Millennium development goals and oral health in cities in southern Brazil
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Community Dent Oral Epidemiol 2010; 38: 197–205 2010 John Wiley & Sons A/S
All rights reserved
Roberto Eduardo Bueno*, Samuel Jorge
Millennium development goals Moysés and Simone Tetu Moysés
Pontifı́cia Universidade Católica do Paraná,
and oral health in cities in Curitiba, Paraná, Brasil
southern Brazil
Bueno RE, Moysés SJ, Moysés ST. Millennium development goals and oral
health in cities in southern Brazil. Community Dent Oral Epidemiol 2010; 38:
197–205. 2010 John Wiley & Sons A ⁄ S.
Abstract – Objectives: To investigate social determinants of oral health,
analysing the occurrence of associations between millennium development
goals (MDG) indicators and oral health (OH) indicators. Methods: An
ecological study was performed in two distinct phases. In Phase 1, MDG
indicators and related covariates were obtained from the demographic census
of the Brazilian Institute of Geography and Statistics, the Ministry of Health
database and the 2000 Human Development Atlas, making up the whole set of
independent variables. Principal component analysis was carried out for the
independent variables showing the correlations among the variables
comprising the main components, and generating a synthetic index allowing
the performance of the cities to be known with regard to the MDG (MDG
index). In Phase 2, the DMFT index (mean number of decay, missing or filled
permanent teeth) and the CF index (prevalence of caries-free individuals), in
12 years old were obtained from the epidemiological survey undertaken in
2002–2003, in 49 cities in southern Brazil, and were analysed in relation to the Key words: dental caries; epidemiology;
MDG index using Spearman’s correlation. Results: A statistically significant health promotion; oral health; social
correlation was found for the DMFT and CF indices, respectively, with: the determinants of health
MDG index (R2 = 0.49 and 0.48; P = 0.00); the socioeconomic status of the Roberto Eduardo Bueno, Alameda Butantã,
population (R2 = 0.12 and 0.12; P = 0.02); the socioenvironmental characteristics 300, Zaniolo, São José dos Pinhais, PR 83025-
745, Brazil
(R2 = 0.41 and 0.46; P = 0.00). Conclusions: The MDG synthetic index of the
Tel.: 55 41 33835552
cities analysed and the respective components relating to their socioeconomic e-mail: roberto.edu.bueno@gmail.com
and socioenvironmental status demonstrated a positive correlation with OH *Grant Holder: CAPES–Coordenação de
indicators. As such, intersectoral public policies based on population strategies Aperfeiçoamento de Pessoal de Nı́vel Superior.
that act on social determinants of general and oral health need to be integrated Submitted 6 November 2009;
so as to impact on the MDG and OH outcomes. accepted 21 December 2009
Development (1994), the World Summit for Social
Introduction Development in Copenhagen (1995) and the World
At the Millennium Summit, held in September Conference on Women in Peking (1995).
2000, 191 countries committed to making efforts to The MDG are addressed to improving living
meet the millennium development goals (MDG) by conditions and promoting social equity. The eight
the year 2015 (1). The MDG were the result of goals are monitored by means of 18 targets with 48
complex negotiations that converged in the indicators. The goals include: (i) eradicating pov-
principal commitments of a series of international erty and hunger; (ii) achieving universal quality
meetings held during the 1990s, such as the primary education; (iii) promoting gender equality
Environmental Conferences in Rio de Janeiro and empowering women; (iv) reducing child
(1992), the Vienna Human Rights Conference mortality; (v) improving maternal health; (vi)
(1993), the Cairo Conference on Population and combating HIV ⁄ AIDS, malaria and other diseases;
doi: 10.1111/j.1600-0528.2010.00531.x 197Bueno et al.
(vii) improving quality of life and ensuring envi- The interconnection between health and devel-
ronmental sustainability; and (viii) encouraging a opment, as thoroughly reflected by the MDG
global partnership for development. The goals can statements, was reaffirmed in the document
also serve as a link between the agendas of prepared by the Commission on Social Determi-
governments, companies and civil society. They nants of Health which criticised the utilitarian view
are extensive references for the formulation of that health is just a resource for economic devel-
intersectoral public policies, aimed at social inclu- opment, arguing instead that socioeconomic con-
sion, reduction of inequities, promotion of health ditions can, also, determine the health of a
and quality of life of more vulnerable populations, population (2). More specifically, and having rele-
with protection of the environment and sustainable vant implications for this study, it is acknowledged
development. at large that socioeconomic influences play a
In Chile in March 2005, the World Health relevant role in the changes observed in health
Organization (WHO) launched the Commission indicators, including oral health. A study based on
on Social Determinants of Health, providing sup- data from 18 industrialized countries showed that
port to governments with theoretical and strategic dental services, measured in terms of the dentist–
inputs for improving the health conditions and population ratio, accounted for 3% of the reduction
well-being of their populations, having equity as a observed in the 12 years old mean caries preva-
fundamental principle (2). lence, through the 1970s and mid 1980s, whereas
The participants of the Commission defined the social factors accounted for 65% of the observed
theory of Dahlgren and Whitehead as one of the reduction (9). These findings undoubtedly may
references used to explain equity in health (3). challenge the still dominant biomedical paradigm
According to this far-reaching theoretical model, in dentistry, because they made it explicit that
equity in health is determined at different levels, socioeconomic factors, such as education levels, the
ranging from the individual to the collective, percentage of economically active highly educated
involving public health policies aimed at equality women and the level of social inequality were able
and the strengthening of individuals and com- to explain 65% of the observed reduction of dental
munities, improved access to essential services caries. These results also confirm that socioeco-
and macro-economic and cultural change. nomic status is strongly related to dental caries
The Division of Equity at the World Health (9–11).
Organization defines health equity as the absence Emphasis has been clearly made in recent liter-
of unfair, avoidable or unnecessary differences in ature on social determinants and their impact on
relation to the health of a given population or health as a whole and on oral health in particular
several groups, within or between countries, (8, 12–17). Political and sectorial agendas working
defined by social, economic, demographic or on social determinants of health can encourage the
geographic criteria (2, 4).Social disadvantages, effective fulfilment of the MDG in nations, states
mainly when accumulated during childhood and and cities. It is therefore important to further
analysed throughout the life course of a person, analyse social determinants of health through the
can exacerbate health inequities (5–7). Inequity associations between MDG indicators and oral
implies failure to avoid or overcome health health indicators.
differences that breach human rights, and are
deeply rooted as unfair social stratification.
Health inequity can therefore be defined as a
moral category engrained in political reality and
Method
in the negotiation of social relations of power This is an ecological study, involving the use of
(2, 4). aggregated data suitable for measuring the health
Widespread poor oral health is one of the most situation of human groups taken globally, and how
evident expressions of inequity with regard to their health is influenced by social, environmental
poverty and social and health exclusion (8). In this and behavioural conditions (18).
sense, the MDG indicators are also considered to be The study was divided into two distinct phases.
important measures of inequities, therefore any In Phase 1, MDG indicators were obtained from the
existing progresses of MDG among populations 2000 demographic census undertaken by the
can be used to guide the analysis of their health Brazilian Institute of Geography and Statistics
dynamics, including oral health. (IBGE) (19), the Ministry of Health database
198Millennium development goals and oral health
(DATASUS) (20) and the UNDP Human Develop- to evaluate assumptions and limitations and to
ment Atlas (21) for the year 2000. Nine MDG estimate the number of principal components from
variables were selected, based on the theoretical eigenvalues. An eigenvalue can be thought of as
input obtained from the review of the literature an index of variance. In principal components
and also based on the availability of information analysis, each principal component yields an
about 49 cities in Southern Brazil, namely: (i) the eigenvalue, which is the amount of the total
percentage of people below the poverty line, variance explained by the component. The
corresponding to the family per capita income of adopted criterion was what is used usually in
less than ½ a minimum wage (Source: UNDP) (21); the specialized literature of the area, the test of
(ii) percentage of functionally illiterate people (less larger eigenvalue than 1 (23).
than 4 years of education); (iii) the ratio of illiterate The final stage in the development of an index
men and women (Source: IBGE) (19); (iv) the was to integrate the set of indicators into a single
mortality rate in children aged under 5 years old measure, after weighting them consistently as to
(per 1000 live births); (v) the percentage of children their relative importance in explaining the features
born to adolescent mothers aged in the range of of the synthetic MDG index. The index so obtained
10–19 years old (Source: DATASUS) (20); (vi) the facilitated further analysis, when the research
percentage of people living in homes with access to objectives aimed at ranking the study cities. Based
mains water supply and a bathroom; (vii) the on this analysis, synthetic MDG index (final scores)
percentage of people having their litter collected; were calculated, per city, using the weighted
(viii) the percentage of people with access to a average of the scores obtained from the factor
telephone; (ix) the percentage of people with a analysis of principal components of the 15 vari-
computer (Source: IBGE) (19). ables ⁄ covariates and the total variance explained
In addition, six covariates associated with oral by the 3 components, using the following equation:
health outcomes according to the literature on this SYNTHETIC MDG INDEX = [(score of the 1st
area were also obtained and analysed, namely: (i) Component · variance of the 1st Compo-
length of time, in years, the water supply has been nent) + (score of the 2nd Component · variance
fluoridated (Source: Oral Health Brazil) (22); (ii) the of the 2nd Component) + (score of the 3rd Com-
1991 Municipal Human Development Index (HDI- ponent · variance of the 3rd Component)] ⁄ total
M 1991); (iii) the 2000 Municipal Human Develop- variance. The synthetic MDG indices described
ment Index (HDI-M 2000); (iv) Per-Capita Income performance towards achieving the MDG, in terms
(Source: UNDP) (21); (v) Population; and (vi) Rate of the observational units (cities), using the regres-
of Urbanization (Source: IBGE 2000 census) (19). As sion method, combining information on those
they showed significant associations by bivariate dimensions of city structure which were likely to
analysis, they were subsequently included in the be most important for the study hypothesis and
whole analysis. developed a typology of cities based on these
Factor analysis of principal components was dimensions which could be used as a basis for
performed to find evidence of possible correlations assessing social determinants of health (23).
between the MDG variables and to simplify the In Phase 2 of the study, the oral health indicators
data by reducing the number of variables aiming at (outcome variables), the DMFT index (mean num-
statistical parsimony. This analysis assumes that a ber of decay, missing or filled permanent teeth) and
smaller number of variables exist subjacent to the the prevalence of 12 years old caries-free children
data (components), which express what the origi- were obtained from the national epidemiological
nal variables have in common. This analysis also survey undertaken in 2002–2003 (22). These
enabled the validity of the variables that made up secondary data were aggregated by city. The
the components to be evaluated, by informing population of the study was originally intended
whether or not they load the concepts they aim to to be comprised of 50 cities located in the southern
express (23). This analysis was the chosen tech- region of Brazil, which had been part of the
nique for weighting and reducing various indica- probabilistic sample of the national survey, but
tors to a single index of cities in this study. Also one city was excluded because of the data lacking
was used to confirm the theory with regard to for the 12 years old, which is the target age of this
social determinants of health. study. The final sample was therefore comprised of
Principal components extraction with Varimax 49 cities, providing total for 7119 individuals aged
(orthogonal) rotation through SPSS 14.0 was used 12 years old.
199Bueno et al.
A descriptive analysis was conducted to explore interquartile range of 1.9. The percentage preva-
association between the oral health outcome vari- lence rate of caries-free children presented mean of
ables and exposure variables. 30.7 (95% CI: 25.79–35.54); median of 31.8; standard
Finally, Spearman’s correlation was applied to deviation of 17.0; and variation interquartile range
the three principal components of the factor of 26.3.
analysis and their synthetic MDG indices in The six included covariates demonstrated signif-
relation to the 49 cities and the respective oral icant association (P = 0.00) with oral health out-
health outcomes, namely the DMFT index and comes variables when bivariate analysis was
the prevalence of caries-free children at 12 years performed. The principal components analysis
old. explained 82.16% of the total variance of the
distribution of the 15 variables ⁄ covariates in the
three principal components identified (Table 1).
The rotated loadings matrix (Table 2) determined
Results how many and which of the 15 variables ⁄ covari-
The asymmetrical distribution for the 49 cities in ables covariates were loaded in each principal
Southern Brazil in 2003 of the index CPO-D to the component.
12 years presented mean of 2.8 (95% CI: 2.37–3.20); Based on the principal components analysis, the
median of 2.3; standard deviation of 1.4; and components obtained were combined into a
Table 1. Total variance explained by the final rotated solution, for the 15 variables ⁄ covariates of 49 cities in the southern
region of Brazil, 2000
Rotation sums of squared loadings
Component Total % Variation Cumulative %
Socioeconomic condition 4.328 28.85 28.85
Human development and mother and child health 4.175 27.84 56.69
Socioenvironmental condition 3.822 25.47 82.16
Extraction method: principal component analysis.
Table 2. Matrix of rotated components, loadings and component labels, for 49 cities of the southern region of Brazil, 2000
Principal components
Human development
Socioeconomic and mother Socioenvironmental
condition and child health condition
Population (city size) 0.862
Proportion of people having a computer 0.818
Per capita income 0.817
Ratio of literate women and men 0.696
Proportion of people having a telephone 0.671
Mortality rate among children aged under 5 years )0.864
Proportion of teenage mothers (10–19 years) )0.800
HDI-M 2000 0.769
Proportion of people below the poverty line )0.736
HDI-M 1991 0.685
Functional illiteracy rate )0.628
Urbanization rate 0.833
Proportion of households having rubbish 0.814
collection
Length of time water supply has been 0.774
fluoridated (years)
Proportion of households with mains 0.703
water and a bathroom
Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization. Rotation
converged in 4 iterations. Component Scoring.
200Millennium development goals and oral health
synthetic MDG index (final score), and this made it separately, of the ‘Socioeconomic condition’ and
possible to classify the cities according to an ‘Socioenvironmental condition’ components, with
ordinal scale (Table 3), ranging from 1.14 (best the DMFT index and prevalence of caries-free
performance) to )1.50 (worst performance) (23). children. On the other hand, no association was
Spearman’s correlation (Table 4) showed a observed between these outcomes and the compo-
statistically significant association of the synthetic nent relating to ‘Human development and mother
MDG index of the performance of the cities and, and child health’. A statistically significant
Table 3. Case summaries of oral health outcomes, principal components and synthetic MDG index (decreasing order of
performance profile) in 49 cities in Southern Brazil, 2000 ⁄ 2003
Socioeconomic Human development ⁄ Socioenvironmental Synthetic
Cities DMFT % Caries-free condition mother and child health condition MDG Index
1 1.06 53.48 3.76 )0.28 )0.26 1.14
2 1.39 47.15 3.72 )0.94 0.36 1.10
3 1.30 50.37 2.31 0.53 0.24 1.07
4 1.30 52.02 1.40 0.70 0.49 0.88
5 1.12 58.85 1.05 1.05 0.35 0.83
6 2.20 33.99 0.34 1.46 0.61 0.80
7 1.19 60.45 0.65 1.13 0.18 0.67
8 1.82 41.52 0.33 0.16 0.91 0.45
9 1.63 53.85 0.48 )0.09 0.97 0.44
10 2.35 34.01 )0.41 0.91 0.83 0.42
11 1.54 43.75 )0.20 0.28 1.03 0.35
12 1.41 45.45 )0.33 0.31 1.11 0.33
13 1.61 41.50 )0.35 0.17 1.22 0.31
14 1.82 40.10 0.41 0.46 0.01 0.30
15 3.33 24.08 )0.08 0.30 0.50 0.23
16 1.83 35.35 )0.84 0.35 1.22 0.20
17 1.63 42.70 )0.17 )0.22 1.05 0.19
18 0.80 62.02 )1.11 0.42 1.38 0.18
19 3.47 25.14 )0.25 0.50 0.31 0.18
20 1.34 48.10 )0.69 )0.17 1.40 0.14
21 5.81 8.51 )0.43 0.67 )0.02 0.07
22 2.55 20.78 )0.12 1.49 )1.28 0.07
23 3.00 20.00 )0.51 1.68 )1.14 0.04
24 2.85 23.60 )0.04 1.18 )1.15 0.03
25 2.11 39.81 0.14 )0.94 0.92 0.02
26 2.29 31.85 )0.35 )0.30 0.75 0.01
27 3.48 17.72 )0.48 1.46 )1.05 0.00
28 1.63 41.40 )0.27 )0.74 1.09 )0.01
29 2.98 24.66 )0.20 )0.62 0.74 )0.05
30 4.54 5.00 )0.35 0.19 0.01 )0.05
31 3.27 29.09 )1.37 0.14 1.21 )0.06
32 3.12 18.60 )0.59 0.53 )0.25 )0.10
33 4.70 13.04 )0.34 0.55 )0.59 )0.12
34 3.80 20.53 )0.04 )0.06 )0.56 )0.21
35 3.49 18.45 0.32 )0.66 )0.33 )0.22
36 2.22 34.87 )0.42 0.09 )0.52 )0.28
37 4.01 7.69 )0.51 0.43 )0.88 )0.30
38 1.36 52.66 )0.71 )1.29 1.02 )0.37
39 3.39 19.16 0.00 )1.53 0.34 )0.41
40 7.21 4.65 )0.45 0.42 )1.50 )0.48
41 4.38 4.76 )0.93 1.01 )1.71 )0.51
42 2.30 45.39 )0.74 )0.57 )0.20 )0.52
43 2.14 32.50 )0.41 )1.14 )0.03 )0.54
44 6.28 6.98 0.30 )0.80 )1.68 )0.69
45 2.43 27.50 0.37 )0.33 )2.61 )0.79
46 5.00 0.00 )0.46 )0.34 )1.86 )0.85
47 4.08 10.59 )0.29 )1.82 )1.13 )1.07
48 4.42 10.75 )0.87 )2.60 )0.43 )1.32
49 3.44 18.18 )0.30 )3.13 )1.08 )1.50
201Bueno et al.
Table 4. Spearman’s correlation between cities MDG performance and oral health outcomes
Human development
Socioeconomic and mother and Socioenvironmental Synthetic MDG
condition child health condition Index
Coefficient P Coefficient P Coefficient P Coefficient P
DMFT )0.340* 0.017 )0.057 0.698 )0.644** 0.000 )0.699** 0.000
% Caries-free 0.342* 0.016 0.022 0.882 0.680** 0.000 0.692** 0.000
*Correlation is significant at the 0.05 level (2-tailed).
**Correlation is significant at the 0.01 level (2-tailed).
correlation was found of the DMFT and CF the DMFT index at 12 years old, as shown in
indices, respectively, with: the MDG index Fig. 2.
(R2 = 0.49 and 0.48; P = 0.00); the socioeconomic
status of the population (R2 = 0.12 and 0.12;
P = 0.02) and the socioenvironmental characteris-
tics (R2 = 0.41 and 0.46; P = 0.00). Even consider-
Discussion
ing the exclusion of the years of water supply The limitations inherent to an ecological study,
fluoridation covariate, the factor related to socio- whereby observations made at the aggregate level
environmental characteristic maintained the of analysis cannot be inferred in relation to
significant correlation with the oral health out- individuals, as well as the risk of cross-classifica-
comes (R2 = 0.37 and 0.43; P = 0.00). tion and migration between population strata
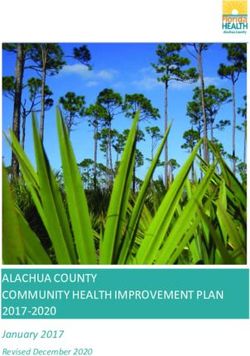
A strong correlation was observed between the must be considered when interpreting the results
outcomes mentioned and the Component relating (18). Nevertheless, one of the likely limitations
to ‘socioenvironmental condition’ which ex- of studies with such approach, which is the
plained 41% of the variance of the DMFT index collinearity of the independent (contextual) vari-
and 46% of the variance in the prevalence of ables ⁄ covariates, has been addressed and mini-
12 years old children free from caries (Fig. 1). The mized through the use of principal component
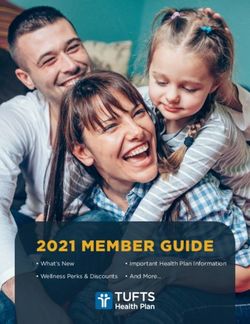
synthetic MDG index explained 48% of the analysis (23).
variance in the prevalence of 12 years old free The principal component analysis used in this
from caries and explained 49% of the variance in study demonstrated a correlation between the
Fig. 1. Correlation between socioenvironmental condi- Fig. 2. Correlation between the Final Score (municipal
tion and the prevalence of 12-year-old caries-free chil- performance profile: synthetic MDG index) and DMFT
dren, in 49 cities in southern Brazil, 2003. index in 12-year olds in 49 cities in southern Brazil, 2003.
202Millennium development goals and oral health
components relating to the cities’ MDG perfor- environmental, curricular and social attributes,
mance, as well as covariates of interest, and the oral among others, had an oral health profile superior
health outcomes. Both the overall performance of to those attending ‘unsupportive’ schools, thus
the cities analysed, as measured by the synthetic resulting in a higher percentage of caries-free
MDG index, and the components relating to schoolchildren.
socioeconomic and socioenvironmental conditions Peres et al. (40) performed an evaluation in the
demonstrated themselves to be correlated with the cities of the state of Santa Catarina on the factors
oral health indicators analysed, namely the DMFT that influence the addition of fluoride to the water
index and the prevalence of 12 years old caries-free supply system, this being a measure indicated by
children. the literature as being predominant in caries
In cities in the state of Paraná and also in prevention and the reduction of the negative
Brazil, better Municipal Human Development impact of social inequalities on caries prevalence.
Indices (HDI-M) have been associated with a The results indicate that municipalities with larger
longer period of fluoridation of the public water populations, higher indices of child development
supply and lower average dental caries experi- and lower rates of illiteracy are associated with a
ence (24, 25). longer period of implementation of water
A tendency of lower DMFT indices was observed fluoridation.
in larger cities. The effectiveness of water fluorida- General socioeconomic and socioenvironmental
tion on caries reduction is a widely accepted fact, factors have played an expressive role in explain-
both by public health specialists and by the dental ing oral health outcomes (24–43). These studies
community, in Brazil and internationally (26). The corroborate the findings of the present study, in
reduction in DMFT rates has been attributed, that the synthetic MDG index of 49 cities in
besides other important factors, to the scaling up southern Brazil explained 49% of the DMFT index
of the fluoridation of the public water supply, variance in 12 years old. This is a significant
especially in southern and south-eastern Brazil epidemiological result, because oral health out-
(27). comes are predominantly explained by biological
Baldani et al. (28) found that access of house- factors and are rarely associated with social factors.
holds to treated and fluoridated water is an In the case of dental caries, a disease of multifac-
important benefit, not only as a means of reducing torial aetiology and usually explained by individ-
caries levels but also for alleviating the impact of ual determinants, the evidences found through this
socioeconomic inequalities on caries prevalence. study can contribute towards more in-depth
These authors also used education indicators such analyses of the social determinants indicated by
as the illiteracy coefficient, the average number of the MDG with regard to caries experience in
years of schooling and repeated school years and populations.
the percentages of children aged 7–14 years not
attending school, among others to show the higher
prevalence of caries in cities in the state of Paraná
Conclusion
with the worst education indicators.
Social class and degrees of hardship have been MDG indicators have significant associations with
associated with dental caries, periodontal diseases, oral health indicators. Both the overall perfor-
tooth loss and toothlessness in adults and children mance of the cities analysed, measured by the
in the United Kingdom, Australia, New Zealand use of the synthetic MDG index, and their
and Chile (16, 17, 29–34). principal factorial components in relation to
In Brazil, there has been an increase in the socioeconomic and socioenvironmental conditions
evidence that average caries experience follows the demonstrate themselves to be correlated to oral
same international tendency in relation to social health indicators. As such, intersectoral public
and health inequities faced by the population policies based on population strategies that act on
(35–40). the social determinants of general and oral health
Moysés et al. (38) in an evaluation of state need to be integrated. However, longitudinal
schools in poor outlying districts of Curitiba studies are needed to evaluate in greater depth
benefited by health promotion policies, observed the performance and the impact of the public
that students attending better schools, referred to healthy policies monitored in this study using the
as ‘supportive’ schools based on their physical, MDG.
203Bueno et al.
gradient: implications for theoretical explanations.
References Community Dent Oral Epidemiol 2006;34:310–9.
1. United Nations Information Centre. United Nations 17. Sabbah W, Tsakos G, Chandola T, Sheiham A, Watt
Millennium Declaration – 2000. Lisbon: United RG. Social gradients in oral and general health. J
Nations Information Centre; 2001. Dent Res 2007;86:992–6.
2. Commission on Social Determinants of Health. A 18. Morgenstern H. Ecologic studies. In: Rothman KJ,
Conceptual Framework for Action on the Social Greenland S, editors. Modern Epidemiology. Phila-
Determinants of Health. Vancouver: Commission on delphia, PA: Lippincott-Rave Publishers, 1998;
Social Determinants of Health; 2007. 459–80.
3. Dahlgren G, Whitehead M. Policies and Strategies to 19. Brazilian Institute of Geography and Statistics
Promote Social Equity in Health. Stockholm: Institute (IBGE). Available at: http://www.ibge.gov.br [last
for Future Studies; 1991. accessed 9 March 2008].
4. Whitehead M. The concepts and principles of equity 20. Brazil, Ministry of Health. Available at: http://
and health. Int J Health Serv 1992;22:429–45. www.saude.gov.br [last accessed 18 March 2008].
5. Watt RG. From victim blaming to upstream action: 21. United Nations Development Programme (UNDP).
tackling the social determinants of oral health Brazilian human development atlas; available at:
inequalities. Community Dent Oral Epidemiol http://www.pnud.org.br [last accessed 27 March
2007;35:1–11. 2008].
6. Bastos JL, Peres MA, Peres KG, Araújo CL, Menezes 22. Brazil, Ministry of Health. Health Care Secretariat.
AM. Toothache prevalence and associated factors: a Basic Care Department. 2003 Brazilian Oral Health
life course study from birth to age 12 yr. Eur J Oral Project: Oral Health Conditions of the Brazilian
Sci 2008;116:458–66. Population 2002–2003: Principal Results. Brazil:
7. Nicolau B, Marcenes W, Hardy R, Sheiham A. A life- Ministry of Health; 2004.
course approach to assess the relationship between 23. Pestana MH, Gageiro JG. Factorial Analysis. In:
social and psychological circumstances and gingival Pestana MH, Gageiro JG, editors. Análise de dados
status in adolescents. J Clin Periodontol 2003;30: para Ciências Sociais: a complementaridade do
1038–45. SPSS, 3rd edn. Lisboa: Edições Sı́labo, 2003;
8. Petersen PE. The World Oral Health Report 2003: 495–544.
Continuous improvement of oral health in the 21 st 24. Gabardo MCL, da Silva WJ, Moysés ST, Moysés SJ.
century – the approach of the WHO Global Water fluoridation as a marker for sociodental
Oral Health Programme. Community Dent Oral inequalities. Community Dent Oral Epidemiol
Epidemiol 2003;31:3–24. 2008;36:103–7.
9. Nadanovsky P, Sheiham A. The relative contribution 25. Moysés SJ, Gabardo MCL, Silva WJ, Olandoski M,
of dental services to the changes in caries levels of Moysés ST. Inequalities in public water supply
12 year-old children in 18 industrialised countries in fluoridation in Brazil: An ecological study. BMC
the 1970s and early 1980s. Community Dent Oral Oral Health 2008;8:9.
Epidemiol 1995;23:331–9. 26. Narvai PC, Frazão P, Castellanos RA. Dental caries
10. Charmichael CL, Rugg-Gunn A, French AD, Cranage experience decline in permanent teeth of the brazil-
JD. The effect of fluoridation upon the relationship ian schoolchildren at end of XX century. Odont Soc
between caries experience and social class in 5 years- 1999;1:25–9.
old children in Newcastle and Northumberland. Br 27. Antunes JL, Peres MA, de Campos de Mello TR,
Dent J 1980;149:163–7. Waldman EA. Multilevel assessment of determinants
11. O’Brien M. Children’s dental health in the United of dental caries experience in Brazil. Community
Kingdom 1993. In: Her Majesty’s Stationery Office Dent Oral Epidemiol 2006;34:146–52.
editor. Report of Dental Survey, Office of Population 28. Baldani MH, Narvai PC, Antunes JLF. Dental caries
Censuses and Surveys. London: HMSO; 1994. 74–6. and socioeconomic conditions in the State of Paraná,
12. U. S. Departament of Health and Human Services. Brazil, 1996. Cadernos de Saúde Pública 2002;18:
Oral health in America: a report of the Surgeon 755–63.
General. Rockville, MD: U. S. Departament of Health 29. Watt R, Sheiham A. Inequalities in oral health: a
and Human Services, National Institutes of Health, review of the evidence and recommendations for
National Institute of Dental and Craniofacial Re- action. Br Dent J 1999;187:6–12.
search. NIH publication 00-4713; 2000. 30. Locker D. Deprivation and oral health: a review.
13. Sheiham A, Watt RG. The common risk factor Community Dent Oral Epidemiol 2000;28:161–9.
approach: a rational basis for promoting oral health. 31. Nuttall N. The prevention of social inequalities in
Community Dent Oral Epidemiol 2000;28:399–406. oral health. In: Murray JJ, Nunn JH, Steele JG,
14. Lopez NJ, Smith PC, Gutierrez J. Higher risk of editors. Prevention of Oral Disease. Oxford: Oxford
preterm birth and low birth weight in women with University Press, 2003; 250–66.
periodontal disease. J Dent Res 2002;81:58–63. 32. Thomson WM, Mackay D. Child dental caries
15. Lopez NJ, Smith PC, Gutierrez J. Periodontal therapy patterns described using a combination of area-based
may reduce the risk of preterm low birth weight in and househol-based socioeconomic status measures.
women with periodontal disease: a randomized Community Dent Health 2004;21:285–90.
controlled trial. J Periodontol 2002;73:911–24. 33. Lopez R, Fernandez O, Baelum V. Social gradients in
16. Sanders A, Slade GD, Turrel G, Spencer AJ, Marcenes periodontal disease among adolescents. Community
W. The shape of the socioeconomic-oral health Dent Oral Epidemiol 2006;34:184–96.
204Millennium development goals and oral health
34. Sanders AE, Spencer AJ, Slade GD. Evaluating the relation to Healthy Cities in Curitiba, Brazil. Health
role of dental behaviour in oral health inequalities. Place 2006;12:48–64.
Community Dent Oral Epidemiol 2006;34:71–9. 40. Peres MA, Fernandes LS, Peres KG. Inequality of
35. Patussi MP, Marcenes W, Croucher R, Sheiham A. water fluoridation in Southern Brazil – the inverse
Social deprivation, income inequality, social cohesion equity hypothesis revisited. Social Sci Med
and dental caries in Brazilian school children. Social 2004;58:1181–9.
Sci Med 2001;53:915–25. 41. Ferrazzano GF, Scaravilli MS, Ingenito A. Dental and
36. Antunes JLF, Frazão P, Narvai PC, Bispo CM, periodontal health status in Campanian children and
Pegoretti T. Spatial analysis to identify differentials relation between caries experience and socio-eco-
in dental needs by area-base measures. Community nomic behavioural factors. Eur J Paediatr Dent
Dent Oral Epidemiol 2002;30:133–42. 2006;7:174–8.
37. Antunes JLF, Narvai PC, Nugent ZJ. Measuring 42. Ahmed NA, Astron AN, Skaug N, Petersen PE.
inequalities in the distribution of dental caries. Dental caries prevalence and risk factors among
Community Dent Oral Epidemiol 2004;32:41–8. 12-year old schoolchildrem from Baghdad, Iraq: a
38. Moysés ST, Moysés SJ, Watt RG, Sheiham A. Asso- post-war survey. Dent J 2007;57:36–44.
ciations between health promotion schools’ policies 43. Pau A, Khan SS, Babar MG, Croucher R. Dental
and indicators of oral health in Brazil. Health pain and care-seeking in 11–14-yr-old adolescents
Promotion International 2003;18:209–18. in a low-income country. Eur J Oral Sci 2008;
39. Moysés SJ, Moysés ST, McCarthy M, Sheiham A. 116:451–7.
Intra-urban differentials in child dental trauma in
205You can also read