Study – Occupant
Protection Task Force
CFTF • Work on rear seat restraints and
Administrative strengthening education for teens/driver ed
Items • Lead suicide prevention coordinator role
• Follow implementation of School Mental
Health Policy related to strengthening
school/community connections to address
student mental healthGoal to have less time spent on
presentations, more time for discussion
Changes in format Committee role in prioritizing issues for
for meetings; study
issue prioritization
and administrative Committees determine 2-3 legislative
recommendations
work
More emphasis on what CFTF can
accomplish administratively (work that
doesn’t involve legislation)Ten minute break!
Committee Reports
Overview of Child Fatality
Prevention System, CFTF Role,
System Strengthening Efforts
Kella Hatcher, JD
Executive Director
NC Child Fatality Task ForceDevelop a communitywide approach to
child abuse and neglect;
Study and understand causes of childhood
Charge of State death;
Child Fatality
Identify gaps in service delivery in systems
Prevention designed to prevent abuse, neglect, and
System [via death; and
Article 14 of NC Make and implement recommendations for
Juvenile Code] laws, rules, and policies that will support
the safe and healthy development of our
children and prevent future child abuse,
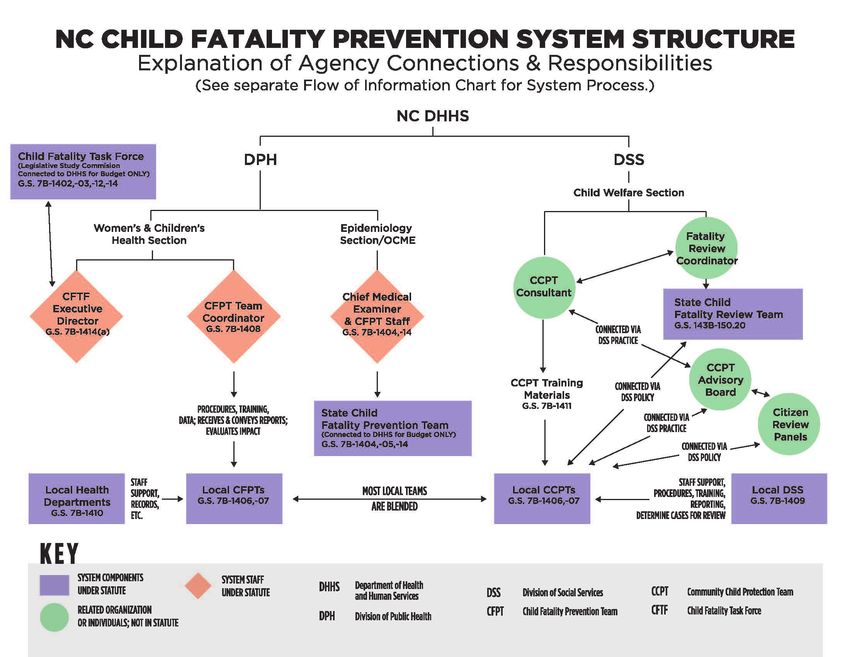
neglect, and death.MAIN COMPONENTS OF CURRENT NC CFP SYSTEM:
FOUR TYPES OF REVIEW TEAMS PLUS TASK FORCE
These three
components State Child
Two Fatality
addressed in
Article 14 of
Types of Uses local team Review
Juvenile Code Local members Team
Review
Teams
This component
State Child addressed in G.S.
Fatality §143B-150.20
Prevention
Team NC Child
Each type of team Fatality One case may be
handles data,
information, and
Task reviewed by
reporting Force three different
differently; minimal types of teams
Policy only; no
data is collected
case reviews• Study, analyze, and report on incidences and
causes of child death
• Develop a system for multidisciplinary review
of child deaths
• Receive and consider reports from State Team
Task Force • Perform other studies and evaluations as
needed in order to carry out its mandate
Responsibilities • Submit annual report to the Governor and
General Assembly with recommendations for
changes to any law, rule, or policy that it has
determined will promote the safety and well-
being of children
[See G.S. §7B-1403, -1412]Current System * Structure *This graphic was created in 2018 and this ED position is now at DHHS
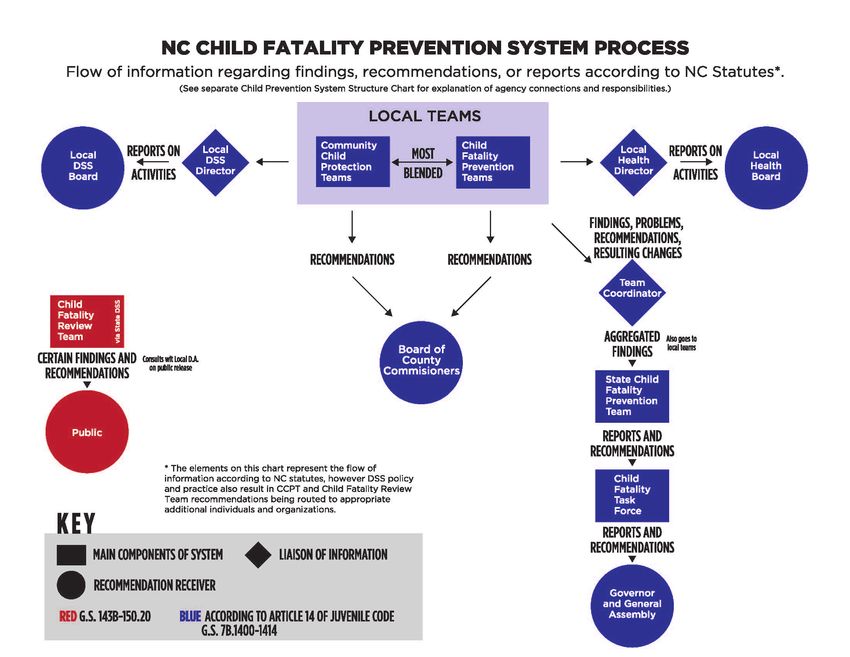
Current System Process
Initial 2017 discussions led to two-day Child Fatality
Prevention System Summit April 2018: gathering of
over 200 people & local team input
Post-Summit work involved research on other states’
CFP systems, consultation with national experts,
stakeholder discussions
Journey of
CFTF recommendations addressing CFP System
CFP strengthening adopted in the Child Welfare Reform
Plan from the Center for Support of Families
Strengthening CFTF recommendations were addressed in 2019
Work Appropriations Act which did not become law (HB 825
was included in HB 966)
NCDHHS has continued work to move
recommendations forward because they are aligned
with DHHS priorities and were part of Child Welfare
Reform Plan; this work has included convening of
stakeholder group by NCIOM• The Task Force met this obligation in the
Why are we (still!) early 1990s when the system was first set
talking about this? up
• Thirty years later (now!) the Task Force
CFP statute says has an important role in ensuring a strong
multidisciplinary review system and
the Task Force effective operation of local teams
shall develop a • A CFP System that is not optimized is a
system for weak link in protecting children from
multidisciplinary child death and maltreatment
review of child • CFP System strengthening
recommendations made by CFTF in 2019,
deaths & study 2020, 2021
the operation of • Legislation has been introduced but has
local teams . . . not advancedSB 703 addresses CFTF recommendations
• Creates a State Office of Child Fatality Prevention (State Office) that brings state-level
support together in one place within DHHS to coordinate and support the work of the
statewide system with an emphasis on supporting local child death review teams;
appropriates recurring funding to establish and operate office and support system.
• Restructures the system of team reviews of child deaths in NC to do the following:
• Combines the functions of the existing four types of review teams into local county
teams & allows counties to choose whether to be a single or multi-county team.
• Allows for the addition of needed experts to participate in a particular review on an ad
hoc basis.
• Eliminates state-level teams while State Office staff and medical examiner child fatality
staff help local teams carry out functions previously performed by state teams.
• Articulates special requirements for the State Office and for local review teams for
reviews of deaths related to abuse or neglect or where a child was known to child
protective services.• Implements a centralized electronic data and information system that includes North Carolina joining 45
other states to participate in the National Child Death Review Case Reporting System (that is web-based
and free to use)
• Requires the Task Force to receive and consider local team information (reports addressing aggregate
data, information, findings and recommendations resulting from local team reviews).
• Changes the types of deaths required to be reviewed to be according to categories of death where
reviews are most likely to yield prevention opportunities; reviews of other deaths optional.
• Formalizes the current structure of the Task Force and expands the scope of its reporting to include the
functioning of the whole CFP System; expands on state leaders who must receive the Task Force report.
• Requires NC DSS to ensure the existence of at least three federally required Citizen Review Panels that
evaluate policies, procedures, and practices of State and local child protection agencies; requires that
panels be operated and managed by organization independent from DSS; requires an annual report by
panels that is made public. [The effect of these provisions is to put federal requirements in state law and
enable DSS to discontinue using all 100 Community Child Protection Teams to satisfy federal requirements
for Citizen Review Panels while ensuring that panels have appropriate access to and protection of
information.]
SB 703 addresses CFTF recommendations (continued)Proposed Model Strengthens Team Reviews, Data, State-level Support, Reporting
Local Review State Office of NC Child
Teams Review info Child Fatality State Office Fatality Task
Counties choose to goes into Prevention
national data
Staff report on Force
be single or multi- Whole-system whole system
system Studies data from
county teams coordination & technical functioning local teams &
support for local teams other sources
One team for all Makes local Aggregate
types of reviews, but reports (e.g. to Centralized Information information & Makes policy
different procedures, County System including use of recs from local recommendations
required participants, Commissioners) national data system teams is & reports on
and degree of state- which also go to reported
Fatality Review & Data whole CFP
level assistance for State CFP
Office Group looks at aggregate system to General
different types of
local team info & OCME Assembly,
reviews (e.g.
info to be liaison of info Governor, other
abuse/neglect or
going to Task Force state leaders
infants).
CAN deaths:
Citizen Review Panels:
7-Day Internal
Evaluates CPS functioning
Reviews by State DSS• OPTIMIZE LOCAL TEAM EFFORTS: CFP State Office structure, and
eliminating duplication supports local teams to optimize work and
Ultimate Goal: facilitate local prevention efforts to save lives and prevent maltreatment.
• DATA TO UNDERSTAND TRENDS: A sophisticated data system that
Prevent Child collects richer layers of data makes reviews more valuable and facilitates
understanding and reacting to what’s happening locally and in NC.
Deaths & • ADDRESSING INFANT MORTALITY: System strengthening involves best
Maltreatment; practice attention to infant deaths at a time when North Carolina’s infant
mortality rate has been among the worst dozen in the nation, disparities
persist, and infant deaths make up two-thirds of all child deaths.
Support Child • ENSURING USE OF INFORMATION LEARNED: Ensuring that
Safety & information/recommendations from reviews reaches appropriate
agencies and leaders is critical to making reviews effective.
Wellbeing • MORE STATE-LEVEL PREVENTION WORK: CFP State Office provides a
structure for facilitating or implementing various prevention initiatives,
including efforts to seek grant opportunities.Local Teams: CCPTs & CFPTs in every county
CCPT Most teams
CFPT
are blended
Must review deaths involving
suspected abuse or neglect Reviews
where there was CPS “additional”
involvement/report within types of deaths
previous 12 mos., as well as when CCPT
selected active CPS cases determines it
will not review
additional
May review “additional” cases
types of deaths
See N.C.G.S §7B-1406• Local Social Services • Guardian ad Litem
Local teams consist • Local Health • Health Care Provider
of community Department • Emergency medical or
leaders; teams are • Law Enforcement firefighter
rich in expertise & • District Attorney • District Court Judge
ripe for • Local Community • County Medical
collaboration Action Agency Examiner
needed to • Local School • Local childcare facility
strengthen health Superintendent or Head Start
and safety in their • County Board of Social • Parent of child who
communities. Services died
• Mental HealthLocal team reports, findings, recommendations
CCPTs Both CFPTs
Activity reports go to Submit any Activity reports go to
local DSS board recommendations to local board of health
BCC rec’s go to NC DSS Board of County Reports on findings and
(per policy) Commissioners (BCC) rec’s from reviews go to
Team Coordinator
End of Year Report to Advocate for system (state-level DPH) who
NC DSS (per policy) improvements and submits aggregated
[Note: no case-specific needed resources findings to State Team
information reported] where gaps and
deficiencies existSupport for Local Teams
CCPTs CFPTs
County DSS Directors provide general Local Health Department Directors
support, procedures, training, reporting, etc. distribute procedures, maintain records,
provide staff support, facilitate reports,
NC Division of Social Services has ongoing etc.
responsibility for training materials for local
CCPTs (a consultant in NC DSS is assigned to A Team Coordinator at NC DPH
this work) By provides general support,
procedures, training, reporting
A CCPT State Advisory Board was formed
by NC DSS and it facilitates CCPT reporting provides statistical information on
aimed at meeting federal law for Citizen child deaths to CFPTs
Review Panels Receives and sends reports from
CFPTs; provides aggregate info to
State CFPTLocal Team Panel Discussion • Jennie Kristiansen, Chatham Co. DSS Director and Chair of combined CCPT/CFPT • Paige Rosemond, Wake Co. Human Services Child Welfare Director, CCPT member • Bruce Robistow, Halifax Co. Health Director and CFPT Chair • George Bryan, Chair of Forsyth Co. CCPT and Chair of CCPT Advisory Board
You can also read

















































