Orthopedic reviews open access journal - eISSN 2035-8164 ı ISSN 2035-8237 ı www.pagepress.org/or
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

open access journal orthopedic reviews eISSN 2035-8164 ı ISSN 2035-8237 ı www.pagepress.org/or

Orthopedic Reviews 2016; volume 8:6256
Treatment of osteoarthritis erature is the dual hinge push brace, followed
by the single hinge pull. Correspondence: Steven Phillips, Global
of the knee with bracing: While a large increase in the number of Research Solutions, Inc., 3228 South Service
a scoping review studies evaluating the treatment of knee Road, Suite 206, Burlington, ON, L7N 3H8
Canada.
osteoarthritis with bracing has occurred in the
E-mail: phillips.steve.a@gmail.com
Steven Phillips,1 Chuan Silvia Li,1,2 past 5 years, there is a lack of high quality
Mark Phillips,1 Markus Bischoff,3 studies evaluating the efficacy of the tech- Key words: Knee bracing; osteoarthritis; litera-
Pervez Ali,4,5 Jas Chahal,6 Matthew nique, as well as a lack of studies comparing ture review.
Snider,3,7 Mohit Bhandari8 bracing types and models.
Acknowledgements: the authors would like to
1
Global Research Solutions Inc., thank Sofia Bzovsky, Olivia Yu, and Sarah Gilbert
for their assistance in data collection.
Burlington, ON; 2Department of Clinical
Epidemiology and Biostatistics, McMaster Introduction Contributions: the authors contributed equally.
University, Hamilton, ON; 3Division of
Orthopedic Surgery, McMaster As one of the leading causes of disability, Conflict of interest: SP, MP and CSL are employ-
University, Hamilton, ON; 4The ees of Global Research Solutions. Dr. Cahal, Dr.
knee osteoarthritis (OA) results in a substan-
Ali, Dr. Bischoff and Dr. Snider report no conflicts
Scarborough Hospital, Toronto, ON; tial decrease in quality of life from people suf- of interest. Dr. Bhandari reports personal fees
5Department of Surgery, University of
fering from the disease, as well as a large eco- from Smith & Nephew, Stryker, Amgen, Zimmer,
Toronto, ON; 6Toronto Western Hospital nomic burden on society.1,2 There are numer- Moximed, Bioventus, Merck, Eli Lilly, Sanofi,
and Women’s College Hospital, University ous treatment methods available for knee OA Ferring, Conmed, grants from Smith & Nephew,
of Toronto Orthopedic Sports Medicine including conservative treatment for milder DePuy, Eli Lily, Bioventus, Stryker, Zimmer,
Amgen, outside the submitted work.
Program (UTOSM), Toronto, ON; 7Grand OA and operative management for severe OA.
River Hospital, Kitchener, ON; 8Division Current clinical guidelines recommend the Funding: the work was supported by a grant from
of Orthopedic Surgery, Centre for use of conservative treatment options to allevi- Össur (Reykjavik, Island).
Evidence-Based Orthopedics, McMaster ate OA related symptoms in order to postpone
University, Hamilton, ON, Canada total knee arthroplasty.3 Received for publication: 14 October 2015.
Knee bracing offers a conservative, non- Accepted for publication: 20 October 2015.
invasive treatment option to alleviate the
This work is licensed under a Creative Commons
symptoms of knee OA by decreasing biome- Attribution NonCommercial 4.0 License (CC BY-
chanical loads on the knee.4,5 Numerous differ- NC 4.0).
Abstract ent braces have been developed, evaluated,
and manufactured.6 These braces are designed ©Copyright S. Phillips et al., 2016
Knee osteoarthritis is a leading cause of dis- to decrease loads within the knee, and accom- Licensee PAGEPress, Italy
Orthopedic Reviews 2016;8:6256
ability around the world. Knee bracing pro- plish so by using various hinge types (single
doi:10.4081/or.2016.6256
vides a conservative management option for hinge or dual hinge) as well as decreasing the
symptom relief. A variety of different bracing load in either the medial or lateral compart-
types, manufacturers and products are cur- ments of the knee by applying a valgus or varus
rently available on the market. The goal of this external force to the knee, respectively. The
study is to examine the current state of the lit- application of this force can be applied either
erature regarding the treatment of knee by the brace pushing (push brace) or pulling
Materials and Methods
osteoarthritis with unloader bracing, specifi- (pull brace) on the knee in order to apply the
cally examining the representation of specific required force to decrease the load on the tar- Scoping review methodology
brace types, manufacturers and models within get compartment of the knee joint.
the literature. overview
Several systematic review have been pub-
A scoping review technique was used A scoping review is a literature review
lished evaluating the efficacy of knee bracing
because of its ability to evaluate research method allowing researchers to summarize a
in the treatment of knee OA, and a recent liter-
activity within an area of study and identify range of evidence in order to describe the
ature review summarized the literature
gaps within the literature. A thorough search breadth and depth of a field.8 Unlike systematic
regarding specific brace models.6-8 Although
of the MEDLINE database was conducted for reviews which address the current literature
these reviews evaluate and summarize the
articles where a knee brace model was identi- on a narrow focus, a scoping review addresses
efficacy of bracing, an examination of trends
fied, and we identified characteristics of the broader research questions where an abun-
studies to evaluate important information within the literature regarding brace types and
manufacturers has not been conducted. dance of interventions or study designs may be
about the body of literature related to knee relevant.9 The literature involving the treat-
bracing for the treatment of osteoarthritis. Therefore, the goal of this scoping review is to
summarize the state of literature on the use of ment on knee OA with bracing covers a wide
Fifty eligible studies were identified. The
knee braces for the treatment of knee OA. The variety of bracing types and study designs.
majority of studies have been published in the
United States, and a large increase in the objectives of this review are: i) to summarize With little known about the types of literature,
number of publications in this field was seen the body of literature and examine trends in or the representation of specific products with-
between 2010-2014. The most prominent study the treatment of knee OA with bracing and ii) in the current literature, performing a scoping
type was prospective comparative studies to determine the representation of different review to map the extent, range, and nature of
(44%), however there is a lack of randomized knee bracing manufacturers, models and available research was the most appropriate
controlled trials (6%) within the literature. hinge types within the current literature. synthesis methodology.
The most prominent hinge type within the lit-
[page 50] [Orthopedic Reviews 2016; 8:6256]
Review
Literature search which 32 studies were duplicates, which left
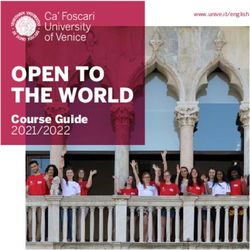
A literature search was conducted on knee Results 331 articles for consideration for inclusion in
bracing for the treatment of OA. Using a combi- this review. We excluded 281 studies due to:
nation of keywords and medical subject heading Citation retrieval being animal studies (3), not written in
(mesh) terms related to knee OA and bracing, English (17), were not relevant to bracing
The search strategy and supplemental
we performed a detailed search of MEDLINE (69), did not focus on knee OA (76), the brace
search identified a total of 363 articles, of
(Table 1). The search was performed in July,
2014. The search was limited to articles pub-
lished up to July, 2014 and to studies published
in English. After the search, a supplemental Table 1. Search strategy.
search was performed in order to look for any
Searches Results
additional articles related to the topic by exam-
ining articles referenced within the articles 1 Braces/or unloader knee brace.mp. 4434
retrieved from the initial literature search. 2 Knee brace.mp. 241
3 Knee osteoarthritis.mp. or osteoarthritis, knee/ 12,050
Study selection
4 Osteoarthritis.mp. or osteoarthritis/ 56,155
Titles and abstracts from the literature
search were compiled and reviewed for eligi- 5 (Osteoarthritis or osteoarthritic).mp. or osteoarthritis/ 57,016
bility. Studies were included if they focused on 6 (Brace* or bracing).mp. 8606
the treatment of knee OA using bracing. 7 1 or 2 or 6 8606
Studies included were meta-analyses, system- 8 3 or 4 or 5 57,016
atic reviews, randomized controlled trials, sur- 9 7 and 8 252
veys, prospective and retrospective compara-
tive studies, case series and conference
abstracts. We excluded basic science and bio-
mechanical research and studies where the
brace brand was not specified (Figure 1).
Studies that were not published in English and
studies that could not be retrieved were also
excluded.
Data abstraction
Important characteristics from each includ-
ed study were abstracted to understand the
characteristics of the literature. These vari-
ables included the year of publication, the geo-
graphic region where the study was conducted,
study design, study perspective, outcomes
assessed, and the model and manufacturer of
the brace examined.
Data analysis
Descriptive statistics were used to summa-
rize all data. Counts, proportions and percent-
ages were used to describe all data. Knee brace
manufacturers and models within the litera-
ture were represented by the number of arti-
cles that each manufacturer/model was exam-
ined in. A manufacturer can only be referenced
once in each article, however within a given
article a manufacturer may have several mod-
els referenced.
Studies were classified by level of evidence.
Level I evidence is high quality randomized
controlled trials and systematic reviews of ran-
domized controlled trials. Level II evidence
includes lower quality randomized controlled
trials, prospective comparative studies, and
systematic reviews of level II evidence. Level
III evidence consists of retrospective compara-
tive studies and level IV evidence includes case
studies. Level V evidence consists of opinion
Figure 1. Literature search results.
pieces.10,11
[Orthopedic Reviews 2016; 8:6256] [page 51]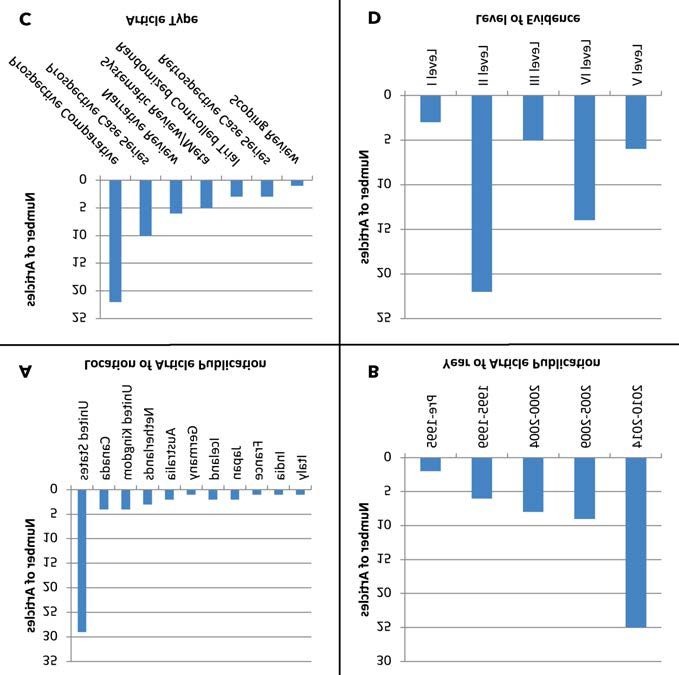
Review
brand was not specified (88), the article could
not be located (11), and biomechanical studies
(17). Therefore, 50 studies involving the use of
bracing for the treatment of knee OA were
included in this scoping review (Figure 1).
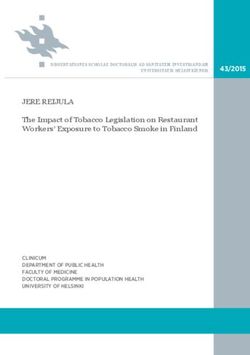
Study design and characteristics
The majority of studies were conducted in
the United States (58%), with fewer studies
conducted in Canada (8%) and the United
Kingdom (8%) (Figure 2A). While the earliest
article involving bracing for the treatment of
knee OA where a brand was specified was pub-
lished in 1986, half (50%) of all publications
have been published between 2010 and 2014
(Figure 2B). The most prevalent type of study
were prospective comparative studies (44%),
followed by prospective case series (20%) and
narrative reviews (12%) (Figure 2C). These
studies were predominantly level II (44%) evi-
dence and level IV (28%) evidence. Very few
level I studies were identified (6%) (Figure
2D). The majority of the published articles
demonstrated a positive effect of bracing
(92%), with 3 articles (6.0%) showing no
effect of bracing, and only one study (2.0%)
claiming a negative effect of bracing.
Comparison of bracing manufacturers
and models
When comparing all brace manufacturers,
ÖssurTM (Reykjavík, Island) had the most mod-
els evaluated in the published literature (8),
followed by DonJoy (DJO, Vista, CA, USA; 7
Figure 2. Study characteristics: A) location of studies; B) year of publication; C) study
models), Breg Inc.TM (Carlsbad, CA, USA; 5 design; D) level of evidence (N=50).
models), and BledsoeTM (Carlsbad, CA, USA; 4
models) (Table 2).
Similarly, the most commonly evaluated
brace manufacturer was Össur (27 articles),
followed by DonJoy (17 articles), and Breg (11
articles) (Table 2). Across the 14 manufactur-
ers, 36 models were examined in the litera-
ture, of which the models evaluated most fre-
quently were the OAdjuster (DonJoy; 13 arti-
cles), the Generation II (Össur; 10 articles),
Unloader (Össur; 9 articles), OAsys (Össur; 8
articles), Unloader ADJ (Össur; 8 articles), and
OA Defiance (DonJoy; 7 articles) (Table 2).
Between the years of 2010-2014, Össur braces
were most commonly evaluated in the litera-
ture (11 articles), followed by DonJoy (10 arti-
cles) and Breg (6 articles) (Figure 3).
Two manufacturers had level I studies with-
in the literature; Össur (2 studies) and
Cropper Medical Inc. (Ashland, OR, USA; 1
study) (Table 3). Össur had the most level II
studies (8 studies) followed by DonJoy (7 stud-
ies). The brace models that were evaluated in
level I studies were the Generation II (Össur),
the OAsys (Össur) and the Bioskin Q (Cropper
Medical) (Figure 4). The brace most refer-
enced in level II studies was the OAdjuster
(DonJoy; 6 studies), followed by the Unloader Figure 3. Number of references for the 5 most referenced bracing manufacturers over
time.
(Össur; 3 studies). The manufacturer with the
[page 52] [Orthopedic Reviews 2016; 8:6256]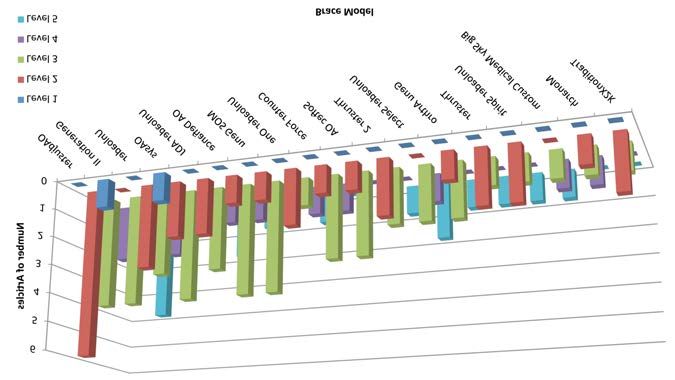
Review
Table 2. Knee brace manufacturers and models.
Manufacturer Articles referenced* Model Articles referenced*
Össur (Reykjavík, Island) 27 Generation II 10
Unloader 9
OAsys 8
Unloader ADJ 8
Unloader One 5
Unloader Select 5
Unloader Spirit 4
Unloader Express 1
DonJoy (Vista, CA, USA) 17 OAdjuster 13
OA Defiance 7
Monarch 3
On-Track 2
Montana 1
OA Lite 1
OA Nano 1
Breg (Carlsbad, CA, USA) 11 Counter Force 5
Tradition X2K 3
Fusion OA 2
Patellar Tracking Orthosis 2
Tradition 1
Bauerfeind (Zeulenroda, Germany) 8 MOS Genu 6
Softec OA 5
Bledsoe (Carlsbad, CA, USA) 8 Thruster 2 5
Thruster 4
Legacy Thruster 1
DUO 1
Otto Bock (Duderstadt, Germany) 4 Genu Arthro 4
Big Sky Medical (Missoula, MT, USA) 3 Custom Unloader 3
VQ OrthoCare (Irvine, CA, USA) 2 Free Stride 1
OActive 1
Cropper Medical (Ashland, OR, USA) 1 Bioskin Q 1
Camp Healthcare (Jackson, MI, USA) 1 Bilateral B1 1
Ongoing Care Solutions (Pinellas Park, FL, USA) 1 Orthopro OA 1
Proteor (Dijon Cedex, France) 1 ODRA 1
St. Clare Engineering Ltd (Eastleigh, UK) 1 TVS 1
* The number of articles for each manufacturer does not equal the total of all articles for models of that manufacturer as multiple models could be mentioned within the same article.
Table 3. Number of brace models by hinge type and manufacturer.
Dual hinge push Single hinge push Single hinge pull Patellofemoral Dual hinge distraction Total
Össur 1 0 7 0 0 8
DonJoy 4 2 0 1 0 7
Breg 4 0 0 1 0 5
Bledsoe 1 3 0 0 0 4
Bauerfeind 1 1 0 0 0 2
VQ OrthoCare 0 2 0 0 0 2
Otto Bock 0 1 0 0 0 1
Big Sky Medical 0 1 0 0 0 1
Cropper Medical 0 0 0 1 0 1
Camp Healthcare 1 0 0 0 0 1
Ongoing Care Solutions 1 0 0 0 0 1
Proteor 0 0 0 0 1 1
St. Clare Engineering Ltd. 0 0 1 0 0 1
Total 13 10 8 3 1 35
[Orthopedic Reviews 2016; 8:6256] [page 53]
Review
most studies with a positive outcome was
Össur (25 studies), followed by DonJoy (17
studies) and Breg (11 articles) (Figure 5).
Comparison of hinge types
Within the literature the majority of brace
models fall under three types; dual hinge push
(14 models), single hinge push (10 models)
and single hinge pull (8 models) (Table 4). Of
the 14 dual hinge push models, DonJoy and
Breg contribute the most models with 4 each.
Amongst single hinge push models 2 of the 10
models belong to Bledsoe braces, while Össur
braces comprise 7 of the 8 single hinge pull
models.
The most referenced bracing type is dual
hinge push (52 references), of which 24 refer-
ences (46.1%) belong to DonJoy braces. A com-
plete summary of braces by manufacturer is
provided in Appendix. Single hinge pull braces
are the second most referenced brace type (43
Figure 4. Level of evidence by bracing model for models with 3 or more articles.
references), with Össur braces comprising 42
(97.8%) of single hinge pull references. The
third most referenced bracing type is single
hinge push braces (26 references) of which 10
references (38.5%) belong to Bledsoe braces.
When classifying the studies by the level of
evidence for each bracing type, we found that
dual hinge push, single hinge pull and patello-
femoral braces each had one level I study in
the literature. The bracing types with the most
level II evidence were dual hinge push braces
(10 studies), single hinge push braces (9 stud-
ies) and single hinge pull braces (7 studies). A
complete summary of study designs by bracing
type is provided in Appendix.
Discussion
The purpose of this review was to summa-
rize the literature regarding knee bracing for
Figure 5. Study outcome by brace manufacturer (n=50).
the treatment of knee OA, and to examine the
Table 4. Number of articles by level of evidence by bracing manufacturer.
Manufacturer Level I Level II Level III Level IV Level V
Össur 2 8 5 6 6
DonJoy 0 7 4 3 3
Breg 0 3 3 2 3
Bauerfeind 0 2 4 1 1
Bledsoe 0 4 2 0 2
Otto Bock 0 1 2 0 1
Big Sky Medical 0 0 1 1 1
VQ OrthoCare 0 2 0 0 0
Cropper Medical 1 0 0 0 0
Camp Healthcare 0 1 0 0 0
Ongoing Care Solutions 0 1 0 0 0
Proteor 0 0 0 1 0
TVS 0 0 0 1 0
[page 54] [Orthopedic Reviews 2016; 8:6256]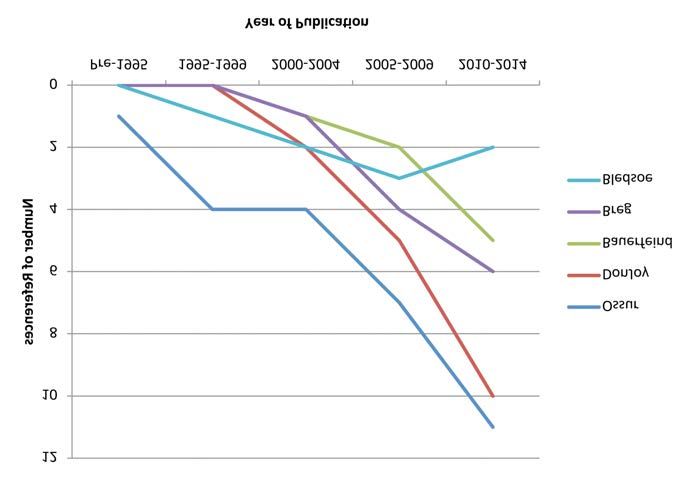
Review
representation of different OA knee brace ing articles published in English may exclude Technol Assess (Full Rep) 2007:1-157.
manufacturers, models and hinge types within applicable articles related to bracing for the 2. National Institute for Health and Care
the scientific literature. To accomplish this, a treatment of knee OA. The final limitation of Excellence. Osteoarthritis: care and man-
scoping review was performed which, unlike a this study is that only articles in which a knee agement. NICE guidelines [CG177].
systematic review, does not evaluate the data brace model was mentioned were included, February 2014. Available from:
within selected articles but rather evaluates which resulted in the exclusion of a large https://www.nice.org.uk/guidance/cg177.
articles to gain an understanding of the char- amount (88) of articles relevant to knee brac- Accessed: October 2015.
acteristics of the published literature.12 This ing for the treatment of knee OA. 3. Hochberg MC, Altman RD, April KT, et al.
approach also allows for the examination of Gaps within the current literature identified American College of Rheumatology 2012
articles that are not randomized controlled tri- in this scoping review are a lack of high quality recommendations for the use of nonphar-
als, such as systematic reviews and meta articles including randomized controlled trials macologic and pharmacologic therapies in
analyses in order to evaluate the total body of evaluating the efficacy of knee bracing for the osteoarthritis of the hand, hip, and knee.
literature associated with a selected topic. treatment of knee OA. Additionally, few articles Arthritis Care Res 2012;64:465-74.
The present scoping review identified 51 comparing hinge type or specific models are 4. Kirkley A, Webster-Bogaert S, Litchfield R,
articles pertaining to the treatment of knee OA present within the literature in order to show et al. The effect of bracing on varus
in which the model of knee brace examined is superiority to one type of brace over others. gonarthrosis. J Bone Joint Surg Am
specified. The majority of articles examining Increasing the number of high quality studies, 1999;81A:539-48.
bracing for the treatment of knee OA are pub- as well as studies comparing brace types (sin- 5. Pollo F, Otis J, Backus S, et al. Reduction of
lished in the United States (58%) between the gle versus dual hinged; push braces versus pull medial compartment loads with valgus
years 2010-2014 (50%). Prospective compara- braces) and models will provide better insight bracing of the osteoarthritic knee. Am J
tive studies were the most common type of into the efficacy of specific brace types on the Sports Med 2002;30:414-21.
study examining knee braces (44%), with very treatment of knee OA. 6. Brooks K. Osteoarthritic knee braces on
few randomized controlled trials being con- the market: a literature review. J Prosthet
ducted (6%). Articles involving bracing for the Orthot 2014;26:2-30.
treatment of knee OA generally displayed posi- 7. Feehan N, Trexler G, Barringer W. The
tive outcomes (92%) with only 4 articles indi- Conclusions effectiveness of off-leading knee orthoses
cating a neutral or negative outcome (8%). in reduction of pain in medial compart-
When examining all knee brace manufactur- The use of knee braces for the treatment of ment knee osteoarthritis: a systematic
ers and models, Össur had the most models knee OA has experienced an increase in the review. J Prosthet Orthot 2012;24:39-49.
within the literature (22.9% of all models), number of publications since 2010; however 8. Raja K, Dewan N. Efficacy of knee braces
with DonJoy (20% of all models) and Breg there is a lack of high quality evidence exam- and foot orthoses in conservative manage-
(14.3% of all models) following. Össur braces ining the efficacy of the treatment method. ment of Kkee osteoarthritis: a systematic
were examined in the most articles (54% of all Few comparative studies examining differ- reviw. Am J Phys Med Rehabil 2011;90:
articles), followed by DonJoy (34% of all arti- ences between hinge types and brace models 247-62.
cles) and Breg (22% of all articles). The most are also present within the literature. Future 9. Levac D, Colquhoun H, O’Brien KK.
studied type of brace was the dual hinge push research should aim to evaluate the efficacy of Scoping studies: advancing the methodol-
(40.9% of references), followed by single hinge bracing for the treatment of knee OA with high ogy. Implement Sci 2010;5:69.
pull braces (33.9% of references). quality studies, as well as studies examining 10. Marx R, Wilson S. Updating the assign-
Strengths of the present study are the wide differences in performance between different ment of levels of evidence. J Bone Joint
search strategy that was used to ensure an bracing types. Surg Am 2015;97A:1-2.
accurate overview of the literature available 11. DeVries J, Berlet G. Understanding levels
regarding the use of knee bracing as a treat- of evidence for scientific communication.
ment for OA of the knee, as well as the division Foot Ankle Specialist 2010;3:205-9.
of braces among manufacturers, models and References 12. Bhandari M, Morrow F, Kulkarni AV,
hinge types in order to provide a more detailed Tornetta P. Meta-analyses in orthopaedic
scope of the literature. Limitations of the pres- 1. Samson DJ, Grant MD, Ratko TA, et al. surgery. A systematic review of their
ent study are that only one database was used Treatment of primary and secondary methodologies. J Bone Joint Surg Am
to investigate the literature. Also, only select- osteoarthritis of the knee. Evid Rep 2001;83A:15-24.
[Orthopedic Reviews 2016; 8:6256] [page 55]
Orthopedic Reviews 2016; volume 8:6303
Levels of evidence in the treat- frequency to Caucasians is highest with
Polynesians (5.6:1), Blacks (3.9:1) and Correspondence: Andrew Moriarity, St. James’s
ment of slipped capital femoral Hispanics (2.5:1).1 Delayed diagnosis is Hospital, James's Street, Dublin 8, Ireland.
epiphysis: a systematic review believed to be the most important factor asso- Tel.: +353.8514.66551.
ciated with poor outcomes.3,4 Less severe and E-mail: andrewmoriarity@gmail.com
Andrew Moriarity,1 Jim Kennedy,1 stable slips have been successfully managed
Key words: Levels of evidence; systematic review;
Joe Baker,2 Pat Kiely2 with in situ pinning to protect against further slipped capital femoral epiphysis; management.
1 displacement. The treatment of high grade
St James’s Hospital, Dublin, 2Our Lady’s
unstable slips is more controversial with a Contributions: the authors contributed equally.
Hospital Crumlin, Dublin, Ireland
recent trend toward surgical hip dislocation
and reduction of the slip normally with a cor- Conflict of interest: the authors declare no poten-
rective femoral osteotomy.5 The residual tial conflict of interest.
healed deformity can lead to femoro-acetabu-
Abstract lar impingement (FAI) and eventual degenera-
Received for publication: 11 November 2015.
Revision received: 13 February 2016.
tive osteoarthritis.6,7 Accepted for publication: 14 April 2016.
The primary aim of this study was to analyze The concept of evidence-based medicine
the current level of evidence available on the (EBM) was first described in the 1980’s as the This work is licensed under a Creative Commons
surgical management of Slipped Capital conscientious, explicit, and judicious use of the Attribution NonCommercial 4.0 License (CC BY-
Femoral Epiphysis (SCFE). Secondary aims current best evidence in making decisions NC 4.0).
were to correlate the level of evidence with the about the care of individual patients.8 The EBM
impact factor of the journal to evaluate the grading system can be obtained in the Oxford ©Copyright A. Moriarity et al., 2016
Licensee PAGEPress, Italy
level of evidence over time, and to evaluate the Centre for Evidence-Based Medicine (CEBM).9
Orthopedic Reviews 2016;8:6303
geographic distribution of the studies. A study gave a level from 1 to 5 on the basis of doi:10.4081/or.2016.6303
Therapeutic studies published in English its design and as 1 of 4 different types on the
between January 1991 and August 2014 that basis of its content. Level 1 is the highest level
reported on SCFE were identified via electron- of evidence, which includes high quality, ran-
ic search was performed using the databases domized controlled trials (RCTs); and level 5, CEBM study types (Table 1) and into treatment
PubMed, EMBASE, and the Cochrane Library. is the lowest level of evidence, and includes type. If a study involved multiple treatment
The search terms used included: Slipped capi- expert opinions. This system is accepted and types it was placed in category that the majori-
tal femoral epiphyses OR SCFE OR Slipped used by most of the medical world including ty of the study involved. If the abstract did not
upper femoral epiphyses OR SUFE AND most orthopedic journals. provide enough information for classification
Management OR Treatment. Correlation Despite the importance of SCFE, to our then the full text was obtained (n=128). Once
between the level of evidence and the impact knowledge there are few studies that explore the decision was made to include the manu-
factor of the journal were analyzed together the surgical management of the condition, and script for further analysis then authorship and
with linear regression models to reveal any even fewer that are of a high level of evidence. journal of publication were assessed. Any dis-
significant trends over time. A total of 1516 The aim of this study is to review the available agreements between reviewers were resolved
studies were found, of which 321 were includ- studies on surgical management of SCFE and by discussion. The senior author was consult-
ed in the final analysis. The most frequent to categorize them by study type and level of ed if a consensus could not be reached at any
study type was the case series (51.1%) fol- evidence as proposed by the Oxford CEBM. stage of the analysis and categorization.
lowed by case reports (22.4%) and expert opin-
ion (14.0%). Randomized control trial account- Inclusion and exclusion criteria
ed for only 0.6%. The Journal of Pediatric We included all studies in English that had a
Orthopedics (American) had the most studies Materials and Methods primary emphasis on the therapeutic manage-
(22.6%) and the highest number of level 2 ment of SCFE. Prognostic and diagnostic stud-
(n=1) and level 3 (n=15) type evidence. There This review adheres to the methodology set ies were included if they defined the relation-
was no progression of level of evidence over down in the Preferred Reporting Items for ship between the treatment and the clinical
time. There was no correlation between level Systematic reviews and Meta-analyses guide- outcomes. Studies that reported solely on out-
of evidence and impact factor of journal. The lines and the Cochrane handbook.10 comes (e.g. CT evaluation of screw position)
majority of therapeutic studies on SCFE are of A systematic electronic search was per- without clinical correlation were excluded.
low level of evidence. High-level RCTs are dif- formed using PubMed (Medline), EMBASE, Reviews including systematic reviews were
ficult to perform in pediatric orthopedic sur- and the Cochrane Library. Studies published excluded if they did not primarily report on the
gery, however the management of SCFE would from January 1st, 1991 to August 1st 2014 were management of SCFE. Studies involving
benefit from well-designed, multicenter, clini- included. The following search terms were patients with genetic or metabolic distur-
cal RCTs to advance evidence-based practice. used: Slipped capital femoral epiphyses OR bances associated with SCFE were excluded.
SCFE OR Slipped upper femoral epiphyses OR Studies on animals, anesthesia and analgesia,
SUFE AND Management OR Treatment. Only biology and histology, cadavers, diagnostic
papers written in English were included. tools, economics, epidemiology, imaging
Introduction results without clinical outcome, rehabilitation
Study selection protocols, revision surgery, and surgery for
Slipped capital femoral epiphysis (SCFE) is The first two authors sorted the studies long term complications such as hip arthro-
the most common hip disorder affecting ado- based on abstracts from the electronic search. plasty for osteoarthritis were excluded.
lescents with an estimated incidence of Each author sorted through the databases, Furthermore, editorials, letters, notes, pro-
between 1 to 24.6 per 100,000 children which was then validated by the other author. ceedings, and conference abstracts were also
between the ages of 8 and 15.1,2 The relative The included studies were then sorted into excluded.
[page 56] [Orthopedic Reviews 2016; 8:6303]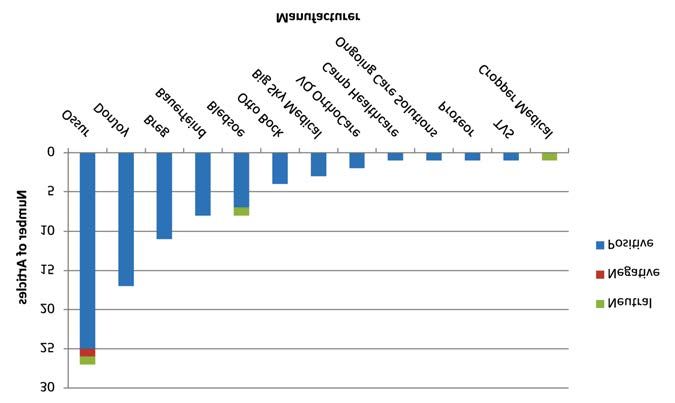
Case Report
Data selection
A database was created using Microsoft
Access (v. 2010, Microsoft). The data extracted
from the reviewed papers included: title,
author, year, journal, volume, issue, pages,
ISSN, abstract, database provider, category,
study type, level of evidence, and country. All
higher-level studies [RCT and systematic
review (SR)] had a deeper analysis performed.
The RCT was ranked level 2 if it had lesser
quality with regards to follow up, randomiza-
tion and blinding. Level of evidence of the
studies determined the SR level. General
reviews were classified as expert opinions
(level 5) as they do not meet the Cochrane cri-
teria of a systematic review. The level of evi-
dence attributed to the study by the publishing
journal was reviewed and in any cases of dis-
crepancy the researchers’ assessment was
used.
Synthesis of results
Statistical analysis was performed using
Stata (StataCorp. 2009. Stata Statistical
Software: Release 11. College Station, TX:
StataCorp LP). Peason correlation coefficients
were calculated between the mean level of evi-
dence and impact factor of journals that had 10
or more articles included.
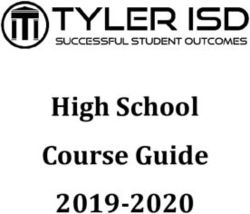
Figure 1. Flow diagram of the literature search progression.
Results
The electronic search yielded a total of 1516
results from the Medline (n=810), EMBASE
Table 1. Frequencies of the included studies.
(n=698) and Cochrane databases (n=8). A
total of 610 duplicate articles were removed: 8 Study type N. %
were from PubMed; 602 were from EMBASE.
Case series 164 51.1
Of the remaining 906 records, 452 were
removed following screening of the abstracts Case report 72 22.4
leaving a total of 454 records. Of records, 133 Expert opinion 45 14.0
were screened, based on the full text for a Comparative study (retrospective) 23 7.2
remaining 321 records, of which 307 were Systematic review 5 1.6
from PubMed, 12 were EMBASE and 2 from the Comparative study (prospective) 4 1.2
Cochrane library (Figure 1).
Case control 4 1.2
Characteristics of studies Randomized control trial 2 0.6
The most frequent study type was the case Economic and decision analysis 2 0.6
series (n=164; 51.1%) followed by case reports
(n=72; 22.4%). The results from categoriza-
tion are shown in Table 1. The most frequent
level of evidence was type 4 (n=166; 51.7%)
and results of the level of evidence classifica- Table 2. Distribution of level of evidence.
tion are shown in Table 2. The level 2 evidence
studies were both RCTs (n=2; 100%). Level of evidence N. %
The top 8 journals by number of publications 1 0 0
represented 63.9% of all studies (Table 3). The
2 2 0.6
Journal of Pediatric Orthopaedics (JPO), The
Journal of Pediatric orthopaedics B (JPOB) 3 36 11.2
and Clinical Orthopaedics and Related 4 166 51.7
Research (CORR) had the most number of 5 117 36.4
[Orthopedic Reviews 2016; 8:6303] [page 57]
Case Report
Table 3. Frequency and distribution of level of evidence in the top 8 journals. Total % is calculated as a percentage of the total amount
of studies. The level of evidence % is calculated as a percentage of the corresponding journal’s studies.
Journal Impact factor Level of evidence Total
1 2 3 4 5
N. % N. % N. % N. % N. % N. %
JPO 1.5 1 1.4 15 20.2 55 74.3 3 4.1 74 22.6
JPO-B 0.6 4 10.0 20 50.0 16 40.0 40 12.2
Clin Orthop Relat Res 2.8 1 2.8 4 11.1 23 63.9 8 22.2 36 11.0
JBJS - Am 5.3 4 16.0 16 64.0 5 20.0 25 7.6
JBJS - Br 3.3 6 66.7 3 33.3 9 2.8
Arch Orthop Trauma Surg 1.6 2 28.6 2 28.6 3 42.9 7 2.14
Int Orthop 2.1 1 14.2 5 71.4 1 14.2 7 2.14
Orthopedics 0.9 3 42.9 4 57.1 7 2.14
studies at 46.7% of all studies. JPO had the Table 4. Distribution of studies by level of evidence and region.
most studies (n=74; 22.6%) and the highest Region Level of evidence Total
number of level 2 (n=1) and level 3 (n=15) 1 2 3 4 5
type evidence. There was no significant corre-
lation between the level of published evidence N.A 2 20 90 77 189
and journal impact factor (Table 3). Europe 9 53 12 74
Over the 23.5-year time period examined, Asia 2 11 24 37
there has been no change in the mean level of
Africa 1 3 4
evidence published. The majority of studies
from 1991 to 2003 were level 4 and 5 case Australia 1 4 5
series/reports (91%) and this remained rela- S.A. 2 4 6
tively unchanged by 2014 (87.6%). The geo- Middle east 2 3 1 6
graphical location of the studies is given in
Table 4. North American journals were noted to
have published 58.9% of the available litera- inherent in the surgical management of chil- Zaidi and colleagues and Obremskey and col-
ture within the reference period, 23.1% of pub- dren. When examining our findings in the con- leagues both proposed that a level-4 study such
lications originated from Europe and 11.5% text of other similar studies our results do not as a retrospective case series could become a
from Asia with the remaining publications stand in isolation. Ostlie and colleagues level 3 study with an historical control
equally distributed across Africa, Australia and reported that RCTs represented only 0.05% of group.13,19 Level 4 studies can provide valuable
the Middle East. all pediatric general surgery studies in the past information for patient management if they
The largest amounts of studies examining decade.11 Within the broader orthopedic litera- are well designed, this includes a prospective,
the surgical treatment options in SCFE were ture therapeutic studies with level 4 and 5 evi- homogenous patient population, strict inclu-
those involving the use of single percutaneous dence are the most common orthopedic stud- sion and exclusion criteria, standardized treat-
in situ screws. Most of the studies were level 4 ies reported in the literature.12-14 Cashin and ment protocol, close patient follow up and pre-
(n=55) followed by level 3 (n=12) and level 2 colleagues examined all available studies pub- determined outcome measures.13
(n=1) evidence as displayed in Table 5. lished in JPO, JPO-B and The Journal of Our finding of no progression of evidence
Children’s Orthopaedics over a four year peri- within the field of SCFE treatment over the ref-
od and determined that evidence graded level 1 erence period is not consistent with the broad-
and 2 made up 8% of the literature while level er orthopedic literature. Fu and colleagues
Discussion and Conclusions 4 studies were again the majority at 58%.15 reviewed all publications pertaining to anteri-
We agree that the high proportion of level 4 or cruciate ligament reconstruction (ACL) over
The aim of this study was to evaluate the and 5 studies in part are due to the ethical bar- a twenty-year period and found a steady pro-
quality of evidence in the surgical manage- riers limiting the use of placebo procedures in gression in the quality of evidence over that
ment of SCFE. Our review identified 321 surgical research.16,17 Given the relative rarity time (REF).20 Zaidi and colleagues reviewed
papers reporting the clinical outcomes of of the condition we agree that cohort studies the levels of evidence of all foot and ankle arti-
SCFE. Disappointingly, but perhaps not unsur- and case reports are easier to perform, cheap- cles from the journals Foot & Ankle
prisingly, there were no published studies con- er, and less time consuming than RCTs.18 International, Foot and Ankle Surgery and the
taining level 1 evidence and there were only 2 Furthermore, RCTs are difficult to facilitate Journal of Bone and Joint Surgery (American
studies which provided level 2 evidence. due to dispersion of cases through a large and British Volumes) and found a trend
Furthermore, most of the studies examining number of centers with incumbent the varia- towards higher levels of evidence from 2000 to
specific surgical treatment options involved tion of patient presentation, and treatment by 2010 but that the proportion of low levels of
single percutaneous screw fixation and were individual surgeons.17 evidence (Level 3-4) articles remained close to
of level 4 evidence. We do not feel that this lack Improving the level of evidence in a number 90%.19 Cashin and colleagues noted a slight
of high quality evidence reflects a lack of of the level 4 studies we reviewed, could have increase in level 3 pediatric orthopedic related
respect in this condition, but instead high- been achieved by performing the study articles from 2003 to 2008 in JPO and JPO-B.15
lights the practical and ethical challenges prospectively and utilizing a control group. We accept that establishing statistically signif-
[page 58] [Orthopedic Reviews 2016; 8:6303]Case Report
icant correlation between time and evidence lished in a particular journal indexed in the studies on SCFE. This is likely due to the
grade for SCFE treatment may hampered lower Journal Citation Reports. Impact factor is the paucity of high-level studies to establish a sig-
number of publications in the field, but we feel most commonly used tool for the reader to nificant correlation. Articles pertaining SCFE
that a strong correlation, if present, would be determine if scientific studies published with- are not widely cited within the broader ortho-
demonstrated in the 326 papers identified. in a journal are widely accepted. We could find pedic literature and would not be a great influ-
Impact factor is a measure of the average no correlation between the impact factor of a ence on impact factor.
number of citations to recent articles pub- journal and the level of evidence of individual While we found that the majority of studies
Table 5. Level of evidence and number of studies supporting each surgical treatment option in the management of slipped capital
femoral epiphysis.
Treatment Level Studies
Percutaneous in situ screw fixation (single) 2 1
Percutaneous in situ screw fixation (single - prophylactic contralateral hip) 2 1
Percutaneous in situ screw fixation (single) 3 12
Percutaneous in situ screw fixation (single vs multiple) 3 4
Percutaneous in situ screw fixation (single vs staged flexion intertrochanteric femoral osteotomy) 3 4
Percutaneous in situ screw fixation (single vs multiple not specified) 3 4
Intertrochanteric versus subcapital osteotomy 3 2
Intertrochanteric femoral osteotomy 3 2
Percutaneous in situ screw fixation (single +/- manipulation) 3 1
Percutaneous in situ screw fixation vs K-wires 3 1
Percutaneous in situ screw fixation (single +/- anchorage device) 3 1
Modified osteotomy of Dunn-Fish vs osteotomy of Imhauser 3 1
Non-operative (casting) 3 1
Intertrochanteric uniplanar flexion osteotomy vs multiplanar osteotomy 3 1
Extracapsular base of neck osteotomy vs Southwick osteotomy 3 1
K-wire fixation 3 1
Percutaneous in situ screw fixation (single) 4 55
Percutaneous in situ screw fixation (single or multiple) 4 23
Percutaneous in situ screw fixation (prophylactic contralateral hip) 4 17
Femoral neck osteotomy 4 12
Percutaneous in situ screw fixation (single or multiple +/- manipulation) 4 6
Dunn's Osteotomy 4 6
Percutaneous in situ screw fixation (arthroscopic) 4 5
Intertrochanteric femoral osteotomy 4 5
K-wires 4 4
Casting and manipulation/reduction 4 4
Percutaneous in situ screw fixation vs K-wires 4 3
Percutaneous in situ screw fixation (single vs femoral osteotomy) 4 3
K-wires with open reduction 4 3
Sugioka's modified Hungria-Kramer intertrochanteric osteotomy 4 2
Closed bone graft epiphysiodesis 4 2
Subcapital osteotomy 4 2
Imhauser femoral osteotomy 4 2
TRO (trans-troch rotational osteotomy) 4 2
Percutaneous in situ screw fixation +/- casting 4 1
Steinmann pins 4 1
Intra-articular hip arthrodesis without subtrochanteric osteotomy 4 1
Valgus-flexion intertrochanteric osteotomy 4 1
Extracapsular base of neck osteotomy versus and Southwick osteotomy 4 1
Subtrochanteric osteotomy 4 1
Extracapsular vs intracapsular reduction and epiphysiodesis 4 1
Open bone peg epiphysiodesis 4 1
Sugioka's modified Hungria-Kramer intertrochanteric osteotomy 4 1
Percutaneous, opening wedge subtrochanteric femoral osteotomy 4 1
[Orthopedic Reviews 2016; 8:6303] [page 59]Case Report
originated in North America, we accept that The delay in diagnosis of slipped capital Level of evidence in anterior cruciate liga-
limiting our search to the English language femoral epiphysis: a review of 102 ment reconstruction research: a systemat-
may introduce bias in our categorization by patients. HSS J 2005;1:103-6. ic review. Am J Sport Med 2013;41:924-34.
not considering the quantity and quality of 5. Madan SS, Cooper AP, Davies AG, et al. The 13. Obremskey WT, Pappas N, Attallah-Wasif
research published outside English speaking treatment of severe slipped capital femoral E, et al. Level of evidence in orthopaedic
countries. JPO is the leading journal in SCFE epiphysis via the Ganz surgical dislocation journals. J Bone Joint Surg Am 2005;87:
publications and accounted for 22.6% of all and anatomical reduction: a prospective 2632-8.
studies. It also provided 50% of the level 2 and study. Bone Joint J 2013;95-B:424-9.
14. Hanzlik S, Mahabir RC, Baynosa RC, et al.
level 3 studies in the top eight pediatric ortho- 6. Leunig M, Casillas MM, Hamlet M, et al.
Levels of evidence in research published
pedic journals. Slipped capital femoral epiphysis: early
SCFE has potentially life changing implica- in the Journal of Bone and Joint Surgery
mechanical damage to the acetabular car-
tions for patients. This is the first review to tilage by a prominent femoral metaphysis. (American volume) over the last thirty
examine critically the quality of evidence avail- Acta Orthop Scand 2000;71:370-5. years. J Bone Joint Surg Am 2009;91:425-
able to aid in treatment decisions. It highlights 7. Beck M, Kalhor M, Leunig M, et al. Hip 8.
the paucity of high-level evidence available to morphology influences the pattern of dam- 15. Cashin MS, Kelley SP, Douziech JR, et al.
guide those, treating this challenging problem. age to the acetabular cartilage: femoroac- The levels of evidence in pediatric
We hope that this work will provide motivation etabular impingement as a cause of early orthopaedic journals: where are we now? J
for further considered and ethical study on this osteoarthritis of the hip. J Bone Joint Surg Pediatr Orthoped 2011;31:721-5.
important and challenging topic. Br 2005;87:1012-8. 16. Meakins JL. Innovation in surgery: the
8. Sackett DL, Rosenberg WMC, Gray JAM, et rules of evidence. Am J Surg 2002;183:399-
al. Evidence based medicine: what it is and 405.
what it isn’t. Brit Med J 1996;312:71-2. 17. Stirrat GM. Ethics and evidence based sur-
References 9. OCEBM Levels of Evidence Working gery. J Med Ethics 2004;30:160-5.
Group. The Oxford Levels of Evidence 2. 18. Brubaker L, Moalli P, Richter HE, et al.
1. Loder RT, Skopelja EN. The epidemiology Oxford Centre for Evidence-Based Challenges in designing a pragmatic clini-
and demographics of slipped capital Medicine. 2014. Available from:
cal trial: the mixed incontinence - medical
femoral epiphysis. ISRN Orthop http://www.cebm.net
or surgical approach (MIMOSA) trial expe-
2011;2011:486512. 10. Moher D, Liberati A, Tetzlaff J, et al.
Preferred reporting items for systematic rience. Clin Trials 2009;6:355-64.
2. Larson AN, Yu EM, Melton LJ, et al.
Incidence of slipped capital femoral epiph- reviews and meta-analyses: the PRISMA 19. Zaidi R, Abbassian A, Cro S, et al. Levels of
ysis: a population-based study. J Pediatr statement. Ann Intern Med 2009;151:264- evidence in foot and ankle surgery litera-
Orthop B 2010;19:9-12. 9. ture: progress from 2000 to 2010? J Bone
3. Kocher MS, Bishop JA, Weed B, et al. Delay 11. Ostlie DJ, St Peter SD. The current state of Joint Surg Am 2012;94:e1121-10.
in diagnosis of slipped capital femoral epi- evidence-based pediatric surgery. J 20. Fu FH, Schulte KR. Anterior cruciate liga-
physis. Pediatrics 2004;113:e322-5. Pediatr Surg 2010;45:1940-6. ment surgery 1996. State of the art? Clin
4. Green DW, Reynolds RAK, Khan SN, et al. 12. Samuelsson K, Desai N, McNair E, et al. Orthop Relat Res 1996;325:19-24.
[page 60] [Orthopedic Reviews 2016; 8:6303]Orthopedic Reviews 2016; volume 8:6357
Heel ultrasound scan quence of interaction of lifetime behavioural
and genetic factors. Osteoporosis has a signif- Correspondence: Faiz R. Hashmi, Trauma and
in detecting osteoporosis icant impact on the economy worldwide. In the Orthopedic Surgery, Warwick Hospital, Larkin
in low trauma fracture patients UK, it is estimated that osteoporosis is costing road, Warwickshire CV34 5BW, UK.
the Government about five million pounds Tel.: +44.0797.7268004 - Fax: +44.01926.482651.
E-mail: hashmi@btinternet.com
Faiz R. Hashmi,1 Khaled O. Elfandi2 daily.3 In the United States, the spending on
1Department of Trauma and Orthopedic osteoporosis is about seventeen billion dollars Key words: Osteoporosis; central bone density;
annually.4 quantitative ultrasound; bone mineral density.
Surgery, South Warwickshire Hospitals
NHS Foundation Trust, Warwick;
2
Department of General Medicine,
Objective Contributions: FRH, acquisition of data, concep-
The aim of this study was to find out tion, study design, drafting the article; KOE
Solihull Hospital, UK acquisition of data, conception, analysis of data,
whether heel ultrasound is as good as central
drafting the article.
bone densitometry scanning in diagnosing
osteoporosis in patients who are at high risk of Conflict of interest: the authors declare no poten-
osteoporosis. Previous studies mainly com- tial conflict of interest.
Abstract pared heel ultrasound and central bone densit-
ometry scanning (DEXA) in screening purpos- Received for publication: 9 December 2015.
Osteoporosis is the most common metabolic es, and inclusion of high risk patients for Accepted for publication: 16 May 2016.
disease with significant impact on the morbid- osteoporosis to our knowledge, has not been
ity and mortality of affected patients. This work is licensed under a Creative Commons
done previously.
Attribution NonCommercial 4.0 License (CC BY-
Osteoporosis has a significant impact on the
NC 4.0).
economy worldwide. The aim of this study was
to find out whether heel ultrasound is as good ©Copyright F.R. Hashmi and K.O. Elfandi, 2016
as central bone densitometry scanning in diag- Materials and Methods Licensee PAGEPress, Italy
nosing osteoporosis in patients who are at Orthopedic Reviews 2016;8:6357
high risk of osteoporosis. This was a prospec- This was a prospective study of patients doi:10.4081/or.2016.6357
tive study of patients comparing heel ultra- comparing heel ultrasound to central bone
sound to central bone densitometry scanning DEXA in patients who presented to the
(dual X-ray absorptiometry, DEXA) in patients. Accident & Emergency Department of
The recruited patients attended for a DEXA and negative predictive values were 60%
Birmingham Heartlands Hospital NHS Trust
scan of the left hip and lumbar spine. All sub- (95%CI: 35-85) and 82% (95%CI: 70-93). The
(now called the Heart Of England NHS
jects had an ultrasound of the left heel using likelihood ratios for positive and negative test
Foundation Trust), with a low trauma fracture.
the quantitative heel ultrasound machine. The results were 3.7 (95%CI: 1.6-8.8) and 0.55
Patients were recruited from the Accident
results of DEXA scan were blinded from the (95%CI: 0.33-0.92) respectively (Tables 2 and
and Emergency Department of Birmingham
results of ultrasound and vice versa. There 3). A positive ultrasound heel test raised the
Heartlands Hospital, who presented with low
were 59 patients who took part in the study, 12 pre-test probability of 28% to a post-test proba-
trauma fractures over an eight month period.
men and 47 women. The mean age was 66 The recruited patients attended for a DEXA bility of 60%. A negative ultrasound heel test
years (SD 11.9) and mean weight was 62.5 kg scan of the left hip and lumbar spine at Solihull lowered the pre-test probability from 28% to a
(SD 10.7). The sensitivity and specificity of the Hospital. The test results are computer gener- post-test probability of 18%.
ultrasound heel test to predict osteoporosis ated and analyzed using WHO criteria for the Specificity for predicting BMD-defined
were 53% (95%CI: 29-77) and 86% (95%CI: 75- diagnosis of osteoporosis. All subjects had an osteoporosis was high (86%), but sensitivity
96) respectively. Specificity for predicting bone ultrasound of the left heel using the was low (53%). A Heel Ultrasound result in the
mineral density (BMD)-defined osteoporosis Quantitative Heel Ultrasound machine (QUS- osteoporotic range was highly predictive of
was high (86%), but sensitivity was low (53%). 2). The results of DEXA scan were blinded from BMD-defined osteoporosis. On the other hand
A heel ultrasound result in the osteoporotic the results of ultrasound and vice versa. The a Heel Ultrasound result in the normal range
range was highly predictive of BMD-defined accuracy was presented as sensitivity, speci- (i.e. no osteoporosis) lowered the per-test
osteoporosis. A positive ultrasound heel test in ficity, predictive value and likelihood ratio. I probability from 28% to a post-test probability
high risk patients is more useful in ruling in have also estimated post-test probability of of 18%. A positive ultrasound heel test in high
osteoporosis than a negative test to rule out having osteoporosis for the study population risk patients is more useful in ruling in osteo-
osteoporosis. depending on whether the test result was pos- porosis than a negative test to rule out osteo-
itive or negative. porosis.
Introduction
Results Discussion and Conclusions
Osteoporosis is the most common metabolic
disease with significant impact on the morbid- There were 59 patients who took part in the Osteoporosis prevalence in developed coun-
ity and mortality of affected patients.1 study, 12 men and 47 women. The mean age tries is very high and is increasing especially
Osteoporosis defined by the World Health was 66 years (SD 11.9) and mean weight was with increasing age and decrease physical
Organization is a condition in which bone 62.5 kg (SD 10.7). Of the 59 patients, 17 (28%) activity.
mineral density is less than 2.5 standard devi- had osteoporosis (Table 1). The sensitivity and In the UK, NICE guideline recommend pro-
ation below the average density in gender specificity of the ultrasound heel test to predict phylactic use of antiosteoporotic medication in
matched young adults.2 It affects both men and osteoporosis were 53% (95%CI: 29-77) and high risk patients especially with low impact
women at different stages of life, as a conse- 86% (95%CI: 75-96) respectively. The positive fractures. The cast and unnecessary intake of
[Orthopedic Reviews 2016; 8:6357] [page 61]Article
medication in normal population has of WHO BMD definitions. It found BUA (Broad
have results in the normal range (osteoporosis
increased the financial burden on NHS which could fairly confidently be ruled out, with a
band ultrasound attenuation) and VOS
is already struggling. post-test probability 18%). However, there
(Velocity of sound) to have higher sensitivities
The use of Quantitative ultrasound in this would be a degree of uncertainty about the
of 77% and 69%, respectively for diagnosing
high risk group will detect patients with osteo- remaining 13.5%, who would then need a
osteoporosis in 100 women aged 60-69 years.8
porosis who can start medication and the DEXA scan to identify those with osteoporosis.
These higher sensitivities may have been due
remaining patients can be discharged safely. Previous studies of Heel Ultrasound as a
to use of higher BUA and VOS cut-off values.
In the light of the pilot Heel Ultrasound predictor of BMD have generally used conven-
As expected, specificities were lower than in
study, how can one interpret Heel Ultrasound tional sensitivity and specificity analyses only,
the above pilot study.
results? If a Heel Ultrasound result is normal not LRs, and have not used the WHO BMD def-
There is no consensus on what cut-off val-
or negative for osteoporosis, it becomes more initions. For example, two community-based
ues to use with QUS to diagnose osteoporosis.
useful in ruling out osteoporosis as it has a cross-sectional studies on 700 post-
It was found that changing the cut-off could
predictive value of 82% and LR of 0.55 (95%CI: menopausal,5 and 1000 peri-menopausal
achieve higher sensitivity, but only by accept-
0.33-0.92). Therefore, if Heel Ultrasound scans women respectively,6 found that there was a
ing higher rates of false positives (lower speci-
were performed on a population similar to the 40-50% overlap in the number of women in the
ficity) and less discriminating likelihood
pilot study population (28% prevalence of lowest quartile of both DEXA and Heel
ratios.
osteoporosis) as all of them are high risk Ultrasound measurements. Two other studies
Quantitative ultrasound has proven to be a
patients having presented with low trauma found Heel Ultrasound parameters to have a
good predictor of fracture risk in several stud-
fractures. Then 15.2% would have a Heel sensitivity of 65-70% for BMD in the lowest
ies.9 In a large prospective study of 6189 post-
Ultrasound result in the osteoporotic range quartile.7 Only one study other than this pilot
menopausal women over age 65, quantitative
(likely to have osteoporosis) and 61% would Heel Ultrasound has evaluated QUS in terms
ultrasonography of the calcaneus predicted hip
fracture as accurately as bone densitometry.10
In a larger study of 14,824 patients that includ-
ed younger women as well as men ages 42 to
82 years, quantitative calcaneal ultrasound
Table 1. Description of demographic characteristic of patients by test results (heel ultra- also was a good predictor of total and hip frac-
sound, HS); 17 patients were positive for osteoporosis defined by dual X-ray absorptiom- ture risk.11 A third study of 2837 women (463
etry scans. ages 20 to 39 years and 2374 ages 55 to 79
Characteristic HS positive HS negative P value years) found that quantitative ultrasound of
the calcaneus worked as well as central DEXA
DEXA positive 9 8 ≤1 for identification of women at high risk for
Age (years), mean ± SD 70.7±12.1 63.1±14.6 0.076 osteoporotic vertebral fractures.12 In addition
Gender to predicting fracture risk, other studies have
Male 0 12 ≤0.001 found that quantitative ultrasound is at least
Female 15 32 ≤0.001 as good as and possibly better than clinical risk
Ethnicity factors for predicting women at risk for osteo-
Caucasian 7 44 ≤0.001 porosis.13,14
Asian 2 6 ≤0.05 A major limitation to using quantitative
ultrasound as a screening tool is that the crite-
ria for diagnosing osteoporosis and recom-
mending treatment based upon ultrasound are
Table 2. Association between quantitative heel ultrasound (QUS) results and bone min- not yet well established.15 Furthermore, ultra-
eral density by dual X-ray absorptiometry in 59 patients. sound cannot reliably be used to follow women
QUS result Bone mineral density Total (n=59) who are treated for osteoporosis because of
Osteoporosis No osteoporosis limited precision and a slow rate of change of
bone mass at peripheral sites. Thus, most
Positive 9 6 15 (25.4%)
women with a high risk ultrasound finding will
Negative 8 36 44 (74.6%) need a confirmatory DEXA both to determine
the need for treatment based upon well estab-
lished guidelines, and as a baseline for moni-
Table 3. Sensitivity and specificity of heel ultrasounds in diagnosing bone mineral den- toring therapy.
sity defined osteoporosis or ruling it out.
95% CI
Sensitivity a / (a+c) 53% 29-77 References
Specificity d / (b+d) 86% 75-96
1. No authors listed. Consensus development
Pre-test Probability ( Prevalence): (a+c) / (a+b+c+d) 29% 17-40
conference: diagnosis, prophylaxis, and
Positive Predictive Value: a / (a+b) 60% 35-85 treatment of osteoporosis. Am J Med
Negative Predictive Value: d / (c+d) 82% 70-93 1993;94:646-50.
Likelihood Ratio + sens / (1-spec) 3.71 1.56-8.81 2. NIH Consensus Development Panel on
Likelihood Ratio - (1-sens) / spec 0.55 0.33-0.92 Osteoporosis Prevention, Diagnosis, and
CI, confidence interval. a, 9 (positive, osteoporosis); b, 6 (positive, no osteoporosis); c, 8 (negative, osteoporosis); d, 36 (negative, no Therapy. Osteoporosis prevention, diagno-
osteoporosis). sis, and therapy. JAMA 2001;285:785-95.
[page 62] [Orthopedic Reviews 2016; 8:6357]You can also read