Post-Covid syndrome pathway Webinar 26.01.2021 - Barnet Primary ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Post-Covid syndrome pathway Webinar 26.01.2021
Agenda • Where we are now • Definitions • Demand • Case studies – Specialist Post Covid Syndrome Clinic, UCLH • Case Studies – Community therapy services, CNWL • Primary care assessment, investigations and referral criteria • Care pathway/service development • Self Care • Next steps Post Covid Syndrome Webinar: 26th January 2021 2

Housekeeping
Q&A
Do stay on mute to Do keep your camera off Feel free to use the Questions posted
reduce any to allow presenters to be chat for any questions/ in the Chat will be
background noise visible. thoughts you have collated and
when others are during the session Answered on a
speaking sheet which will be
distributed out to
all Practices.
Post Covid Syndrome Webinar: 26th January 2021 3
Introduction • Post Covid syndrome recognised early on in the pandemic - still learning • Multi disciplinary care key to effective management • Pathway/service development – local/regional/national level • Collaboration across all providers in NCL – developing NCL integrated Post Covid Care • Provider capacity and new skills required Post Covid Syndrome Webinar: 26th January 2021 4
Definitions
NICE definitions: www.nice.org.uk/guidance/ng188
• Acute COVID-19: signs and symptoms of COVID-19 for up to 4 weeks.
• Ongoing symptomatic COVID-19: signs and symptoms of COVID-19 from 4 to 12 weeks.
• Post-COVID-19 syndrome: signs and symptoms that develop during or after an infection consistent with COVID-19, continue for more than
12 weeks and are not explained by an alternative diagnosis
Post-COVID-19 usually presents with clusters of symptoms, often overlapping, which may change over time and can affect any system within
the body.
Persistent and Cognitive blunting “brain
Breathlessness Pain Anxiety and depression
fluctuating fatigue fog”
What do we know about patient experience nationally?
The following experiences were taken from an Oxford series of interviews with over 100 patients experiencing Long Covid
• Can feel dismissed – patients are told there’s nothing wrong with them or are anxious, particularly if no positive test
• Experience fragmented care – e.g. specialist services can confirm ‘no heart attack’
• Find it hard to access appropriate rehabilitation
• Need to be persistent to organize appointments and access care
The appropriate community response will likely require co-ordination across rehabilitation and long term condition teams, working alongside
mental health colleagues.
Post Covid Syndrome Webinar: 26th January 2021 5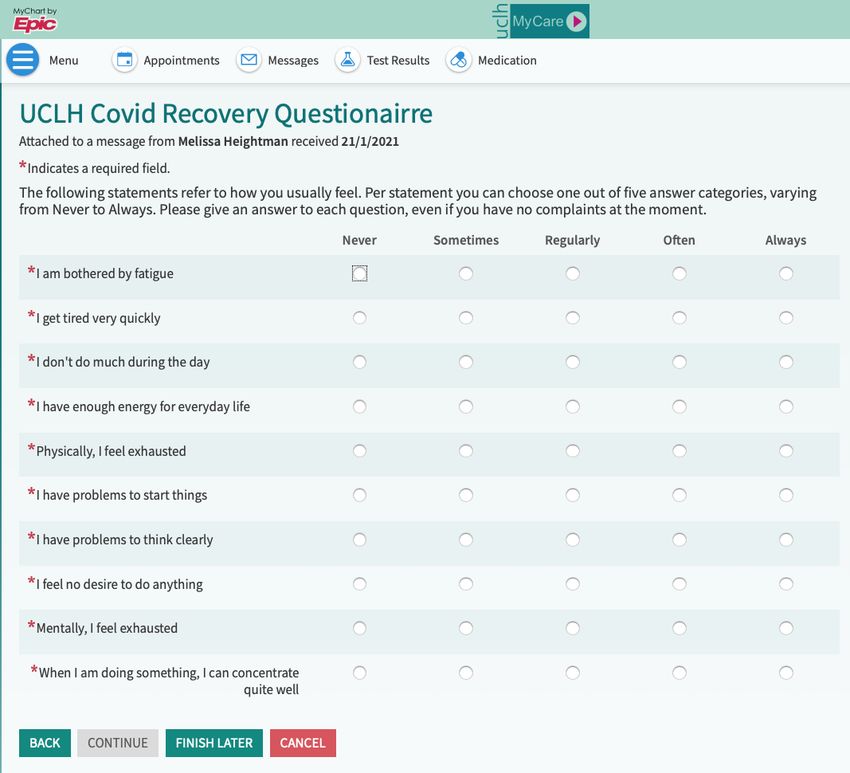
Demand
How many people are affected?
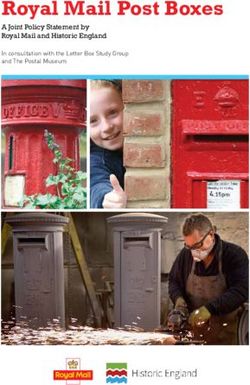
This table and modelling is adapted from NICE guidance: Managing the long-term effects of Covid-19
Category of need Barnet (pop Camden (pop Enfield (pop Haringey (pop Islington (pop Proposed NCL
396k) 262k) 338k) 271k) 240k) model
Diagnosed cases 6,558 (Nov) 3,362 (Nov) 5,768 (Nov) 4,033 (Nov) 3,370 (Nov)
24,771 (Jan) 11,734 (Jan) 25,509 (Jan) 17,433 (Jan) 12,619 (Jan)
People who were unable to 3,960 2,620 3,680 2,710 2,400 Primary Care
work for up to 3 weeks
because of Covid
People with chronic Covid, 1,980 1,310 1,690 1,355 1,200 Primary Care
who haven't recovered Community Team
within 12 weeks Acute Clinic
People with serious 396 (Nov) 262 (Nov) 338 (Nov) 271 (Nov) 240 (Nov) Specialist Clinic
debilitating Covid, not able Community Team
to take part in normal family
life
Post Covid Syndrome Webinar: 26th January 2021 6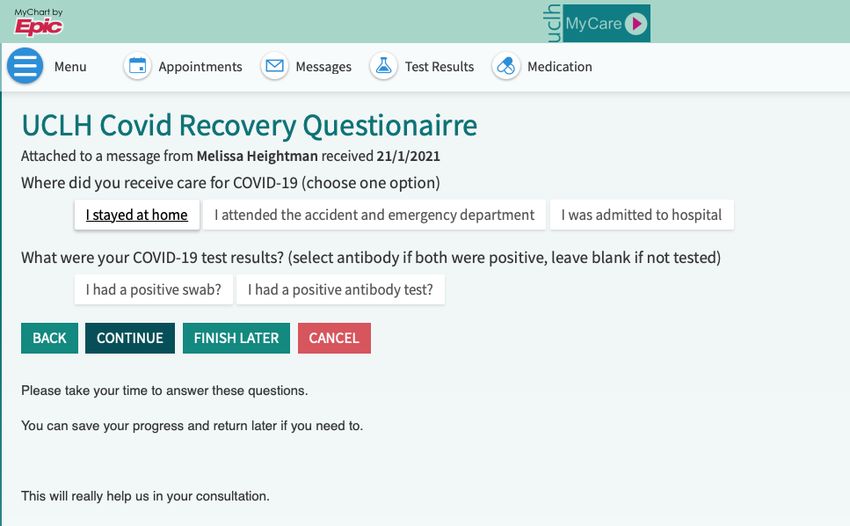
UCLH post covid clinic
• Running since May. 1600 appointments. 50% non hospitalized
• Still seeing wave 1 and now getting wave 2- 80 appointments a week
• GP referred/ Post ED/ Post Hospital
• Some funding from Dec- March 2021.Workforce stability challenge/
consultant delivered service
• Respiratory/ Cardiology/ Gastro/ Neuro/ ENT/ Allergy/ Rheumatology
• Trying to minimise wait times and speed access to diagnostics
• Primary care referral to ERS- then telephone triage to prioritise/ arrange
investigations but then F2F unless minor symptoms
• Borough level SPA may take over this function in due course
• In-house MDT plus community MDTs weekly (compromised by surge)
Post Covid Syndrome Webinar: 26th January 2021 7
UCLH Post-COVID clinic team
Dr. Melissa Dr. Toby Hillman Dr. Kay Roy Dr. Michael Prof. Marie Sculley Dr. Rob Bell Dr. Arjun Nair
Dr. Michael Zandi
Heightman Consultant Consultant Marks Consultant Consultant
Consultant NeurologistProfessor of
Clinical Lead for Respiratory Respiratory Consultant Haematology Cardiologist Radiologist
COVID follow-up Physician Medicine Infectious
clinic at UCLH Diseases
Jade Prof. Jeremy Brown
Dr. Emma Dr. Puja Mehta Alexander Professor of
Brett Gregory Helen Purcell SpR Clinical
Denneny Administrator Respiratory Medicine
Respiratory Respiratory Research
Clinical Research
Rebecca Livingstone Physiotherapist Physiotherapist Fellow
Fellow
Respiratory
Physiotherapist
Stephanie
Smallwood
Respiratory
Physiotherapist
Kameron
Coleman Alisha Chauhan, Rebecca Evans,
Administrator Junior Doctors
Post Covid Syndrome Webinar: 26th January 2021 8
Typical presentation: Case 1 • 37 year old woman • COVID in March 2020- private PCR +ve • Migraine, myalgia, breathlessness • Chest pain- anterior- pressure • Profound fatigue • Some improvement in April- returned to cycling • Deterioration in May- recurrence of chest pain • CTPA via ED – normal • Fluctuating course from there- breathless/ fatigue/ chest pain Post Covid Syndrome Webinar: 26th January 2021 9

Structured Assessment: now done via UCLH patient portal and merges with record Post Covid Syndrome Webinar: 26th January 2021 10
Case 1: structured assessment results Symptoms VAS- breathlessness now 4/10, fatigue 7/10, palpitations 7/10, chest pain 5/10 Overall only 50% of usual health MRC breathlessness 3 and Fatigue Assessment Scale 29 PHQ2=2/ GAD2 =2 Unable to work full time No desaturation on sit to stand but only 27 reps. HR 140 post Post Covid Syndrome Webinar: 26th January 2021 11
Case 1: Initial diagnostics • Bloods: normal FBC, UE, LFT. D-dimer 430. Troponin 3, NT BNP30 c/w POTS. Normal catecholamines at baseline/ tilt. No signs of autonomic failure Post Covid Syndrome Webinar: 26th January 2021 12
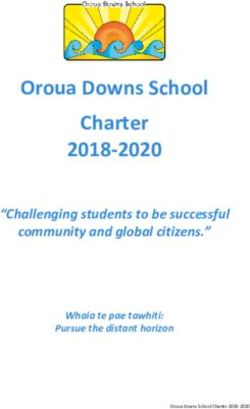
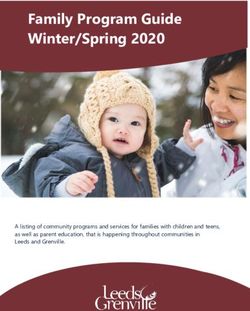
Case 1: initial diagnostics • CMR: resolving myocarditis (repeated as abnormal Coverscan MRI) • Migraine review- over-using zolmitriptan. Couldn’t tolerate amitryp or topiramate. Problem preceded COVID- referred to psychology • 6MWT- normal pO2 and lactate post Stock CMR image as example (not scan from exercise Case 1) Post Covid Syndrome Webinar: 26th January 2021 13
Case 1 Treatment plan • Lifestyle advice for POTS • Trial of low dose bisoprolol for POTS • Trial of colchicine for myocarditis • Ongoing migraine management (complex in her case as preceeding diagnosis) • Referral to fatigue services- careful pacing due to myocarditis and post exercise malaise Post Covid Syndrome Webinar: 26th January 2021 14
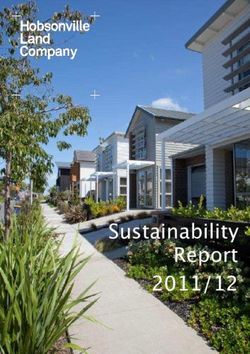
Case 2 • 56 year old woman • COVID in March- not tested. Serology neg. FH of hypermobility • Severe fatigue and breathlessness. Also skin rashes. Palpitations. Limb spasms and calf pain on walking. Unable to work • FAS 41 • Sit to stand: HR increased to 145. No desat. 33 reps Borg 5 Systolic dropped 20 and diastolic 6 on standing. HR 79 to 101 (so not above abnormal threshold for eg POTS) • D-dimer persistently raised 1200. CTPA normal. CK 148 • Holter- HR up to 150 with activity • Awaiting CMR Post Covid Syndrome Webinar: 26th January 2021 15
Case 2 Post Covid Syndrome Webinar: 26th January 2021 16
Case 2 treatment plan • Trial of bisoprolol for HR and BP (intolerant of ACEi prev, nifedipine originally but changed to amlodipine given tachycardia) • Given advice and plan re fatigue management and referred on to community services (letter returned flagging capacity issues at present) • Trial of antihistamine for rashes and checking tryptase level • Referred to ENO breathe program • Awaiting neurology autonomic assessment but not expecting severe abnormality • For further studies to review lactate on walking and D-dimer………. Post Covid Syndrome Webinar: 26th January 2021 17
Covid-19 Case Study Presented by Rachel Okin (Complex Neuro Navigator and Team Lead Camden Community Stroke and Neurology Service) Heidi Ridsdale (Clinical Lead and Manager Camden COPD and Home Oxygen Service) Camden Integrated Adult Services
PD
68 year old male
Lives alone
Works full time for TFL (irregular shift
patterns) PMH: HTN
Interests include: reading, seeing
grandchildren, walking, fishingPatient Journey – Community Managed
Community Managed Specialist Assessment Clinic Community Services
• 29/9/20- Initial symptoms • 30/11/20- initial assessment • 3/12/20-Reviewed by Community neurology
• Suspected Covid – not confirmed • Presented with severe fatigue and team, OT, PT
on testing breathlessness • 11/12/20 – completed key outcome measures
• Nil hospital admission • Referred to community neurology team for • 9/12/20 – onboarded on to Living With Covid
• Remote consultations with GP fatigue management App
• Referred to respiratory physiotherapy • 29/12/20 - Referred to Icope by GP
• Referred to Post Covid Clinic
outpatients for breathing pattern retraining
by GP
• Mid Jan 2020 -Troponin raised plus ECHOInitial Presentation
Fatigue
Cardiorespiratory
Neurology
Mood
•Nil desaturation •Memory impairment •Requiring regular rests in the •Anxiety ++ regarding recovery,
•Breathless with minimal exertion •Difficulties with concentration day •Irritable and ‘short fused’
•Altered breathing pattern •Deconditioned + post Covid •Returned to work full time but •Declined iCOPE and neuro psych
•Fluctuating picture but little •Poor exercise tolerance both due not managing
improvement to breathlessness and muscle at this time
•Assistance housework/shopping
•CXR clear weakness •Low mood- sad about the whole
•Able to walk short distances situation and concerned about
•Unable to divide attention
only the future
•Altered taste
•Poor sleep patterns – waking
multiple times in the night
• Feeling of helplessness
•Fluctuating presentationCurrent Covid Rehabilitation Care
Specialist COVID
Assessment Clinic Living With Covid
Recovery App
Work
Occupational
Health
Primary Care and iCOPE
Cardiology
Community Services Patient
Mental health
Secondary Care
Community Neurology Team
Other (CNSS):
Friends/family OT, PT
GPPresentation at 4 months
•Anxiety ++ regarding
Mood
Cardiorespiratory
•Ongoing review with
Ongoing Rehab Need
Fatigue
•Breathless on exertion •Continues to report •Decreased rest periods recovery
Neurology
•Fluctuating picture with memory and in the day but this community neuro team
concentration deficits
•Referred to iCOPE
some improvement fluctuates considerably •Referral to fatigue group
but improving slowly •Reports feeling irritable
•Troponin raised •Able to walk short •Work OH review
distances •iCope +/- further mental
•Medication from GP for
sleep health support
•Altered breathing pattern •Provided with
strategies to manage •Able to return to work, •Provided with sleep hygiene •Self management through
with improved insight and but has just been signed digital platform
management. memory advice and taking on board
off again these strategies
•Breathlessness now not •Referred to OH at work
main symptom •Taught strategies around
•Using a fatigue diary to relaxation
manage fatigue •Reports finding the app +
symptoms/pacing helpful and reassuringSA
44 year old male
Lives with wife and 12 year old child
2nd Floor Flat
Bangladeshi
Works full time in retail No significant previous past medical
Car Driver history
Interests include: badminton, Very seldom visited the GP
football, walking, involvement in the
Mosque, local community and
leading a charityPatient Journey – Hospital Admission
Hospital Admission Community Services
12/4/20 - 12/6/20 To date Specialist Assessment Clinic To date
•13/4/20 ITU admission Intubation
and ventilation required for 4 • 12/6/20 Discharge to Assess (D2A) – Ensured • 13/07/20 Initial f2f appointment
weeks safe at home, discussed with Camden • Referred to specialist Cardiology, Neurology,
community teams and referred for community ENT
•23/4/20 MI rehab
•Proning injury peroneal nerve • 15/6/20 – Return to hospital as breathless + • Investigations: CT, Bloods, ECHO. Cardiac MRI,
causing foot drop Cardiac Stress Test
desaturating,
• 30/6/20- Joint assessment with Community • Exercise desaturation linked to post-COVID
Neuro and COPD services fibrosis
• SLT, Neuro Psychology, OT and PT • Initiated on Prednisolone (30mg OD)
• Regular reviews in collaboration with • Providing ongoing support f2f and virtually
Specialist Clinic and GP
• *** Living With COVID Recovery AppInitial Presentation on Discharge from
Acute Hospital
Fatigue
Diabetes Control
Mood
Neurology
•Foot drop •Requiring regular •Anxiety ++ regarding
Cardiovascular
•HTN, monitored by Respiratory •Desaturating on 1 •Fluctuating blood
GP flight of stairs •Falls risk due to above rests in the day recovery, finance, sugars
•Cardiac •Breathless at rest •Using stick •Able to walk for 1-2 return to work •New diabetes
investigations by •In respiratory •Walking indoors only min then rest management by GP
secondary care ‘distress’ likely due •Deconditioned, global •Assistance from wife •Low mood in and community
to post Covid lung muscle weakness relation to physical Diabetes team
•Limited to gentle with ADLs
disease
exercise only due •Not sleeping symptoms and
to cardiac risk •Quieter voice – speed of recovery,
•Coughing at night •Altered diet to reduce
difficulty speaking on also role in
so not sleeping the phone •Cognitive ‘fogging’ sugar intake
household
•Pain due to •Different sounding •Self reported
coughing voice memory problemsCurrent Post Hospital Covid Rehabilitation
Care
Specialist COVID
Assessment Clinic Community Community
Wife Neurology Team
COPD Team
(CNSS):
OT, PT, SLT,
Social Neuropsych
Worker
D2A (discharged
to CNSS, COPD GP
team)
Patient
Primary Care and
Community Services Living With
Dietician COVID Recovery
Secondary Care App
Social Services and
Camden
Housing Council –
ENT/Voice rehousing
Referral to
Neurology
Voc Rehab
CardiologyPresentation at 8 Months
Cardiorespiratory
Neurology and Current Function
•Unable to play • Significant and variable •Regular medical
Ongoing Medical Involvement
Mood
Fatigue
•Remains off work •Remains worried about
sports/run with son •Remains deconditioned fatigue role in the household and appointments across all
•Breathless on 3-4 •Residual foot drop with • Walking with stick outdoors his return to work specialities
flights of stairs/ pain in leg • Sleeping in the day •Anxious about going •Remains under the care of
walking 20 minutes • Requiring rest days without outside Community Neuro and
leaving the flat 2-3 COPD teams for rehab/
•Independent with ADLs monitoring
•Coughing much •Voice has got louder and times/week •Mood variable but
improved generally low and anxiety •Using Living With COVID
he can speak on the Recovery App
•Steroids weaned and phone, but still sounds •Able to walk 30 min to pick increasing
stopped different son up from school 2-3 •Has strategies to use to •?Discharge
times/week with 2-3 rests help manage anxieties
•Using fatigue diary to •Recently accepted
enable management referral to talking
therapies for moodWhat have we learnt clinically? • Complex medical and rehabilitation needs – this is not ONLY a respiratory presentation • Safety netting is key • Varying phenotypes, signs and symptoms • Patient presentation fluctuates significantly over time • High levels of anxiety +/- low mood and FATIGUE • Subtle presentation such as cognition (‘brain fog’) • Wider MDT and collaborative working is essential
Assessment in general practice
History: Care planning:
• Patient to complete pre- • Agree patients' goals
assessment questionnaire
• Confirm date Dx and tests
undertaken
• Symptoms at start of infection
and currently, identify if
fluctuating and trends
• Fatigue – general and after
activity
• Psychosocial issues
Post Covid Syndrome Webinar: 26th January 2021 30Assessment in general practice Examination (guided by presenting symptoms): • Temperature • Oxygen saturation • Pulse rate and rhythm • BP sitting and standing • Sit to stand test • Heart sounds • Chest • CNS/PNS Post Covid Syndrome Webinar: 26th January 2021 31
Assessment in general practice Investigations: • Covid-19 serology (if no previous • Cortisol (9am – if persistent fatigue)* antigen test results) • CXR • FBC, U&Es, TFTs, LFTs, Calcium* • ECG* • Ferritin • Vit D • CRP • Hba1c* • BNP* • Lipid profile *dependent on presenting symptoms Post Covid Syndrome Webinar: 26th January 2021 32
Symptom specific pathway
Cough Breathlessness
• If ongoing cough at 4-6 weeks arrange CXR via • Persistent breathlessness is common up to 4-6 weeks
normal referral route. If CXR shows extensive but the trend should be showing improvement.
abnormality refer patient to the Post-Covid • If ongoing breathlessness, conduct a general
Clinic. Check STS and if desaturating is urgent. respiratory examination and sit to stand test
• If CXR changes minor/ improving monitor considering asthma and other causes. Note HR/ chest
clinical course and repeat at 12 weeks. If pain- consider if features of PE. Complete CXR as per
abnormalities still present or worsening cough
symptoms, refer to the Post-Covid Clinic. • If no desaturation and improving trend/ CXR clear or
• Consider acid reflux, post-nasal drip and improving continue to monitor in primary care. Note
asthma (using home peak flow diary). MRC breathlessness score (patient self score).
• Assess breathlessness in conjunction + • 1-2, advise your covid recovery website for self
complete sit to stand test to look for management
desaturation (needs urgent referral to Post • 3 refer to community rehabilitation
COVID clinic) • 4+ or other red flags/ desaturation/ CXR
concern refer to Post-Covid Clinic
Post Covid Syndrome Webinar: 26th January 2021 33Symptom specific pathway
Palpitations Presyncope/ orthostatic intolerance
• Palpitations are common post COVID. Take • If patient has postural dizzness take cardiac
history of nature/ triggers/ any associated history + carry out CVD exam including, pulse,
chest pain or presyncope BP sitting and standing (consider 10 minute
• Arrange ECG and consider 24 hr Holter lean test), sit to stand test.
• Look for features of POTS- HR >120 or • Consider other CVD causes (e.g. myocarditis
increase of >30 on standing. Look for and pericarditis may cause dizziness). Consider
orthostatic hypotension-drop of >20mmHg in pulmonary embolism (which can present with
systolic or > 10mmHg in diastolic within 3 presyncope and tachycardia without
mins of standing desaturation or chest pain (greater incidence of
• Consider risk of PE if persistent tachycardia. PE in first 4- 6 weeks post-Covid)
Greater risk in first 4-6 weeks.
• Consider POTS as per palpitations and
• If exertional chest pain/ presyncope consider consider referral
referral to post covid clinic.
• If no indication of other causes, refer to Post-
Covid Clinic. Do not consider for community
rehabilitation.
Post Covid Syndrome Webinar: 26th January 2021 34Symptom specific pathway
Chest Pain
• If patient has ongoing chest pain consider
ischaemic heart disease, pleuritic chest pain
and MSK chest pain (if Costochondritis treat
with anti-inflammatories).
• Refer for CXR and ECG, thinking about
pericarditis on ECG.
• Consider post-Covid clinic referral if severe,
exertional or other worrying features on sit to
stand or discuss in MDT for consideration of
referral for troponin and cardiac MRI
• Assessment may be needed to reassure re
fitness for rehab (clinical judgement)
Post Covid Syndrome Webinar: 26th January 2021 35Symptom specific pathway
Fatigue Depression and anxiety
New onset related to Covid vs. premorbid
• This is often a long lasting symptom post
depression and anxiety. Consider early referral
COVID and should be considered alongside
to IAPT. Be aware of increased risk suicidal
other symptoms such as breathlessness/ brain
ideation.
fog
Assess using PHQ9 and GAD questionnaire –
• Ask re presence of post exercise malaise
manage expectations here, talk about learning
• Consider other causes (anaemia/ thyroid etc.) to manage understandable elevations in
• If severe consider referral to post covid clinic emotional distress/ MH symptoms. Signpost to
or community services depending on whether learning tools to prepare for a recovery journey
other red flags symtoms from COVID using peer support and community
COVID resources (e.g. recovery apps, recovery
• Signpost patient to colleges, Covid support groups and courses)
www.yourcovidrecovery.nhs.net for advice re
pacing. Period of reduced activity may be If a patient was on ICU they MAY have received
necessary to allow progress input from hospital health psychology. Confirm
before referral to IAPT, if no health psychology
input, refer to Post Covid Integrated MDT
Consider features of post traumatic stress
Post Covid Syndrome Webinar: 26th January 2021 36Symptom specific pathway
Cognitive impairment/ brain fog Muscle and joint pain
• Assess using GPCOG , take a detailed history • Take a history to identify any symptoms of auto-
of symptoms. Assess for underlying depression immune or inflammatory conditions, carry out
and anxiety, or other symptoms indicating baseline investigations. If joint swelling and
dementia stiffness, consider referral to rheumatology or
post covid clinic depending on symptom
• If dementia considered, undertake dementia
spectrum. Consider CK level/ autoantibody
screen in addition to tests already completed
profile
and consider referral to Memory service.
• If investigations are normal, signpost to Your • If no synovitis/ other concern, manage as fatigue
Covid Recovery and follow up – if does not (as above) and discuss with MDT. Signpost to
help refer to MDT discussion for further Your Covid Recovery. Recommend analgesia
signposting and referral Poor sleep quality
• If physical fatigue presenting alongside • Take full history, consider managing underlying
cognitive fatigue, see fatigue management physical causes or depression and anxiety (see
(above) above)
• If unusual neurology symptoms in a non- • Give sleep hygiene advice and signpost to Your
hospitalised patient, consider other Covid Recovery
neurological causes and refer as appropriate
Post Covid Syndrome Webinar: 26th January 2021 37Symptom specific pathway
Headaches Anosmia / Parosmia
• Carry out neurological assessment. If • Offer smell, taste, nasal hygiene advice.
features of migraine manage as per migraine
• 0-6 weeks send link to smell training
advice. This symptom is common in the first
six weeks so review the trend over time. • Refer to specialist smell clinic under Mr Peter
Andrews, RNENT UCL after 12 weeks if no
• If red flag refer to neurology urgently. improvement – or general post covid clinic if
• If normal neurological examination and non- multiple other symptoms
improving headaches with eg treatment for
migraine – discuss at MDT for next steps or Skin rashes
refer post covid neurology clinic.
• Some patient report urticarial type lesions.
Take history of wheezing/ abdominal cramps/
diarrhoea). Possibility of mast cell activation
syndrome – uncertain incidence/ ? rare
• COVID digits (consider referral to post covid
clinic if non resolving/ multiple digits involved.
Confirm peripheral pulses present)
Post Covid Syndrome Webinar: 26th January 2021 38Supporting self-management
Your Covid Recovery Voluntary sector offers
Online portal for self-guided recovery – Connecting people to voluntary sector
encouraging primary care to refer organisations who can provide support
patients to self manage online where with post-Covid Syndromes including
appropriate. English National Opera, yoga and smell
https://www.yourcovidrecovery.nhs.uk/ training.”
We are working with NHS charities on
how best to use charity funding to
support patients with post-Covid
syndrome, with a focus on digital
inclusion and health inequalities.
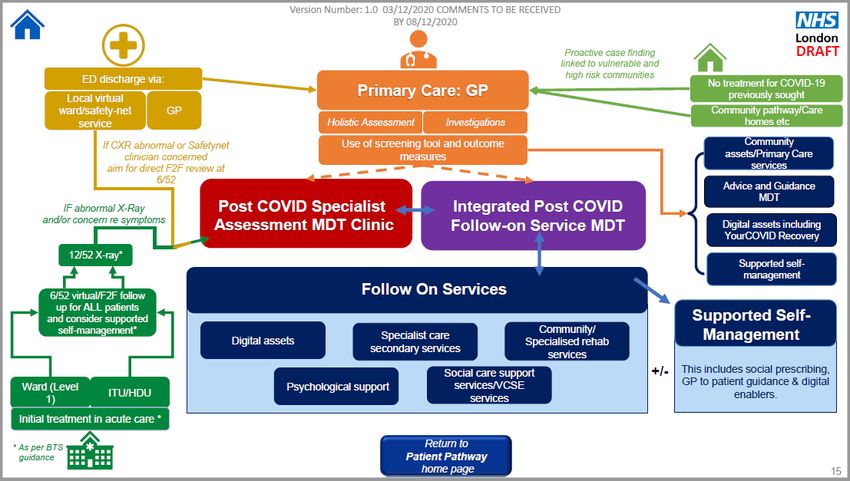
Post Covid Syndrome Webinar: 26th January 2021 39Post-Covid Pathway (10 Dec 2020)
Key Nomenclature – Post COVID terminology Key Nomenclature – multi-disciplinary team (MDT) terminology
Post COVID-19 Pathway: Inclusive of acute, ongoing Integrated Post COVID Follow-on Service MDT “Single Point of Access” - This is
symptoms and post COVID as per NICE definition and the multidisciplinary gateway service into follow on rehabilitation and
irrespective of discharge from an acute trusts, previous community services. The single point of access service would act on the trusted
positive SARS-Cov-2 serology or clinical diagnosis in the assessment from the specialist assessment clinic and provide navigation into
absence of a clinical test. local rehabilitation assets, which they would have a role in curating taking
account of local service configuration. Follow on services should include
Post COVID Syndrome: Signs and symptoms that physical, mental, neurocognitive and social integration.
develop during or following an infection consistent with
COVID-19, continue for more than 12 weeks and are not Post COVID Specialist Assessment MDT Clinic “Specialist Assessment Clinic”
explained by an alternative diagnosis The specialist assessment clinic is part of the network of designated sites
delivering to the national specification and funding. This includes access to
Post COVID Syndrome Pathway: Describing the patient diagnostic, functional, psychological needs and physiological assessment. This is
pathway from presentation with symptoms aligned with a multidisciplinary specialist clinic as defined in the national commissioning
Post COVID Syndrome to, and including, referral to guidance providing personalised care plans and trusted assessment for primary
onward support and self-management and a loop back care and referral to single point of access services to access rehabilitation
into the MDT services services.
Post Covid Syndrome Webinar: 26th January 2021 40Post-Covid syndrome - high level
pathway
Face to face assessment including vital stats, sit to stand test, respiratory exam, anxiety and
depression screening, nervous system assessment, functional assessment, social, financial and
cultural circumstances. Consider rehab referral or referral to NCL Post-Covid Clinic. Support to self
manage using Your Covid Recovery resources.
Community rehabilitation including necessary fatigue and breathlessness management. Input
from specialist community nurse (where available). Consider referral to NCL Post-Covid Clinic if
appropriate.
3 clinics weekly. Aim for initial face to face assessment for diagnostic tests and for doctor and
physio review and then remote follow-up where possible. If needs ongoing physio assessment/
input or complex then further face to face arranged. Weekly MDTs with therapies, cardiology
and neurology. Some joint clinics where needed. Referral onwards to other hospital specialties
as required.
Post Covid Syndrome Webinar: 26th January 2021 41Post-Covid syndrome – role of
each area
Primary Care
Patients identified in Face to face assessment including vital stats, sit to stand test, respiratory exam, anxiety and
depression screening, nervous system assessment, functional assessment, social, financial and
Community (proactive cultural circumstances. Consider rehab referral or referral to NCL Post-Covid Clinic. Support to self NCL Post-
case finding by GPs manage using Your Covid Recovery resources.
Covid
focused on vulnerable Syndrome
groups MDT
Community Offer Attendees:
Community rehabilitation including necessary fatigue and breathlessness management. Input GP, NCL Post-
from specialist community nurse (where available). Consider referral to NCL Post-Covid Clinic if Covid
appropriate. Consultants,
Care Navigator,
Patients identified Community
following acute NCL Post-Covid Syndrome Clinic therapists,
Specialist
3 clinics weekly. Aim for initial face to face assessment for diagnostic tests and for doctor and
episode physio review and then remote follow-up where possible. If needs ongoing physio assessment/
Community
nurses,
input or complex then further face to face arranged. Weekly MDTs with therapies, cardiology psychology
and neurology. Some joint clinics where needed. Referral onwards to other hospital specialties
as required.
Post Covid Syndrome Webinar: 26th January 2021 42Model settings
Sector / Offer Cohort Geography / referral pathway
Provider
UCLH NCL Post-Covid Complex Post-Covid Syndrome symptoms requiring specialist, Pan NCL
Syndrome Clinic multi-disciplinary support for people who have ongoing Covid Referrals from Primary Care,
(to manage post- related needs. Community or Acute
Covid syndrome) In reach from Community and Primary Care
All Co-ordinated Integrated offer linking rehabilitation and mental health Borough based
community Community services for both Post-Covid Syndrome cohort and people who Referrals from Primary or Acute or
providers rehabilitation have been discharged after a Covid related admission. NCL Post-Covid Syndrome Clinic
Case management through UCLH app
All acute Post covid clinics Post discharge support for all patients following covid related Post discharge or referral only
sites (upon discharge) admission. Some of these patients may require referral to NCL
Post-Covid Syndrome Clinic.
Can refer on to community or discharge to primary care
General Long covid Registered cohort Borough based
Practice / support Agreed pathway to community or direct to specialist clinic Practice cohort
primary care Option to refer to local acute if single specialty input needed
network
NCL GP NCL Covid-19 Service offers acute Covid clinical support to primary care Operating from 2 sites across
Federations Support Service GPs, remote telephone triage and home visiting for patients Pan NCL
Post Covid Syndrome Webinar: 26th January 2021(there will be no face-to-face at either site in this phase). 43Developing the Post-Covid Syndrome multi-
disciplinary team (MDT)
MDT-working design Camden Post-Covid Syndrome MDT
• Steering group meeting fortnightly since • Virtual MDT tested with primary care,
November 2020 with representation from UCLH, CNWL and mental health input
the whole pathway and all NCL boroughs
• Continues to be iterated and tested again
• Created a best-practice pathway for co- based on attendee feedback to ensure best
ordinated patient care between primary value for people’s time and to create a
care, community and hospital settings spreadable model for consistency in NCL
• Guidance for primary care in final draft with • Plan to begin spreading to other NCL
approval from LMC – practices will be able boroughs from January onwards beginning
to draw on the GP Capacity Fund to with Whittington Health
resource case-finding, assessment and
• Identifying ongoing primary and community
multi-agency working
development needs and resource required
• Borough-based MDTs will support primary to deliver a regular service.
care clinicians, and provide expert input into
complex and ongoing cases
Post Covid Syndrome Webinar: 26th January 2021 44Next steps
1. Post-Covid syndrome teaching webinar for primary care 26 January
2. Launch primary care post-Covid guidance with primary care including
supporting resources (EMIS templates, screening tools, referral forms
etc.)
3. Scale up post-Covid MDT to all NCL boroughs
4. Ongoing monitoring of service capacity and training needs to ensure a
high quality service offer in all boroughs
5. Continue to work with voluntary sector and NHS charities to create a
broader community offer to residents
Post Covid Syndrome Webinar: 26th January 2021 45You can also read