Recent Developments in Federal and State Regulation of Private Health Insurance
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Recent Developments in
Federal and State Regulation
of Private Health Insurance
By: Jessica Sharpe Breanna Patterson
Committee Staff Administrator Legislative Committee Analyst
Banking and Insurance Banking and Insurance
Legislative Research Commission Legislative Research Commission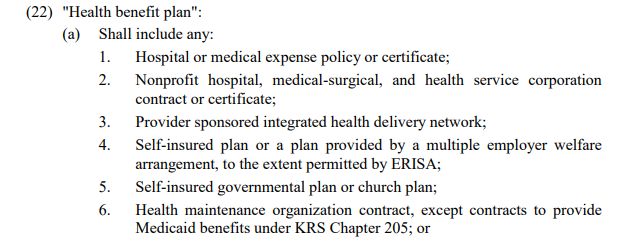
What We Do
Assist legislators in:
Drafting legislation; and
Obtaining information relating to banking and
insurance issues
Staff the General Assembly’s Banking and
Insurance committees
Important Disclaimer Any views expressed in this presentation are the views of the presenters alone and do not necessarily reflect the views of the Legislative Research Commission.
Presentation Overview
Health Insurance Generally
State and Federal Regulation of Private Health
Insurance
Legislative Update
Kentucky
Selected Federal
Note: For purposes of this presentation,
Selected Caselaw Update private health insurance does not include
Medicaid, CHIP, Medicare, TRICARE, the
state employee health plan, or Workers’
CompensationRegulation of Health Insurance Generally
What is health insurance?
Black’s Law Dictionary (11th ed. 2019):
“Insurance covering medical expenses resulting from sickness or
injury – Also termed accident and health insurance; sickness and
accident insurance”
KRS 304.5-040:
“‘Health insurance’ is insurance of human beings against bodily
injury, disablement, or death by accident or accidental means,
or the expense thereof, or against disablement or expense
resulting from sickness, and every insurance appertaining
thereto.” Note: Always check for definitions.
Seemingly generic terms such as
“insurer” or “health plan” often have
specific meanings for a given
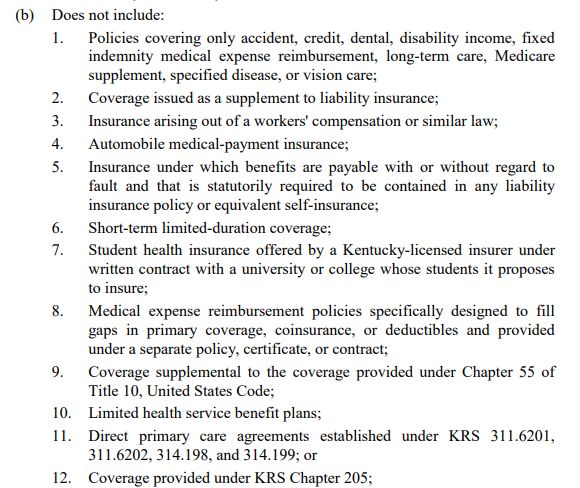
requirement.Are all health insurance plans subject to the
same requirements?
Private health insurance can be categorized in a variety of ways including
but not limited to:
Individual plans Based on the type of insurer offering the
plan:
Group plans
Ex. Health Maintenance Organization (HMO),
Small group
Preferred Provider Organization (PPO), etc.
Large group
Based on the type of coverage:
Employer-sponsored plans
Ex. Comprehensive
Self-funded
Ex. Limited- dental only, vision only, etc.
Fully-insured
Ex. Coverage for a specific procedure or
condition
Private health insurance is sometimes regulated based on how the insurer/insurance is
categorized and these categories are not always mutually exclusive.Are all health insurance plans subject to the same requirements?
2019 Health Coverage Estimates in Kentucky
Uninsured
Military 6%
1%
Medicare
16%
Employer
47%
Medicaid
26%
Non-group
4%
Employer Non-group Medicaid Medicare Military Uninsured
This chart was created based on data from: Health Insurance Coverage of Total Population, Kaiser Family Foundation (last visited May 14, 2021)
https://www.kff.org/other/state-indicator/total-
population/?currentTimeframe=0&selectedRows=%7B%22states%22:%7B%22kentucky%22:%7B%7D%7D%7D&sortModel=%7B%22colId%22:%22Location%
22,%22sort%22:%22asc%22%7D2019 EMPLOYER-SPONSORED COVERAGE IN THE PRIVATE
SECTOR IN KENTUCKY
Self-insured Fully-insured
Fully-insured
37%
Self-insured
63%
This chart was created based on data from: https://meps.ahrq.gov/data_stats/summ_tables/insr/state/series_2/2019/tiib2b1.htm (Last visited
June 1, 2021)State and Federal Regulation of
Private Health InsuranceState Constitutional Power “Under its police power and as the creator of the corporation, or its permission to do domestic business, as the case may be, the state may prescribe terms and conditions on which an insurance company may do business.” Kenton & Campbell Benev. Burial Association v. Goodpaster, 304 Ky. 233, 239-240 (1946)
Kentucky
health
insurance
laws
Note: Some statutes outside the
insurance code may also be applicable
to private health insurance.Kentucky Health Insurance Laws (cont.)
KRS Chapter 304:
Subtitle 12- trade practices and frauds
Subtitle 14- contains contract requirements and laws relating to
Medicare supplement insurance, long-term care insurance, &
short-term nursing home insurance
Subtitle 17- applies to individual plans (see KRS 304.17-020)
Subtitle 17A- generally applies to health benefit plans
Subtitle 17C- generally applies to limited health service benefit
plans
Subtitle 18- applies to group and blanket health insurance (see KRS
304.18-070)
Subtitle 32- generally applies to non-profit hospital, medical-
surgical, dental and health service corporations & self-insured
employer plans
Subtitle 38- generally applies to health maintenance organizationsKentucky Health Insurance Laws (cont.)
Kentucky law includes a variety of requirements
for health insurance, including:
Coverage mandates- examples include:
Ex.
Diabetes treatment (KRS 304.17A-138), emergency medical
conditions (KRS 304.17A-580), colorectal cancer screenings
(KRS 304.17A-257)
Mandates can differ based upon the market (group or
individual) and the scope of insurance (comprehensive or
limited)Kentucky Health Insurance Laws (cont.)
Mandates were once duplicated in each subtitle to which
the mandate applied.
Ex. Coverage for treatment for mental illness. KRS 304.17-318;
304.18-036; 304.32-165; 304.38-193.
In recent years, mandates have primarily been enacted in
KRS Ch. 304.17A, applying to “health benefit plans”
Ex. Coverage for autism spectrum disorder KRS 304.17A-142Kentucky Health Insurance Laws (cont.)
Regulatory Requirements
Licensing, examination, and review of policies, rates, financial stability,
and trade practices by the Department of Insurance
See generally, KRS Ch. 304.2, 304.3, 304.6, 304.7, 304.8, 304.12, 304.13,
304.17A
Disclosure and Contracting Requirements
For insureds
Ex. Provider directories (KRS 304.17A-254, 510), internal and external appeal
rights when claims are denied (KRS 304.17.600 to 633)
For health care providers contracting with insurers
Ex. Notice of proposed material changes to contract (KRS 304.17A-235),
Prohibition of certain gag clauses (KRS 304.17A-164, 254, 530), timely payment
of claims (KRS 304.17A-700 to 730)“Health benefit plan”- KRS 304.17A-005(22)
Federal Constitutional Power “No commercial enterprise of any kind which conducts it activities across state lines has been held to be wholly beyond the regulatory power of Congress under the Commerce Clause. We cannot make an exception for the business of insurance.” U.S. v. South-Eastern Underwriters Association, 322 U.S. 533, 553 (1944).
The McCarran Ferguson Act
Enacted in reaction to decision in U.S. v. South-
Eastern Underwriters Association, 322 U.S. 533 (1944)
Provides that the business of insurance shall be
subject to state law (Emphasis added)(15 U.S.C. §
1012(a))
Provides that federal law will not preempt state law
unless the federal law acts specifically on the
business of insurance (15 U.S.C. § 1012(b))
Provides exemption to anti-trust laws for insurance
regulated by state law(15 U.S.C. § 1012(b))
15 U.S.C. § 1013 was recently amended to eliminate exemption for
health insurance (Pub. L. 116-327)
Steven Plitt, Daniel Maldonado, Joshua D. Rogers & Jordan R. Plitt, Couch on Insurance, McCarran-Ferguson Act, generally, §
2.4 (3rd ed. 2020)Federal Health Insurance Laws Since the McCarran Ferguson Act, several federal laws have been enacted to regulate private health insurance. The majority of the laws are located in: The Public Health Service Act, 42 U.S.C. ch. 6A § 201 et. seq.; The Employee Retirement Income Security Act of 1974, 29 U.S.C. ch. 18 § 1001 et. seq.; and The Internal Revenue Code, 26 U.S.C. Bernadette Fernandez, Vanessa C. Forsberg & Ryan J. Rosso, Federal Requirements on Private Health Insurance Plans, Congressional Research Service (last visited May 14, 2021) https://fas.org/sgp/crs/misc/R45146.pdf
Employee Retirement Income Security
Act of 1974 (ERISA)
Establishes standards for employee retirement and
welfare benefit plans in the private sector
“Employee welfare benefit plan” is defined in 29
U.S.C. § 1002(1)
Includes “any plan, fund, or program… established or
maintained by an employer or by an employee
organization, or by both, to the extent that such plan,
fund, or program was established or is maintained for the
purpose of providing for its participants or their
beneficiaries, through the purchase of insurance or
otherwise, (A) medical, surgical, or hospital care or
benefits or benefits in the event of sickness, accident,
disability….”Employee Retirement Income Security Act of
1974 (ERISA) See Ky. Ass’n of Health Plans, Inc.
v. Miller, 538 U.S. 329 (2003)
General Savings Clause Deemer Clause
Preemption 29 U.S.C § 29 U.S.C. §
29 U.S.C. § 1144(b)(2)(A) 1144(b)(2)(B)
1144(a)
“Our interpretation of the deemer clause makes clear
Note: There is a significant amount that if a plan is insured, a State may regulate it
of case law interpreting these indirectly through regulation of its insurer and its
provisions and the scope of ERISA insurer's insurance contracts; if the plan is uninsured
preemption. [self-funded], the State may not regulate it.” FMC Corp
v. Holliday, 498 U.S. 52, 64 (1990)Employee Retirement Income Security Act of 1974 (ERISA) “Thus, ERISA preempts state laws that (1) ‘mandate employee benefit structures or their administration;’ (2) provide ‘alternate enforcement mechanisms;’ or (3) ‘bind employers or plan administrators to particular choices or preclude uniform administrative practice, thereby functioning as a regulation of an ERISA plan itself.’” Penny/Ohlmann/Nieman, Inc. v. Miami Valley Pension Corp., 399 F.3d 692 (6th Cir. 2005)(internal quotation omitted)
Patient Protection and Affordable Care
Act (ACA)
Applies to almost all health insurers, including self-insured
ERISA plans
Requirements can vary based on whether plan is a large group,
small group, individual, “grandfathered”, or “grandmothered”
plan
Some commonly known coverage provisions include:
Prohibition on pre-existing condition exclusions (42 U.S.C. § 300gg-
3)
Requirement for individual & small group plans to cover essential
health benefits (42 U.S.C. § 18022)
Requirement to cover certain preventive services without cost-
sharing (42 U.S.C. § 300gg-13)Patient Protection and Affordable Care
Act (ACA)
Other provisions:
Prohibit lifetime and annual limits on coverage
Guarantee issue and renewability
Rating limitations
Tax penalty for certain employers with 50 or more full-
time employees that do not meet minimum health
coverage requirements
Individual exchanges
Premium tax credits and cost-sharing reductions for qualified
individuals purchasing coverage on the exchanges
Kaiser Family Foundation, Summary of the Affordable Care Act (Last visited June 4th, 2021), https://files.kff.org/attachment/Summary-of-the-
Affordable-Care-ActPatient Protection and Affordable Care
Act (ACA)
Preemption language:
“Nothing in this title shall be construed to preempt any State law that does not
prevent the application of the provisions of this title.”
42 U.S.C. § 18041(d)
“Subject to paragraph (2) and except as provided in subsection (b), this part, part
D, and part C insofar as it relates to this part or part D shall not be construed to
supersede any provision of State law which establishes, implements, or continues in
effect any standard or requirement solely relating to health insurance issuers in
connection with individual or group health insurance coverage except to the extent
that such standard or requirement prevents the application of a requirement of this
part or part D.”
42 U.S.C. § 300gg-23(a)
“Subject to subsection (b), nothing in this part (or part C insofar as it applies to this
part) shall be construed to prevent a State from establishing, implementing, or
continuing in effect standards and requirements unless such standards and
requirements prevent the application of a requirement of this part.”
42 U.S.C. § 300gg-62(a)Other federal laws concerning health insurance: Consolidated Omnibus Budget Reconciliation Act (COBRA) Health Insurance Portability and Accountability Act of 1996 (HIPAA) Mental Health Parity and Addiction Equity Act of 2008 Note: This list is not (MHPAEA) intended to be The Genetic Information Nondiscrimination Act of 2008 exhaustive. (GINA) Newborns’ and Mothers’ Health Protection Act of 1996 (NMHPA) Womens’ Health and Cancer Rights Act of 1998 (WHCRA) Various provisions of the Internal Revenue Code contained in 26 U.S.C. Subtitle K
Federal Regulation of Private Health
Insurance- Recap
Congress’ Commerce Clause powers can apply to the business
of insurance.
Congress, through the McCarran Ferguson Act, has given
states general authority to regulate insurance except when it
acts specifically with regard to insurance, such as in the case
of ERISA and the ACA.
Under ERISA, states can be preempted from regulating self-
insured employer sponsored plans.
Under the ACA, states are generally permitted to regulate
health insurance except to the extent that state law would
prevent the application of the ACA.Legislative Updates
KentuckyNote: Please consult the legislation and any other relevant authority to determine the effective date of any legislation or of specific provisions within legislation as the effective dates may vary.
HB 48: AN ACT relating to reimbursement for Defines “insurer”
pharmacist services. for purposes of
Section 1 of the
bill
Requires insurers to reimburse a pharmacist for a service or procedure at a
rate not less than that provided to other non-physician practitioners if the
service or procedure:
Is within the scope of the practice of pharmacy;
Would otherwise be covered if provided by a physician, advanced practice registered
nurse, or a physician assistant; and
Is performed by the pharmacist in strict compliance with laws and administrative
regulations related to the pharmacist’s license.
2021 Ky. Acts Ch. 30 sec. 1
Requires all insurers transacting health insurance in the state to use uniform
claims forms for pharmacy services and procedures
2021 Ky. Acts Ch. 30 sec. 2
Applies to Kentucky Access, the state employee health plan, and workers’
compensation.
2021 Ky. Acts Ch. 30 sec. 4, 5, 6Compare to 42
HB 50: AN ACT relating to mental health U.S.C. § 300gg-26;
26 U.S.C. § 9816; 29
parity. U.S.C. § 1185a
(MHPAEA)
Prohibits health benefit plans that provide coverage for treatment of
a mental health condition from imposing:
A nonquantitative treatment limitation (NQTL) for mental health
condition benefits that does not apply to medical and surgical
benefits in the same classification; and
Medical necessity criteria or an NQTL for mental health condition
benefits unless… any processes, strategies, evidentiary standards,
or other factors used in applying the criteria or limitation… are
comparable to, and are applied no more stringently than, the
processes, strategies, evidentiary standards, or other factors used
in applying the criteria or limitation to medical and surgical
benefits in the same classification
2021 Ky. Acts ch. 15 sec. 2HB 50: AN ACT relating to mental health
parity.
Requires NQTL provisions to be construed to require, at a minimum, compliance
with the requirements for NQTL set forth in the Mental Health Parity and Addiction
Equity Act of 2008, 42 U.S.C. § 300gg-26, as amended, and any related federal
regulations
2021 Ky. Acts Ch. 15 sec. 2
Requires insurers to submit an annual report to the Department of Insurance
regarding the insurer’s compliance with mental health parity requirements (Similar
to 42 U.S.C. § 300gg-26)
2021 Ky. Acts Ch. 15 sec. 2
Eliminates exemptions in Kentucky’s current mental health parity law (KRS 304.17A-
660 to KRS 304.17A-669) for:
Individual health benefit plans
Employer-organized associations as defined in KRS 304.17A-005
2021 Ky. Acts Ch. 15 sec. 3HB 95: AN ACT relating to prescription
insulin.
Requires health benefit plans to limit cost sharing for
a covered prescription insulin drug to $30 per 30-day
supply of each drug regardless of the amount or type
of insulin needed to meet the covered person’s insulin
needs.
2021 Ky. Acts ch. 75 sec. 1
Exempts self-insured governmental plans other than
the state employee health plan
2021 Ky. Acts ch. 75 sec. 1HB 140: AN ACT relating to telehealth.
Amends existing telehealth coverage mandate in KRS
304.17A-138:
Utilizes a new definition of telehealth
Requirescoverage of telehealth services provided by a
home health agency
Requires an originating site reimbursement to rural
health clinics, federally qualified health centers, and
federally qualified center look-alikes when certain
conditions are met
2021 Ky. Acts ch. 67 sec. 10HB 140: AN ACT relating to telehealth.
Requires covered telehealth services to meet all clinical, technology, and
medical coding guidelines for participant safety and appropriate delivery
of services as established by the DOI or the provider’s professional
licensure board
Requires reimbursement for telehealth services provided by a provider
licensed in another state if allowed under a recognized interstate
compact
Requires reimbursement of rural health clinic, federally qualified health
clinics, and federally qualified health center look-alikes for covered
telehealth services regardless of whether the provider was on the
premises
Permits health benefit plans to utilize audits for medical coding accuracy
in the review of telehealth services specific to audio-only encounters
Encourages providers and home health agencies to use audio-only
encounters as a mode of delivering telehealth services when no other
approved mode of delivering telehealth services is available
2021 Ky. Acts ch. 67 sec. 10HB 140: AN ACT relating to telehealth.
Requires certain agencies promulgating administrative
regulations relating to telehealth to:
Use terminology consistent with the glossary of
telehealth terms established by CHFS
Comply with minimum requirements for telehealth
established by CHFS
Comply with other requirements and limitations set
forth in Act
State agencies subject to provisions include Department
of Insurance, Cabinet for Health and Family Services
(includes the Department for Medicaid Services), and
professional licensure boards.
2021 Ky. Acts ch. 67 sec. 3SB 44: AN ACT relating to access to Similar to 45 C.F.R. §
156.1250, except
health care. adds certain non-
profit entities
Requires health benefit plans to accept, and count towards the insured’s
contributions to any applicable premium or cost-sharing requirement,
premium and cost-sharing payments made on behalf of an insured from the
following:
A state or federal government program, including payments made by programs
operating in accordance with the Ryan White HIV/Aids Program
An Indian tribe, tribal organization, or urban Indian organization
A program conducted by an organization that certifies that the organization is:
Exempt from taxation under 26 U.S.C. sec. 501(a), as amended;
Described in 26 U.S.C. sec. 170(b)(1)(A)(i) to (vi); and
Operating in compliance with applicable federal laws, including the False Claims Act, 31
U.S.C. secs. 3729 to 3733.
2021 Ky. Acts ch. 133 sec. 1SB 44: AN ACT relating to access to
health care.
Exceptions:
If the application of the requirements would be the sole cause of a health
benefit plan’s failure to qualify as a high deductible health plan under 26
U.S.C. § 223, then the provision does not apply until the minimum
deductible has been satisfied.
Does not apply to payments from nonprofit organizations referenced
under Section 1(2)(c) of the bill that receive funding in any form from a
health care provider as defined in KRS 304.17A-005.
Expressly permits health benefit plans, to the extent permitted by
federal law, to accept, and count towards the insured’s contributions
to any applicable premium or cost-sharing requirement, premium and
cost-sharing payments made on behalf of an insured from any person
not referenced in the bill.
2021 Ky. Acts ch. 133 sec. 1SB 45: AN ACT relating to prescription Defines “health plan” for
purposes of Section 1 of
drugs. the bill
Prohibits insurers of health plans from excluding cost-sharing
amounts paid by an insured or on behalf of an insured by another
person for a prescription drug when calculating an insured’s
contribution to any cost-sharing requirement
Prohibition does not apply to prescription drugs in which there is
a generic alternative, unless the insured has obtained access to
the brand prescription drug through prior authorization, step
therapy protocol, or the insurer’s exceptions and appeals process
Exempts the state employee health plan
2021 Ky. Acts ch. 134 sec. 1SB 51: AN ACT relating to addiction “Prospective review” &
“concurrent review”
treatment. are defined in
KRS 304.17A-600
Prohibits health benefit plans from requiring or
conducting a prospective or concurrent review for a
prescription drug:
That:
Is used in the treatment of alcohol or opioid use disorder; and
Contains Methadone, Buprenorphine, or Naltrexone; or
That was approved before January 1, 2022, by the U.S. Food
and Drug Administration for the mitigation of opioid
withdrawal symptoms
2021 Ky. Acts ch. 201 sec. 1SB 51: AN ACT relating to addiction
treatment.
Requires insurers to report annually to the Commissioner of the
Department of Insurance (DOI), for claims made during the
preceding plan year, the number and type of providers that have
prescribed medication for addiction treatment to its insureds in
conjunction with and not in conjunction with behavioral therapy
2021 Ky. Acts ch. 201 sec. 3
DOI is required to report to the General Assembly, State Board of
Medical Licensure, and the Kentucky Board of Nursing concerning
the information reported to the Commissioner.
2021 Ky. Acts ch. 201 sec. 3SB 51: AN ACT relating to addiction
treatment.
Requires a treating facility to, prior to discharging a patient
that has received medication for addiction treatment, submit a
written discharge plan to the patient and a patient’s third-party
payor, if any, describing arrangements for additional services
needed following discharge.
2021 Ky. Acts ch. 201 sec. 5
Bill also contained sections relating to the review of medication
for addiction treatment under Medicaid
2021 Ky. Acts ch. 201 sec. 2, 4, 5, 6SB 154: AN ACT relating to home health
care and declaring an emergency.
Amends existing coverage mandates for home health care to
include home health care prescribed and supervised by an
advanced practice registered nurse or physician assistant
2021 Ky. Acts ch. 59 sec. 2, 3, 4, 5
Amends existing coverage mandates to permit an advanced
practice registered nurse or physician assistant to certify that
hospitalization or confinement in a skilled nursing facility would
be required if home health care was not provided
2021 Ky. Acts ch. 59 sec. 2, 3, 4, 5Legislative Updates
FederalNote: Please consult the legislation and any other relevant authority to determine the effective date of any legislation or of specific provisions within legislation as the effective dates may vary.
H.R. 133: Consolidated Appropriations
Act of 2021
Division
BB- Private Health Insurance and
Public Health Provisions
Title I: No Surprises Act
Title II: Transparency
Title III: Public Health ProvisionsH.R. 133: Consolidated Appropriations
Act of 2021: No Surprises Act
Applies to almost all health insurers, including self-insured ERISA plans
Some provisions apply to grandfathered plans (See 42 U.S.C. 18011(a)(5))
Requires coverage for the following services, without regard to whether
the provider/facility is a participating provider:
Emergency services (if the plan covers services in an emergency department
or independent free-standing emergency department)
Covered nonemergency services at a participating facility, if certain notice
and consent criteria are not met by the provider
Covered air ambulance services
Sets forth requirements for initial reimbursement to providers
Allows independent dispute resolution process to dispute initial
reimbursement
Pub. L. 116-260; 42 U.S.C. § 300gg-111; 42 U.S.C. § 300gg-112 ; 26 U.S.C. § 9816; 26 U.S.C. §
9817; 29 U.S.C. § 1185e; 29 U.S.C. § 1185f.Prohibition applies
H.R. 133: Consolidated Appropriations to “ancillary
services” regardless
Act of 2021: No Surprises Act of notice/consent
criteria
Prohibits providers from balance billing for covered services (except
nonemergency services when notice and consent criteria have been satisfied)
Provider can bill for applicable cost-sharing
Pub. L. 116-260; 42 U.S.C. § 300gg-131 (emergency services);
Pub. L. 116-260 42 U.S.C. § 300gg-132 (nonemergency
services)
Requires the following information on physical or electronic plan or insurance
identification cards:
Plan deductibles
Out-of-pocket maximum limitations
Consumer assistance telephone number
Consumer assistance website address
Pub. L. 116-260; 42 U.S.C. § 300gg-111(e);
26 U.S.C. § 9816(e); 29 U.S.C. § 1185e(e)H.R. 133: Consolidated Appropriations
Act of 2021: No Surprises Act
Requires an advanced explanation of benefits for items or
services to be provided, including but not limited to the
provider’s network status, good-faith estimates of what the
plan will pay, and good-faith estimates of the insured’s cost-
sharing.
Pub. L. 116-260; 42 U.S.C. § 300gg-111(f);
26 U.S.C. § 9816(f); 29 U.S.C. 1185e(f)
Compare to:
KRS 304.17A-527(1)(b);
Sets forth requirements relating to continuity of care with KRS 304.17A-643
respect to changes in provider network status.
Pub. L. 116-260; 42 U.S.C. § 300gg-113; 26
U.S.C. § 9818; 29 U.S.C. § 1185gH.R. 133: Consolidated Appropriations
Act of 2021: No Surprises Act
If designation of a primary care provider is required, plans are required Compare to
KRS 304.17A-520
to allow the designation of any participating primary care provider
available to accept the insured
Pub. L. 116-260; 42 U.S.C. § 300gg-117(a);
26 U.S.C. § 9822(a); 29 U.S.C. § 1185k(a)
If designation of a primary care provider is required for child, plans are
required to allow the designation of a participating provider that is a
physician specializing in pediatrics as the child’s primary care provider
Pub. L. 116-260; 42 U.S.C. § 300gg-117(b);
26 U.S.C. § 9822(b); 29 U.S.C. § 1185k(b)H.R. 133: Consolidated Appropriations
Act of 2021: No Surprises Act
If designation of a primary care provider is required and the
plan provides coverage for obstetric or gynecologic care, plans
are prohibited from requiring authorization or referrals for
participating providers specializing in obstetrics or gynecology
Pub. L. 116-260 ; 42 U.S.C. § 300gg-
117(c); 26 U.S.C. § 9822(c); 29 U.S.C. §
1185k(c)
Requires plans to maintain a database, verification process, and
response protocol relating to network-status of providers
Pub. L. 116-260; 42 U.S.C. § 300gg-115;
26 U.S.C. § 9820; 29 U.S.C. § 1185iH.R. 133: Consolidated Appropriations
Act of 2021: Transparency
Requires price comparison guidance by telephone and
access to an online price comparison tool
Pub. L. 116-260; 42 U.S.C. § 300gg-114;
26 U.S.C. § 9819; 29 U.S.C. § 1185h
Prohibits entering into agreements with providers that
impose certain restrictions on the disclosure of specified
information, including price and quality information
Pub. L. 116-260; 42 U.S.C. § 300gg-119;
26 U.S.C. § 9824; 29 U.S.C. § 1185mH.R. 133: Consolidated Appropriations
Act of 2021: Transparency
Establishes reporting requirements with respect to
pharmacy benefits and drug costs
Pub. L. 116-260; 42 U.S.C. § 300gg-120;
26 U.S.C. § 9825; 29 U.S.C. § 1185n
Requires plans to perform, document, and in certain Compare to 21 RS
HB 50
circumstances submit, comparative analyses of the design
and application of NQTLs
Pub. L. 116-260; 42 U.S.C. § 300gg-26(a);
26 U.S.C. § 9812(a); 29 U.S.C. § 1185a(a)H.R. 1319: American Rescue Plan Act of
2021
Provides premium assistance for COBRA coverage
Pub. L. 117-2
Temporarily expands access to premium tax credits
Pub. L. 117-2; 26 U.S.C.36B
Temporarily removes requirement to reconcile premium tax
credits
Pub. L. 117-2; 26 U.S.C. 36BH.R. 1418: Competitive Health Insurance
Reform Act of 2020
Amends 15 U.S.C. § 1013 to:
Add the following:
“Nothing contained in this Act shall modify, impair, or supersede the
operation of any of the antitrust laws with respect to the business of
health insurance (including the business of dental insurance and
limited scope dental benefits).”
Specifies activities relating to health insurance that
continue to be exempt from anti-trust laws
Adds a note to the statute relating to new language’s
relationship and applicability to certain aspects of the
Federal Trade Commission Act.
Pub. L. 116-327; 15 U.S.C. § 1013Selected Caselaw Updates
Rutledge v. Pharmaceutical Care Management
Association, 141 S. Ct. 474 (2020)
In
2015, the Arkansas legislature passed Act 900
regulating pharmacy benefit managers by:
Requiring “PBMs to tether reimbursement rates to
pharmacies’ acquisition costs” Id. at 479.
Requiring PBMs to “provide administrative appeal
procedures for pharmacies to challenge MAC reimbursement
prices that are below the pharmacies’ acquisition costs” Id.
Permitting “a pharmacy to decline to sell a drug to a
beneficiary if the relevant PBM reimburses the pharmacy at
less than its acquisition cost” Id.Rutledge v. Pharmaceutical Care Management
Association, 141 S. Ct. 474 (2020)
Issue: “Whether the Employee Retirement Income
Security Act of 1974 (ERISA), 88 Stat. 829, as amended, 29
U.S.C. § 1001 et. seq., pre-empts Act 900.” Id. at 487.
Holding: Act 900 had “neither an impermissible
connection with nor reference to ERISA and is therefore
not pre-empted.” Id.
“In sum, Act 900 amounts to cost regulation that does not
bear an impermissible connection with or reference to
ERISA.” Id. at 483.California v. Texas, 19-840, 19-1019,
consolidated
Pending challenge to the Affordable Care Act, U.S.
Supreme Court heard oral arguments on November 10,
2020.
The 2017 Tax Cuts and Jobs Act (TCJA) zeroed out the
shared responsibility payment for the individual mandate
to purchase health insurance.
Pending issues include:
1. The constitutionality of the individual mandate in light of
TCJA amendment; and
2. Severability of the remaining provisions of the ACA.
California v. Texas, 945 F.3d 355, (5th Cir. 2020), cert. granted, 140 S.Ct. 1262
(U.S. March 2nd, 2020) (No. 19-840, 19-1019, consolidated)Conclusion
Both state and federal law regulate health
insurance
Many state and federal laws are duplicative or
similar
Federal preemption determination depends on
the language in each law
Updates to state and federal health insurance
laws continue to change the landscape of health
insurance regulationYou can also read