Prevention and management of moisture-associated skin damage - Ennogen
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PRODUCT FOCUS
Prevention and management of
moisture-associated skin damage
T
he promotion and maintenance of skin integrity is a
common challenge in all care settings and is often ABSTRACT
used as an indicator of the overall quality of nursing Disruption to the integrity of the skin can reduce patient wellbeing and
care provided. In simple terms, skin integrity can be quality of life. A major cause of skin breakdown is prolonged exposure to
defined as the skin being ‘whole, intact and undamaged’ and moisture, but this is often overlooked. When skin is wet, it becomes more
disruption to skin integrity can have a negative effect on susceptible to damage from friction and shearing forces, and skin flora can
patient wellbeing and quality of life (Woo et al, 2017; penetrate the disrupted barrier, causing further irritation and inflammation.
Fletcher et al, 2020). If untreated, moisture-associated skin damage (MASD) can rapidly lead to
While the threats to skin integrity presented by pressure, excoriation and skin breakdown. MASD includes incontinence-associated
shear and friction are well known, frequent exposure of a dermatitis (IAD), which is caused by prolonged skin exposure to urine and
patient’s skin to excessive moisture is often overlooked as a stool, particularly liquid stool. For patients at a high risk of developing IAD,
major cause of skin breakdown. preventive measures should be instituted as soon as possible. The main
The term moisture-associated skin damage (MASD) has one is to prevent excessive contact of the skin with moisture. Optimal
been adopted to describe the spectrum of damage that results skin care should be provided to patients with any form of MASD. It should
from prolonged exposure of a patient’s skin to various be based on a structured regimen and include the use of a gentle skin
sources of moisture, including urine or stool, perspiration, cleanser, a barrier product and moisturiser. Derma Protective Plus is a
wound exudate, mucus and saliva (Voegeli, 2019). However, liquid barrier that gives long-lasting protection against chafing or ingress of
MASD is a general umbrella term to describe any skin urine and stool into the skin. This product is less greasy than others, and
damage caused by moisture, and generally considered to provides a barrier and a healing environment, with resistance to further
include four commonly encountered separate conditions that maceration from IAD or persistent loose stools.
often coexist. These are: incontinence-associated dermatitis Key words: Moisture-associated skin damage ■ MASD ■ Incontinence-
(IAD); intertrigo; periwound moisture-associated dermatitis; associated dermatitis ■ IAD ■ Derma Protective Plus
and peristomal moisture-associated dermatitis (Figure 1).
This article provides a general overview of the
mechanisms of moisture-associated skin damage, focusing on ‘rivets’ called desmosomes; this is the so-called ‘bricks and
IAD, and outlines the components of effective prevention mortar’ model (Rawlings, 2010).
strategies and interventions to manage MASD and promote Enzymes within the epidermis act on phospholipids to
skin health. produce a mixture of ceramides, free fatty acids and
cholesterol (Darlenski et al, 2011), which help to regulate
Normal skin barrier and control of moisture stratum corneum structure and function. The stratum
A major function of healthy, intact skin (Figure 2) is the corneum also contains a mix of substances that actively
maintenance of a physical barrier against the external attract and hold water in the corneocytes, collectively termed
environment. This prevents the entry of noxious substances natural moisturising factor. The natural moisturising factor
and pathogens, as well as providing an important moisture acts by absorbing water from the atmosphere and deeper
barrier, preventing excessive fluid gain and loss from the layers of the skin, enabling the outermost layers of the skin to
body. remain hydrated, despite the drying action of the
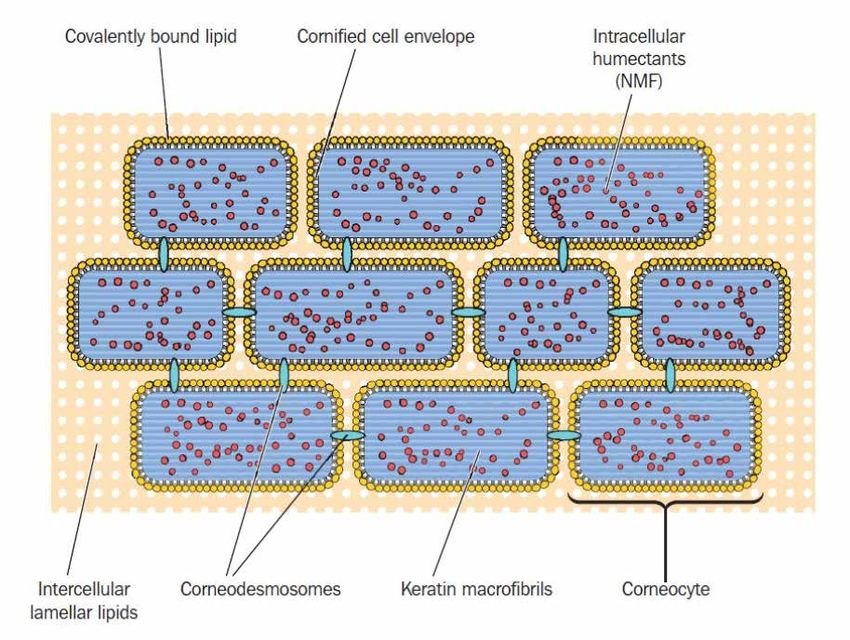
This is achieved by the uppermost layer of the skin, the environment. By increasing intracellular water, they allow the
epidermis, in particular its outermost part, the stratum corneocytes to retain their turgidity and shape, thus
corneum (Figure 3). The stratum corneum is composed of maintaining a flexible, barrier (Voegeli, 2012).
tightly packed, flattened, protein-rich cells called corneocytes, The skin barrier is further enhanced by the maintenance
which are held together by a lipid-rich matrix and protein of an acidic surface with a pH of 4–6, termed the acid
mantle. This helps to maintain a healthy balance of resident
skin bacteria; it is also recognised that skin pH plays an
© 2021 MA Healthcare Ltd
David Voegeli, Professor of Nursing, Faculty of Health and
Wellbeing, University of Winchester. David.Voegeli@winchester.ac.uk important role in regulating skin health and stratum
Sarah Hillery, Urology Advanced Nurse Practitioner, York Hospitals
corneum cohesion (Ali and Yosipovitch, 2013).
NHS Foundation Trust. sarah.hillery@nhs.net Disruption of these carefully balanced mechanisms can
Accepted for publication: June 2021 lead to either excessive skin dryness (xerosis) or too much
water (which can predispose the skin to MASD), both of
This article was reprinted from the British Journal of Nursing 2021, Vol 30, No 15: TISSUE VIABILITY SUPPLEMENT
PRODUCT FOCUS
exact mechanisms by which excessive moisture causes
irritation are still debatable and, to date, comparatively little
Incontinence- work has been done to explore the mechanisms involved in
each type of MASD. However, histological studies have
associated Intertrigo shown that moisture damage appears to be a result of the
dermatitis intercellular lipid ‘mortar’ of the stratum corneum and the
corneocytes being disrupted and, in effect, ‘dissolving’ the
physical barrier (Warner et al, 2003).
Moisture- Once saturated, wet skin is more susceptible to damage
caused by friction and shearing forces, and further irritation
associated skin and inflammation can occur as the normal skin flora is able
damage to penetrate the disrupted skin barrier and activate the skin’s
well-developed immune defences (Newman et al, 2007).
Incontinence-associated dermatitis
IAD is perhaps the most widely recognised type of MASD,
Peristomal Periwound and certainly one of the most widely studied (Gray et al,
dermatitis dermatitis 2012; Beeckman et al, 2015). It is suggested that prevalence
rates for IAD vary from 5.6% to 50% across all healthcare
settings and are highest in people with faecal incontinence
Figure 1. Conditions that fall under the umbrella term of moisture-associated and those who live in residential care settings (Beeckman et
skin damage al, 2015;Voegeli, 2019).
A national audit conducted across 66 hospitals in Wales
which can cause the skin barrier to fail. evaluated a total of 8365 patients and found IAD in 360,
More recent models of skin barrier function suggest it representing a prevalence of 4.3% (Clark et al, 2017). Several
comprises four separate components involving different risk factors for the development of IAD have been identified,
layers of the skin (surface microbiome, chemical barrier, the main ones being incontinence of urine, faeces (or both),
physical barrier and immune barrier) working in harmony to frequent incontinence episodes, use of occlusive containment
maintain overall skin integrity and offer some insight into products, pre-existing skin conditions, poor mobility/dexterity
the mechanisms involved in MASD (Eyerich et al, 2018). and an inability to maintain personal hygiene (Johansen et al,
Overhydration of the skin, particularly the stratum 2018;Van Damme et al, 2018). Given the large number of
corneum, can precipitate inflammation by facilitating the patients affected, the prevention and management of IAD
passage of irritants into the skin, leading to dermatitis. The presents a significant financial burden for healthcare systems. In
the community in England alone 406 376 prescriptions for
barrier products were issued in 2020, at a cost of £1.42
Peter Lamb
million (NHS Business Service Authority, 2021). However the
true cost is likely to be much higher, with many patients
self-funding their own preferred product.
Typically, IAD presents as inflammation of the skin surface
characterised by redness and, in extreme cases, swelling and
blister formation. In urinary incontinence, this generally affects
the labia in women and the scrotum in men, as well as the
inner thigh and buttocks in both sexes.
If untreated, IAD can rapidly lead to excoriation and skin
breakdown. In obese individuals, it often coexists with a
degree of intertrigo in the skin folds. This be followed by
infection by the skin flora (eg candida), leading to a vicious
circle of increased inflammation and skin breakdown.
Although IAD is one of the forms of MASD that attract the
most interest, the exact mechanisms remain poorly understood
(Koudounas et al, 2020).
It is generally agreed that urinary incontinence on its own
does not necessarily lead to IAD but, when combined with
faecal incontinence or the passage of liquid stool, the risk
© 2021 MA Healthcare Ltd
increases significantly. This is thought to be because of
overhydration of the epidermis and an increase in the skin pH
away from the protective slightly acidic range. The change to a
more alkaline pH activates digestive enzymes present in the
Figure 2. Skin structure faeces, which then further contribute to the damage caused to
This article was reprinted from the British Journal of Nursing 2021, Vol 30, No 15: TISSUE VIABILITY SUPPLEMENTPRODUCT FOCUS
Figure 3. Bricks and mortar arrangement of the stratum corneum (Voegeli, 2012)
the epidermis. Liquid stool tends to be richer in digestive important actions that can be taken. Ideally, skin care
enzymes, and this, when combined with its elevated water provided to any patient with any form of MASD should be
content, is particularly damaging to the skin (Gray et al, 2012). based on a structured regimen and involve the use of a gentle
skin cleanser, a protectant (barrier product) and moisturiser
Preventing and treating moisture-associated (if indicated). The use of ordinary soap and water should be
skin damage avoided as, in most cases, the pH of the soap is too alkaline
As the single causative agent in MASD is the overexposure of and may contribute to the skin irritation (Voegeli, 2012).
the skin to moisture, the main preventive measure should be Many newer cleansing products combine a cleanser with a
to avoid excessive contact of the skin with moisture. protectant and moisturiser, and are pH balanced to help
Although the quality of evidence for the prevention and maintain the normal, slightly acidic skin pH.
management of the different forms of MASD varies and is Following cleansing, the skin needs to be protected against
generally low, there is now an accumulated body of subsequent contact with moisture by a skin protectant or
knowledge and expert clinical consensus to guide practice barrier product. It is important to recognise the difference
(Wounds UK, 2018; Fletcher et al, 2020), and between emollients (moisturisers) and barrier products, as the
recommendations should ideally be reflected in local skin two are not interchangeable.
care protocols. In the case of IAD, a simple categorisation Barrier products are designed to repel moisture and
tool— the Ghent Global IAD Categorisation Tool protect the skin from the harmful effects of repeated
(GLOBIAD)—has recently been developed and validated exposure to excessive moisture. Basic barrier preparations
(Beeckman et al, 2017). This can be used in conjunction with consist of a lipid/water emulsion base with the addition of
current guidelines to deliver evidence-based practice. metal oxides (such as zinc or titanium), which form a thin
In individuals assessed as being at a high risk of developing layer on the surface of the skin to repel potential irritants.
IAD, preventive measures should be instituted as soon as The more sophisticated ones, often contain a water-repellent,
possible. It has been shown that IAD can occur in susceptible silicone-based ingredient dimethicone, such as Derma
patients within four days of admission to a critical care unit Protective Plus.
© 2021 MA Healthcare Ltd
(Bliss et al, 2011) and more recent work by Phipps et al Unfortunately, there is always the potential for some of
(2019) demonstrated changes in skin barrier function after these ingredients to cause irritation in sensitive individuals,
15 minutes’ exposure to a wet incontinence pad in and this should always be kept in mind, particularly if the
healthy volunteers. skin irritation appears to worsen when using any preparation.
The provision of optimal skin care is one of the most Should this occur, advice should be sought from the relevant
This article was reprinted from the British Journal of Nursing 2021, Vol 30, No 15: TISSUE VIABILITY SUPPLEMENTPRODUCT FOCUS
nurse specialist. and should not be used in infected, incised, deep or
penetrating wounds. The manufacturer also advises against its
Derma Protective Plus Skin Protectant use in cases of serious burns and animal bites.
management and prevention of IAD For product risks, cautions and warnings please refer to
and MASD the patient information leaflet.
The information in this section is from the information Derma Protective Plus is up to 60% cheaper than other
leaflet provided with Derma Protective Plus (Ennogen, leading brands, and could therefore present a significant cost
Dartford). saving to the NHS.
Derma Protective Plus is a new 1% dimethicone skin
barrier product with a uniform, gel-like and sticky Case 1. Skin vulnerable to IAD
consistency, and is non-greasy and less oily than market A 68-year-old woman attended the continence clinic for
competitors. Applied directly to the skin, it provides long- management of recurrent and refractory urinary tract
lasting protection against chafing or further ingress of irritant infections. The patient’s older husband is her sole carer and
urine and faecal materials, afforded by a comfortable and she is a wheelchair user; she uses pads to manage urine
resilient barrier. The main benefits of Derma Protective Plus leakage. For some time, she had been complaining of burning
include the promotion of a healing environment for and irritation of her perinanal skin. In attempt to manage
damaged skin exposed to urine and faecal matter and this, she applied liberal amounts of petroleum jelly daily. The
resistance to further maceration from IAD or persistent patient had also recently developed antibiotic-associated
loose stools. diarrhoea (since hospitalisation for treatment with
For patients at risk of or already experiencing moisture- antibiotics) which increased the frequency of skin wiping
injured skin, the area of concern should be fully and carefully with dry paper.
cleansed with an appropriate cleansing solution. Once the During continence assessment, the patient’s vulnerability
tissue is clean, Derma Protective Plus should be generously to IAD was readily identified. Examination of the skin found
applied by hand in a thicker layer for severely damaged skin redness and inflammation; the skin had remained in
and for more moist environments to enable its superior tissue prolonged contact with urine and there were some scratch
adhesion to provide optimum moisture barrier protection. marks from where the patient had experienced itching.
For prevention, reduce amount used to a thin layer. It may be Thankfully, no erosions were evident but urgent revision of
reapplied as frequently as needed to ensure the integrity of the management plan was required to prevent more invasive
the barrier is maintained; prolonged and consistent skin skin damage. The findings were documented and the patient
contact with the product is safe. and her carer advised regarding a skin care regimen,
Extremely dry skin may also benefit from the regular including the use of Derma Protective Plus in place of
application of Derma Protective Plus as the constituents of petroleum jelly after each toilet visit and after bathing.
dimeticone and polyethylene glycol 3350 also aid vital At 2-week follow-up, the skin was reviewed and the
moisture retention in this indication. inflammation previously noted had disappeared. The patient
Derma Protective Plus is licensed for external use only was no longer experiencing burning and itchiness as the
Derma Protective Plus allowed the continence management
pads to absorb more effectively. As a result, the skin’s integrity
and resilience improved and the risk of incidental abrasions
or moisture-associated damage was minimised.
Case 2. Minor/early IAD
An 87-year-old woman who was obese, confined to bed and
experiencing urinary incontinence was exhibiting signs of
self-neglect and refusing to accept personal care. She
complained of burning in skin clefts and around her vulva.
She felt she had thrush but, on examination, her skin was
seen to be inflamed from contact with urine, the leakage of
which she managed with bathroom towels within the bed.
She also had intertrigo in the groin folds. The patient had
been applying Sudocrem to the areas of skin soreness she
could reach, but these areas had not improved.
The patient was fully counselled regarding the long-term
risks to skin integrity from leaving incontinence unmanaged
with the concomitant consequences including hospital
© 2021 MA Healthcare Ltd
admission for treatment. Once she had understood that she
would be vulnerable to wound infection that would require
more intense and regular intervention, the patient agreed to
skin cleansing and treatment of skin folds with antifungal
Derma Protective Plus ointment. A continence assessment was undertaken and a
This article was reprinted from the British Journal of Nursing 2021, Vol 30, No 15: TISSUE VIABILITY SUPPLEMENTPRODUCT FOCUS
management plan initiated with respect to urinary leakage.
Regular application (three times a day) of Derma Protective KEY POINTS
Plus was integrated into the care plan. The reduced the skin ■ Incontinence-associated dermatitis (IAD) presents a significant financial
pH and contact with body fluids, and promoted a healing burden for healthcare systems
environment where the antifungal could work optimally. ■ Prolonged exposure of a patient’s skin to excessive moisture is a major
At continence follow-up at 1, 2 and 4 weeks, the patient’s cause of skin breakdown but is often overlooked
skin had much improved, with better protection against ■ Introducing an effective and long-lasting moisture barrier can help prevent
skin shearing from contact with wet sheets and general damage to skin vulnerable to IAD and moisture-associated skin damage
moisture contact. (MASD)
Immediate application of Derma Protective Plus over
■ Early intervention can stop IAD and MASD occurring or worsening
antifungal treatment is not contraindicated if it is allowed to
dry completely before applying. Good compliance with skin ■ Skin damage from IAD and MASD can be reversed with the incorporation of
management regimen was facilitated by the carers, with an effective moisture barrier into the skin care regimen
obvious positive results. ■ Derma Protective Plus has proven its effectiveness against MASD and IAD
and provides a 60% cost saving to the NHS
Case 3. Moderate damage
A 78-year-old man living independently had a fall in his
home and was brought into ED. During physical assessment, The case studies suggest Derma Protective Plus has
he was found to have overflow incontinence from chronic significant efficacy in retaining moisture within the skin’s
urinary retention. He also clearly had longstanding faecal layers and preventing damage to the skin from contact with
incontinence as his buttocks were widely excoriated with urine and faeces.
focal indurations of faecal involvement of the tissues. Because Other barrier products are available, but their sticky or
of the patient’s neurological and regenerative deficits in greasy consistency can be off-putting to use or seep into
peripheral nerves, he was unaware of the damage to his skin, fabrics. Equally, other skin barrier products have been shown
which had long remained in adverse conditions not to impair the moisture-wicking properties of continence
conducive to healing. management products, which is not the case with Derma
Once admitted to hospital, the patient’s skin was Protective Plus.
comprehensively assessed and found to be moderately Given the large number of patients affected, the
moisture damaged but with no deeper ulcerations or breaks prevention and management of IAD presents a significant
aside from the numerous sore patches where faeces had financial burden for healthcare systems. Therefore, it is
become ingrained. The tissue viability nurse specialist important to use a competitively priced effective product,
thoroughly cleansed the area, removing as much matter as such as Derma Protective Plus. Derma Protective Plus has
possible without undue disruption of the wound matrices. proven its effectiveness against MASD and IAD and provides
Derma Protective Plus was then liberally applied across the a 60% cost saving to the NHS compared with the brand
whole buttock area. A plan was instituted to ensure consistent leader. The product is effective in promoting optimum skin
skin management while on the ward, with particular care integrity in the management of both urinary and
taken not to allow the skin to dry out or further faecal incontinence. BJN
incontinence to remain suboptimally managed. Derma
Protective Plus was applied at each toileting and pad change Declaration of interest:The publication of this article was supported
totalling at least 4 times in 24 hours. by Ennogen
Ten days later, the skin had dramatically improved, with all
areas of faecal ingress expelled gradually from the dermal Ali SM,Yosipovitch G. Skin pH: from basic science to basic skin
layers by virtue of moisture retention. Inflammation had care. Acta Derm Venereol. 2013;93(3):261–277. https://doi.
org/10.2340/00015555-1531
dispelled, there were only very small pink patches where the Beeckman D, Campbell J, Campbell K et al. Incontinence-associated
faecal indurations had been and the overall skin integrity was dermatitis: moving prevention forward. London: Wounds International;
much improved with no further evidence of moisture lesions. 2015. https://tinyurl.com/6uruwak (accesssed 30 June 2021)
Beeckman D,Van den Bussche K, Alves P et al. The Ghent Global IAD
All three cases demonstrated an improvement in the patient’s Categorisation Tool (GLOBIAD). Skin Integrity Research Group, Ghent
skin condition after the product was introduced as part of University; 2017. https://tinyurl.com/fvnnxenm (accessed 30 June 2021)
their skin care regimen. Bliss DZ, Savik K, Thorson MA, Ehman SJ, Lebak K, Beilman G.
Incontinence-associated dermatitis in critically ill adults: time
to development, severity, and risk factors. J Wound Ostomy
Conclusion Continence Nurs. 2011;38(4):433–445. https://doi.org/10.1097/
WON.0b013e318220b703
The risks of moisture-associated skin damage and Clark M, Semple MJ, Ivins N, Mahoney K, Harding K. National audit of
incontinence-associated dermatitis remain a perennial pressure ulcers and incontinence-associated dermatitis in hospitals across
concern for people with all forms of incontinence. The pain Wales: a cross-sectional study. BMJ Open. 2017;7(8):e015616. https://
© 2021 MA Healthcare Ltd
doi.org/10.1136/bmjopen-2016-015616
and embarrassment of living with these conditions (not to Darlenski R, Kazandjieva J, Tsankov N. Skin barrier function: morphological
mention their costly, time-consuming treatment at the basis and regulatory mechanisms. J Clin Med. 2011;4(1):36–45
Eyerich S, Eyerich K, Traidl-Hoffmann C, Biedermann T. Cutaneous
expense of the NHS) can be avoided or mitigated by barriers and skin immunity: differentiating a connected network. Trends
ensuring evidence-based skin management protocols, which Immunol. 2018;39(4):315–327. https://doi.org/10.1016/j.it.2018.02.004
include the application of a skin-protectant moisture barrier. Fletcher J, Beeckman D, Boyles S et al. International best practice
This article was reprinted from the British Journal of Nursing 2021, Vol 30, No 15: TISSUE VIABILITY SUPPLEMENTPRODUCT FOCUS
recommendations: prevention and management of moisture-associated Continence Nurs. 2019;46(4):315–320. https://doi.org/10.1097/
skin damage (MASD). London: Wounds International. 2020. https:// WON.0000000000000549
tinyurl.com/yjjdhyaa (accessed 30 June 2021) Rawlings AV. Recent advances in skin ‘barrier’ research. J Pharm Pharmacol.
Gray M, Beeckman D, Bliss DZ et al Incontinence-associated dermatitis: a 2010;62(6):671–677. https://doi.org/10.1211/jpp.62.06.0002
comprehensive review and update. J Wound Ostomy Continence Nurs.
Van Damme N, Clays E,Verhaeghe S,Van Hecke A, Beeckman D.
2012;39(1):61–74. https://doi.org/10.1097/WON.0b013e31823fe246
Johansen E, Bakken LN, Duvaland E et al. Incontinence-associated Independent risk factors for the development of incontinence-associated
dermatitis (IAD): prevalence and associated factors in 4 hospitals in dermatitis (category 2) in critically ill patients with fecal incontinence:
southeast Norway. J Wound Ostomy Continence Nurs. 2018;45(6):527– a cross-sectional observational study in 48 ICU units. Int J Nurs Stud.
531. https://doi.org/10.1097/WON.0000000000000480 2018;81:30–39. https://doi.org/10.1016/j.ijnurstu.2018.01.014
Koudounas S, Bader DL,Voegeli D. Knowledge gaps in the etiology and Voegeli D. Moisture-associated skin damage: aetiology, prevention and
pathophysiology of incontinence-associated dermatitis: a scoping review. treatment. Br J Nurs. 2012;21(9):517–521. https://doi.org/10.12968/
J Wound Ostomy Continence Nurs. 2020;47(4):388–395. https://doi. bjon.2012.21.9.517
org/10.1097/WON.0000000000000656 Voegeli D. Prevention and management of moisture-associated skin damage.
Newman D, Preston A, Salazar S. Moisture control, urinary and faecal Nurs Stand. 2019;34(2):77–82. https://doi.org/10.7748/ns.2019.e11314
incontinence, and perineal skin management. In: Krasner D., Rodeheaver Warner RR, Stone KJ, Boissy YL. Hydration disrupts human stratum
G, Sibbald R (eds). Chronic wound care: a clinical source book for corneum ultrastructure. J Invest Dermatol. 2003;120(2):275–284.
healthcare professionals. 4th edn. Malvern: HMP Communications; 2007: https://doi.org/10.1046/j.1523-1747.2003.12046.x
609–627
Woo KY, Beeckman D, Chakravarthy D. Management of moisture-associated
NHS Business Service Authority. Prescription Cost Analysis – England
2020/21. 2021. https://www.nhsbsa.nhs.uk/statistical-collections/ skin damage: a scoping review. Adv Skin Wound Care. 2017;30(11):494–
prescription-cost-analysis-england/prescription-cost-analysis-england- 501. https://doi.org/10.1097/01.ASW.0000525627.54569.da
202021(accessed 13 July 2021) Wounds UK. Best practice statement: maintaining skin integrity. London:
Phipps L, Gray M, Call E. Time of onset to changes in skin condition Wounds UK. 2018. https://tinyurl.com/tyu29jyc (accessed 30
during exposure to synthetic urine: a prospective study. J Wound Ostomy June 2021)
CPD reflective questions
■ What practices do you use to help prevent skin damage from incontinence in the patients for whom you care?
■ Do you educate your patients regarding skin damage from incontinence?
■ Do you know and understand the properties of the products you use and recommend for your patients?
© 2021 MA Healthcare Ltd
This article was reprinted from the British Journal of Nursing 2021, Vol 30, No 15: TISSUE VIABILITY SUPPLEMENTYou can also read