Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
n ORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient
Daptomycin-Containing Regimens in Osteomyelitis
Thomas Delate, PhD, MS1,2; Julia K Nguyen, PharmD3; Jonathan T Truong, MD4; Fang Niu, MS5;
Arman Haghigatgoo, PharmD3 Perm J 2021;25:20.297
E-pub: 05/26/2021 https://doi.org/10.7812/TPP/20.297
ABSTRACT strongly recommends vancomycin as first therapy choice
Background: Use of daptomycin at doses ≥ 6 mg/kg for for a duration of 6 weeks or alternative parenteral/highly
treatment of osteomyelitis is increasing in clinical practice; un- bioavailable oral antimicrobial therapy despite the low
fortunately, limited data are available to guide optimal dosing and quality of supporting evidence.2
duration. The objective of this study was to assess daptomycin Despite its historic low acquisition cost, concerns may limit
dosing and duration regimens for osteomyelitis treatment.
vancomycin use as monotherapy in methicillin-resistant
Methods: This was a retrospective, multi-site, cohort study
S. aureus (MRSA) osteomyelitis due to its treatment failure
conducted in an integrated healthcare delivery system. Non-
pregnant patients ≥ 18 years of age with osteomyelitis diagnosed
rates as high as 46% and emergence of vancomycin-
between November 1, 2003 and June 30, 2011, ≥ 2 weeks out- intermediate S. aureus.3-5 In addition, costly routine moni-
patient daptomycin therapy, and ≥ 1 month of follow-up were toring and pharmacokinetic dose adjustments to prevent
included. Daptomycin doses < 6 mg/kg and ≥ 6 mg/kg at du- vancomycin-associated nephrotoxicity and renal failure sup-
rations of < 6 weeks and ≥ 6 weeks were examined with univariate port consideration of other empiric anti-MRSA agents.6
and multivariate analyses to assess treatment success and all- Daptomycin is a rapid, concentration-dependent bactericidal
cause mortality. agent that, unlike vancomycin, is able to kill high inocula of
Results: A total of 247 patients were included, with 39 (15.8%), both susceptible and resistant (vancomycin mic >1.5 µg/mL)
37 (15.0%), 107 (43.3%), and 64 (25.9%) receiving < 6 mg/kg staphylococci in 24 hours.7 It is administered via once daily
and ≥ 6 weeks, < 6 mg/kg and < 6 weeks, ≥ 6 mg/kg and ≥ 6 weeks,
2- or 30-minute infusion, has a modest side effect profile,
and ≥ 6 mg/kg and < 6 weeks of daptomycin therapy, respectively.
and penetrates bone.8 Available as a generic since 2016, its
Patients had a mean age of 58 years and had received prior
vancomycin therapy (65.6%). Patients receiving < 6 weeks of
acquisition cost no longer remains high as the first cyclic
therapy were less likely to experience treatment success lipopeptide of its class. Unfortunately, there are few studies
compared with ≥ 6 weeks (41.5% vs 25.3%, adjusted odds ratio = of daptomycin use in patients with osteomyelitis.
0.55; 95% confidence interval = 0.31-0.98) independent of du- One observational study noted clinical success rates of
ration. There were no differences across groups in mortality after 81%-83% with first-line daptomycin dosing between 6 and
adjustment. 10 mg/kg/d for treatment of staphylococcal osteomyelitis.9
Conclusion: In a diverse clinical population, daptomycin for A retrospective study of device-associated osteomyelitis strati-
treatment of osteomyelitis of 6 weeks or longer duration was fied by daily daptomycin dose of < 6 mg/kg, 6-< 8 mg/kg,
associated with success independent of dose. This finding sup- and ≥ 8 mg/kg reported that the longest time to treat-
ports longer treatment with daptomycin as a first-line agent in
ment failure was observed in the 6 to < 8 mg/kg group.10
antimicrobial stewardship initiatives.
Key Points Author Affiliations
1
Pharmacy Outcomes Research Group, Kaiser Permanente National Pharmacy, Aurora, CO
is retrospective cohort study evaluated 247 patients 2
Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of
who were treated outpatient with daptomycin for osteo- Colorado Anschutz Medical Campus, Aurora, CO
myelitis. After multivariable adjustment, including MRSA 3
Kaiser Permanente Southern California Outpatient Infusion Pharmacy, Panorama City Medical Center,
and risk scores, ≥ 6 weeks daptomycin treatment duration Panorama City, CA
4
Kaiser Permanente Southern California Infectious Diseases Clinic, Lancaster, CA
was associated with clinical success independent of dap- 5
Pharmacy Outcomes Research Group, Kaiser Permanente National Pharmacy, Downey, CA
tomycin dose.
Corresponding Author
INTRODUCTION Julia K Nguyen, PharmD (Julia.K.Nguyen@kp.org); Thomas Delate, PhD, MS (Tom.Delate@kp.org)
Osteomyelitis, an inflammation of bone tissue commonly Keywords: antimicrobial stewardship, bone diseases, daptomycin, home infusion therapy, infectious, vancomycin
caused by Staphylococcus aureus, requires adequate antimi-
crobial therapy often in combination with extensive surgical Abbreviations: AHR, adjusted hazard ratio; ANOVA, analysis of variance; CCI, Charlson comorbidity index; ClCr,
debridement.1 In vertebral osteomyelitis treatment guide- Creatinine Clearance; CPK, creatinine phosphokinase; FDA, Food & Drug Agency; IDSA, Infectious Diseases
Society of America; KPCA, Kaiser Permanente Northern and Southern California; Mg/kg, milligram per kilogram;
lines, the Infectious Diseases Society of America (IDSA) MIC, minimum inhibitory concentration; MRSA, methicillin-resistant Staphylococcus aureus; OPAT, outpatient
parenteral antimicrobial therapy
·
The Permanente Journal https://doi.org/10.7812/TPP/20.297 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. 1ORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
Although available data continue to drive higher daptomycin prescription after diagnosis were eligible for inclusion.
dosing (ie, ≥ 6 mg/kg/d) for indications such as endocarditis Confirmation of diagnosis was made with relevant positive
and bacteremia, extrapolation may not be apparently appli- bacterial culture from blood or overlying ulcers, wounds,
cable to Staphylococcus predominant osteomyelitis.11 Prudent fistulas, etc. for susceptible Staphylococcus, Streptococcus, and
dosing strategies for dose optimization are warranted for Enterococcus within 6 weeks before and up to 2 days after
antimicrobial stewardship, conservation of healthcare re- initiation of parenteral antibiotic or via biopsy or radiog-
sources, and patient safety. us, the aim of this study was to raphy (e.g., magnetic resonance imaging, x-ray, bone scan).
describe the patterns of care and treatment outcomes for In addition, patients had to have received at least 2 weeks
daptomycin-containing dosing regimens for osteomyelitis in of parenteral antimicrobial therapy in the outpatient
the outpatient parenteral setting. setting (defined as infusion center, skilled nursing fa-
cility, or home), > 1 month of follow-up from conclusion
MATERIALS AND METHODS of therapy, and crossover exposure to daptomycin in the
Study Design and Setting setting of vancomycin allergy, vancomycin-resistant En-
is was a retrospective, cohort study of outpatient terococcus, elevation in serum creatinine > 0.5 mg/dL while
daptomycin use in patients with osteomyelitis conducted on vancomycin, and vancomycin minimum inhibitory
in the Kaiser Permanente Northern and Southern Cal- concentration (MIC) > 1 µg/mL. All diagnoses were
ifornia (KPCA) regions. e KPCA regions are integrated verified via manual chart review. e study index date was
healthcare delivery systems and serve approximately 8 million the date of OPAT enrollment. Continuous enrollment in
members. Patients diagnosed with acute osteomyelitis (ie, KPCA during the 6 months prior to index date was required
not recurrent defined as diagnosis within 2 weeks of onset of to collect baseline characteristics reliably.
symptoms) between November 1, 2003 and June 30, 2011
were identified. Electronic chart reviews were conducted by Data Collection
multiple unblinded reviewers under the supervision of site Information on osteomyelitis diagnoses and patient
investigators. Patients were followed from date of dapto- characteristics was obtained from queries of the KPCA
mycin initiation until February 14, 2014; disenrollment electronic, administrative databases. Patient characteristics
from KPCA; or death. included age, sex, weight, and comorbidities. Information
e KPCA outpatient parenteral antimicrobial therapy on daptomycin dose and duration of use were obtained from
(OPAT) program receives referrals from hospital, infusion the OPAT administration database. Information on clinical
center, medical clinic, and skilled nursing facility settings outcomes, prior vancomycin use, MRSA infection status,
for treatment of long-term parenteral antimicrobials. e adverse events, and mortality were obtained from electronic
OPAT offers significant benefits through shorter or avoided chart reviews.
hospital stays, prevention of hospital-associated conditions,
and improved patient quality of life.12 Antimicrobial stew- Clinical Outcomes
ardship oversight is provided by prescriber consultation with e primary outcome was clinical success. is was
the OPAT interdisciplinary team, which includes an infectious defined as a composite of infection resolution and im-
diseases physician, a specialist pharmacist, and a home health provement. Resolution was defined as a subsiding of the
nurse coordinator at initiation of care and during follow-up. pathologic state based on clinical signs and symptoms of
Coded and free-text medical, laboratory, emergency de- normal baseline surrogate biomarkers: C-reactive protein
partment, hospitalization, and membership information and erythrocyte sedimentation rates, confirmatory imaging,
from within the delivery system, as well as from contracted or negative bacterial culture. Improvement was defined as
and affiliated facilities, are captured in KPCA’s administrative partial resolution of clinical signs and symptoms. Failure
and claims databases. e Kaiser Permanente Southern was defined as clinical failure, microbiologic failure, death,
California Institutional Review Board reviewed and ap- or premature discontinuation within 12 weeks of treatment
proved all study activities. Because this was a retrospective initiation. Clinical failure was defined as having no response
evaluation, informed consent was not required. on the basis of ongoing signs and symptoms of infection
and the presence of persistent abnormal biomarkers or
Patient Population documented surgical intervention. Microbiologic failure
Patients aged ≥ 18 years with a diagnosis of acute os- was defined as persistent or relapsing S. aureus infection
teomyelitis, defined as an International Classification of demonstrated by either ongoing positive cultures leading
Diseases Ninth Edition 730.xx related code, between to discontinuation of treatment or subsequent isolation
November 1, 2003 and June 30, 2011 who were enrolled of S. aureus of the same strain type after apparent clinical
in the OPAT for at least 2 weeks with a daptomycin improvement. Secondary outcomes included all-cause
2 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. ·
The Permanente Journal https://doi.org/10.7812/TPP/20.297ORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
mortality and daptomycin-related adverse events. Ele-
vated serum creatinine was defined as > 0.5 mg/dL above
the recorded value at time of initiation of therapy. Elevated
creatinine phosphokinase (CPK) was defined as > 170 (U/L)
with or without acute renal failure. Leukopenia was defined
as an absolute white blood cell count of less than 4000/µL
requiring change in therapy. An adjudication panel com-
prised of study investigators representing infectious dis-
eases medical specialty and outpatient parenteral antimicrobial
pharmacy blinded to treatment reached consensus to de-
termine final diagnosis and outcome(s) for questionable
cases.
Data Analysis
No a priori power analysis was performed because this
study was primarily descriptive in nature and all patients
meeting eligibility criteria during the study period were in-
cluded. Patients were categorized based on initial daily dap-
tomycin dose and continuous duration of therapy: ≥ 6 mg/kg Figure 1. Patient disposition.
and ≥ 6 weeks, ≥ 6 mg/kg and < 6 weeks, < 6 mg/kg
and ≥ 6 weeks, and < 6 mg/kg and < 6 weeks. Categorization
of doses at < 6 mg/kg vs ≥ 6 mg/kg was performed to assess hardware, surgical debridement, inpatient length of stay,
the lowest effective dose based on the FDA-approved MRSA status, prior vancomycin use, and CCI. A Nelson–
6 mg/kg dosing for S. aureus. Age was determined as of the Aalen cumulative hazard curve was constructed with
index date. e presence of specific comorbidities was the dose/duration groups to describe time to all-cause
determined using the Quan adaptation of the Charlson mortality. Safety of daptomycin use was described by
comorbidity index (CCI).13 e algorithm was applied to frequency of reported adverse events and elevated cre-
diagnoses collected during the 6 months prior to the index atinine phosphokinase. All data were analyzed using
date to provide a 30-point comorbidity score for each SAS version 9.4 (SAS Institute, Cary, NC). e alpha
patient. Comorbidities reported include chronic kidney was set at 0.05.
disease stage 3-5, diabetes, and hypertension.
Patient characteristics are reported as means and standard RESULTS
deviations or medians and interquartile ranges for interval- and During the 8-year study period, 2464 patients were
ratio-level variables (eg, age) and percentages for nominal- identified as having a diagnosis of osteomyelitis and had
and ordinal-level variables (eg, sex, comorbidity history). received ≥ 2 weeks of OPAT. Of these, 1580 patients
e Shapiro-Wilk test was used to assess normality for were initiated initially on vancomycin, and 247 patients
interval- and ratio-level variables. Differences across/between met all eligibility requirements (Figure 1). ere were
patient groups were tested using ANOVA/t-tests or non- 39 (15.8%), 37 (15.0%), 107 (43.3%), and 64 (25.9%)
parametric equivalent tests for interval- and ratio-level patients who received < 6 mg/kg and ≥ 6 weeks, < 6 mg/kg
variables and the χ 2 tests of association or Fischer’s exact and < 6 weeks, ≥ 6 mg/kg and ≥ 6 weeks, and ≥ 6 mg/kg
test for nominal- and ordinal-level variables. A multivariate and < 6 weeks of daptomycin therapy, respectively (Table 1).
logistic regression model was constructed to identify factors ere were 65 (26.3%), 11 (4.5%), 137 (55.5%), 13 (5.3%),
associated with clinical success including independent 15 (6.1%), 3 (1.2%), and 3 (1.2%) patients who received 4,
dose (< 6 mg/kg vs ≥ 6 mg/kg) and duration (< 6 weeks 5, 6, 7, 8, 9, and 10 mg/kg, respectively.
vs ≥ 6 weeks) variables to increase power to detect differ- Patients primarily were male, were < 65 years of age, had a
ences with these factors. A Cox proportional hazard model body mass index > 30, and had prior vancomycin exposure.
was constructed to identify factors associated with time e majority of osteomyelitis sites were lower extrem-
to all-cause mortality. All models were adjusted, based on ity infections (60.3%). e mean daptomycin dose was
clinical judgement (eg, variable indicates a risk of more 5.7 mg/kg (±1.3), and median duration of treatment was
serious infection) and statistical analysis (ie, variable with 36 days (interquartile range [IR] = 16-54 days). e
p value < 0.2 in the across groups univariate analysis), median durations of prior antibiotic treatment and all
for age, sex, diabetes comorbidity, presence of orthopedic combined antibiotic treatments were 10 (IR = 1-28) and
·
The Permanente Journal https://doi.org/10.7812/TPP/20.297 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. 34
Table 1. Patient characteristics by daptomycin dose and duration (N = 247)
p
Characteristic < 6 mg/kg and ≥ 6 wk (n = 39) < 6 mg/kg and < 6 wk (n = 37) ≥ 6 mg/kg and ≥ 6 wk (n = 107) ≥ 6 mg/kg and < 6 wk (n = 64) valuea
·
Age ≥ 65 years (n, %) 14, 35.9% 21, 56.8% 39, 36.4% 20, 31.3% 0.074
Female (n, %) 22, 56.4% 14, 37.8% 31, 29.0% 26, 40.6% 0.023
Infection site (n, %)
Head 2, 5.1% 0, 0.0% 3, 2.8% 1, 1.6%
Lower extremity 25, 64.1% 28, 75.7% 57, 53.3% 39, 60.9%
ORIGINAL RESEARCH ARTICLE
Pelvis 4, 10.3% 0, 0.0% 7, 6.5% 3, 4.7%
0.151
Spine 3, 7.7% 3, 8.1% 28, 26.2% 12, 18.8%
Thorax 0, 0.0% 2, 5.4% 1, 0.9% 2, 3.1%
Upper extremity 5, 12.8% 4, 10.8% 11, 10.3% 7, 10.9%
Mean body mass index (kg, SD) 30.3 (6.1) 33.2 (12.2) 30.3 (7.4) 30.3 (9.2) 0.674
Diabetes comorbidity (n, %) 18, 46.2% 21, 56.8% 49, 45.8% 30, 46.9% 0.699
Kidney disease stage 3-5 (n, %) 10, 25.6% 13, 35.1% 20, 18.7% 18, 28.1% 0.198
Surgical debridement (n, %) 31, 79.5% 28, 75.7% 78, 72.9% 45, 70.3% 0.762
Presence of orthopedic hardware (n, %) 11, 28.2% 4, 10.8% 31, 29.0% 18, 28.1% 0.157
Mean inpatient length of stay (days, SD) 3.9 (4.4) 7.7 (11.3) 6.7 (10.2) 8.3 (11.1) 0.058
Mean Charlson comorbidity index (SD) 4.3 (2.99) 5.2 (3.27) 3.4 (2.51) 4.3 (3.14) 0.022
MRSA infection (n, %) 20, 51.3% 14, 37.8% 47, 43.9% 24, 38.1% 0.543
Other infectious agents (n, %)
Coagulase negative Staphylococcus 3, 7.7% 4, 10.8% 20, 18.7% 11, 17.2% 0.331
Diptheroids 0, 0.0% 0, 0.0% 1, 0.9% 0, 0.0% 0.726
Enterobactericiae (Proteus, Morganella, 3, 7.7% 3, 8.1% 7, 6.5% 4, 6.3% 0.980
Providencia, Klebsiella)
Enterococcus 5, 12.8% 5, 13.5% 6, 5.6% 5, 7.8% 0.345
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved.
Pseudomonas 2, 5.1% 1, 2.7% 2, 1.9% 4, 6.3% 0.770
Methicillin-sensitive Staphylococcus aureus 4, 10.3% 4, 10.8% 13, 12.1% 7, 10.9% 0.987
Stenotrophomonas 1, 2.6% 0, 0.0% 1, 0.9% 0, 0.0% 0.510
Streptococcus 2, 5.1% 0, 0.0% 1, 0.9% 4, 6.3% 0.115
Administered anti-infectives (n, %)
Cephalosporin, Carbapenem, or B-lactam 4, 10.3% 9, 24.3% 11, 10.3% 8, 12.5% 0.159
Combination of agents 4, 10.3% 1, 2.7% 6, 5.6% 3, 4.7% 0.520
Other single agent 1, 2.6% 7, 18.9% 5, 4.7% 3, 4.7% 0.010
Vancomycin only 28, 71.9% 18, 48.6% 82, 76.6% 44, 68.8% 0.016
·
None 2, 5.1% 1, 2.7% 3, 2.8% 6, 9.4% 0.243
a
Across groups comparison.
MRSA = methicillin-resistant S. aureus.
The Permanente Journal https://doi.org/10.7812/TPP/20.297
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in OsteomyelitisORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
Table 2. Select patient characteristics by < 6 vs ≥ 6 mg/kg daptomycin dose and < 6 vs ≥ 6 wk duration (N = 247)
Characteristic < 6 mg/kg (n = 76) ≥ 6 mg/kg (n = 171) p-value1 6 wk (n = 101) ≥ 6 wk (n = 146) p valuea
Age ≥ 65 years (n, %) 35, 46.1% 59, 34.5% 0.084 41, 40.6% 53, 36.3% 0.495
Female (n, %) 36, 47.4% 57, 33.3% 0.036 40, 39.6% 53, 36.3% 0.598
Mean body mass index (kg, SD) 31.8 (9.7) 30.3 (8.1) 0.279 31.4 (10.5) 30.3 (7.1) 0.859
Diabetes comorbidity (n, %) 39, 51.3% 79, 46.2% 0.457 51, 50.5% 67, 45.9% 0.476
Kidney disease stage 3-5 (n, %) 23, 30.3% 38, 22.2% 0.176 31, 30.7% 30, 20.5% 0.069
Surgical debridement (n, %) 58, 77.3% 121, 72.0% 0.385 71, 71.7% 108, 75.0% 0.568
Presence of orthopedic hardware (n, %) 15, 19.7% 46, 26.9% 0.228 21, 20.8% 40, 27.4% 0.237
Mean inpatient length of stay (days, SD) 5.4 (8.2) 7.3 (10.6) 0.098 7.9 (11.0) 5.9 (9.1) 0.086
Mean Charlson comorbidity index (SD) 4.8 (3.1) 3.8 (2.8) 0.018 4.6 (3.2) 3.7 (2.7) 0.025
MRSA infection (n, %) 34, 44.7% 71, 41.5% 0.637 38, 37.6% 67, 45.9% 0.196
Administered anti-infectives (n, %)
Cephalosporin, carbapenem, or β-lactam 13, 17.1% 19, 11.1% 0.195 17, 16.8% 15, 10.3% 0.131
Combination of agents 5, 6.6% 9, 5.3% 0.680 4, 4.0% 10, 6.8% 0.334
Other single agent 8, 10.5% 8, 4.7% 0.085 10, 9.9% 6, 4.1% 0.069
Vancomycin only 46, 60.5% 126, 73.7% 0.038 62, 61.4% 110, 75.3% 0.019
None 3, 3.9% 9, 5.3% 0.657 7, 6.9% 5, 3.4% 0.208
a
Between groups.
MRSA = methicillin-resistant S. aureus.
Table 3. Select patient characteristics by clinical outcome status
Characteristic Clinical success (n = 168) Clinical failure (n = 79) p value
Daptomycin dose < 6 mg/kg (n, %) 54, 32.1% 22, 27.9% 0.495
Daptomycin duration < 6 wk (n, %) 59, 35.1% 42, 53.2% 0.007
Age ≥ 65 years (n, %) 64, 38.1% 30, 38.0% 0.986
Female (n, %) 63, 37.5% 30, 38.0% 0.943
Mean weight (kg, SD) 91.3 (27.4) 92.7 (28.7) 0.719
Diabetes comorbidity (n, %) 75, 44.6% 43, 54.4% 0.151
Surgical debridement (n, %) 125, 74.4% 57, 72.2% 0.708
Presence of orthopedic hardware (n, %) 50, 30.5% 14, 17.7% 0.044
Mean inpatient length of stay (days, SD) 6.1 (8.3) 8.3 (12.9) 0.281
Mean Charlson comorbidity index (SD) 3.9 (2.9) 4.3 (3.0) 0.310
MRSA infection (n, %) 70, 41.7% 35, 44.9% 0.636
Vancomycin use (n, %) 115, 68.5% 47, 59.5% 0.167
Kidney disease stage 3-5 (n, %) 37, 22.0% 24, 30.4% 0.156
MRSA = methicillin-resistant S. aureus.
49 (IR = 30-79) days, respectively. Patients in the < 6 mg/kg In univariate analyses, daptomycin duration < 6 weeks
and < 6 weeks group had the highest mean CCI (p = 0.022). was associated with clinical failure (p = 0.007) (Table 3).
Patients in the ≥ 6 mg/kg and ≥ 6 weeks group had the In multivariate analysis of clinical success, daptomycin
highest percentage of vancomycin use (p = 0.016). duration < 6 weeks was associated independently with
Comparing patients who received < 6 mg/kg with ≥ 6 mg/kg being less likely to achieve clinical success (adjusted odds
of daptomycin, patients who received < 6 mg/kg were more ratio = 0.56; 95% confidence interval [CI] = 0.31-0.97;
likely to be female and had a higher mean CCI but were less p = 0.046) (Table 4). Patients in the ≥ 6 mg/kg and ≥ 6 weeks
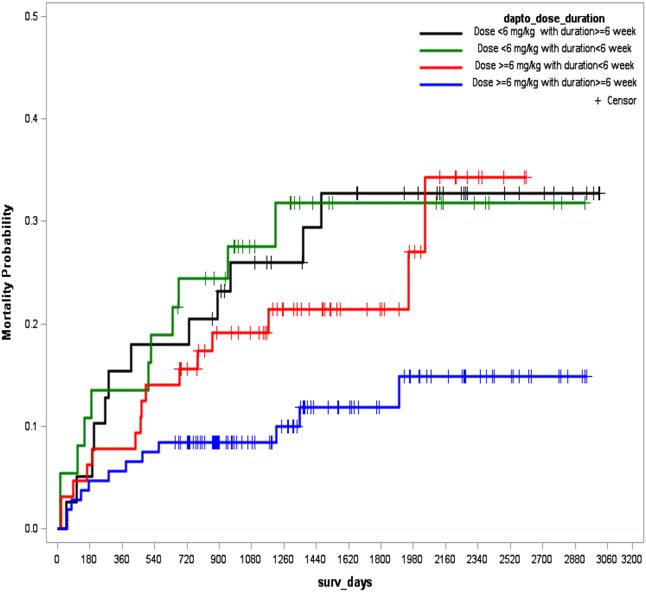
likely to have had vancomycin use (all p < 0.05) (Table 2). group had the lowest mortality (12, 11.2%) compared with
Comparing patients who had < 6 weeks to ≥ 6 weeks the < 6 mg/kg and ≥ 6 weeks (12, 30.8%), < 6 mg/kg and
duration of daptomycin therapy, patients who had < 6 weeks < 6 weeks (11, 29.7%), and ≥ 6 mg/kg and < 6 weeks (15,
of therapy had a higher mean CCI and were less likely to 23.4%) groups (p = 0.015). After adjustment, there were no
have had vancomycin use (both p < 0.05). differences in time-to-death across the groups (Figure 2).
·
The Permanente Journal https://doi.org/10.7812/TPP/20.297 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. 5ORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
Table 4. Patient characteristics tested for association with
clinical success
95% confidence
interval p
Factor Odds ratio Lower Upper value
Daptomycin dose < 6 mg/kg 1.45 0.76 2.78 0.257
Daptomycin duration < 6 wk 0.56 0.31 0.97 0.046
Female 0.84 0.45 1.57 0.588
Age ≥ 65 years 1.03 0.50 2.10 0.945
Diabetes comorbidity 0.75 0.39 1.4 0.370
Presence of orthopedic hardware 1.98 0.94 4.17 0.071
Inpatient length of stay 0.98 0.96 1.01 0.181
MRSA infection 0.90 0.50 1.63 0.731
Vancomycin use 1.56 0.84 2.90 0.158
Kidney disease stage 3-5 0.74 0.36 1.42 0.404
Charlson comorbidity index 1.02 0.90 1.15 0.790
c-statistic = 0.666; 95% confidence interval 0.594-0.737.
MRSA = methicillin-resistant S. aureus.
Figure 2. Nelson–Aalen cumulative hazard of mortality curve.
Within the survival analysis, age ≥ 65 years (adjusted
hazard ratio = 2.93; 95% CI = 1.38-6.24; p = 0.005) and first study to identify that standard daptomycin dosing of ≥
increased Charlson Comorbidity Index (adjusted hazard 6 mg/kg for ≥ 6 weeks appears to be a reasonable treatment
ratio = 1.22; 95% CI = 1.08-1.37; p = 0.001) were associated option for S. aureus osteomyelitis. is finding is aligned
with a higher likelihood of all-cause mortality (Table 5). with the IDSA’s recommendations, based on expert opinion,
In across-groups (≥ 6 mg/kg and ≥ 6 weeks, ≥ 6 mg/kg for high-dose daptomycin (8-10 mg/kg) in select populations
and < 6 weeks, < 6 mg/kg and ≥ 6 weeks, and < 6 mg/kg (eg, persistent MRSA bacteremia and vancomycin treatment
and < 6 weeks) analyses, the frequencies of adverse effects failures, native valve endocarditis caused by Staphylococci)
were equivalent for overall adverse effects (n = 66; 26.7%; even though IDSA does not explicitly recommend high-
p = 0.189), elevated CPK that resulted in discontinuation of dose daptomycin for osteomyelitis.14
daptomycin (n = 47; 19%; p = 0.417), muscle cramps (n = 9; Although suboptimal dosing of daptomycin has been
3.6%; p = 0.605), elevated serum creatinine (n = 12; 4.9%; attributed to the development of resistance during therapy
p = 0.673, and paresthesia (n = 1; 0.4%; p = 0.148). ere were and treatment failure, a more complex picture unfolds
no differences in daptomycin discontinuation across the groups for different types of bacteria and infections. High-dose
(p = 0.165). In between-groups (< 6 mg/kg vs ≥ 6 mg/kg daptomycin 10 mg/kg was associated with lower 30-day
and < 6 weeks vs ≥ 6 weeks) analyses, only the frequency of mortality for the treatment of vancomycin-resistant En-
overall adverse effects was higher in the > 6 mg/kg group terococcus bacteremia compared with lower daily doses.15
(30.4% vs 18.4%; p = 0.049) independent of duration. Limited information exists examining daptomycin use in
Severe side effects, such as eosinophilic pneumonia and patients with osteomyelitis. In a small retrospective study,
Clostridium difficile-associated diarrhea, were not observed. Moenstar et al16 matched 17 daptomycin-receiving pa-
tients to 34 vancomycin-receiving patients. ey reported
DISCUSSION daptomycin dosing ranging from 3.7 to 7.2 mg/kg, and
is retrospective cohort study of 247 patients with os- significantly fewer patients treated with daptomycin had a
teomyelitis from 2 integrated healthcare delivery systems recurrence. Malizos et al’s9 retrospective study of device-
who were treated with outpatient daptomycin identified associated osteomyelitis reported that the longest time
that a dosing duration ≥ 6 weeks was associated indepen- to treatment failure was observed in a ≥ 6 to < 8 mg/kg
dently with clinical success (a composite of infection res- treatment group, although the clinical significance of this
olution and improvement). Additionally, we identified that finding was limited due to small sample sizes for < 6 mg/kg
dose was not independently associated with clinical success. (n = 10) and ≥ 8 mg/kg (n = 6). Our findings support this
Although we observed that patients in the ≥ 6 mg/kg dosing evidence and provide additional information on the patient
and ≥ 6 weeks duration group had the numerically highest characteristics associated with daptomycin clinical failure.
survivorship, our study was likely underpowered to identify e strengths of our study include broad sampling to
a statistically significant value. To our knowledge, this is the reduce practice bias, nonmanufacturer sponsorship minimizing
6 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. ·
The Permanente Journal https://doi.org/10.7812/TPP/20.297ORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
Table 5. Cox proportional hazards modeling of all-cause mortality
95% confidence interval
Factors Hazard ratio Lower Upper p value
< 6 mg/kg daptomycin dose and ≥ 6 wk duration 1.96 0.78 4.91 0.151
≥ 6 mg/kg daptomycin dose and < 6 wk duration 1.45 0.61 3.47 0.406
≥ 6 mg/kg daptomycin dose and ≥ 6 wk duration 0.66 0.26 1.69 0.391
< 6 mg/kg daptomycin dose and < 6 wk duration — —— —— ——
Female 0.60 0.29 1.23 0.162
Age ≥ 65 years 2.93 1.38 6.24 0.005
Diabetes comorbidity 0.92 0.48 1.79 0.813
Presence of orthopedic hardware 0.33 0.12 0.94 0.039
Inpatient length of stay 1.02 1.01 1.04 0.025
MRSA infection 1.52 0.80 2.91 0.205
Vancomycin use 1.08 0.55 2.11 0.829
Kidney disease stage 3-5 1.45 0.73 2.90 0.294
Charlson Comorbidity Index 1.22 1.08 1.37 0.001
MRSA = methicillin-resistant S. aureus.
conflict of interest, high cohesion of OPAT antimicrobial factors) and unknown confounding may have been present.
stewardship initiatives in an integrated healthcare delivery Patients who failed therapy may have been less likely to
system, and validation of diagnoses with imaging and remain on or to tolerate therapy for 6 weeks, thus leading to
cultures. We did identify modest rates of adverse effects. fewer patients who experienced clinical success.
Over 20% of patients experienced elevated CPK. Clinical Future research to assess initiation of standard dose
trial data identified 5.6% of patients experienced a CPK at 6 daptomycin for first-line treatment of MRSA osteomyelitis
mg/kg dosing.17 e authors extrapolated to higher doses and its effect on vancomycin-selective pressure may offer a
and hypothesized that up to 15.3% of patients would global antimicrobial stewardship strategy. is would
experience a CPK elevation at 10 mg/kg.17 e upper enhance current literature on dose-optimization dosing
dose limit in our patients was 10 mg/kg; nevertheless, we protocols and the role of oral antibiotic therapy.18-20
had a numerically higher rate of elevated CPK. Our Exploration of vehicles such as acrylic microparticles to
higher rate may be related to concomitant statin (owing to improve daptomycin activity/delivery can be affected by
substantial diabetes comorbidity in our sample) and dapto- biofilm maturity and bacterial strain could facilitate drug
mycin therapy dosing based on actual body weight in the enhancement.21 Evaluation of selective combination ther-
earlier years of our study. apy such as rifampicin to overcome resistance where higher
Our study did have limitations. Prior antibiotic exposure daptomycin dosing is unlikely to achieve therapeutic area
without a washout-window limits the extrapolation of under curve/MIC ratios would be informative.
daptomycin’s effect in an antibiotic-naive population. As-
sessment for reduced daptomycin susceptibility or poor CONCLUSIONS
clinical response through repeat cultures was not performed. Osteomyelitis is a costly infection that can lead to
Additionally, although the poor outcomes seen among multiple complications and can become poorly responsive
patients with < 6 weeks of treatment, dosing < 6 mg/kg, and to antibiotic treatment alone. is study identified that
body mass index > 30 could be attributed to inadequate daptomycin dosing at a prolonged duration of ≥ 6 weeks
dosing, the manufacturer FDA-approved dosing remains was associated independently with clinical success after
based on actual body weight up to a maximum of 6 mg/kg. adjustment for daptomycin dose and other potential con-
is likely represented real-time dosing and was sufficient. founders. Future prospective research is needed to identify
Although overall rates of daptomycin resistance in S. aureus the most appropriate daptomycin dosing and duration for
remain rare, daptomycin susceptibility and MIC were not osteomyelitis. v
performed during the study period. Furthermore, combined
Disclosure Statement
antibiotic regimens with vascular reconstruction and sur-
The author(s) have no conflicts of interest to disclose. No information in this
gical debridement were not evaluated. We adjusted for manuscript has been presented or published elsewhere. All information pertaining
potential confounders; however, other (eg, socioeconomic to the role of the sponsor is disclosed on the title page.
·
The Permanente Journal https://doi.org/10.7812/TPP/20.297 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. 7ORIGINAL RESEARCH ARTICLE
Patterns of Care and Treatment Outcomes for Outpatient Daptomycin-Containing Regimens in Osteomyelitis
6. Jeffres MN. The whole price of vancomycin: toxicities, troughs, and time. Drugs 2017 Jul;
Funding 77(11):1143-54. DOI: https://doi.org/10.1007/s40265-017-0764-7, PMID:28573434
This work was supported by a Kaiser Permanente Southern California Regional 7. LaPlante KL, Rybak MJ. Impact of high-inoculum Staphylococcus aureus on the activities
Research Committee grant from the Southern California Permanente Medical of nafcillin, vancomycin, linezolid, and daptomycin, alone and in combination with
Group Research and Evaluation Department and Direct Community Benefit gentamicin, in an in vitro pharmacodynamic model. Antimicrob Agents Chemother 2004
Investment funds. Additional funding and support were provided by the Pharmacy Dec;48(12):4665–72. DOI: https://doi.org/10.1128/AAC.48.12.4665-4672.2004, PMID:
15561842
Outcomes Research Group, Kaiser Permanente National Pharmacy. Financial
8. Grillon A, Argemi X, Gaudias J, et al. Bone penetration of daptomycin in diabetic patients
support for the conduct of the research and preparation of the article was provided with bacterial foot infections. Int J Infect Dis 2019 Aug;85:127-31. DOI: https://doi.org/10.
by Kaiser Permanente. 1016/j.ijid.2019.05.011, PMID:31096056
9. Malizos K, Sarma J, Seaton RA, et al. Daptomycin for the treatment of osteomyelitis and
orthopaedic device infections: real-world clinical experience from a European registry. Eur
Author Contributions J Clin Microbiol Infect Dis 2016 Jan;35(1):111-8. DOI: https://doi.org/10.1007/s10096-015-
Thomas Delate, PhD, designed the research, interpreted the analysis, revised 2515-6, PMID:26563898
the manuscript, and approved the version of the manuscript for submission. Julia K 10. Hermsen ED, Mendez-Vigo L, Berbari EF, Chung T, Yoon M, Lamp KC. A retrospective
Nguyen, PharmD, designed the research, interpreted the analysis, revised the study of outcomes of device-associated osteomyelitis treated with daptomycin. BMC
manuscript, extracted information from data sources, drafted the initial version of Infect Dis 2016 Jun;16:310. DOI: https://doi.org/10.1186/s12879-016-1590-3, PMID:
27343082
the manuscript, and approved the version of the manuscript for submission.
11. Senneville E, Caillon J, Calvet B, Jehl F. Towards a definition of daptomycin optimal
Jonathan T Truong, MD, designed the research, interpreted the analysis, revised dose: Lessons learned from experimental and clinical data. Int J Antimicrob Agents
the manuscript, drafted the initial version of the manuscript, approved the version 2016 Jan;47(1):12-9. DOI: https://doi.org/10.1016/j.ijantimicag.2015.11.005, PMID:
of the manuscript for submission. Fang Niu, MS, designed the research, interpreted 26712134
the analysis, revised the manuscript, performed the statistical analysis, and 12. Odom EB, Patel KB, Odom DC. Inpatient care versus subacute care for long term
approved the version of the manuscript for submission. Arman Haghigatgoo, intravenous antibiotics: cost from the patient perspective. Am J Hospital Med 2016
PharmD, designed the research, interpreted the analysis, revised the manuscript, Jul-Sep;8(1). Accessed 27 June 2020. https://medicine.missouri.edu/sites/default/files/
Inpatient%20Care%20versus%20Subacute%20Care%20for...%20American%20Journal
and approved the version of the manuscript for submission. All authors have made %20of%20Hospital%20Medicine.pdf.
substantial contributions to all the following: 1) the conception and design of the 13. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in
study, or acquisition of data, or analysis and interpretation of data, 2) drafting the ICD-9-CM and ICD-10 administrative data. Med Care 2005 Nov;43(11):1130-9. DOI:
article or revising it critically for important intellectual content, and 3) final approval https://doi.org/10.1097/01.mlr.0000182534.19832.83, PMID:16224307
of the version to be submitted. 14. Jorgensen J, Satlin M, Esparza G, et al. Ad hoc working group to reassess daptomycin
breakpoint for enterococci; 2018. Accessed 27 June 2020. https://clsi.org/media/2307/
2018_june_ast_bpwg_report_2__dapto_ceftaroline_cefiderocol.pdf.
Data Sharing Statement 15. Britt NS, Potter EM, Patel N, Steed ME. Comparative effectiveness and safety of
The data used for this study contain protected health information; thus, standard-, medium-, and high-dose daptomycin strategies for the treatment of
individual level data may not be made publicly available due to the Institutional vancomycin-resistant enterococcal bacteremia among Veterans Affairs patients. Clin
Review Board, business, and privacy concerns. Data are available for researchers Infect Dis 2017 Mar;64(5):605-13. DOI: https://doi.org/10.1093/cid/ciw815, PMID:
who meet the criteria for access to confidential data. Please contact the KPSC 28011602
Institutional Review Board (kpsc.irb@kp.org) for more information. 16. Moenster RP, Linneman TW, Finnegan PM, McDonald JR. Daptomycin compared to
vancomycin for the treatment of osteomyelitis: a single-center, retrospective cohort study.
Clin Therapeut 2012 Jul;34(7):1521-7. DOI: https://doi.org/10.1016/j.clinthera.2012.06.
References 013, PMID:22748973
1. Schmitt SK. Osteomyelitis. Infect Dis Clin North Am 2017 Jun;31(2):325-38. DOI: https:// 17. Bhavnani SM, Rubino CM, Ambrose PG, Drusano GL. Daptomycin exposure and the
doi.org/10.1016/j.idc.2017.01.010 probability of elevations in the creatine phosphokinase level: data from a randomized trial
2. Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 infectious diseases society of America of patients with bacteremia and endocarditis. Clin Infect Dis 2010 Jun;50(12):1568-74.
(IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral DOI: https://doi.org/10.1086/652767, PMID:20462352
osteomyelitis in adults. Clin Infect Dis 2015 Sep;61(6):e26-46. DOI: https://doi.org/10. 18. Ross JL, Rankin S, Marshik P, Mercier RC, Brett M, Walraven CJ. Antimicrobial
1093/cid/civ482, PMID:26229122 stewardship intervention and feedback to infectious disease specialists: a case study in
3. Dombrowski JC, Winston LG. Clinical failures of appropriately-treated methicillin-resistant high-dose daptomycin. Antibiotics (Basel) 2015 Jul;4(3):309-20. DOI: https://doi.org/10.
Staphylococcus aureus infections. J Infect 2008 Aug;57(2):110-5. DOI: https://doi.org/10. 3390/antibiotics4030309, PMID:27025626
1016/j.jinf.2008.04.003, PMID:18533269 19. Tran TT, Palmer HR, Weston J, et al. Evaluation of a daptomycin dose-optimization
4. Gawronski KM, Goff DA, Brown J, et al. A stewardship program’s retrospective evaluation protocol. Am J Health Syst Pharm 2012 Jun;69(11):979-84. DOI: https://doi.org/10.2146/
of vancomycin AUC24/MIC and time to microbiological clearance in patients with ajhp110279, PMID:22610031
methicillin-resistant Staphylococcus aureus bacteremia and osteomyelitis. Clin 20. Li HK, Rombach I, Zambellas R, et al. Oral versus intravenous antibiotics for bone and
Therapeut 2013 Jun;35(6):772-9. DOI: https://doi.org/10.1016/j.clinthera.2013.05.008, joint infection. N Engl J Med 2019 Jan;380(5):425-36. DOI: https://doi.org/10.1056/
PMID:23795575 NEJMoa1710926, PMID:30699315
5. Khadem C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious 21. WoischnigA-K, GonçalvesLM, Ferreira M, et al. Acrylic microparticles increase
Diseases Society of America for the treatment of methicillin-resistant Staphylococcus daptomycin intracellular and in vivo anti-biofilm activity against Staphylococcus
aureus infections in adults and children. Clin Infect Dis 2011 Feb;52(3):e18-55. DOI: aureus. Int J Pharm 2018 Oct;550:372-9. DOI: https://doi.org/10.1016/j.ijpharm.2018.
https://doi.org/10.1093/cid/ciq146, PMID:21208910 08.048
8 ·
The Permanente Journal For personal use only. No other uses without permission. Copyright © 2021 The Permanente Press. All rights reserved. ·
The Permanente Journal https://doi.org/10.7812/TPP/20.297You can also read

















































