Plan Oral Health - NY.gov
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Oral Health
Plan
for New York State
New York State Department of Health December 2014

A Message Dear Colleague: Last year, the New York State Department of Health released a five-year plan to improve the health and quality of life for everyone who lives in New York State – the Prevention Agenda 2013-2017. The plan is a blueprint for local community action to improve health and address health disparities, and is the result of a collaboration with 140 organizations, including hospitals, local health departments, health care providers, health plans, employers and schools that identified key priorities. Oral health, an important component of overall health, features prominently in this plan. I am pleased to present a plan specific to improving the oral health of all New Yorkers: Oral Health Plan for New York State. The 2014 Plan builds upon the progress made and lessons learned in implementing previous oral health efforts, and fits within the broader goal of improving overall health. The updated Oral Health Plan was developed by the New York State Department of Health in collaboration with stakeholders from across the state. Goals, objectives and strategies have been identified, covering a broad spectrum of issues. Emphasis has been placed on achieving optimal oral health for all, targeting at-risk populations and maximizing the use of evidence-based interventions. As we move forward with efforts to reduce preventable disease and improve the health care system, this plan emphasizes the importance of oral health. Oral disease has a huge economic and social cost, and can lead to complications and serious systemic conditions. Preventing dental caries and other oral diseases can reduce pain, suffering and health care expenses. Building on the efforts of the Prevention Agenda 2013-2017 and Healthy People 2020, this plan represents an opportunity to bring stakeholders together to improve the lives of all New Yorkers. We thank everyone who has contributed to this important endeavor. As the Oral Health Plan 2014 moves forward, we invite all stakeholders and interested partners to actively participate in promoting the oral health of all New Yorkers. Sincerely, Howard Zucker, MD, J.D. Acting Commissioner of Health


Table of Contents
I. Executive Summary 1
II. Overview of Oral Health 4
III. Priority Areas of Opportunity for Improving Oral Health:
Goals, Objectives and Strategies 6
IV. Prevalence, Risk Factors and Workforce 21
References 33
Appendix
2014 State Oral Health Plan Contributors 35
• State Oral Health Plan Advisory Committee
• Additional Work Groups
• Bureau of Dental Health
2005 State Oral Health Plan Contributors 37
• Bureau of Dental Health
• Steering Committee Members
• Work Group Members

I. Executive Summary
people 65 years of age and older, the percentage of people
who have lost all their teeth varied from 5.8 percent
among those with college education to 36 percent among
those with less than 12 years of education. Although most
oral diseases are preventable, not all individuals and
communities benefit fully from preventive measures. For
example, the percentage of mouth and throat cancers
detected in the early stages in 2011 varied from 22 percent
among black males to 42.1 percent among white females.
While community water fluoridation has been found to be
highly effective in controlling tooth decay, only about
72 percent of the population on public water supplies
receives fluoridated water. Dental sealants, a protective
The improvement in oral health observed in New York
coating applied on the chewing surfaces of teeth to prevent
State (NYS) during the latter half of the past century has
tooth decay, are present in approximately 40 percent
continued in this decade through the actions of individuals,
of third-grade children in New York State, still short of
professionals, policy makers, state and local governments,
the Maternal and Child Health Block Grant performance
educational institutions and health care organizations.
measure of 50 percent.
The New York State Department of Health’s (NYSDOH)
efforts to promote oral health through community-based In recent years, new scientific reports have linked poor
prevention interventions and programs are a testament to oral health to adverse general health outcomes. The role
its commitment to the achievement of optimum oral health of treating chronic low-grade periodontal (gum) infections
for all New Yorkers. However, much more can be done to in reducing the risk for heart and lung diseases, stroke,
improve oral health. Solutions will require collaboration low birth weight and premature births is being studied.
among multiple stakeholders. New York State can play a A strong association between diabetes and periodontal
leadership role and provide direction for future action. infection has been observed. The effect of early childhood
caries (tooth decay) on weight gain and failure to thrive
These efforts are needed because oral diseases such as
has been reported. The impact of tooth loss on food choices
tooth decay and gum infections and orthodontic problems
is well documented. Behaviors that affect general health,
still affect a large proportion of the population. Among
such as tobacco use, excessive alcohol use and poor dietary
children, tooth decay is the most common chronic disease; it
choices, are also associated with poor oral health outcomes.
is five times more common than asthma, and 20 times more
The emergence of this connection between oral health
common than diabetes. In NYS, approximately 44 percent
and general health and common risk factors supports oral
of children experience tooth decay by the third grade. Tooth
health care as an essential component of health programs
decay and advanced gum diseases ultimately lead to loss
and policies.
of some or all teeth. About 41 percent of 35- to 44-year-
old adults have lost one or more teeth due to tooth decay The federal Patient Protection and Affordable Care Act
or gum diseases. About 17 percent of people 65 years of (ACA) extends health coverage, including dental benefits, to
age and older have lost all of their teeth. Life-threatening millions of children who now lack such coverage. The ACA
cancers of the mouth and throat are detected in five New specifically included pediatric oral health care among the 10
Yorkers every day. “essential health benefits” that all qualified health plans are
required to cover for children beginning in 2014.
Disparities in oral health observed in national surveys
are also apparent in New York State. For example, among
1
NYS has impressive resources and assets. With five the 2005 State Oral Health Plan for oral health promotion,
academic institutions training dentists, 10 dental hygiene disease prevention, and control. A steering committee of
schools and more than 50 training programs in advanced representatives of partner organizations guided the plan
education in dentistry, New York has much to offer in development. The plan includes specific objectives for
education, training and research. New York State has one future reductions in oral disease and related risk factors and
of the best population-to-dentist ratios in the country. A objectives for the promotion of oral health. It recognizes
provider network of health centers, hospitals and public earlier efforts to address children’s oral health and workforce
health programs supports the dental health needs of shortages in rural areas. Participants at the 2011 Oral Health
vulnerable populations. New York’s infrastructure is further Policy Workshop developed an inventory of strategies which
strengthened by Medicaid and public insurance programs informed the steering committee in its work to update the
that ensure access to care for needy populations. 2005 Oral Health Plan for New York State.
NYS must capitalize on the strengths of its infrastructure This plan’s goals and objectives will serve as a blueprint
while enabling change and engaging new allies to better for all involved in improving and achieving optimal oral
address the following challenges: health. All stakeholders can use this plan as a tool to enlist
partners, attract funding sources and promote action.
• Improving the public perception that oral health is
The scope of this plan is broad, covering a spectrum of
important to overall health;
issues and concerns regarding policy, prevention, access,
• Improving the utilization of effective preventive workforce, surveillance and research. The following
measures at the individual and community levels; strategies have been identified as priorities:
• Improving the diversity and flexibility of the dental 1. Bring together stakeholders periodically and develop
workforce, with particular attention to the uneven a statewide agenda for action related to:
distribution of dental professionals;
a. Laws and regulations that affect the provision
• Addressing the high cost of dental education and of dental services, and practice of dentistry and
the debt burden for new graduates that limits their dental hygiene
ability to practice in underserved areas;
• Improving the measurement and tracking of oral
diseases, risk factors, the dental workforce and
utilization of dental services.
For New Yorkers to enjoy overall health and well-being,
there must be new vehicles to promote oral health and
prevent disease. Public-private partnerships at the state
and local levels that involve a variety of stakeholders have
the potential to become these vehicles. It is, therefore,
imperative to create an environment that develops, nurtures
and sustains these partnerships.
With this in mind, the NYSDOH worked collaboratively
with many partner organizations and individuals to update
2
3. Strengthen the oral health surveillance system
so that oral diseases and their risk factors can be
periodically measured by key socio-demographic
and geographic variables and tracked over time to
monitor progress.
4. Encourage educational and training programs to
update competencies and standards to enhance the
treatment of children and people with special health
care needs. Explore opportunities to educate the
dental workforce in the care of patients with special
health care needs.
b. Financing of dental education, including
scholarship and loan repayment programs
c. Effective approaches to address disparities in
oral health, including changes to curricula in
schools of dentistry and dental hygiene
d. Improving the flexibility of the dental workforce
to address need, considering items identified by
the Medicaid Redesign Team.
2. Explore opportunities to form regional partnerships
by encouraging local health departments, preventive
dentistry programs, rural health networks, providers,
educational institutions, agencies focused on helping
families, and other community coalitions to work
together to identify prevention opportunities and
address access to dental care in their communities
as outlined in the New York State Prevention Agenda
Toward the Healthiest State 2013-2017.
3
II. Overview of Oral Health
Tooth decay is the most common chronic childhood disease,
with almost 80 percent of all children experiencing tooth
decay by the time of high school graduation. In the United
States, 18 percent of all children’s health expenditures
are devoted to dental care. Although most dental diseases
are preventable, many children unnecessarily suffer the
consequences of dental diseases because of inadequate
home care, and inability to access preventive and treatment
services in a timely manner.1-5
According to a recent report on children’s dental health
issued by the Pew Charitable Trust, three systemic factors
contribute significantly to poor dental health and the lack
of access to care among disadvantaged children: (1) too
few children having access to proven prevention measures,
including dental sealants and fluoridation; (2) too few
dentists willing to treat Medicaid-enrolled children; and (3)
a limited number of dentists in many communities available
to provide care.6
Oral diseases in adults negatively impact their ability to eat
healthy food, overall health and, ultimately, employability.1
There are clear socioeconomic disparities in the distribution
Several reports link low-grade chronic infection in the
of oral health problems. Children from low-income families
mouth (periodontal diseases) to systemic illnesses such as
have a higher prevalence of dental caries, higher frequency
cardiovascular diseases, respiratory ailments and adverse
of untreated disease and lower utilization of preventive
pregnancy outcomes. People with diabetes are also at
services.1, 3-5, 11-14 These differences are observed in children
increased risk for periodontal infections.1
as young as two to four years of age as well as in the elderly.
Many risk factors for oral diseases are known.1 Early The reasons for these disparities include lack of awareness
childhood caries are associated with frequent feeding in of the importance of oral health, unfamiliarity with the
young children and the transmission of caries-causing dental health care delivery system, lack of providers willing
bacteria from mothers to children through common to participate in publicly-financed programs and lack of
practices such as tasting infant’s food before feeding.7-9 resources to pay for care.1, 15-17
Lack of fluoride, frequent snacking and inadequate home
Although oral diseases can be controlled, lack of continuous
care, such as lack of tooth brushing, increase the risk of
insurance coverage is a problem for many children and
dental caries in older children. Tobacco use is associated
adults.1, 3, 5 Nationally, as many as one in four children lack
with periodontal disease and oral cancer in adults.10
dental insurance coverage. For every person without health
insurance coverage, there are as many as three people
without dental health insurance coverage.18 Further, access
to dental care providers is extremely limited for many
children in rural and inner city areas. 1, 4-5, 11, 13, 19-20
4According to the 2010 Medical Expenditure Panel Survey,
35.8 percent of the civilian non-institutionalized population Key Facts
in NYS had dental care expenditures. The mean expenditure
for dental care was $528 in 2010, with about 48.1 percent of • At least 75 million Americans
dental expenses paid by private insurance and 33.1 percent (25 percent) have either limited
paid out of pocket.5 or no access to oral health care.
In 2011, there was an estimated total of $1.33 trillion • Almost 60 percent of children
paid for health care received by the U.S. civilian ages 5-17 have cavities.
non-institutionalized population. Dental expenses
comprised a larger proportion of expenses for children
• 26 percent of adults
under age 18 (18.1 percent) than adults aged 18-64 (ages 19-64) have untreated
(6.1 percent) or age 65 and older (3.6 percent).21 decay, and 5 percent of adults
have no teeth.
• Those who are low-income or
minorities are at higher risk
for experiencing dental caries
(cavities) and dental decay.
• Children and adults who receive
regular dental care are more
likely to have their decayed teeth
diagnosed and treated.
• Water fluoridation is one of the
most cost-effective measures of
prevention; on average every $1
invested in water fluoridation in
large communities saves about
$38 per year in dental costs.
Source: Kaiser EDU, accessed 12/2012 at
http://www.kaiseredu.org/Issue-Modules/Den-
tal-Care/Background-Brief.aspx
5III. Priority Areas of Opportunity for Improving Oral Health:
Goals, Objectives and Strategies
Issues
Goal 1: Integrate oral health
• A significant portion of the NYS population is not
into systems, policies and served adequately by the oral health care system.
programs which improve Many vulnerable and underserved populations
overall health. utilize health care frequently, but do not seek routine
oral health care.
• Oral health is not well integrated into all health
Background programs. Opportunities for prevention are lost if risk
factors such as tobacco and alcohol use, poor diet
More than a decade ago, the U.S. Surgeon General
identified the need to enhance the public’s understanding and other health habits, which are common to many
of oral health and the relationship of the mouth to the rest illnesses including oral diseases are not addressed.
of the body. While the surgeon general’s report raised the • Not all educational and training programs integrate
awareness of the importance of oral health, it is still treated oral health and general health programs optimally
as separate and distinct from broader health care. A sizeable and provide specialized dental services.
proportion of the population suffers from a disproportionate
burden of preventable oral diseases such as dental caries, • Barriers to care and treatment arise from fears and
periodontal disease and oral cancer. common misconceptions about oral health.
The U.S. Department of Health & Human Services Strategic • Comprehensive, culturally-competent education
Plan, Fiscal Years 2010-2015, proposes to promote policies to campaigns and materials are not available to fulfill
integrate oral health into primary care, including prevention appropriate literacy level requirements for all
and improved literacy. New York can take advantage of populations in multiple languages.
national policies to integrate oral health into general health
Objectives
and address risk factors such as poor oral hygiene, tobacco
and alcohol use and dietary practices. Interdisciplinary bjective 1.a: By 2017, ensure that oral health is
O
efforts to improve health often identify improving oral included in all statewide comprehensive health
health as a key barrier to achieving good overall health, and planning activities as appropriate.
best-practice models for collaboration are emerging in areas
such as prenatal care. NYS has begun to include oral health Objective 1.b: By 2017, establish an ongoing process
in statewide strategic health planning. In the Prevention of engaging statewide partners and stakeholders
Agenda, reducing tooth decay was identified as a priority to assess opportunities for policy change, including
area for improving the overall health of mothers, infants changes in laws and regulations to promote the
and children. integration of oral health improvement into overall
health improvement efforts.
Objective 1.c: By 2017, assess the ability of electronic
medical and dental record systems to share key health
information between providers, and implement policies
to include oral health systems in New York’s regional
health information organizations.
6• Ensure oral health is included in all care
coordination activities.
• Provide assistance to school-based health
centers with the integration of oral health into
comprehensive health services.
• Encourage professional organizations, educational
institutions, key state agencies and other stakeholders
to examine and make recommendations on:
• Laws and regulations that affect the provision
of dental services, and practice of dentistry and
dental hygiene.
• Financing of dental education, scholarship and
loan repayment programs.
Objective 1.d: By 2017, evaluate the implementation of
• Effective approaches to address disparities in
dental coverage in New York State’s health insurance
oral health, including changes to curricula in
exchange.
schools of dentistry and dental hygiene.
Objective 1.e: By 2017, increase referrals between oral
• Strengthening the dental health workforce,
health care providers and other health specialists as
including integrating dental hygiene education
warranted by examinations and health history.
and training programs into undergraduate
Objective 1.f: By 2017, expand the oral health and graduate programs to advance the careers
component of existing surveillance systems to provide of dental hygienists, and changes in dental
more comprehensive and timely data (See Goal 7). hygiene practice as recommended by the
Medicaid Redesign Team.
Objective 1.g: By 2017, engage multidisciplinary
stakeholders, such as health care providers, social • Identify and disseminate information regarding
workers, teachers, health educators and home health electronic health records models that have
aides, in community outreach and oral health successfully integrated oral health.
education efforts.
• Monitor New York’s health insurance exchange to
Strategies ensure proper access to the pediatric dental benefit
of the ACA, assuring comprehensive affordable
• Inform and educate policymakers and officials at
health insurance coverage for all NYS children.
local, state and federal levels about oral health
needs, evidence-based interventions and successful • Analyze the cost and benefits of essential dental
programs. health benefit package in New York’s health
exchange that includes oral health preventive and
• Engage partners and stakeholders to implement the
treatment services for adults.
Prevention Agenda.
• Facilitate initial and continuous enrollment of low-
• Leverage opportunities to integrate oral health into
income children in Medicaid and Child Health Plus,
ongoing public health programs.
including presumptive eligibility.
7• Promote the integration of oral health care into the
health homes initiative and other care coordination Goal 2: Prevent oral diseases
efforts. http://www.hrsa.gov/publichealth/clinical/
oralhealth/primarycare/oralhealthprimarycare.pdf
and address risk factors through
evidence-based interventions.
• Work with professional groups to increase referrals
among oral health care providers and other health
professionals. Work with organizations of health
care professionals to target physicians’ offices for
Background
integrating oral health screening as part of routine Many risk factors for oral diseases are well known: poor oral
physical examinations, and providing anticipatory hygiene, lack of self-care, inappropriate infant and toddler
guidance to families on proper oral health care. feeding practices (such as frequent snacking and putting
children to bed with bottles), lack of regular dental visits,
• Assess the impact of efforts to improve
and tobacco and alcohol use. Furthermore, interventions
interdisciplinary collaboration and include oral health
are available. Programs such as water fluoridation, fluoride
as a part of overall health in the knowledge, skills,
supplementation, school-based or linked dental sealant
attitudes and behaviors of health care professionals.
programs, screening and referral, counseling with fluoride
varnish application, and tobacco control have the potential
to reduce the burden of oral diseases. However, both
community and individual interventions are underutilized.
While interventions such as risk assessment, fluoride
varnish application, oral health counseling by non-dental
providers, and tobacco cessation counseling are being
promoted, their adoption is uneven.
Issues
• Dental diseases are preventable for the most part.
Evidence-based interventions, available both at
community and individual levels, are not being
utilized to the fullest extent.
• While the NYS Medicaid program covers risk
assessment, fluoride varnish and anticipatory
guidance for young children by physicians and nurse
practitioners, many clients and providers are not
aware of the benefit.
• Water fluoridation reaches only 48% of residents
outside of New York City. The public and
policymakers lack access to reliable information
about the the benefits of water fluoridation.
• Barriers remain to promoting other fluoride and
sealant programs.
8Objectives • Seek guidance from the Centers for Medicare and
Medicaid Services (CMS) on the allowability of
Objective 2.a: By 2017, increase the percentage of NYS Medicaid financing for community water fluoridation
population receiving fluoridated water by 10 percent. as a strategy to reduce oral disease burden while
(NYS Prevention Agenda Objective 5-4. Baseline 71.4 lowering aggregate Medicaid dental expenditures.
percent in 2012)
• Work with foundations to establish a funding stream
Objective 2.b: By 2017, increase the proportion of NYS for initiating and maintaining fluoridation.
children who have protective dental sealants by at
least 10 percent (NYS Prevention Agenda Objective • Work with stakeholders, including insurance
5-2), and increase the proportion of third-grade providers, professional groups and policymakers,
children who have dental sealants to 50 percent by to implement guidelines for preventive oral health
2020. (Baseline: 2012 New York City 26.3 percent, 2011 services and ensure that fluoride varnish, risk
Rest of State 42 percent.) assessment and anticipatory guidance are available
and reimbursable in all appropriate care settings.
Objective 2.c: By 2017, reduce the proportion of third
grade children with dental caries experience and • Strengthen public awareness campaigns by
untreated caries to no more than 41.5 percent and 21.6 coordinating activities and funding, partnering with
percent respectively (NYS Prevention Agenda Objective stakeholders, and securing foundation support.
5-1), and further reduce by 2020 the proportion of
• Seek federal or foundation funding to establish an
third grade children with dental caries experience and
evidence-based public education campaign to promote
untreated caries to no more than 40 percent and 20
oral health, including a focus on early childhood caries,
percent respectively.
prevention, the oral health of pregnant women, and
Objective 2.d: By 2017, increase the proportion the oral health of at-risk populations.
of adults who receive information from a dentist
• Collaborate with stakeholders to improve the dental
or dental hygienist on reducing tobacco use or
health screening initiative in schools, Head Start
smoking cessation.
Centers and other such settings.
Strategies • Promote dental sealants by Dental
• Actively promote fluoridation in large communities providing sealant equipment and Sealants
(more than 10,000 people) and in counties with low funding to selected providers
fluoridation penetration rates. Educate the public in targeted areas where dental
about the benefits of fluoride by incorporating sealant utilization is low.
effective messages in health campaigns.
• Encourage Article 28 facilities
• Ensure the quality of the fluoridation program by to establish school-based dental
monitoring fluoride levels in water, conducting programs in schools and Head
periodic inspections and providing feedback to water Start Centers to promote preventive
plant operators. Continue the education program for dental services in high-need areas.
water plant personnel.
• Provide technical assistance to every dental office
and clinic in New York State to implement the U.S.
Public Health Services’ Guidelines for Treating
Tobacco Use and Dependence.
9• The capacity of safety net clinics is not sufficient to
Goal 3: Eliminate oral health meet the needs of the population.
disparities and improve access • Dental insurance programs are not available for the
to high quality, comprehensive, elderly, and Medicare does not cover routine
continuous oral health services dental care.
for all New Yorkers. • Access to dental care for vulnerable populations
is limited, while their numbers continue to grow.
Vulnerable populations include:
Background • People with developmental disabling
conditions, or physically challenged children
Dental diseases and unmet need for dental care are more
and adults;
prevalent where people cannot pay for services or lack
adequate insurance, have language and transportation • Those with low incomes, including children, the
barriers to care, and cannot find providers and services homeless and migrant workers;
for complex oral and medical health conditions. While
Medicaid, Child Health Plus and Family Health Plus • Pregnant and parenting women who also need
insurance programs and public health clinics have inter-conceptional care;
expanded efforts to enroll eligible people, the unavailability • Children with special health care needs;
of providers trained to handle complex oral health
problems remains a problem in certain geographic areas. • People living with HIV and AIDS;
Compounding the problem is the inability of many patients • Adults with severe mental illness, substance
to maintain dental appointments on a regular and frequent abuse or tobacco dependence;
basis. In addition, dental offices and clinics often do not
have extended hours of service to accommodate patients • The elderly, including those who are
during evening hours and weekends, presenting a barrier homebound and institutionalized; and
for the working poor to see dentists. • Children in need of medically necessary
Issues orthodontic care.
• Dental caries in low-income and minority children Objectives
has a significant impact due to the difficulty in Objective 3.a: By 2017, increase the number of Article 28
obtaining access, including a lack of providers to treat facilities providing dental services across the state, and
young children and the cost of care. increase the number of high-risk elementary schools
• Many women of childbearing age do not seek with school-based or school-linked sealant programs.
dental care in a timely manner, so opportunities for Objective 3.b: By 2020, increase the number of children
preventing dental problems in women and children and adolescents ages two to 20 years in Medicaid and
are missed. Child Health Plus who have had at least one preventive
• Oral health programs in health centers and hospitals dental visit within the past year to 65 percent from the
do not have the resources for outreach, education 2010 baseline of 37.3 percent for Medicaid and
and services which enable access to care. 63 percent for Child Health Plus.
10Objective 3.c: By 2020, increase the number of children • Evaluate network adequacy and utilization of
who visit a dentist annually, meeting the Healthy People dental services in public insurance programs
2020 (HP 2020) goal of 49 percent for all population such as Medicaid Managed Care and health
groups of children. [NYS Prevention Agenda objective insurance programs.
5-3: By 2017, increase the proportion of NYS children
• Explore loan repayment incentives for dentists and
who receive regular dental care by at least 10 percent.
hygienists linked to services reimbursed by public
(2010 Baseline: 42 percent of two to 20-year-olds with
insurance programs (also related to Goal 6).
Medicaid, 72.4 percent of third-graders in New York City,
83.4 percent of third-graders in the rest of the state.)] • Increase the number of safety net dental clinics in
community health centers and migrant health centers,
Objective 3.d: By 2020, increase the number of
and improve their capacity to provide care, by:
Medicaid-enrolled adults aged 22-64 who had at least
one preventive dental visit within the past year to 32 • Assessing potential funding sources for dental
percent from the 2010 level of 29.2 percent. health programs.
Objective 3.e: By 2020, increase the percentage of adult • Removing administrative and legal barriers for
New Yorkers who have seen a dentist in the past year innovative models.
to 80 percent from the 2010 level of 72.5 percent.
• Encouraging health centers and hospitals that do
Objective 3.f: By 2020, increase the number of women not provide dental care to offer dental services.
in the Medicaid program who visited dentists during
• Provide technical assistance to overcome
their most recent pregnancies to 54.6 percent from the
barriers to providing these services (e.g.
2008 level of 49.6 percent.
resources, staffing, financing), and develop an
Objective 3.g: By 2020, reduce the number of dental- action plan to address barriers.
related visits to ambulatory surgery facilities and
• Work with Area Health Education Centers
emergency rooms by children younger than six years
and professional organizations to strengthen
from the 2008 level of 4,800 to 2,400 per year by
recruitment opportunities.
addressing tooth decay earlier and more effectively.
• Disseminate information about services which
Objective 3.h: By 2020, increase the percentage of
have demonstrated effectiveness at providing
adults receiving an annual examination for oral and
greater access to oral health care.
pharyngeal cancers to 50 percent from the 2003 level of
approximately 30 percent. • Work with the New York State Dental
Association to strengthen the Donated Dental
Strategies
Services program.
• Promote structured, evidence-based learning
• Maintain and expand the availability of school-
collaborations to identify and address areas for
based preventive dental programs in targeted
improvement in clinical practice, including the
high-need, underserved communities.
management of early childhood caries, dental
sealants, and improving the oral health of • Conduct annual community health assessments
pregnant women. to determine availability of dental practices,
including capacity for new clients, what kinds
of insurances are accepted and distribute
information in up-to-date local resource guides.
11and competent in providing oral health services for
Goal 4: Strengthen systems patients with special needs.
which improve the oral health • Inadequate financing and a lack of access to
of people with special health adequate facilities contribute to poor access to dental
needs. care for people with special needs.
• Data are lacking on utilization of dental services
by patients with special needs and the barriers to
Background accessing dental care.
Children and adults with special health care needs have oral Objectives
health needs which require particular consideration and
Objective 4.a: By 2017, identify successful
approaches. Special health care needs refer to any physical,
reimbursement strategies for providers and hospitals
developmental, mental, sensory, behavioral, cognitive or
that address the additional time and resources needed
emotional impairment or limiting condition that requires
to treat people with special health needs.
medical management, health care intervention or use of
specialized services or programs . The condition may be Objective 4.b: By 2017, ensure that systems developed
developmental and cause limitations in performing daily to increase interprofessional collaboration and inform
self-maintenance activities or substantial limitations in consumers about dental care address the challenges
a major life activity. In the United States, the limited data faced by people with special health needs.
available indicate that, compared to the general public,
Objective 4.c: By 2017, implement changes in the
people with special needs have poorer oral hygiene, more
surveillance system to enable data collection on oral
missing teeth and untreated caries, and increased levels of
health and access to dental care for people with special
gingivitis and periodontal disease.
health needs.
Challenges to achieving optimal oral health include the
Objective 4.d: By 2017, identify Centers of Excellence
need to improve home care as well as access to preventive
for providing oral health care to people with special
and treatment services. Barriers to optimal oral health
health needs.
for people with special health needs must be identified
and documented, including those which also affect the
provision of other health care services. Innovative solutions
to finance prevention and treatment that recognize the
challenges of providing care to patients with special
needs could have a substantial positive impact, along with
improved provider training.
Issues
• The number of dentists available to treat children and
adults with special health care needs is limited.
• The training time available in dental and dental
hygiene education programs is not sufficient to
ensure that providers and caregivers are comfortable
12• Convene a summit of stakeholders to discuss the
financing options available in other states regarding
the oral health care for people with special health
needs and develop recommendations.
• Partner with hospitals to identify and implement best
practices that reduce operating room wait times for
people with special health needs.
• Identify reimbursement incentives and strategies for
providers and hospitals, which reflect the additional
time and resources needed to treat low-income
children and those with special health needs.
Objective 4.e: By 2017, assess the number of dental • Work with community stakeholders to conduct
providers serving people with special health care needs outreach to hospitals to increase awareness of the
and determine how many are needed to serve people importance of oral health for people with special
with special health needs. health needs.
Objective 4.f: By 2017, develop and implement strategies • Identify strategies which have increased the number
to ensure that waiting times for routine appointments of dental providers serving people with special health
are no longer than one month, and dental emergencies needs, and replicate their success in New York State.
are addressed within 24 hours for patients with special
• Identify workforce models that improve access to
health needs.
care for people with special health needs.
Objective 4.g: By 2020, ensure that all health care
• Encourage educational and training programs to
workers employed to assist people with special health
update competencies and standards to enhance the
care needs are trained in their daily oral health care.
treatment of people with special health care needs.
Objective 4.h: By 2017, develop research activities that
• Convene a workgroup of researchers and public
address the oral health issues of people with special
health practitioners to develop and set priorities for a
health care needs.
research agenda which addresses oral health care for
Also see NYS Prevention Agenda Objective 5-5: By people with special health care needs.
December 31, 2017, strengthen systems to improve the oral
• Identify existing data collection systems for people
health of people with special health needs.
with special health needs and explore opportunities
www.health.ny.gov/prevention/prevention_
to include oral health indicators.
agenda/2013-2017/
• Work with community stakeholders and caregivers
Strategies
to collect, share and use data regarding oral health
• Develop a campaign to educate stakeholders about status and unmet treatment needs for people with
the unique oral health challenges facing people with special health needs.
special health needs.
• Expand and support Centers of Excellence for special
needs populations.
13Objectives
Goal 5: Increase knowledge-
Objective 5.a.: By 2017, support expansion of oral health
sharing statewide to enhance coalitions, partnerships and networks in every region
the adoption of best practices, of the state to provide an opportunity for organizations,
replicate proven efforts, and consumers, and providers to collaborate, gain access to
the media, and promote communication.
improve community oral
health literacy. Objective 5.b.: By 2017, develop and promote a
system which educates oral health providers about
evidence-based practices for improving oral health
at the individual and community levels, and informs
Background providers about best practices for improving access and
Dental disease prevention and health promotion programs utilization of oral health services.
are underutilized, including water fluoridation, school-
Objective 5.c: By 2017, assess and address gaps in oral
based interventions, tobacco control, case management
health educational materials. Update and distribute
and efforts to integrate oral health into programs such as
culturally and linguistically appropriate materials that
the Special Supplemental Nutrition Program for Women,
enhance oral health literacy to the public and providers.
Infants and Children (WIC) program. Achieving and
maintaining oral health requires actions by individuals, Objective 5.d: By 2017, build upon existing efforts and
professionals, communities, health care and social service explore new areas for involvement with campaigns that
agencies and educational institutions. The American communicate the importance of oral health, signs and
Association of State and Territorial Dental Directors symptoms of oral disease and ways of reducing risk
has compiled a directory of many best and promising such as Children’s Dental Health Month, National Dental
approaches for community oral health programs. Hygiene Month, Oral Cancer Awareness Week, Give
Linking private and public sectors, and involving many Kids a Smile, Special Olympics Special Smiles, tobacco
stakeholders, provides opportunities to capitalize on unique cessation campaigns and diabetes education campaigns.
strengths and resources. NYSDOH has partnered with the
Oral Health Technical Assistance Center and The Pew Center
on the States to develop a consumer-oriented website with
information regarding fluoridation.
http://newyork.ilikemyteeth.org/
Issues
• Lack of oral health infrastructure at the local level has
hindered the ability to communicate best practices
and programs.
• Public-private partnerships that address oral health
issues at the state and local level are limited in
number.
• There is no effective mechanism to educate
stakeholders about collaboration, networking and
sharing of experiences.
14Strategies
• Disseminate guidelines, recommendations and best
practices regarding childhood caries, maternal oral
health, and tobacco and alcohol use to the dental
health workforce, physicians, nurse practitioners,
counselors and other related health care workers.
• Widely disseminate best practices for infection
control and provide technical assistance to dental
professionals.
• Promote the fluoridation-related “I like my teeth”
website. [www.ilikemyteeth.org]
• Enhance communication between stakeholders in
different regions in the state.
• Develop an inventory of effective programs and best
practices that can be widely disseminated.
• Provide technical assistance to local groups and
help procure funding for evidence-based oral health
Objective 5.e: By 2017, develop and promote a system programs.
which provides consumers with information about
• Develop and implement structured, evidence-based
community water fluoridation and other best practices
quality improvement collaborations to identify and
for improving oral health.
address areas for improvement in clinical practice
Objective 5.f: By 2017, develop and promote a system such as management of early childhood caries and
which provides information about programs and reduced no-show rates.
resources for consumers seeking oral health care.
• Communicate changes to statewide programs in
an organized, systematic and culturally competent
manner, with the understanding that New Yorkers
have diverse backgrounds.
• Integrate oral health into health literacy programs.
Develop and disseminate educational materials
focusing attention on topics such as caries in young
children, maternal oral health, oral cancer, fluoride,
dental sealants and the importance of good
dietary habits.
15Issues
Goal 6: Increase capacity, diver- • The geographic distribution of oral health care
sity, and flexibility of the work- providers, especially in rural areas and inner city
force to meet the needs of all neighborhoods, is inadequate to meet the needs of
all New Yorkers. This is further compounded by the
New Yorkers. aging of the workforce.
• Incentives for the dental workforce are insufficient to
ensure the care for many low-income residents.
Background
• Alternative solutions are needed to improve the oral
Access to dental services and an understanding of the
health literacy of those not reached by traditional
importance of oral health, especially prevention efforts, are
interventions, including exploring new models and
key elements to achieving optimal oral health. To address
increased involvement from primary care providers.
these needs, New Yorkers need an adequate oral health
workforce, including any provider or caregiver with the • Schools of dentistry and dental hygiene face difficulty
ability to provide oral health services or education. While in recruiting and retaining faculty.
the state has one of the best population-to-dentist ratios in
• Educational and training opportunities are needed in
the country, the distribution of practitioners is uneven, with
underserved areas to improve the oral health
shortages of dentists and dental hygienists in many rural
of communities.
and inner-city areas. This is compounded by the inadequate
number of dentists treating underserved population groups • Students and practicing dental professionals are
and under-representation of minorities in the workforce. not adequately exposed to public health issues and
training. Practitioners are isolated, for the most part.
Since 2007, dentists intending to practice in NYS have
been required to undergo one year of internship training
in accredited advanced education programs. This prepares
future dentists to treat more complex dental and medical
problems and creates opportunities for rural and inner-city
hospitals and health centers to establish training programs,
attract dentists, and expose them to the unique needs of
underserved populations. Students trained in the community
are more likely to return to practice in these settings.
Collaboration between medical and dental providers has
the potential to address some workforce shortages where
dental personnel are not available. Increasingly, primary
care providers have an opportunity to provide preventive
oral health services, becoming involved members of the oral
health workforce. Making use of the abilities of the entire
oral health workforce, as well as the consideration of new
and expanded workforce models, are potential components
of a multifactorial approach to improving access to dental
care for all.
16Objectives
Objective 6.a: By 2017, include core competencies for
oral health in training programs that improve the skills
of primary care providers, nurses, social workers and
case managers.
Objective 6.b: By 2015, ensure that health care
workers employed to assist the elderly and people
with disabilities are trained to provide their daily oral
health care.
Objective 6.c: By 2017, encourage all hospitals and
health centers in federally designated Dental Health
Professional Shortage Areas to develop training
programs to meet the continuing educational needs of
dental workforce members.
Strategies
Objective 6.d: By 2017, create opportunities for all dental,
• Using proven education and training models
dental hygiene students and residents to work in dental
(e.g., Learning Collaborative, Smiles for Life, AAP
professional shortage areas for a significant period
Children’s Oral Health Education and Training) to
through externships, internships and partnerships.
improve the skills of primary care providers, nurses,
Objective 6.e: By 2017, designate eligible areas as social workers and case managers in applying
Dental Health Professional Shortage Areas so they can evidence-based practices.
access federal resources. www2.aap.org/oralhealth/EducationAndTraining.
html
Objective 6.f.: By 2017, increase the under-represented
minority enrollment in schools of dentistry and dental • Improve the productivity of dental providers through
hygiene to more closely reflect the population of the development of policies and practices for utilizing
New York. all team members to the full extent of their education
and training.
Objective 6.g: By 2017, evaluate the ability of new
models of oral health care to improve access to oral • Provide information about resources and incentive
health services and improve oral health literacy. programs like State Primary Care Service Corps to
dental residents and dental hygienists willing to
Objective 6.h: By 2017, identify the opportunities for
practice in underserved areas.
dentists, dental hygienists and other providers who
address oral health to improve their knowledge, skills • Explore models from other states that allow dental
and competency in public health practice, health hygienists to bill for services provided in schools,
literacy and effective communication strategies. nursing homes and other public health settings (also
related to Goal 1). Evaluate the laws and statues
related to the practice of dentistry in other states and
the impact of recent changes in New York State in
order to address workforce issues.
17• Collaborate with dental and dental hygiene schools Goal 7: Maintain and enhance
to employ best practices in the recruitment and
retention of under-represented minority students.
the existing surveillance system
Examine how other professions recruit and retain to measure key indicators of oral
minority students. health adequately and identify
• Develop and enhance programs that encourage key performance measures for
children in elementary and middle schools to tracking progress.
consider careers in oral health.
• Explore ways to attract and retain qualified dental
and dental hygiene faculty and to engage community Background
providers in the education of new practitioners.
Several data sources are used to monitor oral diseases,
• Survey all hospitals and health centers providing risk factors, access to programs, utilization of services and
dental services to determine their interest in workforce. The New York State Oral Health Surveillance
participating in educational programs. System includes data from oral health surveys of third-
grade children. The Behavioral Risk Factor Surveillance
• Explore best practices used in dental and dental
System, the Cancer Registry, the Congenital Malformations
hygiene schools that provide internship and
Registry, the Water Fluoridation Reporting System,
externship experience outside traditional training
the Pregnancy Risk Assessment Monitoring System,
environments.
Medicaid, Managed Care Performance Reports and the
• Identify factors that affect the participation of the State Education Department’s licensing data are used for
dental workforce in public health programs, locating planning and evaluation as well as to contribute to the
their practices in dental health professional shortage national database for monitoring trends in dental health.
areas and serving underserved populations. Enhancement and expansion of the current system will
provide data needed to identify problems, set priorities,
• Provide incentives to encourage dentists, dental
establish quality improvement measures and assess
hygienists and dental assistants to work in public
progress toward goals and objectives. Preventing and
health settings. Identify interventions to attract well-
controlling oral diseases, and ensuring high quality and
trained and motivated providers.
effective programs, requires rigorous studies to support
• Provide opportunities for training in cultural evidence-based practice. This can be accomplished through
competency for all oral health care providers. collaboration and coordination among academic and
research institutions, and public health practitioners.
• Evaluate the application of teledentistry to the Evaluation should be built into existing programs and
provision of dental care in remote locations. campaigns to guide future efforts.
18Issues Strategies
• Oral health problems are not measured and • Encourage stakeholders to participate in surveillance
reported adequately, including dental caries, activities and use the data that are obtained.
periodontal disease, trauma, oral cancer, risk factors,
• Develop measures, both quantitative and qualitative,
and distribution of the workforce and utilization of
for quality improvement among dental plans.
dental services.
• Develop metrics to determine network adequacy
• Evaluation measures and systems for continuous
among dental plans, and identify measurable
quality improvement are needed in programs aimed
indicators to assess quality of care as well as the
at improving oral health.
plans’ ability to meet community needs.
• Current strategies for improving oral health are not
• Conduct a survey of providers, clients and health
addressing disparities adequately.
plans to identify key issues affecting the delivery of
Objectives services and client utilization.
Objective 7.a: By 2015, develop measures to assess • Convene a workgroup of researchers and public
the implementation of pediatric dental benefits in the health practitioners to develop and set priorities for a
Affordable Care Act. research agenda.
Objective 7.b: By 2015, establish a collaborative process • Identify potential collaborators and funding
to develop and implement a quality improvement opportunities to support research priorities.
framework for dental care plans throughout NYS. Disseminate research findings so they can be used
by community organizations and are accessible to
Objective 7.c: By 2017, enhance systems which provide
the public.
evaluation and improvement of health care plans and
consumer-based information systems by developing • Evaluate the effectiveness of existing campaigns in
and including oral health measures. improving public knowledge, behavior and attitudes
toward oral health.
Objective 7.d: By 2017, bring together academic and
research institutions and public health practitioners to • Offer technical assistance to providers for evaluation
develop and implement a research agenda. of their public health programs.
Objective 7.e: By 2017, expand the New York State • Work with CDC and the State Education Department
Oral Health Surveillance System to collect data from to explore inclusion of oral health questions in the
additional sources, including community dental Youth Risk Behavior Surveillance System (YRBSS).
clinics, schools, private dental practices and care
• Assess smokeless tobacco use in the oral health
coordination entities.
module in the BRFSS and YRBSS.
Objective 7.f: By 2017, develop a system to continuously
• Identify existing data collection systems regarding
update information about workforce, facilities
diabetes, the elderly and pregnant women and explore
and demographics that will identify areas for the
opportunities to include oral health indicators.
development of new dental practices.
19• Expand the Pregnancy Risk Assessment and • Create partnerships to promote, share and use data.
Monitoring System (PRAMS) to ascertain the need for
• Increase the capacity to evaluate programs by
dental care.
collaborating with partners.
• Replicate the survey of physicians and nurses
• Explore the feasibility of adding a measure on
(administered as part of their re-registration process
dental sealants to the Medicaid Managed Care
every three years) to collect information about
quality measures.
dentists and dental hygienists. Use the Statewide
Planning and Regional Cooperative System (SPARCS) • Evaluate and implement quality standards for early
to assess oro-facial injuries. care and education programs that promote healthy
meals and snacks and promote personal oral health
• Collect data from school-based programs to assess
care practices.
the occurrence of oro-facial injuries and factors
involved in the injury.
• Develop and maintain a page on the NYSDOH web
site to display oral health data.
• Communicate surveillance data results to local health
units, health centers, hospitals, schools of dentistry
and dental hygiene and professional organizations.
20IV. Prevalence, Risk Factors and Workforce
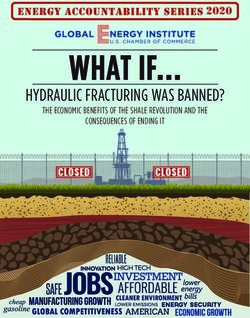
In New York State, data are available on oral health status, Cleft Lip and Cleft Palate
risk factors, workforce and the use of dental services to
Cleft lip and cleft palate are among the most common
assess problems, monitor progress and identify solutions.
congenital anomalies. These conditions may occur as
The following indicators provide useful information to
isolated defects or as part of other syndromes. Among
assess progress toward selected Healthy People 2020 oral
children born in 2008, NYS had 128 cases of cleft palate
health objectives.
(5.2 per 10,000 live births), 57 cases of cleft lip
Oral Health Status in Young Children (2.3 per 10,000 births) and 113 cases of cleft palate and lip
(4.6 per 10,000 births).23
In the United States, dental caries in children is the most
common chronic disease, and the need for treatment is also Oral Health Status in Third-Grade Children
most frequent. Nationally, the most recent data indicate that
The following data are derived from a survey of third-
approximately 24 percent of three to five year-old children
grade children conducted during 2009-12 by NYSDOH
have untreated dental decay (HP 2020 target 21.4 percent).
in collaboration with many partners. In this survey, oral
Only 26.7 percent of low-income children had received
health screenings were conducted on 6,758 third-grade
any preventive dental service. A survey of a disadvantaged
students from selected elementary schools in the 57
group of children in northern Manhattan found a high level
counties and New York City. Schools were selected using a
of unmet need.22 Because management of young children in
stratified random sampling method. Dental screenings were
a dental office is difficult, many children require treatment
conducted in schools to obtain data related to dental caries
in an operating room. In New York, approximately 5,683
and sealant use. A questionnaire was used to gather data on
children younger than six years of age visited a hospital
last dental visit, fluoride tablet use and dental insurance.
emergency department or ambulatory care center in 2008
for the treatment of dental caries.
Figure 1. Clift palate and cleft lip cases per 10,000 live births. New York State Congenital Malformation Registry, 2008.
Prevalence/10,000 Live Births
6
5.2
4 4.6
2
2.3
0
Cleft Palate Cleft Lip Cleft Lip and Palate
Source: www.health.ny.gov/diseases/congenital_malformations/cmrpubli.htm
21You can also read