PRISE EN CHARGE DE L'INFECTION A HELICOBACTER PYLORI : LES RECOMMANDATIONS INTERNATIONALES SONT-ELLES APPLICABLES EN AFRIQUE ?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PRISE EN CHARGE DE L’INFECTION A
HELICOBACTER PYLORI : LES
RECOMMANDATIONS INTERNATIONALES
SONT-ELLES APPLICABLES EN AFRIQUE ?
Dr Ruffin NTOUNDA,
•
CHU Saint-Pierre, Bruxelles
Belgian Hp and microbiota Study Group (BHpMSG)
Journées Scientifiques de la SCGE
Yaoundé, Octobre 2019
Barry J. Marshall et
La découverte de H. pylori par Marshall et Warren J. Robin Warren, Prix
en 1982 a bouleversé cette conception et a fait de Nobel 2005 de médecine
l'ulcère gastroduodénal une maladie
essentiellement infectieuse...
! sérendipité !
1/ Est- ce qu'il faut eradiquer Helicobacter pylori ? 2/ Les recommandations internationales sont-elles applicables en Afrique ?
Pathogenesis of Helicobacter pylori Infection
- Host immune gene polymorphisms and gastric acid secretion largely determine the bacterium's ability to
colonize a specific gastric niche.
- Bacterial virulence factors such as the cytotoxin-associated gene pathogenicity island-encoded protein
CagA and the vacuolating cytotoxin VacA aid in this colonization of the gastric mucosa and subsequently
seem to modulate the host's immune system
Johannes G. Kusters, Arnoud H. M. van Vliet, and Ernst J. Kuipers Clin Microbiol Rev. 2006 Jul; 19(3): 449–490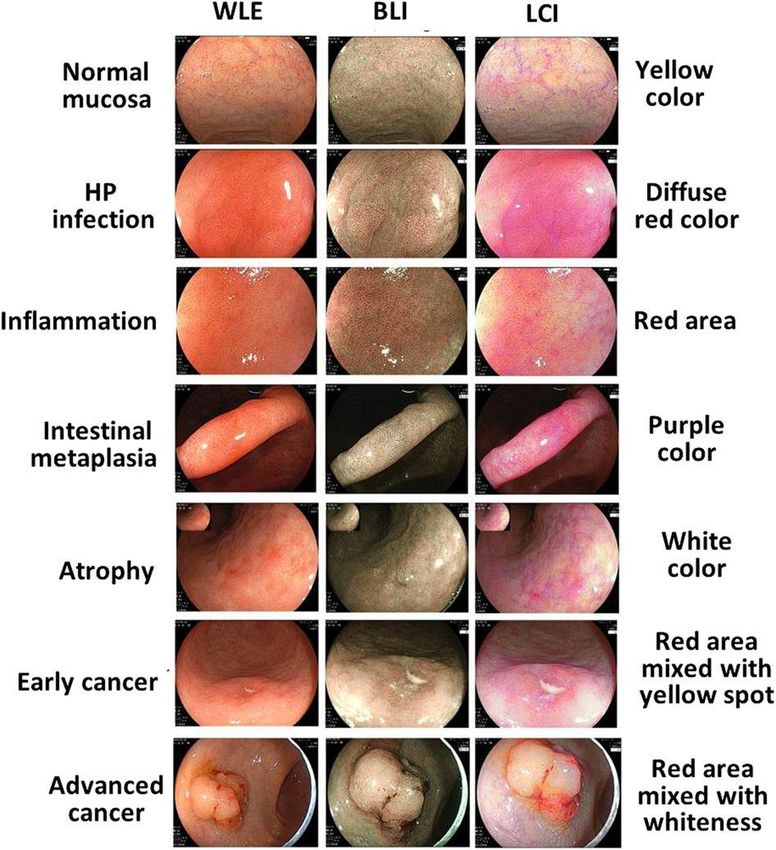
PREVENTION OF GASTRIC CANCER AND OTHER COMPLICATIONS (WORKSHOP 3)
With 4 Guidelines on H pylori, What Should
Clinicians Do Differently?
Since 2015, 4 major Helicobacter pylori consensus documents have been published
❑ American College of Gastroenterology Clinical Guideline
❑ Toronto Consensus
❑ Houston consensus
❑ Maastricht V/Florence Consensus Report (which was updated
from an initial report published in 2012)
David A. Johnson, Medscape Gastroenterology, Aug 29, 2018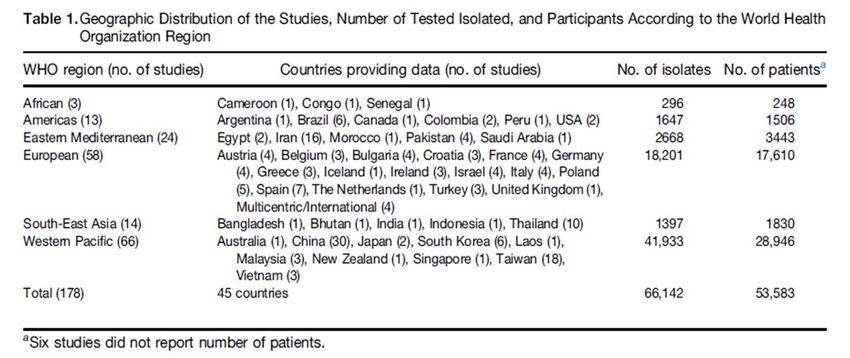
The Maastricht Florence Consensus
1996- Maastricht I- Gut 1997
2000- Maastricht II- APT 2002
2005- Maastricht III-Florence- Gut 2007
2010- Maastricht IV-Florence- Gut 2012
2015 – Maastricht V- Florence- Gut 2016INDICATIONS THERAPEUTIQUES
Helicobacter Pylori Infection
When to Eradicate, How to Diagnose and Treat
Wolfgang Fischbach and Peter Malfertheiner, Dtsch Arztebl Int 2018; 115(25): 429-36Dépistage ciblé
HOUSTON CONSENSUS CONFERENCE ON TESTING FOR
HELICOBACTER PYLORI INFECTION IN THE UNITED STATES
Recommandation 7:
Tester et rechercher Hp chez les immigrants de première
génération (prévalence élevée d’infection )
(82% sont d'accord / tout à fait d’accord, Grade 1B).
Recommandation 8:
Les latino-américains et Les afro-américains peuvent être
testés en raison du taux élevé de l’infection à Hp dans ces
groupes
(91% d’accord / tout à fait d’accord, Grade 2C).
HASHEM B. EL-SERAG, JOHN Y. KAO, FASIHA , AL.
Clinical Gastroenterology and Hepatology 2018;16:992–1002HOUSTON CONSENSUS CONFERENCE ON TESTING FOR
HELICOBACTER PYLORI INFECTION IN THE UNITED STATES
Recommandation 11:
Tester les membres de la famille vivant dans le même foyer
que des patients dont l’infection est activement prouvée
(experts versus sondage: 91% contre 78% sont d’accord / tout à fait d'accord, avis d’expert 1B)
Recommandation 12:
Tester Hp chez des patients avec ATCD familiaux d’ulcère
peptique
(experts versus sondage: 91% contre (73%) d'accord / tout à fait d'accord, avis d’expert 1B) .
HASHEM B. EL-SERAG, JOHN Y. KAO, FASIHA , AL.
Clinical Gastroenterology and Hepatology 2018;16:992–1002HOUSTON CONSENSUS CONFERENCE ON TESTING FOR
HELICOBACTER PYLORI INFECTION IN THE UNITED STATES
Recommandation 14:
Tester H pylori chez les patients traités par des médicaments
dont l'absorption peut être affectée par l’infection (par exemple
L-DOPA, thyroxine)
(experts versus enquête 63% vs 68% d’accord / tout à fait d’accord, niveau d’experts 2C)
HASHEM B. EL-SERAG, JOHN Y. KAO, FASIHA , AL.
Clinical Gastroenterology and Hepatology 2018;16:992–1002Colm O’Morain
Summary of the main studies performed from 1993
à 2002 evaluating the impact of H. pylori eradication on the
regression of low grade gastric MALT lymphoma
Author Year N. Patients %
remission
Wotherspoon,al 1993 6 83
Bayerdörffer, al 1995 33 69
Roggero, al. 1996 25
Accumulated data 1993-2002 604 72,8%60
Fischbach, al. 1995 15 93
Montalban, al. 1996 9 88
Pinotti, al. 1997 45 68
En 2010: 32 séries
Neubauer, al. 1997 publiés, 50
1271 cas 80
Nobre-Leitao, al. 1997 17 100
Steinbach, al. 1998 28 50
Thiede, al. 1999 84 81
Fischbach, al. 2000 36 89Gastric Malt Lymphoma Stage IE-IIE
Hp positive Hp neg or
t (11;18 ) or undertermined Hp pos with t (11;18 )
Hp eradication therapy with Antibiotic resistant or
Standard antibiotics and PPI regimen
No lymphoma response
t repeat EGD 2-3 months
after eradication therap ry
Hp test at 2-3 months and
2nd ligne antibiotic regimen if Hp detected Repeat
EGD and biopsies at 3-6 months Antibiotic resistant
After Hp eradicationGastric Malt Lymphoma Stage IE-IIE
After Hp eradication
Neg. for lymphoma Pos. for residual Pos. lymphoma , symptomatic
Lymphoma, asymptomatic or with other treat.
indications - overt
progression
- deep invasion
- nodal invasion
- t (11;18) translocation
EGD and biopsy EGD and biopsy Radiotherapy
Every 6 months for 2 years Every3- 6 months
Then every 12-18 months Chlorambucil or other alkylants
and or rituximab when
radiotherapy is not feasible or not
indicatedGastric Malt Lymphoma, stade IV
Hp eradication therapy with standard antibiotics and PPI regimen
if the infection is present
Asymptomatic lymphoma Smptomatic lymphoma or
with other treatment indications:
- overt progression
- bulky disease
- Impending organ damage
Wait and see with EGD and
biopsies and EUS/ 6 months - patient preference
Additional imaging if clinically
indicated bone marrow biopsy if Chemotherapy and/or Rituximab
clinical indicated
Consider enrollment in clinical trialTests Diagnostiques
Diagnostic tests for the detection of H,pylori
infection: Non invasive
Test Se(%) Sp(%) Advantages Disadvantages
Serology 76-84 79-90 Widely available, inexpensive Positive result may reflect previous
rather than current infection, not useful
after treatment
UBT >95 >95 High negative and positive False-negative results possible in the
predictive values, presence of PPI or with recent use of
useful before and after antibiotics of bismuth preparations,
treatment consederable resources and personnel
required to perform test
Stool 96 97 High negative and positive Process of stool collection may be
antigen predictive values distasteful to patient, false-negative
test Useful before and after results possible in the presence of PPI
treatment or with recent use of antibiotics or
bismuth preparationsDiagnostic tests for the detection of H,pylori
infection: Invasive
Test Se(%) Sp(%) Advantages Disadvantages
Histology 95 99 Excellent sens, and Sp, Expensive ( endoscopy and
especially with special and histopathology costs), interobserver
immune stains, provides variability, accuracy affected by PPIs
additionnal information about and antibiotics use, requires trained
gastric mucosa personnel
Rapid 90 93 Rapid results, accurate in Requires endoscopy, less accurate after
Urease patients not using PPIs or treatment or in patients using PPIs
test antibiotics, no added
histopathology cost
Culture 58,1 100 Sp 100%, allows antibiotics Variable sensitivity: requires trained
sensitivity testing staff and properly equipped facilities,
expensive
PCR ?Colm O’Morain
Colm O’Morain
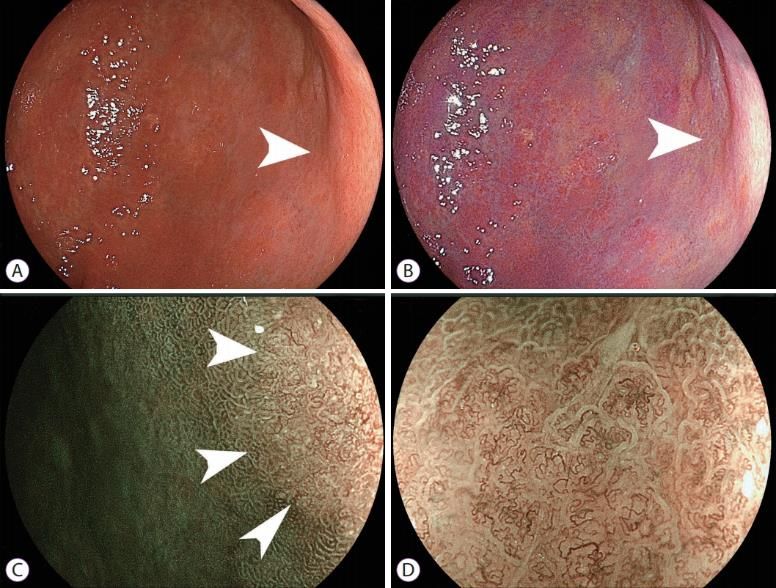
Artificial intelligence diagnosis of Helicobacter pylori infection
using blue laser imaging-bright and linked color imaging: a
single-center prospective study
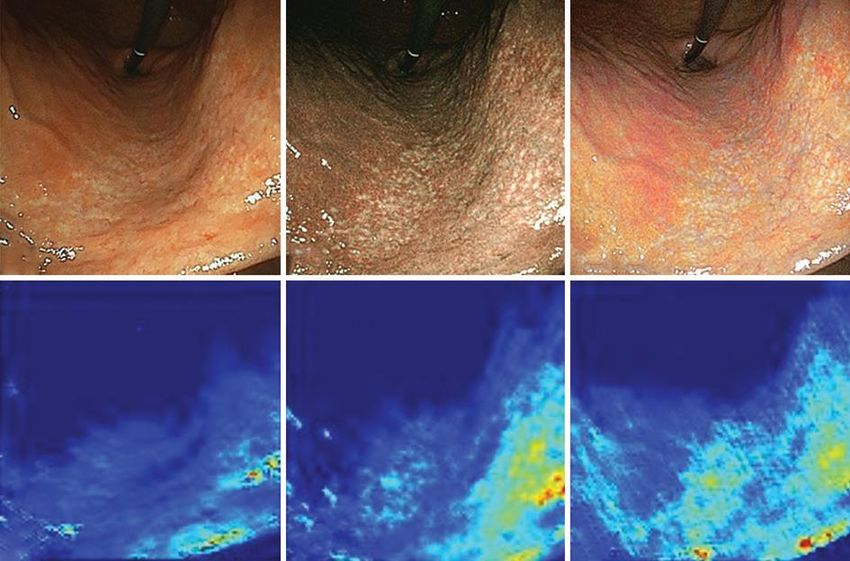
Feature maps of the AI corresponding to the endoscopic images. Endoscopic images of a H. pylori-positive subject (test group). An image in WLI of EGD (A) shows
yellowish mucosa in the lesser curvature (lower part of the picture). An image in BLI-bright (B) shows small whitish spots scattered over the mucosal surface (region
between the central part and the lower right part of the picture). An image in LCI (C) shows a pale-white color change in the same area. Feature maps of convolutional
layers during the AI test are also shown for WLI (D), BLI-bright (E) and LCI (F). In each IEE image, the AI responded to the lesser curvature of the stomach, which was the
region of mucosal atrophy with intestinal metaplasia, indicated by a light green or a light blue color
AI, artificial intelligence; WLI, white light imaging; BLI, blue laser imaging; LCI, linked color imaging; H. pylori, Helicobacter pylori
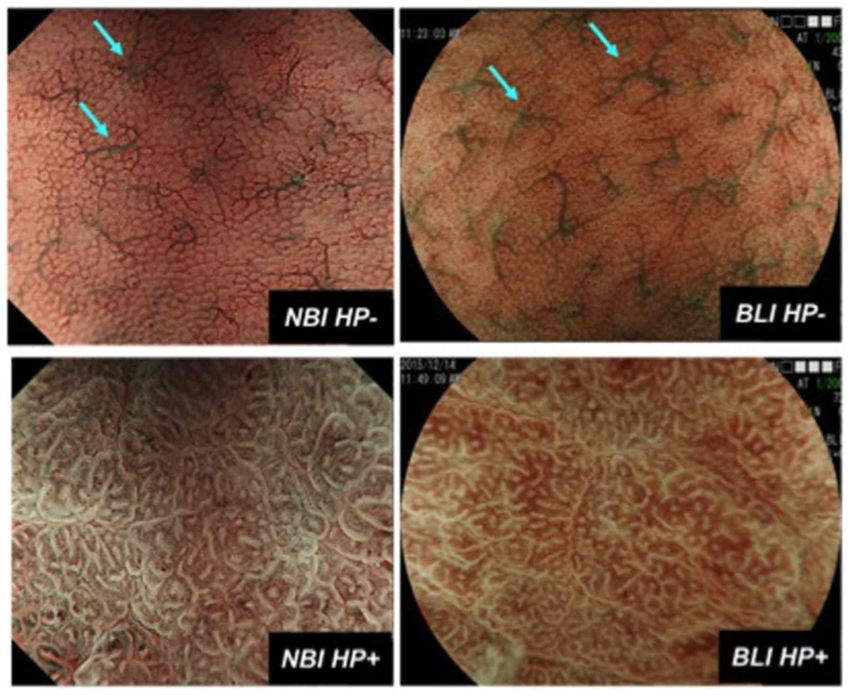
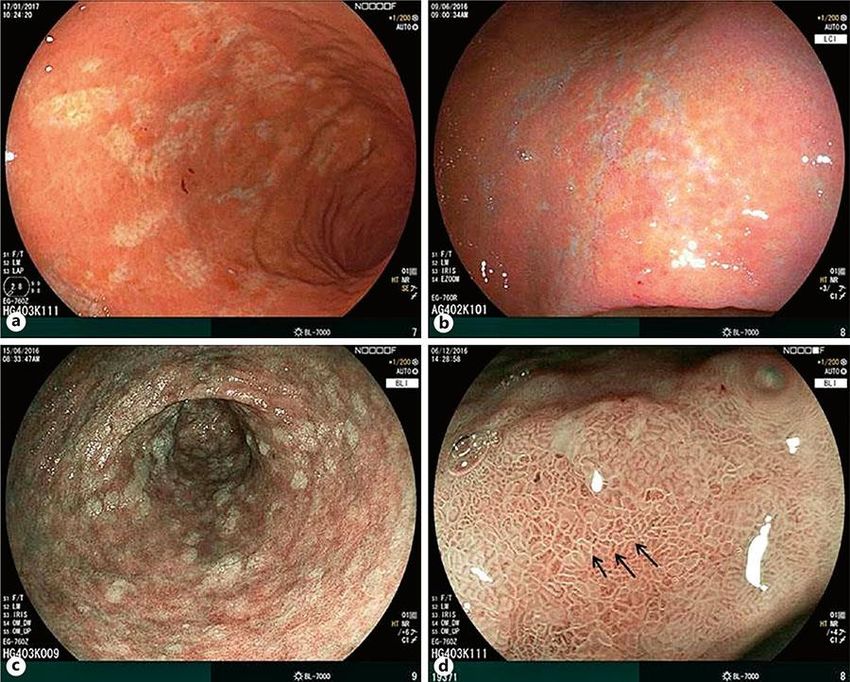
Hirotaka Nakashimaa , al,Annals of Gastroenterology (2018) 31, 1-7Image enhanced endoscopy. (A) Narrow band imaging (NBI) of the gastric mucosa. Round homogeneous sized pits with regularly arranged collecting venules are shown (left). This pattern (regular arrangement of collecting venules) named ‘RAC’ pattern in the corpus mucosa highly indicates a Helicobacter pylori negative state. In the H. pylori-infected mucosa with inflammation, pit patterns are elongated, varied in sizes and shapes with spaces between them. Collecting venules are obscured owing to inflammation (centre). When intestinal metaplasia develops, the pit pattern is further elongated with light blue lines (light blue crest sign) decorating the pits margins (right). The images were provided by Dr Kazuyoshi Yagi. (B) Blue laser imaging (BLI) of the gastric mucosa. BLI is a new modality of image enhancement. The BLI- bright mode can easily obtain lower magnification images, similar to the NBI images in (A) (left). With BLI-magnification mode, further mucosal details including periglandular capillary networks (red coloured circles surrounding the pits) are seen (centre). BLI endoscopy is useful for identifying the area of intestinal metaplasia where greenish coloured elongated pit patterns predominate (right). The images were provided by Dr Hiroyuki Osawa, Jichi Medical University.
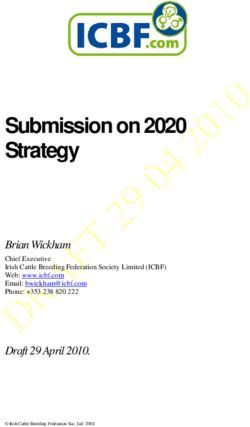
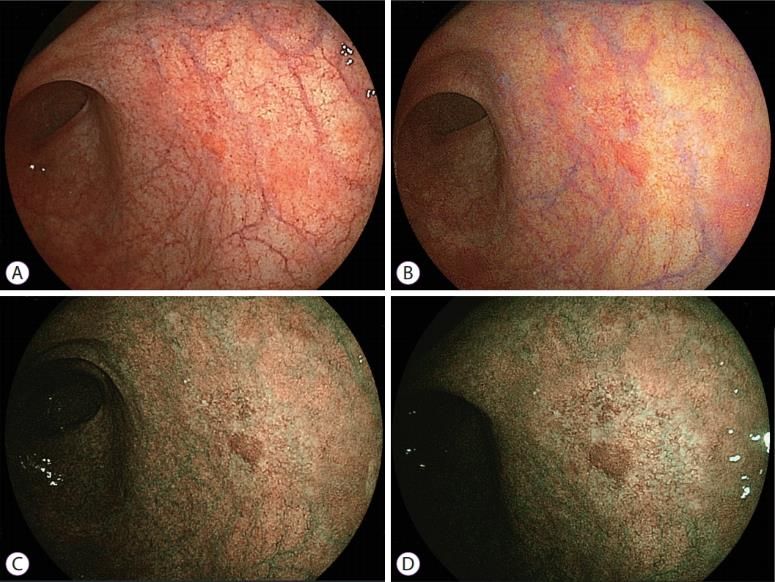
Magnifying NBI (left) and BLI (right) features of Hp infection negative (Hp−, upper) and positive (Hp+, lower) gastric mucosa. Hp− gastric mucosa is characterized as small, round pits, accompanied with regular honeycomb-like SECNs, being regularly interspersed with collecting venules (light blue arrow). On the other hand, Hp+ gastric mucosa is characterized as enlarged or elongated pits with unclear SECNs or dense fine irregular vessels. NBI, narrow-band imaging; BLI, blue laser imaging; Hp, Helicobacter pylori; SECNs, subepithelial capillary networks.
Typical images for gastric pathology using MLI. a, b Same patient, (c, d) different patients. a Overview image of CG with larger areas of mucosal atrophy with a yellow appearance in white light. b Mucosal atrophy at the lesser curvature using LCI atrophy appears white and deeper vascular structures can be visualized. c Patchy distribution of IM in the antrum appearing as white areas in BLI mode. d Magnification of angulus revealing light blue crest sign (arrows) as a sign of IM.
A) White light imaging with a small-caliber endoscope shows a small red area measuring 3 mm in diameter on the posterior wall near the gastric angle, which is not suspicious for gastric cancer. (B) Linked color imaging enhances the red lesion and the surrounding red portion. (C) Bright blue laser imaging reveals a discolored lesion measuring 10 mm around a central red area. (D) Blue laser imaging produces a high color contrast between the malignant lesion and the surrounding mucosa. Several irregular vessels are seen in the discolored lesion even with small-caliber endoscopy, suggesting early gastric cancer.
Esophagogastroduodenoscopy (EGD) is of growing importance in the diagnosis of Helicobacter pylori (H. pylori) gastritis, Image-enhanced endoscopy (IEE) with magnifying function is useful for improving the diagnosis of H. pylori infection. H• The AI demonstrated an excellent ability to diagnose H. pylori infection using the novel IEEs AI technology with IEE is likely to become a useful image diagnostic tool for H. pylori infection Hirotaka Nakashimaa , al,Annals of Gastroenterology (2018) 31, 1-7
Gisbert JP, EHMSG , Magdeburg 2016
Gisbert JP, EHMSG , Magdeburg 2016
Traitement empirique de l'infection à Hp en France
après Maastricht V
Quadritherapie Bismuthée 10j ou Concomitant au moins 10j
1e Ligne
Echec Echec
2e Ligne Concomitant 14j Q. Bismuthée 10j
Echec Echec
Culture ou PCR
Trithérapie optimisée en fonction
3e Ligne De la sensibilité à la Clari et Aux
quinolones
- Clari-S : IPP-Amoxi-Clari 14 jours (Amoxi 1gx3)
- Clari-R et Quinolones-S : IPP-Amoxi-Levo 14j
JD de Korwin. JFHOD 2016
- Clari-R et Quinolones-R : IPP-Amoxi-Metro 14jUpdated German Guidelines 2016
Risk factors for clarithromycin Fischbach W et al. Z Gastroenterol 2016;54:327-63
resistance
- Geographical background
- Prior macrolide exposure
- Femal gender
Low risk of Clari-R High risk of Clari-R
1st Line STT
days)(14
or days better than 7 Bismuth
therapy orquadruple
Bismuth quadruple therapy Concomitant quadrupleThe Toronto Consensus Carlo A Fallone, al. Gastroenterology 2016;151:51–69
Evidence-based Treatment Regimens for H. pylori Infection in
North America, Listed in Recommended Order
Sheila E. Crowe, N Engl J Med 2019;380:1158-65SCHEMAS THERAPEUTIQUES et RESULTATS
Triple therapy when Hp infection is known to
be susceptible to clarithromycin
•PPI x2
•Amoxi (1g) x2
•Clari (500mg) x2
(or Tini or Metro (500mg) x2)
For 10 days, preferably 14 daysTraitement Hp en 2019: Triple therapie standard
Low Clari-R
Pays Type trait Tx d'éradication Auteurs, Année
Japon Controlé: Metro vs Clari Metro: 98% Mabe K, 2018
Clari: 60%
Rwanda Controlé: Metro:64% Kabakambira JD, 2018
Metro vs Clari vs Cipro Clari: 87%
Cipro: 81%
Turquie Meta Analyse: Durée 7j vs 14j 57% vs 60% Sezgin O, 2019
Chine Controlé: Triple vs Bismuth Triple 7j: 79% Leow AH, 2018
triple 14j;89=%
Bismuth 7j: 82%
Inde Controlé: standard vs “ Daily 86% vs 90% Shahbazi S, 2018
Single-dose triple (meilleure
compliance)
O'Connor et al. Helicobacter 2019Sequential therapy
• PPI + Amoxi (1g) x2 for 5 days
followed by
• PPI +Clari (500mg) + Tini (500mg) or
Metro (500mg) x2 for a further 5 days
( Total 10 days)Concomitant therapy
• PPI +
• Amoxicillin (1g) +
• Clarithromycin (500mg) +
• Tinidazole or Metro (500mg)
Twice daily for 10-14 daysSequential - Concomitant therapy
or Hybrid
PPI +Amoxicillin (1g) x2 for 7 days
Followed by
PPI, Amoxi (1g), Clari(500mg) and Tini
or Metro (500mg) for a further 7 days
( Total 14 days)Traitement Hp en 2019
Quadruple: concomitant, Sequentiel, Hybrid
Pays Type trait Tx d'éradication Auteurs, Année
Meta-analyse, Conc. vs Conc 5-10 j > Triple 7-1à j Chen MJ, 2018
triple Mais Conc = Triple 14j
23 études controlées
N=6632
Hybrid bénéfice du sequentiel +
conco; mais compliance
mauvaise
Taiman Etude controlée Reverse -Hybrid 96% HSU PL, 2018
N=352 Q. Bismuth= idem
Espagne Cross selected selectional Conco 98% Macias Garcia,2019
Bismuth 94%
Rescue 3è ligne Résistant Huang HT, 2018
Conco 14j - Clari-R:79%
- Levo-R: 95%
- Metro-R: 67%
Non resistant: 81%Bismuth quadruple therapy •PPI x2 •Bismuth x4 (subsalicylate or subcitrate) •Tetracycline hydrochloride (500mg) x4 with meals and at bedtime (bismuth and TTC) •Tinidazole or Metro (500mg) x3 with meal (for 10 days, or preferaly 14 days) Alternatives: • Pylera + PPI x2 for 10-14 days
The fourth chinese consensus report on the management of H.pylori infection Nonghua Lu ,EHMSG , Magdeburg 2016 Liu Wen Zhong, al. J Digestive Disease 2013;14:211-221
Essais thérapeutiques avec Pylera
(Bismuth, metro, TTC)Traitement Hp en 2019: Bismuth
Pays Type trait Tx d'éradication Auteurs, Année
Europ N=1141 88% McNicholl AG, 2019
Hp-Eurog 1è ligne
Italie N=500 Seq= 91% Fiorini, 2018
Pylera= 92%
Chine controlé Avec Bismuth=85% Long X, 2018
Sans Bismuth= 64%
O'Connor et al. Helicobacter 2019Real-Word studies of Bismuth-based
quadruple regimens
Study Zagari Agudo-Fernandez
Country Italy Spain
Number 376 185
1st line (%) 91,4 78,2
2nd line(%) 87,5 85,3
3rd line (%) 91,7 61,3
Adverse Events(%) 32,4 3,8
Abondoned(%) 6,1 4,9
O'Connor et al. Helicobacter 2019Fluoroquinolone therapy when Hp infection is
known to be susceptible to fluoroquinolones
•PPI x2
•Amoxi (1g) x2
•Fluoroquinolone (Levo 500mg) x1
(or x2)
For 10-14 daysTraitement Hp en 2019: Levofloxacine
Pays Type trait Tx d'éradication Auteurs, Année
Iran Controlé Seq 10j: 78% Hajiani E, 2018
Conco 14j: 83%
Mexico Controlé Levo triple:63% Ladron-e-Guevara,2018
Stand triple:58%
Pakistan Controlé Levo 14j: 92% Latif S, 2018
N=300 Stand: 87%
Italie Levo avec lactoferine:96% Ciccaglione, 2019
+/- lactoferine Sans lactoferine: 75%
O'Connor et al. Helicobacter 2019Rifabutin triple therapy • PPI x2 + • Rifabutin (150mg) x2 + • Amoxicillin (1g) x2 ( Total 14 days)
Review article: rifabutin in the treatment of
refractory Helicobacter pylori infection
J. P. Gisbert,X. CalvetAliment Pharmacol Ther 2012; 35: 209–221One randomized trial showed that regimens with
rifabutin were effective rescue therapies in
patients with treatment failure who had H. pylori
infection that was resistant to both
metronidazole and clarithromycin
Perri F, Festa V, Clemente R, et al. Am J Gastroenterol 2001; 96: 58-62.Traitement Hp en 2019: Probiotics
Pays Type trait Tx d'éradication Auteurs, Année
Espagne Standard vs Concomitant Placebo= 95% McNicholl AG.2018
+ Lacobacillus vs Placebo Probiotics=97%
N=209
By MetaAnalyse - ↑ Eradication Dore MP.2019
Chinese 40 etudes - ↓ Effet II
Group 8924 patients
O'Connor et al. Helicobacter 2019Vonoprazan
The First-in-Class Potassium-
Competitive Acid Blocker,
(Vonoprazan Fumarate)
Kawashima K, al. Dig Liver Dis. 2016Eradication rate of Vonoprazan VPZ triple
therapy (1wk)
VAC or LAC triple
Murakami K et al. Gut 2016; 65: 1439-46Traitement Hp en 2019: Vonoprazan
- N= 1355, 1stline
Standard 86%
Voroprazan Triple 97% erad
- MetaAnalyse, 5 studies, 1599 patients
Clari-S: Vonoprazan triple = Standard triple: 95% vs 93%
Clari-R: Vonoprazan triple ≠ Standard triple: 82% vs 40%
Mori N, al.Biomed Rep. 2018
Li M, al. Helicobacter. 2018Helicobacter Pylori: New Therapies
❑ Bromopyruvate ( anticancereux)
❑ Goshuyuto ( Herbicide): Japon
❑ Lactoferrine bovine 10 mg/ml
❑ Dual therapy > concomitant ( Taiwan)
- IPP+ Amoxi high dose
Yang X, al.Medicine (Baltimore) 2019
Sue S, al. J Gastroenterol Hepatol 2019DISCUSSION
Evolution of primary resistance of H.pylori to Clarithromycin,
Metronidazole and Fluoroquinolones in Brussels, Belgium
Macrolides (10.5% to 18%), VERONIQUE Y MIENDJE DEYI; M'Kinansoi S Lare, Alain
Nitro-imidazoles (28% to 40%) Burette; Ruffin NTOUNDA; Samy Cadranel; Okyay ELKILIC,
PATRICK BONTEMS; Marie HALLIN,
Fluoroquinolones (12.4% to 22.8%) Diagn Microbiol Infect Dis. 2019 Jul 30:114875Hp resisance to antibiotics in the studies published
during the last year worldwide
Author N Region AMO% CLA% Met% Quin% TTc% Rif% Fur%
Liu 1117 China 3,4 22,1 78,2 19,2 1,9 1,5 -
Forini 1424 Italy 0,06 35,9 40,2 29,3 - - 0,06
Bashir 270 Algeria 5,2 29,7 46,7 17,2-17,9 2,6 - -
Lopo 2194 Portugal 0,1 42 25 9-18 0,2 - -
Gonzalez- 191 Chile - 31,2 - 14,1 - - -
Hormazabal
Mosites 800 USA - 28,8 42,8 45-58,7 - - -
Saniee 218 Iran 27,1 34,4 79,4 27,9 38,5 - 23,9
Khien 2318 Vietnam 15 34,1 69,4 - 17,9 - -
Kageyama 208 Japan 13 48 49 - - - -
Zhang 144 China - 70 - 6 - - -
Pinkowska 170 Poland - 46 56 39,2 - - -
Lee 74 S-Korea 6,7 31 41,8 - - -
O'Connor et al. Helicobacter 2019Pan- European Registry on H. pylori management (Hp- EuReg):
interim analysis of 16 600 first- line treatments
A. G. McNicholl et al. Helicobacter 2018Pan- European Registry on H. pylori management
(Hp- EuReg): interim analysis of 16 600 first- line treatments
❑ La gestion de l'infection à Hp par les gastro-
entérologues européens est hétérogène, sous-
optimale et souvent en contradiction avec les
recommandations actuelles.
❑ Seuls les quadruple-therapies d'une durée d'au
moins 10 jours peuvent atteindre un taux
d'éradication supérieur à 90 %.
A. G. McNicholl et al. Helicobacter 2018A recent observational study showed that only 35% of patients who had been treated for H. pylori infection underwent follow-up testing to confirm eradication and that many patients who had treatment failure were retreated with the same regimen Rubin J, Lai A, Al.Gastroenterology 2018; 154: S503-S504.
Epidémiologie de l’infection à Helicobacter Pylori à Yaoundé :
de la particularité à l’énigme Africaine
171 sujets symptomatiques.
Test rapide à l'uréase kit commercial Pronto Dry®
La prévalence Hp 72,5% (124/171)
H.pylori était de 63,0% pour l'ulcère duodénal,
50% pour l'ulcère gastrique et
100% pour le cancer gastrique.
Conclusion: la prévalence de l'infection à H.pylori au Cameroun est très élevée et
significativement liée à l'âge de moins de 40 ans.
Firmin Ankouane Andoulo, Dominique Noah Noah,&, Michèle Tagni-Sartre3,
Elie Claude Ndjitoyap Ndam, Katleen Ngu Blackett
Pan African Medical Journal. 2013 16:115Molecular detection of Hp and its antimicrobial
resistance in Brazzaville, Congo
•Hp prevalence :
89 %
Antibiotics Resistance (%)
Clarithromycin 1,7
Tetracycline 2,5
Quinolone 50
•Ontsira Ngoyi EN, al. Helicobacter. 2015 Aug;20(4):316-20Profil de resistance aux antibiotiques de l’Hp dans la région
du Sud-Kivu : Resultats préliminaires d’une étude
monocentrique
• 58 patients (Dl Abd), Age moyen=39 ans homme=60 %
• Biopsies stockées à -18° (Kivu), puis congelées à -70 °(BXL)
• 23 souches ( 1 souche morte, 5 souches contaminées)
Antibiotique Tx Resistance (%)
Amoxicilline 0
Tetracycline 0
Clarithromycine 8,9
Levofloxacine 75
Metronidazole 100
Natmako S, Nteranya O, Mwengte J, Van Gossum M, Miendje Y, 2016.Resistance Primaire en Algerie
Clarithromycine Metronidazole
Boucekkine Mouffok Djennane- LARH
Hadibi 2003 2013 2008
2015
37%
12,5% 12% 33%
Boucekkine T,al. 2003
Mouffok F, al.Saidal santé Fev 2013
Djennane-Hadibi F,al. Microbiol drug Resistance 2015•Reza Ghotaslou, al, World J Methodol,2015 Sep 26;5(3):164-174
Prevalence of Antibiotic Resistance in Helicobacter pylori:
A Systematic Review and Meta-analysis in World Health
Organization Regions
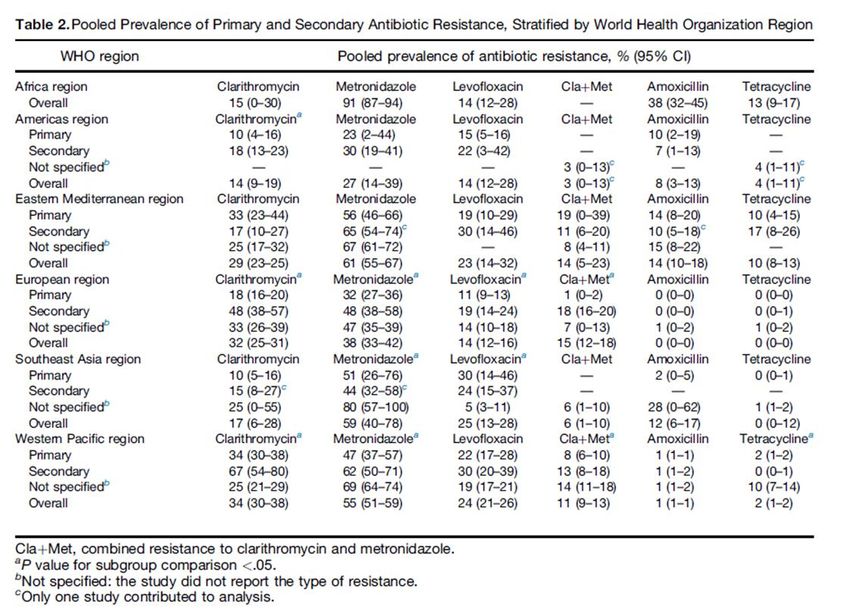
Alessia Savoldi, Elena Carrara, David Y. Graham, Michela Conti, and Evelina Tacconelli. Gastroenterology 2018;155:1372–1382Prevalence of Antibiotic Resistance in Helicobacter pylori:
A Systematic Review and Meta-analysis in World Health
Organization Regions
Alessia Savoldi, Elena Carrara, David Y. Graham, Michela Conti, and Evelina Tacconelli. Gastroenterology 2018;155:1372–1382Prevalence of Antibiotic Resistance in Helicobacter pylori:
A Systematic Review and Meta-analysis in World Health
Organization Regions
Alessia Savoldi, Elena Carrara, David Y. Graham, Michela Conti, and Evelina Tacconelli. Gastroenterology 2018;155:1372–1382Prevalence of Antibiotic Resistance in Helicobacter pylori:
A Systematic Review and Meta-analysis in World Health
Organization Regions
Alessia Savoldi, Elena Carrara, David Y. Graham, Michela Conti, and Evelina Tacconelli. Gastroenterology 2018;155:1372–1382Efficacy of Helicobacter pylori eradication regimens
in Rwanda: a randomized controlled trial
JD Kabakambira, al.BMC Gastroenterol. 2018; 18: 134.Efficacy of Helicobacter pylori eradication regimens
in Rwanda: a randomized controlled trial
- Coûts, efficacité et profil d'innocuité documentés dans cette
étude; => utiliser clarithromycine et des thérapies combinées à
base de ciprofloxacine pour l'éradication de H. pylori au Rwanda.
- Métronidazole à base de la trithérapie est inférieure et mauvais
choix parmi les quatre schémas thérapeutiques étudiés.
JD Kabakambira, al,BMC Gastroenterol. 2018; 18: 134.Classification de OLGA et OLGIM: impacts de
facteurs ethniques, démographiques et
environnementaux
Afr. sub-saharienne: Hp elevé, moins d'ulcus et cancer
< type de souche, facteurs immunitaires, génétiques, diététiques
G1: Patient europeens (680) G2= centre africain (250)
- Pas de différence significative sur la sévérité des gastrites
- Role de l'Hp et l'âge dans la sévérité, mais pas de facteurs
geographiques
- Lésions endoscopiques significatives: 27% G1 et G2
Van Gossum M, al. JFHOD 2020Images obtained with a normal-caliber endoscope: (A) white light imaging and (B) linked color imaging cannot clearly reveal the site of the
early gastric cancer (white arrows) because of the tangential view. (C) Blue laser imaging with middle magnification shows a brown
malignant lesion surrounded by green mucosa (white arrows). (D) Blue laser imaging using high magnification shows irregular
microvascular and irregular microstructural patterns on the mucosal surfacePimentel-Nunes Pedro et al. MAPS II … Endoscopy 2019; 51: 365–388
•Facteurs à retenir lors du choix d’un traitement éradicateur Hp •WGO Global Guideline Hp in developing countries, 2010
Niveau de ressources à disposition et options
diagnostiques
•WGO Global Guideline Hp in developing countries, 2010•Prevalence of antibiotic resistance in Hp:
A recent literature review
Reza Ghotaslou, al, World J Methodol,2015 Sep 26;5(3):164-174Contrôle d’éradication ❑ Au plus tôt 4 semaines après la fin du traitement. ❑ Lorsque l'endoscopie n'est pas nécessaire, seul le BTU ou le test à l'antigène fécal est acceptable. ❑ Le bismuth et les ATB doivent être arrêtés pendant 28 j et les IPP pendant 14 j avant le BTU ❑ Le HpSAg fécal ne devrait pas être effectué moins de 4 sem ( de préférence 8 à 12 sem) après le traitement.
Conclusion I - Helicobacter pylori est carcinogene de classe 4, son éradication ne laisse aucun doute dans les inications bien précises - Les recommandations internationales offrent actuellement plusieurs possibilités de prise en charge qui peuvent s'appliquer partout dans le monde - La zone Afrique, particulièrement la zone sub-saharienne soufre beaucoup du manque de moyens diagnostiques et therapeutiques, mais les resultats des études publiées, certes peu nombreux, montrent que ces recommandations sont bien adaptables
Conclusion II - Afr. sub-saharienne: Hp elevé, moins d'ulcus et cancer < type de souche, facteurs immunitaires, génétiques, diététiques - L'endoscopie diagnostique fait de grands progrès. est ce que l'intelligence artificielle est l'avenir ? Celà reste à demontrer et difficile à généraliser - Le consensus Brésilien par exemple recommande encore les schemas à base de Clarithromycine malgré Clari-R> 15% car Bismuth non disponible - Levofloxacin, Sitafloxacin, Furazolidone, Rifabutine restent interessants en “Rescue”
« Tant que les lions n'auront pas leurs propres historiens, les histoires de chasse ne peuvent que chanter la gloire du chasseur ».
You can also read