Metformin ! - und dann ? - Therapie des Typ 2 DM: Stefan Bilz Klinik für Endokrinologie/Diabetologie
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Therapie des Typ 2 DM:
Metformin ! – und dann ?
Stefan Bilz
Klinik für Endokrinologie/Diabetologie
stefan.bilz@kssg.ch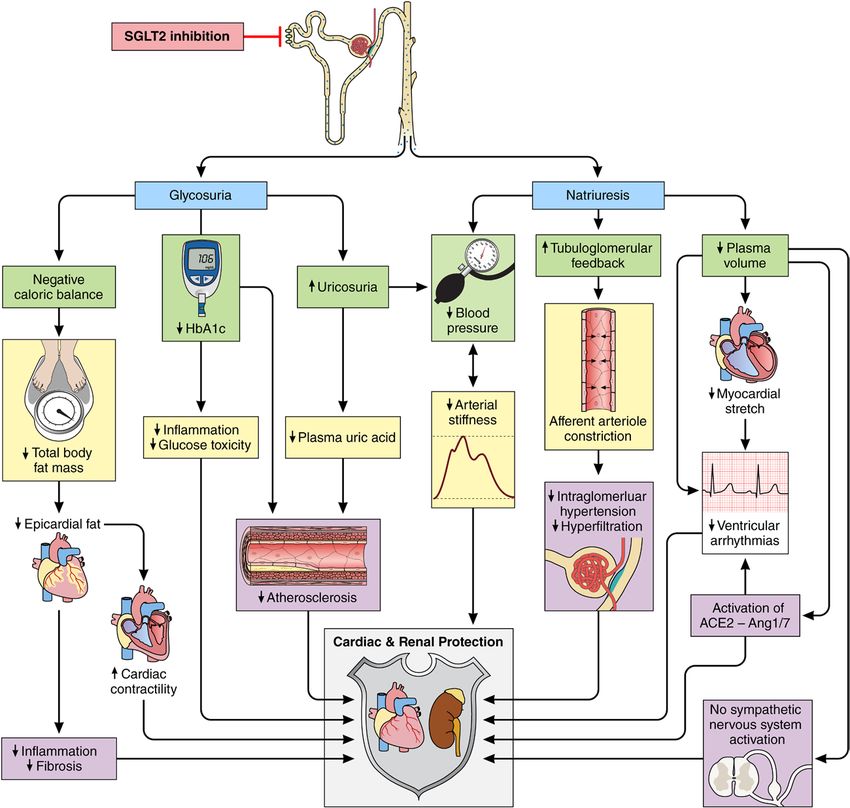
Geschichte .... • DCCT 1993: intensive Diabeteseinstellung verhindert mikrovaskuläre Komplikationen beim Typ 1 DM • UKPDS 1998: intensive Diabeteseinstellung ab Erstdiagnose verhindert mikrovaskuläre Komplikationen beim Typ 2 DM • Steno 2 2003: Multifaktorielle Behandlung aller Risikofaktoren reduziert die kardiovaskuläre Morbidität beim Typ 2 DM • UKPDS Follow-up 2008: anhaltende Reduktion mikrovaskulärer Endpunkte und im Langzeitverlauf makrovaskuläre Risikoreduktion nach intensiver Therapie ab Erstdiagnose beim Typ 2 DM („legacy effect“) • VADT, ADVANCE und ACCORD 2008/9: keine makrovaskuläre Risikoreduktion durch intensive Blutzuckersenkung bei langjährigem Typ 2 DM, Exzessmortalität in der ACCORD-Studie
Glibenclamide
Relative risk (95%
1·24 (1·07–1·44) credible interval)
1·52 (1·13–2·04) I2=75%39,50,51,53,58,64–67
Chlorpropamide 1·34 (0·98–1·86)
I2=89%36,53,58,61–64,66,68
Tolbutamide 1·13 (0·90–1·42)
1·49 (1·29–1·73) Glibenclamide (reference group) Reference
Gliclazide I2=21%53,58,64,66 Glimepiride
1·00 (0·91–1·10) Glipizide 0·98 (0·80–1·19)
I2=46%37,50,51,58,63,65–67 3·52 (3·16–3·91) 0·83 (0·68–1·00)
Glimepiride
I2=68%50,58
Gliclazide 0·65 (0·53–0·79)
2·89 (2·56–3·25)
Das
ReviewAuftreten von Hypoglykämien ist mit einem
1·57 (1·21–2·03) 1·93 (1·56–2·39)
I2=73%50,58
1·32 (1·23–1·40)
0·5 1·0 2·0
schlechten klinischen Outcome assoziiert
I2=60%58 Lower risk than for reference group Higher risk than for reference group
I2=62%58,63,66 I2=0%58
Figure 3: Comparison of all-cause mortality between sulfonylureas using
1·20 (1·14–1·27) 1·68 (1·23–2·28) 1·20 (1·03–1·39)
direct and indirect evidence
I2=0%50,51,58,65–67 I2=78%58,61,68 I2=74%58,61,68 Data are pooled relative risks and 95% credible intervals calculated by network
meta-analysis of direct and indirect evidence from 18 studies.3,34–37,39,50,51,53,58,61–68
Glipizide 1·10 (1·01–1·19) Tolbutamide
I2=0%58
1·42 (0·95–2·12) No severe
Severe Hazard ratio compared with those who did not. This increased risk Relative risk (95%
3·50 (3·10–3·94) hypoglycaemia hypoglycaemia (95% CI) seems to be shared by people with type 1 and type credible 2
I2=82% 3,53,68
interval)
I2=70%50,58 (n=231) (n=10 909)
diabetes, 23
although the magnitude of the risks varies with
Chlorpropamide 1·45 (0·88–2·44)
Major macrovascular events 33 (11·5%) 6·64 (2·00–22·08)
53
1114 (10·2%) 3·76 (2·97–4·76)
3·53 (2·41–5·17) diabetes type, background cardiovascular risk, presence of
Major microvascular events 24 (10.4%) 1107 (10·1%) I =79% 2·19 (1·40–3·45)
2 58 Tolbutamide 1·11 (0·79–1·55)
2·53 (0·80–7·99) comorbidities, severity of hypoglycaemia, temporality of
Death from anyI2=0%
cause53,68 45 (19·5%) 986 (9·0%) 3·27 (2·29–4·65) Glibenclamide (reference group) Reference
hypoglycaemia to the event, length of follow-up, and level
Cardiovascular disease 22 (9·5%) 520 (4·8%) 3·79 (2·36–6·08)
of adjustment for potential confounders. The association1·01 (0·72–1·43)
Glipizide
Non-cardiovascular disease 1·09 (0·95–1·26)
23 (10·0%) 466 (4·3%) 2·80 (1·64–4·79) Glimepirideto hypoglycaemia induced by insulin—a 0·79 (0·57–1·11)
I2=0%34,35,68
is not confined
Chlorpropamide 0·1 1·0
Gliclazide
similar association has been reported for hypoglycaemia0·60 (0·45–0·84)
Metformin 10·0
induced by sulfonylureas.30 Additional post-hoc analyses
Figure 1: Association of severe hypoglycaemia with the risk of an adverse clinical outcome or death 0·1 1·0 10·0
Figure 2: Comparison of all-cause mortality between sulfonylureas using direct evidence in other trials with cardiovascular outcomes have also
The hazard ratio represents the risk of an adverse clinical outcome or death among patients reporting severe Lower risk than for reference group Higher risk than for reference group
Data are taken from 18
hypoglycaemia studieswith
compared thatthose
reported direct evidence
not reporting of the risk of
severe hypoglycaemia. all-cause
The centres ofmortality
the squares foraretwo or more
placed at
raised the likely contribution of confounding as an
sulfonylureas and are compared by meta-analyses. 3,34–37,39,50,51,53,58,61–68
The pooled relative
the point estimates and the horizontal lines represent the corresponding 95% CIs. The area of each square isrisks with 95% CIs are explanation for the association.11,12
reported for each pairwise
proportional comparison.
to the inverse A solid
of the variance lineestimate.
of each shows the association
Reproduced fromisZoungas
statistically
10
et al, signifi cant andofathe
by permission dotted The Figure 4: Comparison
observational natureof cardiovascular-related
of many of the analyses mortality between
and
line shows the association
Massachusetts MedicalisSociety.
not statistically significant. Arrowheads point to the drug with higher risk within each sulfonylureas using direct and indirect
the inability to capture all hypoglycaemic episodes evidence
pair. The number of arrowheads pointing to each drug gives an approximation of the overall risk of mortality (particularly Data aremilder
pooled relative risks and 95% episodes
or asymptomatic credible intervals calculated by network
that might
relative to the others. meta-analysis of direct and indirect evidence from 13 studies.3,34,36,37,39,52,58,61,63,64,66–68
which showed no increase in mortality, the frequency of contribute to cardiovascular events), have made it
severe hypoglycaemia in ACCORD was four to five times difficult to confirm or refute causality, particularly in
higher. The Veteran’s Affairs Diabetes Trial (VADT), relation to cardiovascular events. Nevertheless, results
6 www.thelancet.com/diabetes-endocrinology Published online October 23, 2014 http://dx.doi.org/10.1016/S2213-8587(14)70213-X
which was done over the same period, was underpowered from some studies have shown an association between
to measure the effect of hypoglycaemia on mortality.8 cardiovascular events (particularly myocardial infarction)
Int. Hypoglycemia Study Group, Lancet Diab Endocrinol 7: 385, 2019
However, all three studies showed a significant association and hypoglycaemia;24 the evidence seems less consistent
between severe hypoglycaemia and mortality. In VADT for Simpson SH et al.,
the association Lancet
between Diab Endocrinol
hypoglycaemia and stroke.3: 43, 31 2015
and ADVANCE, severe hypoglycaemia predicted later Therefore, this Review mainly focuses on studies that
mortality (ie, downstream of the hypoglycaemic episode); report links between mortality and severe hypoglycaemia.
in ADVANCE, the median time from severe In most studies, severe hypoglycaemia is defined as
hypoglycaemia to death was 1·05 years. The difference in episodes that require the assistance of another person to
diabetes duration between these later studies and UKPDS recover. However, where reliable studies reporting
might be relevant to their different outcomes since the cardiovascular events were available, these were included.
UKPDS studied those newly diagnosed, whereas the The debate might also be framed by asking whether
Therapie des Typ 2 DM:
HbA1c, Hypoglykämierisiko und Gewicht
HbA1c-Senkung Hypoglykämierisiko Gewichtsveränderung
Prandiales Insulin ↓↓↓ ↑↑↑ ↑↑
Basisinsulin ↓↓↓ ↑ ↑
Sulfonylharnstoffe ↓↓ ↑↑ ↑
Gliclazid ↓↓ ↑ ↑
Metformin ↓↓ ↔ ↔
GLP-1-RA ↓↓ ↔ ↓↓
SGLT2i ↓ ↔ ↓
DPP-IV-Hemmer ↓ ↔ ↔
Glitazone ↓ ↔ ↑Diabetologia (2019) 62:357–369 359
CANVAS Program (CANagliflozin cardioVascular Assessment Study [CANVAS] plus CANVAS-Renal [CANVAS-R])
CV outcome studies of canagliflozin
CARMELINA (CArdiovascular and Renal Microvascular outcomE study with LINAgliptin)
CV outcome study of linagliptin
CAROLINA (CARdiovascular Outcome trial of LINAgliptin versus glimepiride in type 2 diabetes)
CV outcome study of linagliptin vs glimepride
CREDENCE (Canagliflozin and Renal Endpoints in Diabetes with Established Nephropathy Clinical Evaluation)
Kidney outcome study of canagliflozin
DECLARE-TIMI 58 (Dapagliflozin Effect on CardiovascuLAR Events-TIMI 58)
CV outcome study of dapagliflozin
ELIXA (Evaluation of LIXisenatide in Acute Coronary Syndrome)
CV outcome study of lixisenatide
EMPA-REG OUTCOME (Empagliflozin, Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients)
CV outcome study of empagliflozin
EXAMINE (EXamination of cArdiovascular outcoMes with alogliptIN versus standard of carE)
CV outcome study of alogliptin
EXSCEL (EXenatide Study of Cardiovascular Event Lowering)
CV outcome study of exenatide modified release (long-acting)
Harmony Outcome
CV outcome study of albiglutide
LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results)
CV outcome study of liraglutide
PIONEER-6
CV outcome study (phase 3) of oral semaglutide
REWIND (Researching cardiovascular Events with a Weekly INcretin in Diabetes)
CV outcome study of dulaglutide
SAVOR-TIMI 53 (Saxagliptin Assessment of Vascular Outcomes Recorded in patients with diabetes mellitus-TIMI 53)
CV outcome study with saxagliptin
SUSTAIN-6 (Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type
2 Diabetes)
CV outcome study of s.c. semaglutide
TECOS (Trial Evaluating Cardiovascular Outcomes with Sitagliptin)
CV outcome study with sitagliptin
Home P., Diabetologia 62: 357, 2019
presented in the supplementary materials of the original publi- of insulin and high rates of new insulin starters during the
cation and, while the numbers within subgroups provide low study (Table 1), to the extent that it could be argued that the
power, no concerns are obvious [18]. results are only generalisable to insulin-treated populations.
While the three studies of DPP4 inhibitors agree that short- The generalisability issue is further marred by the very high
term (Aktuelle Empfehlungen zur medikamentösen Therapie
des T2 DM (ADA, EASD; Januar 2019)
S94
Pharmacologic Approaches to Glycemic Treatment
Diabetes Care Volume 42, Supplement 1, January 2019
Figure 9.1—Glucose-lowering medication in type 2 diabetes: overall approach. For appropriate context, see Fig. 4.1. ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; CV, cardiovascular;
CVD, cardiovascular disease; CVOTs, cardiovascular outcomes trials; DPP-4i, dipeptidyl peptidase 4 inhibitor; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon-like peptide 1 receptor agonist; HF, heart failure;
SGLT2i, sodium–glucose cotransporter 2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione. Adapted from Davies et al. (39).ocyte concentration and direct toxicity to tency have also been observed in serotonin
the enterocytes. reuptake transporter (SERT) knock-
There are a number of putative mech- out mice (39,40). In addition, a recent
anisms whereby increased luminal met- study from the GoDARTS (Genetics
Figure 2—Association of a GRS derived from
SLC29A4 (PMAT) and SLC22A1 (OCT1) with formin may increase GI intolerance to of Diabetes Audit and Research in
metformin intolerance. Bars indicate SE metformin (outlined in Fig. 3). Firstly, a Tayside Scotland) cohort showed asso-
around the mean. *P , 0.05. higher concentration of metformin in the ciation of a composite SERT genotype, 5-
gut has been shown to inhibit uptake of HTTLPR (5-hydroxy tryptamine [serotonin]
histamine and serotonin, leading to in- transporter-linked polymorphic region)/
creased luminal concentration of these rs25531, with intolerance to metformin
study, we demonstrated a significant biogenic amines (13). Metformin also in subjects with type 2 diabetes (13). In
association of the G allele of an intronic inhibits diamine oxidase, an enzyme this study, carriers of the low-expressing
Gastrointestinale Metforminintoleranz:
SNP, rs3889348, in SLC29A4 encoding
PMAT, with higher odds of GI intolerance
that degrades histamine, at therapeutic
doses (6). Biogenic amines play an im-
portant role in the GI pathophysiology.
SERT S* alleles had .30% increased odds
of metformin intolerance (OR 1.31 [95%
CI 1.02–1.67], P = 0.031). Histamine is a
Genetische Variation für kationische Metformintransporrter und
after metformin therapy. Each copy
of the G allele was associated with Elevated levels of serotonin and hista- monogenic amine stored in the entero-
interferierende Medikamente modifizieren das Risiko signifikant (OR 2-3) !
1.34 times higher odds of metformin mine in the GI tract cause GI symptoms chromaffin-like cells within the gastric
Figure 3—Possible mechanisms for metformin intolerance. A: Metformin is absorbed from the gut lumen via cation transporters such as PMAT, OCT1,
Dawed AY drugs
SERT, and OCT3. B: Increased level of metformin in the gut lumen is observed when metformin is taken with cation transporter-inhibiting et al.:
suchDiabetes
as Care 42:1027, 2019
PPIs, TCAs, and codeine. These drugs competitively inhibit metformin uptake by the cation transporters. Metformin is also shown to inhibit diamine
oxide, an enzyme that metabolizes biogenic amines. In addition, transport capacity of the cation transporters could be reduced in carriers of reduced
function (420del, 61C, 401S in SLC22A1) or low-expressing alleles (rs3889348_G in SLC29A4) and hence increase luminal metformin level. The
increased level of metformin increases the level of biogenic amines, affects the gut microbiota, and elevates bile acid levels. These may cause symptoms
of GI adverse effects.Blutzuckerverlauf
Herr R.W., 1948
Patient:
Wyss 4, Rolando
Druckbereich:
01.03.2012 - 01.04.2019
00:00 - 23:59
ED T2DM 2004, Stoffwechselverschlechterung 2011/12
HbA1c 13.1%
HbA1c 7.4%
HbA1c < 6%
2012 2019
Druckdatum: 12.06.2019 Seite: 1Blutzuckerverlauf
Herr R.W., 1948
Patient:
Wyss 4, Rolando
Druckbereich:
01.03.2012 - 01.04.2019
00:00 - 23:59
ED T2DM 2004, Stoffwechselverschlechterung 2011/12
HbA1c 13.1%
HbA1c 7.4%
HbA1c < 6%
-12 kg Metformin/Sitagliptin
2012 2019
1 Stunde Fitness täglich
Druckdatum: 12.06.2019 Seite: 1Articles
Durability of a primary care-led weight-management
intervention for remission of type 2 diabetes: 2-year results
of the DiRECT open-label, cluster-randomised trial
Michael E J Lean*, Wilma S Leslie, Alison C Barnes, Naomi Brosnahan, George Thom, Louise McCombie, Carl Peters, Sviatlana Zhyzhneuskaya,
Ahmad Al-Mrabeh, Kieren G Hollingsworth, Angela M Rodrigues, Lucia Rehackova, Ashley J Adamson, Falko F Sniehotta, John C Mathers,
Hazel M Ross, Yvonne McIlvenna, Paul Welsh, Sharon Kean, Ian Ford, Alex McConnachie, Claudia-Martina Messow, Naveed Sattar, Roy Taylor*
Einschlusskriterien
Summary Studienprotokoll
Lancet Diabetes Endocrinol Background The DiRECT trial assessed remission of type 2 diabetes during a primary care-led weight-management
• T2 DM, Dauer < 6AtJahre
2019; 7: 344–55
programme. • in
1 year, 68 (46%) of 149 intervention participants were „Counterweight
remission and 36 (24%)plus“ Programm
had achieved at least
Published Online 15 kg weight loss. The aim of this 2-year analysis is to assess the durability of the intervention effect.
• HbA1c
March 6, 2019 6.0-12% • Formula-basierte „very low calorie“ Diät für 3-
http://dx.doi.org/10.1016/
Methods DiRECT is an open-label, cluster-randomised, controlled trial 5 Monate (8 Std.
done at primary Instruktion)
care practices in the UK.
• Keine
S2213-8587(19)30068-3
See Comment page 326
Insulintherapie
Practices were randomly assigned (1:1) via a computer-generated list to provide an integrated structured weight-
management programme
2 (intervention) or best-practice care • in Schrittweise
accordance with Einführung
guidelines Normalkost
(control), with für 1-2
eGFR
• *Contributed > 30
equally
ml/min/m
Human Nutrition,
stratification for study site (Tyneside or Scotland) and practice list Monate
size (>5700 or ≤5700 people). Allocation was
School of Medicine, concealed from 2 the study statisticians; participants, carers, and study research assistants were aware of allocation. We
BMI
•Dentistry 27 –recruited
45 kg/m
and Nursing individuals aged 20–65 years, with less than 6 years’ duration • Strukturierte Unterstützung
of type 2 diabetes, BMI 27–45 kg/m², and not
(Prof M E J Lean MD, receiving insulin between July 25, 2014, and Aug 5, 2016. The intervention consisted of withdrawal of antidiabetes and
bis 24 Monate (30
antihypertensive drugs, total diet replacement (825–853 kcal per dayMin prodietMonat)
W S Leslie PhD,
N Brosnahan PGDip,
formula for 12–20 weeks), stepped food
G Thom•MSc,Randomisierung
L McCombie BSc) reintroduction von ca. 20% der gescreenten
(2–8 weeks), and then structured support for weight-loss maintenance. The coprimary outcomes,
and Institute of Cardiovascular analysed hierarchically in the intention-to-treat population at 24•months, „Rückfallplan“
were weight loss of at least 15 kg, and
andPatienten
Medical Science remission of diabetes, defined as HbA less than 6·5% (48 mmol/mol) after withdrawal of antidiabetes drugs at
(P Welsh PhD,
Prof N Sattar FMedSci),
baseline (remission was determined independently at 12 and 24 •months).
1c
Ko-primäre Endpunkte:
The trial is registered with the ISRCTN
College of Medical, Veterinary registry, number 03267836, and follow-up is ongoing.
& Life Sciences, and General
• > - 15 kg
Practice and Primary Care
(Y McIlvenna MSc) and
HbA1c
Findings The intention-to-treat population consisted of 149 participants per•group. < 6.5%
At 24 months, ohne
17 (11%) Therapie
intervention
participants and three (2%) control participants had weight loss of at least 15 kg (adjusted odds ratio [aOR] 7·49,
Robertson Centre for
Lean MEJ et al., Lancet
95%391: 541,to2018
CI 2·05
Biostatistics (S Kean,
& p=0·0023)
27·32; Lancet Diaband Endocrinol 7: 344, 2019
53 (36%) intervention participants and five (3%) control participants had
remission of diabetes (aOR 25·82, 8·25 to 80·84; pArticles
Durability of a primary care-led weight-management
Articles intervention for remission of type 2 diabetes: 2-year results
of the DiRECT open-label, cluster-randomised trial
Michael E J Lean*, Wilma S Leslie, Alison C Barnes, Naomi Brosnahan, George Thom, Louise McCombie, Carl Peters, Sviatlana Zhyzhneuskaya,
Ahmad Al-Mrabeh, Kieren G Hollingsworth, Angela M Rodrigues, Lucia Rehackova, Ashley J Adamson, Falko F Sniehotta, John C Mathers,
Hazel M Ross, Yvonne McIlvenna, Paul Welsh, Sharon Kean, Ian Ford, Alex McConnachie, Claudia-Martina Messow, Naveed Sattar, Roy Taylor*
Summary
A B
Lancet Diabetes Endocrinol Background The DiRECT trial assessed remission of type 2 diabetes during a primary care-led weight-management
2019; 7: 344–55 100 Year 1: Fisher's exact test pAktuelle Empfehlungen zur medikamentösen Therapie des T2 DM (ADA, EASD; Januar 2019)
Heerspink et al
CV und renale Effekte
der SGLT2-Hemmer
Heerspink et al., Circulation. 2016;134:752–772
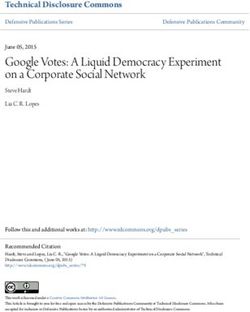
Figure 2. Physiologic mechanisms implicated in the cardiovascular and renal protection with SGLT2 inhibition.
HbA1c indicates hemoglobin A1c; and SGLT2, sodium-glucose cotransporter-2.
fect of combining the SGLT2 inhibitor canagliflozin with RAAS activation, which is then inhibited pharmacological-
a thiazide, nor does the combination produce a greater ly by angiotensin-converting enzyme (ACE) inhibition or
natriuretic effect in comparison with either drug alone.45 an angiotensin receptor blocker, resulting in enhanced
Similar to this report using canagliflozin,45 the addition BP lowering is not known. Alternatively, angiotensin II in-
of a thiazide diuretic to dapagliflozin does not yield ad- creases SGLT2 mRNA expression and proximal tubularCardiovascular Risk and SGLT2 Inhibition
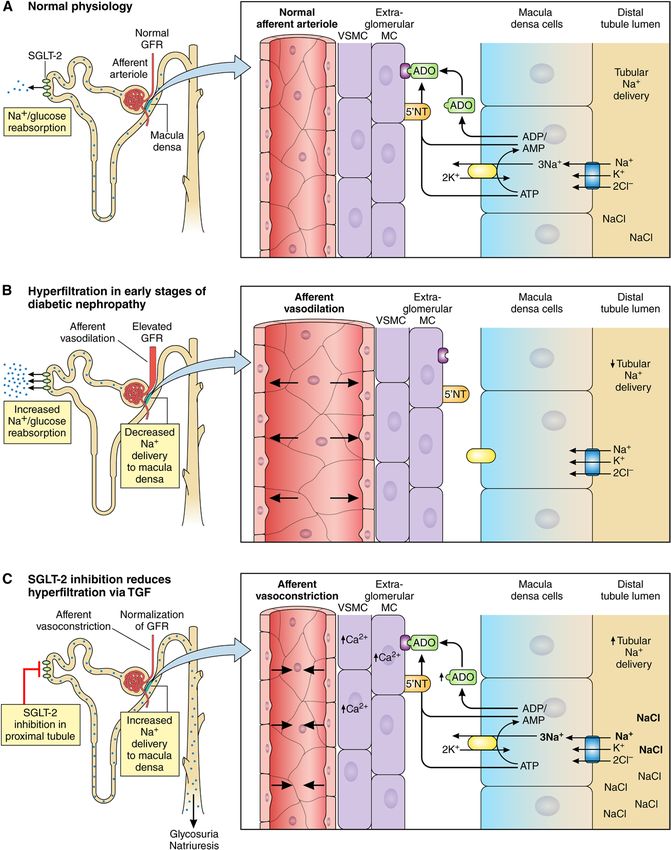
Renale Effekte der SGLT2-Hemmer
STATE OF THE ART
Reduktion der glomerulären Hyperfiltration
durch Effekte auf den tubuloglomerulären
Feedback-Mechanismus
Heerspink et al., Circulation. 2016;134:752–772
Figure 5. Putative mechanism for sodium-mediated changes in adenosine bioactivity at the afferent arteriole.
During normal conditions (A), sodium-glucose cotransport leads to minimal glycosuria. If, under these nondiabetic conditions, NaCl
delivery to the macula densa was reduced in the context of a physiological stress such as hypotension, renal perfusion would
decrease, leading to a reduction in NaCl transit across macula densa cells, thereby causing less adenosine triphosphate (ATP)
release and breakdown to adenosine, which is a vasoconstrictor. Consequently, less vasoconstrictive adenosine (Continued )
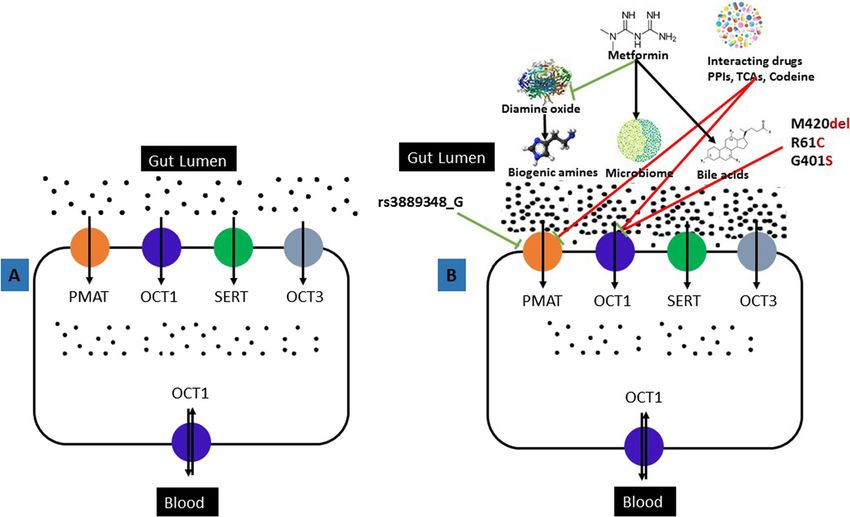
Circulation. 2016;134:752–772. DOI: 10.1161/CIRCULATIONAHA.116.021887 September 6, 2016 761Kardiovaskuläre Endpunktstudien –
SGLT2-Hemmer
EMPA-REG OUTCOME CANVAS DECLARE
(Empagliflozin) (Canagliflozin) (Dapagliflozin)
Studienteilnehmer (n) 7‘020 10‘142 17‘160
Follow-up (Jahre) 3.1 3.6 4.2
Atherosklerotische
99% 66% 41%
kardiovaskuläre Erkrankung
MACE Placebogruppe (%/Jahr)
4.4 3.2 2.4
(Kv Tod, MI, Schlaganfall)
Hazard ratio (HR) und 95% Konfidenzintervall
MACE
0.86 (0.74-0.99) 0.86 (0.75-0.97) 0.93 (0.84-1.03)
(Kv Tod, MI, Schlaganfall)
Kv Tod 0.62 (0.49-0.77) 0.90 (0.71-1.15) 0.98 (0.82-1.17)
Herzinsuffizienz 0.65 (0.50-0.85) 0.67 (0.52-0.87) 0.73 (0.61-0.88)
Renaler Endpunkt* 0.54 (0.40-0.75) 0.60 (0.47-0.77) 0.53 (0.43-0.66)
Home P., Diabetologia 62: 357, 2019
*Verdoppelung Serumkreatinin oder 40% Abfall eGFR, ESRD, Tod an Nierenerkrankung Zelniker et al., Circulation 139: 2022, 2019NAL RESEARCH
A B
ARTICLE
SGLT2-Hemmer und chronische
Neuen et al Niereninsuffizienz (CANVAS study)
CV/Renal Outcomes With Canagliflozin in CKD
ORIGINAL RESEARCH
HbA1c BD sys C
Gewicht D
Albuminurie
A B
ARTICLE
Neuen et al CV/Renal Outcomes With Canagliflozin in CKD
Figure 1. Changes in intermediate outcomes with canagliflozin compared to placebo in participants with eGFRTThhee neew
n w eeng
ngllaan
ndd jjoouurrna
nall ooff meedic
m diciin
nee
AA Primary
PrimaryComposite
CompositeOutcome
Outcome BB Renal-Specific
Renal-Specific Composite
Composite Outcome
Outcome
100
100 30
30 100
100 20
20
Hazardratio,
Hazard ratio,0.70
0.70(95%
(95%CI,
CI,0.59–0.82)
0.59–0.82) Hazard ratio,
Hazard ratio, 0.66
0.66 (95%
(95% CI,
CI, 0.53–0.81)
0.53–0.81)
90
90 25 P=0.00001
25 90
90 PTThhee neew
n w eeng
ngllaan
ndd jjoouurrna
nall ooff meedic
m diciin
nee
AA Primary
PrimaryComposite
CompositeOutcome
Outcome BB Renal-Specific
Renal-Specific Composite
Composite Outcome
Outcome
100
100 30
30 100
100 20
20
Hazardratio,
Hazard ratio,0.70
0.70(95%
(95%CI,
CI,0.59–0.82)
0.59–0.82) Hazard ratio,
Hazard ratio, 0.66
0.66 (95%
(95% CI,
CI, 0.53–0.81)
0.53–0.81)
90
90 25 P=0.00001
25 90
90 Pdisease, doubling of th
A Urinary Albumin-to-Creatinine Ratio Median Baseline
Canagliflozin Placebo or death from renal o
913.5 918.0 than those who received
1200 canagliflozin group also
1000 Placebo stage kidney disease, h
Geometric Mean
800 failure, and the comp
death, myocardial infa
600
results indicate that can
Canagliflozin
CREDENCE Studie fective treatment option
400
200 cular protection in patie
Albuminurie und eGFR über die Zeit 0
0 6 12 18 24 30 36 42
with chronic kidney dis
The observed benef
Months since Randomization background of renin–an
T h e n e w e ng l a n d j o u r na l No.o fofmPatients
e dic i n e ade, the only approved
Placebo 2113 2061 1986 1865 1714 1158 685 251 tions in type 2 diabetes
Canagliflozin 2114 2070 2019 1917 1819 1245 730 271
the clinical significan
disease, doubling of the serum creatinine level, contrast to completed
A Urinary Albumin-to-Creatinine Ratio Median Baseline B Change from Baseline in Estimated GFR Baseline (ml/min/1.73 m2)
Canagliflozin Placebo or death from renal or cardiovascular causes trials of SGLT2 inhibito
Canagliflozin Placebo
913.5 918.0 than those who received placebo. Patients in the 56.4 56.0 population at high risk
1200 canagliflozin group also 0 had a lower risk of end- had a primary outcom
Least-Squares Mean Change
−2
1000 Placebo stage kidney disease, −4
hospitalization for heart points. In addition, we
(ml/min/1.73 m2)
Geometric Mean
800 failure, and the composite −6 of cardiovascular received canagliflozin (
Canagliflozin
death, myocardial infarction,−8 or stroke. These a reduced estimated G
600
results indicate that−10 canagliflozin
−12
may be an ef- lower risk of the prima
Canagliflozin
400 fective treatment option −14 for renal and cardiovas- those in the placebo gr
200 cular protection in patients
−16 with type 2 diabetes Placebo
stage kidney disease. T
−18
0
with chronic kidney disease.
−20 served despite very mo
0 6 12 18 24 30 36 42 The observed benefits 0 3 were 6 obtained
12 18 on 24 a 30 36 42 ferences in blood glu
Months since Randomization background of renin–angiotensinMonths system block-
since Randomization blood pressure and in c
No. of Patients ade, theNo. only approved renoprotective medica-
of Patients cern about the initial a
Placebo 2113 2061 1986 1865 1714 1158 685 251 tions inPlacebo
type 2 diabetes, 2178 a factor
1985 that
1882 highlights
1720 1536 1006 583 210
timated GFR observed
Canagliflozin 2114 2070 2019 1917 1819 1245 730 271 Canagliflozin 2179 2005 1919 1782 1648 1116 652 241
the clinical significance of the findings. In This suggests that the
B Change from Baseline in Estimated GFR Baseline (ml/min/1.73 m2) contrast to completed cardiovascular outcome likely to be independen
Figure 3. Effects on Albuminuria and Estimated GFR.
Canagliflozin Placebo trials of SGLT2 inhibitors,5-7 our trial included a may possibly stem from
Panel A shows the effects of canagliflozin and placebo on the urinary albu-
56.4 56.0 population at high risk
min-to-creatinine ratio forthekidney
in failure and
intention-to-treat population. Panel B shows merular pressure,11-13 wi
0
had atheprimary outcome of major
level in renal end GFR in the on-treat-
Least-Squares Mean Change
−2 change from the screening the estimated nisms presently being s
Perkovic V et al.,confidence
N Engl Jinterval
Med inepub 14. April 2019
−4 points.ment
In addition,
population.weThefound that patients
I bars indicate the 95% who Panel
Our trial population
(ml/min/1.73 m2)
−6 A and
received the standard error
canagliflozin in Panelthose
(including B. The who
albumin-to-creatinine
had ratio was
−8 Canagliflozin calculated with albumin measured in milligrams and creatinine measured cardiovascular outcom
−10
a reduced estimated GFR at baseline) had a death, myocardial infarc
in grams.
−12 lower risk of the primary outcome overall than ization for heart failur
−14 those in the placebo group, as well as less end- the population over a
−16 Placebo
−18
stage kidney disease. These findings were ob-
hospitalizations for heart failure (NNT, 46; 95% follow-up. The signific
−20 served despite very modest CI, 29 tobetween-group dif-
124) and 25 composite events of cardio- diovascular outcomes,
0 3 6 12 18 24 30 36 42 ferences in blood glucose level, weight, andDECLARE-TIMI 58 Studie
Effekt von Dapagliflozin vs. Placebo in Abhängigkeit von
der Kato
EF/Herzinsuffizienzanamnese
et al
bei Studienstart
Clinical Efficacy of Dapagliflozin by Ejection Fraction
ORIGINAL RESEARCH
ARTICLE
Kato ET et al., Circulation 139:2528, 2019
Figure 1. Cardiovascular outcomes by heart failure (HF) category.
There were 671 patients with HF with reduced ejection fraction (HFrEF) defined as left ventricular ejection fraction (EF)DECLARE-TIMI 58 Studie
Effekt von Dapagliflozin vs. Placebo in Abhängigkeit von
der Kato
EF/Herzinsuffizienzanamnese
et al
bei Studienstart
Clinical Efficacy of Dapagliflozin by Ejection Fraction
ORIGINAL RESEARCH
ARTICLE
Kato ET et al., Circulation 139:2528, 2019
Figure 1. Cardiovascular outcomes by heart failure (HF) category.
There were 671 patients with HF with reduced ejection fraction (HFrEF) defined as left ventricular ejection fraction (EF)CKD und/oder Herzinsuffizienz
Metformin ! – und SGLT2i* !!
*Empagliflozin, Canagliflozin, DapagliflozinBekannte und diskutierte Nebenwirkungen von
SGLT2-Hemmern und Vorsichtsmassnahmen bei der
Anwendung
Nebenwirkung Massnahme
Genitalmykosen, HWI Patienteninstruktion, Hygiene, Therapie
Polyurie und Polydipsie Patienteninstruktion, cave Prostathyperplasie
Volumendepletion, Orthostase Patienteninstruktion, Anpassung Antihypertensiva bzw. Diuretika
Euglykämische Ketoazidose Patienteninstruktion, Therapiestopp bei schweren interkurrenten
Erkrankungen, KI in kataboler Situation
Minor-Amputationen Patienteninstruktion, sorgfältige Überwachung von Patienten mit DFS
Akutes Nierenversagen Gemäss neueren Analysen nicht gehäuft
Fourniergangrän (nekrotisierende Fallserie
Fasziitis des Perineums)
Osteoporose - Frakturrisiko Kein erhöhtes Frakturrisiko unter SGLT2i, GLP-1-RA und DPP-IV-
Hemmern
Ueda et al., BMJ 363:k4365, 2018; Bersoff-Matcha et al., Ann Int Med 170: 764, 2019;
Gilbert RE et al., Diabetes Obesity Metabol epub 3. Mai 2019; Hidayat et al., Osteoporosis Int, epub 27. Mai 2019GLP-1-Rezeptor-Agonisten
REVIEWS
Brain
↓ Appetite
Muscle Heart
↑ Satiety ↓ Blood pressure
↑ Glycogen synthesis
↑ Glucose oxidation ↑ Heart rate
↑ Myocardial contractility
GLP1 ↑ Diastolic function
7
↑ Cardioprotection
Kidney His Ala Glu Gly Thr Phe Thr Ser Asp
↑ Endothelial function
↑ Natriuresis Val
Ser
Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Glu
36
Phe
Ile Ala Trp Leu Val Lys Gly Arg CONH2
Gastrointestinal tract
Adipose tissue ↓ Gastric emptying
↑ Lipolysis ↓ Acid secretion
Pancreas
↑ Glucose uptake ↑ Insulin secretion
↓ Glucagon secretion
↑ β-cell proliferation
GLP1RAs Physiological levels of GLP1 Pre-clinical studies
Fig. 1 | Effects of GLP1 and GLP1RAs on various tissues. The applied colour code indicates whether the effect on the
target tissue has been observed in preclinical studies (blue boxes), at physiological levels of glucagon-like peptide 1 (GLP1)
in clinical studies (yellow boxes) or after treatment with GLP1 receptor agonists (GLP1RAs; red boxes). The figure depicts
amidated GLP1 (GLP1 7–36)2,3,11,13,14,126–128.
Andersen A et al., Nature Rev Endocrinol 14: 390, 2018
with individuals with normal glucose tolerance25; by only 53% structural homology with native GLP1 but
contrast, a meta-analysis suggested that GLP1 secretion activates the GLP1R with the same potency as native
was not altered in patients with T2DM26. GLP1 and it is resistant to degradation by DPP4 owing
Whereas the role of an altered GLP1 secretion in to a glycine instead of an alanine at position two (the
T2DM remains somewhat debated, it is well established cleavage site of DPP4)31. Another strategy is to alter the
that GLP1 maintains robust insulinotropic properties amino acid sequence of native GLP1 to avoid degra-
in these patients, although this occurs with a reduced dation by DPP4. Currently, seven different GLP1RAs
potency compared with that seen in healthy individu- have been approved for the treatment of T2DM, andREVIEWS
Short-acting Long-acting
Native human GLP1 (3.3 kDa) Exenatide once weekly
DPP4 recognition site
His Ala Glu Gly Thr Phe Thr Ser Asp Exenatide
Val
Ser
molecules
Bydureon®
Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Glu Biodegradable
polyactide-co-
Phe glycolide
Ile Ala Trp Leu Val Lys Gly Arg CONH2 polymer matrix
Exenatide twice daily (4.2 kDa) Liraglutide (3.8 kDa) Dulaglutide (59.7 kDa)
His Gly Glu Gly Thr Phe Thr Ser Asp C16 His Ala Glu Gly Thr Phe Thr Ser Asp His Gly Glu Gly Thr Phe Thr Ser Asp Val
Leu fatty acid Val Ser
26 Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Ser Glu Ser Glu
Trulicity ®
Arg Val Ala Glu Glu Glu Met Gln Lys Lys Ala Ala Gln Gly Glu Leu Tyr Ser Phe Ile Ala Trp Leu Val Lys Gly Gly Gly
Leu Glu
Phe Phe Fc domain
Ile Glu Trp Leu Lys Asp Gly Gly Pro Ser Ile Ala Trp Leu Val Arg Gly Arg Gly
Ser Phe Ile Ala Trp Leu Val Lys Gly Gly Gly
Glu
Gly Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Byetta®
Ser Pro Pro Pro Ala
Victoza® His Gly Glu Gly Thr Phe Thr Ser Asp Val
Ser
GLP-1-RA unterscheiden sich
Semaglutide (4.1 kDa) insbesondere bzgl. ihrer Wirkdauer
Lixisenatide (4.9 kDa) 8
His Gly Glu Gly Thr Phe Thr Ser Asp
Albiglutide (73.0 kDa) C18
fatty acid
His Aib Glu Gly Thr Phe Thr Ser Asp und Analogie zum GLP-1-Molekül
8 Val
Leu
Spacer
Ser His Gly Glu Gly Thr Phe Thr Ser Asp Ser
Arg Val Ala Glu Glu Glu Met Gln Lys Val Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Leu Glu
Ser
Phe Lys Ala Ala Gln Gly Glu Leu Tyr Ser Phe
Ile Glu Trp Leu Lys Asp Gly Gly Pro Ser Glu Ile Ala Trp Leu Val Arg Gly Arg Gly
Ser Phe
Ile Ala Trp Leu Val Lys Gly Arg His Gly Glu Gly Thr Phe Thr Ser Asp
Lys
Lys Ser Pro Pro Pro Ala
Gly
Val Ozempic ®
Ser
Lyxumia® Lys Lys Ala Ala Gln Gly Glu Leu Tyr Ser
Lys Lys Lys
Eperzan® Glu
Phe
Ile Ala Trp Leu Val Lys Gly Arg rH-albumin
Fig. 2 | Structure and molecular mass of native GLP1 in comparison with have fatty acid chain (C16 and C18, respectively) attachments for reversible Andersen A et al., Nature Rev Endocrinol 14: 390, 2018
approved and emerging GLP1RAs. Exenatide twice daily and lixisenatide are binding to albumin (yellow boxes). Albiglutide and dulaglutide are covalently
short-acting glucagon-like peptide 1 (GLP1) receptor agonists (GLP1RAs) that bound to larger carrier proteins (red boxes), such as recombinant human serum
are based on an exendin 4 structure. Exenatide once weekly is the only albumin (rH-albumin) and an immunoglobulin G4 crystallizable fragment (IgG4
approved long-acting GLP1RA that is based on an exendin 4 structure, whereas Fc) fragment. The dark blue colour indicates homology with native GLP1, while
the remaining long-acting GLP1RAs (liraglutide, dulaglutide, albiglutide and the light blue colour indicates non-homology. Aib, α-aminoisobutyric acid;
semaglutide) are all based on a GLP1 structure. Liraglutide and semaglutide DPP4, dipeptidyl peptidase 4.
anti-exenatide antibodies were significantly correlated for extended release. Liraglutide has a C16 fatty acid
with smaller reductions in HbA1c, whereas several other chain attached at Lys26, and the hydrophobic properties
studies have demonstrated no clinically relevant effect result in the formation of heptamers, delaying absorp-GLP-1-Agonisten:
R EVIEWS potente HbA1c-Reduktion
GETGOAL-X LEAD-6 DURATION-1 DURATION-5 DURATION-6 HARMONY 7 AWARD-1 AWARD-6 SUSTAIN-3 SUSTAIN-7
0.0
Change in HbA1c compared with baseline (mmol/mol)
–0.2
–0.4
–0.6
–0.8
* †
–1.0
–1.2
P < 0.0001
–1.4
*
P < 0.0010
–1.6 P < 0.0001
P < 0.0018
P < 0.0001
–1.8
‡
–2.0 P = 0.0023 Exenatide twice daily Liraglutide Albiglutide Semaglutide
Lixisenatide Exenatide once weekly Dulaglutide
Fig. 3 | HbA1c reductions in phase III head-to-head trials comparing (REF.55), AWARD-6 (REF.59), SUSTAIN-3 (REF.71) and SUSTAIN-7 (REF.72). P values
GLP1RAs in type 2 diabetes mellitus. The results from the following trials are reported where appropriate. GLP1RAs, glucagon-like peptide 1 receptor
are displayed: GETGOAL-X 48, LEAD-6 (REF. 44) , DURATION-1 (REF. 43) , agonists. *Noninferiority criteria met. †Noninferiority criteria not met.
DURATION-5 (REF.54), DURATION-6 (REF.57), HARMONY 7 (REF.58), AWARD-1 ‡
Superiority criteria met.
Andersen A et al., Nature Rev Endocrinol 14: 390, 2018
(albiglutide and dulaglutide), and they are administered 1.8 mg has also proved superior to exenatide once
either once daily (liraglutide) or once weekly (exenatide weekly, dulaglutide and albiglutide in reducing body
once weekly, albiglutide and dulaglutide). weight57–59. The limited effect of albiglutide on body
In clinical phase III studies, long-acting GLP1RAs weight compared with liraglutide in the HARMONY 7
have generally proved superior to exenatide twice trial stands out, as patients treated with albiglutide had a
daily in terms of reducing HbA1c levels and fasting body weight reduction of 0.6 kg compared with a 2.2 kg
plasma levels of glucose, while lixisenatide has not yet reduction with liraglutide after 32 weeks of treatment58.GLP-1-Agonisten:
REVIEWS Gewichtsreduktion
GETGOAL-X LEAD-6 DURATION-1 DURATION-5 DURATION-6 HARMONY 7 AWARD-1 AWARD-6 SUSTAIN-3 SUSTAIN-7
–0
Change in body weight compared with baseline (kg)
–1
P < 0.0500
–2
† P < 0.0001
–3
P < 0.2235
–4 P = 0.0005 P = 0.0011
P = 0.8900
*
–5
–6 P < 0.0001
‡
–7
Exenatide twice daily Liraglutide Albiglutide Semaglutide
Lixisenatide Exenatide once weekly Dulaglutide
Fig. 5 | Body weight reductions in phase III head-to-head trials AWARD-1 (REF.55), AWARD-6 (REF.59), SUSTAIN-3 (REF.71) and SUSTAIN-7
comparing GLP1RAs in type 2 diabetes mellitus. The results from the (REF.72). P values are reported where appropriate. GLP1RAs, glucagon-like
following trials are displayed: GETGOAL-X48, LEAD-6 (REF.44), DURATION-1 peptide 1 receptor agonists. *Significance not stated. †No significant
(REF.43), DURATION-5 (REF.54), DURATION-6 (REF.57), HARMONY 7 (REF.58), difference. ‡Superiority criteria met.
Andersen A et al., Nature Rev Endocrinol 14: 390, 2018
cardiovascular safety of glucose-lowering therapeu- myocardial infarction and nonfatal stroke when com-
tics was highlighted after serious concern was raised pared with placebo (HR 0.87; 95% CI 0.78–0.97 and HR
about the cardiovascular safety of rosiglitazone owing 0.74; 95% CI 0.58–0.95, respectively). In LEADER, the
to a meta-analysis demonstrating a significant increase cardiovascular effect was mainly driven by a significant
in the risk of myocardial infarction in patients treated reduction in death from cardiovascular causes (HR 0.78;
with the compound82. Consequently, the cardiovascu- 95% CI 0.66–0.93), whereas the observed reductions in
lar effects of all approved and emerging GLP1RAs have incidence of nonfatal myocardial infarction or nonfatalKardiovaskuläre Endpunktstudien –
GLP-1-Rezeptor-Agonisten
LEADER SUSTAIN 6 EXSCEL REWIND
(Liraglutide) (Semaglutide) (Exenatide ER) (Dulaglutide)
Studienteilnehmer (n) 9‘340 3‘297 14‘752 9‘901
Follow-up (Jahre) 3.8 2.1 3.2 5.4
Atherosklerotische
81% 71% 73% 31.5%
kardiovaskulär Erkrankung
MACE Placebogruppe (%/Jahr)
3.9 4.2 4.0 2.5
(Kv Tod, MI, Schlaganfall)
Hazard ratio (HR) und 95% Konfidenzintervall
MACE
0.87 (0.78-0.97) 0.74 (0.58-0.95) 0.91 (0.83-1.00) 0.88 (0.79-0.99)
(Kv Tod, MI, Schlaganfall)
Kv Tod 0.78 (0.66-0.93) 0.98 (0.65-1.48) 0.88 (0.76-1.02) 0·91 (0·78–1·06)
Herzinsuffizienz 0.87 (0.73-1.05) 1.11 (0.77-1.61) 0.94 (0.78-1.13) 0·93 (0·77–1·12)
Makro-
Renaler Endpunkt* 0.89 (0.67-1.19) 1.28 (0.64-2.58) 0.88 (0.74-1.05)
albuminurie ↓
*Verdoppelung Serumkreatinin oder 40% Abfall eGFR, Home P., Diabetologia 62: 357, 2019, Gerstein et al., Lancet epub 10. Juni 2019
ESRD, Tod an Nierenerkrankung Zelniker et al., Circulation 139: 2022, 2019Effects of Liraglutide on Cardiovascular
primary composite end point occurred in 128 of 1265
Events in Patients With a History of
patients (10.1%) with an incidence rate of 2.6 per 100
Established Atherosclerotic Cardiovascular PYO in the liraglutide group compared with 123 of the
Disease Without MI/Stroke 1300 patients (9.5%) with an incidence rate of 2.5 per
The primary composite end point occurred in 158 100 PYO in the placebo group (HR, 1.08; 95% CI, 0.84–
of the 1538 patients (10.3%) with an incidence rate 1.38). The HRs for liraglutide versus placebo for time to
of 2.7 PYO in the liraglutide group compared with the first of the individual components of the 3-point
199 of the 1545 patients (12.9%) with an incidence MACE were as follows: 0.99 (95% CI, 0.67–1.46) for
rate of 3.4 per 100 PYO in the placebo group (HR, cardiovascular death, 1.00 (95% CI, 0.67–1.49) for
LEADER Studie
0.76; 95% CI, 0.62–0.94). Individual components nonfatal MI, and 1.12 (95% CI, 0.68–1.82) for nonfa-
of 3-point MACE were consistently reduced with li- tal stroke (Figures 1 and 2). The HR for all-cause death
raglutide, including cardiovascular death (HR, 0.59; was 0.95 (95% CI, 0.72–1.27; Figure 2). Liraglutide
CVOT Liraglutide vs. Placebo bei sehr hohem CV Risiko
95% CI, 0.41–0.84), nonfatal MI (HR, 0.91; 95% CI,
0.68–1.22), and nonfatal stroke (HR, 0.68; 95% CI,
treatment showed a similar trend for the key secondary
expanded end point (incidence rate, 3.9 per 100 PYO)
A B
Kardiovaskuläre Risikoreduktion
bei Patienten in der 2° Prävention
• Herzinfarkt/Schlaganfall
• Kv Erkrankung ohne Herzinfarkt/
C D Schlaganfall
Figure 1. Occurrence of the primary composite outcome (A), cardiovascular (CV) death (B), nonfatal myocardial infarction (MI; C), and nonfatal
Verma et al., Circulation 138:2884, 2018
stroke (D), stratified by history of MI and/or stroke, established cardiovascular disease (CVD) without MI/stroke, or cardiovascular risk factors alone.
Primary composite end point (cardiovascular death, nonfatal MI, or nonfatal stroke) from randomization to follow-up. The x axis was truncated at 54 months
becausend the proportion inhibitor, metformin, sulfonylurea, insulin, or angioten-
nd adverse events sin-converting enzyme inhibitor or angiotensin-receptor
were analysed with blocker at the last visit (appendix p 36).
is registered with The primary composite outcome occurred in
952. 594 (12·0%) participants (2·4 per 100 person-years)
assigned to dulaglutide and 663 (13·4%) participants
(2·7 per 100 person-years) assigned to placebo (HR 0·88,
d by Eli Lilly and 95% CI 0·79–0·99; p=0·026; figure 2, table 2). Consistent
teering committee effects were observed for all three components of the
Research Institute composite primary outcome (pheterogeneity=0·89),19 with HRs
d all data analyses.
n were provided by
employed by the
REWIND-Studie
of 0·91 (95% CI 0·78–1·06; p=0·21) for cardiovascular
death, 0·96 (0·79–1·16; p=0·65) for non-fatal myocardial
infarction, and 0·76 (0·61–0·95; p=0·017) for non-fatal
ee and contributed
n, and data inter-
Dulaglutide vs. Placebo bei T2DM mit relativ tiefem
stroke (figure 2, table 2).
When assessed within subgroups, the HR of the
or jointly made the
The corresponding
kardiovaskulären Risiko (70% 1° Prävention)
intervention on the primary outcome was similar in
participants with and without previous cardiovascular
a in the study and
sion to submit for A Composite cardiovascular outcome B Cardiovascular death
18 Placebo HR=0·91 (95% CI 0·78–1·06)
Dulaglutide p=0·21
15
Cumulative risk (%)
013, 12 133 patients 12
ries. 10 917 eligible 9
iod, of whom 9901 6
group (dulaglutide,
ollow-up ended on
3 HR 0·88 (95% CI 0·79–0·99)
p=0·026
Kardiovaskuläre Risikoreduktion
0
0 1 2 3 4 5 6 0 1 2 3 4 5 6 bei Patienten in der 1° Prävention
years [SD 6·5], and Number at risk
ppendix p 35).17 At Placebo 4952 4791 4625 4437 4275 3575
Dulaglutide 4949 4815 4670 4521 4369 3686
742
741
4952 4854 4748 4617 4499 3813 802
4949 4866 4773 4663 4556 3887 807
• MACE
reported previous
2%) had a baseline C Non-fatal myocardial infarction D Non-fatal stroke
• V.a. Schlaganfall
3 m². The median 18 HR 0·96 (95% CI 0·79–1·16) HR 0·76 (95% CI 0·61–0·95)
p=0·65 p=0·017
s (IQR 5·5–14·5), 15
–8·1), and median
Cumulative risk (%)
12
IQR 61·4–91·1).
9
ears (IQR 5·1–5·9)
primary composite 6
7·1%) participants 3
ticipants assigned 0
4952 participants 0 1 2 3 4 5 6 0 1 2 3 4 5 6
ne discontinuation Number at risk
Time since randomisation (years) Time since randomisation (years)
reas 3621 (73·2%) Placebo 4952 4819 4680 4518 4372 3672 766 4952 4826 4692 4534 4396 3710 777
Dulaglutide 4949 4833 4705 4574 4443 3772 767 4949 4847 4736 4606 4476 3796 776
(71·1%) assigned
the last visit. Par- Figure 2: Cumulative incidence of cardiovascular outcomes
Gerstein et al., Lancet epub 10. Juni 2019
ok study drug for HR=hazard ratio. HbA1c=glycated haemoglobin A1c.
9 http://dx.doi.org/10.1016/S0140-6736(19)31149-3 5Klinische kardiovaskuläre
Erkrankung
Metformin ! – und SGLT2i oder GLP-1-RA*!!
• Liraglutide, Semaglutide, Dulaglutide, ibs. wenn Gewichts- und/oder starke HbA1c-Reduktion angestrebt
• HbA1c- & Gewichtsreduktion Semaglutide > Dulaglutide (Sustain 9 & whs. Liraglutide – Sustain 10)Articles
Oral semaglutide versus subcutaneous liraglutide and
placebo in type 2 diabetes (PIONEER 4): a randomised,
Articles
double-blind, phase 3a trial
Richard Pratley, Aslam Amod, Søren Tetens Hoff, Takashi Kadowaki, Ildiko Lingvay, Michael Nauck, Karen Boje Pedersen, Trine Saugstrup,
Juris J Meier, for the PIONEER 4 investigators
• Durch die Verwendung eines
Summary
A Treatment policy estimand Trial product estimand
Resorptionsenhancers
Background
100 Glucagon-like peptide-1 (GLP-1) receptor agonists are 100 effective treatments for type 2 diabetes, lowering Published Online
glycatedMean
8·5
haemoglobin
baseline HbA : 8·0%(HbA 1c) and weight, but are currently only approved for use as subcutaneous injections. Oral
(SD 0·7; 64
1c mmol/mol [SD 8])
8·5
Mean baseline HbA : 8·0% (SD 0·7; 64 mmol/mol [SD 8]) 1c („SNAC“; intestinal
June 8, 2019
http://dx.doi.org/10.1016/
semaglutide, a novel GLP-1 agonist, was compared 65
with subcutaneous liraglutide and placebo in patients 65
with permeation enhancer) wird
HbA1c (mmol/mol)
HbA1c (mmol/mol)
8·0 8·0 S0140-6736(19)31271-1
type 2 diabetes.
die orale Bioverfügbarkeit
HbA1c (%)
HbA1c (%)
60 60
7·5 7·5 See Online/Comment
55 55 http://dx.doi.org/10.1016/
7·0 7·0
Methods In this randomised, double-blind, double-dummy,
6·5
50 phase 3a trial, we recruited patients with type50 2 diabetes
6·5 von Semaglutide erhöht
S0140-6736(19)31350-9
from 100 sites in 12 countries. Eligible patients45were aged 18 years or older, with HbA1c of 7·0–9·5% (53–80·3 mmol/mol),
Oral semaglutide 45 AdventHealth Translational
6·0 Subcutaneous liraglutide 6·0
on a stable Placebo
0
inhibitor.
dose of metformin (≥1500 mg or maximum tolerated) with or without a sodium-glucose co-transporter-2
0 4 Participants 20 were 32randomly 45 assigned (2:2:1) with an 0interactive 14web-response 32 system 45 and52 stratified by
• s.c. -> 1 mg/Woche
Research Institute for
Metabolism and Diabetes,
p.o. -> 14 mg/Tag
8 14 26 38 52 0 4 8 20 26 38
Orlando, FL, USA
background glucose-lowering
Number of patients medication and country
Time since randomisation (weeks)
Numberofoforigin,
patients to once-daily oral semaglutide (dose escalated to
Time since randomisation (weeks)
(Prof R Pratley MD); Life
14 mg),
Oral semaglutide once-daily
285 282 276 272 subcutaneous
268 278 274 272 liraglutide
273 275 (dose escalated to 1·8 285
Oral semaglutide mg),
280 or272 placebo
259 246 for 23852234
weeks.227 Two 226 estimands
220 were Chatsmed Garden Hospital and
Subcutaneous liraglutide 284 276 270 269 268 272 267 269 268 269 Subcutaneous liraglutide 284 272 266 259 251 245 240 239 233 230
defined:
Placebo treatment
142 139 137 136 policy 133 134(regardless
133 133 of study
132 133 drug discontinuation Placebo 142 or137rescue
133 128 medication)
119 112 104 and99trial 87product 82 (assumed Nelson R Mandela School of
Medicine, Durban, South Africa
all participants
B
were on study drug without rescue medication) in all participants who were randomly assigned. The
(A Amod MD); Novo Nordisk
treatment policy estimand was the primary estimand. The primary endpoint was change from baseline to week 26 in
Oral semaglutide A/S, Søborg, Denmark
Subcutaneous liraglutide
HbA 1001c (oralPlacebo
semaglutide superiority vs placebo and non-inferiority 100 [margin: 0·4%] and superiority vs subcutaneous (S T Hoff MD, K B Pedersen MD,
ETD: –1·4
liraglutide) and the confirmatory
ETD: –1·1 secondary endpoint was change fromETD:baseline
ETD: –1·0 –1·2 to week 95% CI 26
–1·6 toin
–1·2 bodyweight (oral T Saugstrup MSc); Department
0·5 95% CI –1·2 to –0·9 95% CI –1·2 to –0·8 0·5 95% CI –1·4 to –1·0 pOptionen nach MET
+ SGLT2i/GLP-1-RA
• DPP-IV-Hemmer
• Günstiges NW-Profil
• Sitagliptin (TECOS) und
Linagliptin (CARMELINA) mit
„neutralen“ CVOT
• Keine Kombination mit GLP-1-RA
• Basisinsulin !!!
• SGLT2i + GLP-1-RA
• Kostengutsprache nötig
• GliclazidS94
Pharmacologic Approaches to Glycemic Treatment
Diabetes Care Volume 42, Supplement 1, January 2019
Figure 9.1—Glucose-lowering medication in type 2 diabetes: overall approach. For appropriate context, see Fig. 4.1. ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; CV, cardiovascular;
CVD, cardiovascular disease; CVOTs, cardiovascular outcomes trials; DPP-4i, dipeptidyl peptidase 4 inhibitor; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon-like peptide 1 receptor agonist; HF, heart failure;
SGLT2i, sodium–glucose cotransporter 2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione. Adapted from Davies et al. (39).Vielen Dank !
You can also read