Review Article Antisense oligonucleotides for the treatment of cardiomyopathy in Duchenne muscular dystrophy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Am J Transl Res 2019;11(3):1202-1218
www.ajtr.org /ISSN:1943-8141/AJTR0085739
Review Article
Antisense oligonucleotides for the treatment of
cardiomyopathy in Duchenne muscular dystrophy
Quynh Nguyen1, Toshifumi Yokota1,2
1
Department of Medical Genetics, Faculty of Medicine and Dentistry, University of Alberta, 8812-112 St.,
Edmonton, AB T6G 2H7, Canada; 2The Friends of Garret Cumming Research and Muscular Dystrophy Canada HM
Toupin Neurological Science Research Chair, 8812-112 St., Edmonton, AB T6G 2H7, Canada
Received September 19, 2018; Accepted January 2, 2019; Epub March 15, 2019; Published March 30, 2019
Abstract: Duchenne muscular dystrophy (DMD) is an X-linked recessive fatal neuromuscular disorder characterized
by progressive muscle degeneration which affects one in 3500-5000 males born worldwide. DMD is caused by
loss-of-function mutations in the dystrophin (DMD) gene encoding for dystrophin, a cytoskeletal protein that sup-
ports the structural integrity of myofibers during cycles of muscle contraction and relaxation. DMD patients do not
only experience skeletal muscle deterioration but also severe cardiomyopathy, which is recognized as the current
leading cause of death for the disease. Among the therapies being developed, exon skipping using antisense oligo-
nucleotides (AOs) is one of the most promising approaches. AOs effectively restore dystrophin expression in skeletal
muscles; however, they are highly inefficient in the heart due to endosomal entrapment. Improving skeletal muscle
function without restoring dystrophin expression in cardiac tissue may exacerbate cardiomyopathy due to increased
voluntary activity. This review consolidates the preclinical antisense approaches to improve dystrophin restoration,
with a special focus on the heart.
Keywords: Duchenne muscular dystrophy, dystrophin, cardiomyopathy, antisense therapy, morpholinos, drug de-
livery
Introduction damage, patients with DMD have markedly ele-
vated serum levels of creatine kinase (CK), even
Duchenne muscular dystrophy (DMD) is an at birth [11]. Death usually occurs in their 20s
X-linked recessive disorder characterized by due to respiratory or cardiac complications
progressive muscle degeneration [1]. The prev- [11-14].
alence of DMD is estimated to be 1 in 3500-
5000 live male births, making it the most com- DMD is caused by mutations in the DMD gene,
mon lethal neuromuscular disorder [2, 3]. Pa- which encodes a membrane-associated protein
tients with DMD generally stay asymptomatic at called dystrophin. Dystrophin has 4 domains:
birth although they could show signs of delayed an actin-binding N-terminal domain, a rod do-
gross motor development compared to their main consisting of 24 spectrin-like repeat
peers [4-6]. The disease progresses rapidly, motifs for structural flexibility, a cysteine-rich
with muscle weakness and wasting observed domain for facilitating protein-protein interac-
first in the proximal muscles then extending to tion, and a C-terminal domain for binding sarco-
the more distal muscles [7]. Affected boys lemmal proteins [15, 16]. As a member of the
often lose ambulation by the age of 12 and dystrophin-glycoprotein complex (DGC), dystro-
experience multiple organ system dysfunction phin functions to link the actin cytoskeleton of
such as neuromuscular scoliosis, joint contrac- muscle cells to the extracellular matrix, provid-
ture, osteoporosis, restrictive lung disease, ing mechanical support and membrane stabili-
obstructive sleep apnea, cardiomyopathy, and zation during muscle contraction and relaxation
psychological problems [8-10]. The age of cycles [15, 17-20]. In the absence of dystrophin,
onset and the rate of decline are highly variable muscle fibers experience mechanical stress
among patients. Due to continuous muscle and become susceptible to tearing and frag-Antisense therapy for DMD cardiomyopathy
mentation, resulting in degeneration [21, 22]. has been pushed into the late 20s [12, 13].
Other studies have suggested that dystrophin Since respiratory dysfunction is now better
also serves non-mechanical roles [23]. managed, cardiomyopathy is presently the lea-
ding cause of death among DMD patients.
The DMD gene is located on the short arm of Cardiomyopathy is estimated to present in 25%
the X chromosome (Xp21.3-p21.2) spanning of patients at the age of 6, and 59% of patients
2.4 Mb with 79 exons which produces a 14 kb at the age of 10 [27, 46]. The majority of
transcript [24-26]. The DMD gene has 3 main patients will have developed cardiomyopathy
promoters that produce full-length dystrophin by 18 years of age. Recognition of signs and
(M, B, and P), with other promoters responsible symptoms of cardiac dysfunction can be chal-
for the transcription of different, smaller iso- lenging since DMD patients are usually wheel-
forms [27, 28]. The M promoter produces the chair-bound and do not perform increased car-
Dp427m isoform which is expressed in cardiac diac workload [47]. The correlation between a
and skeletal muscle, the B promoter produces patient’s genotype and the severity of their car-
the Dp427c isoform which is expressed in neu- diac phenotype remains uncertain [48-52].
rons of the cortex and the Cornu Ammonis (CA)
region of the hippocampus, and the P promoter The earliest clinical signs of cardiomyopathy
produces the Dp427p isoform which is ex- are either decreased systolic function or sinus
pressed in the Purkinje cells of the brain. Other tachycardia, with the latter commonly seen in
shorter isoforms include Dp260 expressed in teenage DMD patients [53, 54]. Sinus tachycar-
the retina, Dp140 expressed in the kidney and dia results in elevated heart rate, which in-
brain, Dp116 expressed in the peripheral creases the workload of the already deteriorat-
nerves and Dp71 which is ubiquitously ex- ing dystrophic myocardium [55-57]. Arrhyth-
pressed [29-33]. mias are a common cardiac involvement in
patients with DMD and are significantly corre-
DMD is considered one of the largest genes in
lated with decreased heart function. App-
the human genome. Furthermore, it is located
roximately 44% of DMD patients show signs of
in a genomic region with high rates of recombi-
arrhythmias [58]. Supraventricular tachycardia
nation [34-36]. Due to its length and location,
(SVT) and ventricular tachycardia (VT) are
DMD is highly susceptible to mutation. Ap-
observed in 10% of individuals with DMD [58].
proximately 60% of DMD cases are due to dele-
Although DMD cardiomyopathy is routinely
tions of one or more exons, ~6% due to duplica-
tions, and the rest due to small insertions/dele- described as dilated cardiomyopathy (DCM),
tions or point mutations [11, 16, 37, 38]. These patients with decreased systolic or diastolic
mutations usually disrupt the reading frame or function do not necessarily show ventricular
introduce a premature stop codon, both of dilation [49, 59, 60]. Additionally, myocardial
which lead to the absence of dystrophin. There fibrosis usually precedes left ventricular dys-
is no significant correlation between mutation function (LVD) [61, 62]. The age of onset and
size and disease severity [39-41]. Most muta- the rate of progression are variable for LVD.
tions that maintain the DMD reading frame pro- However, patients with onset of LVD before 18
duce truncated yet partly functional dystrophin, years of age were found to have a significantly
and often result in a milder form of the disease shorter lifespan compared to those who had
known as Becker muscular dystrophy (BMD) LVD after 18 years old [48]. Other features of
[42-44]. Although the skeletal muscle symp- DMD cardiomyopathy include abnormal cardiac
toms are less severe, the majority of BMD conduction (as caused by, for example, vacuole
patients also develop cardiomyopathy, and it is degeneration in the Purkinje fibers), congestive
the leading cause of death in patients with heart failure and sudden cardiac arrest [27, 28,
BMD [45]. 47, 63-66].
Cardiomyopathy in DMD patients Myocardial issues in DMD patients are unavoid-
able since dystrophin serves the same func-
The life expectancy for patients with DMD used tions in cardiomyocytes as in skeletal muscle
to be less than 20 years of age just two decades cells [67]. In the absence of dystrophin, cardio-
ago. Due to advancements in ventilator support myocytes experience increased structural vul-
and spinal surgery, the average age of mortality nerability and are susceptible to membra-
1203 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
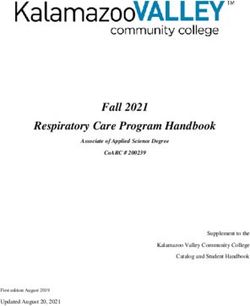
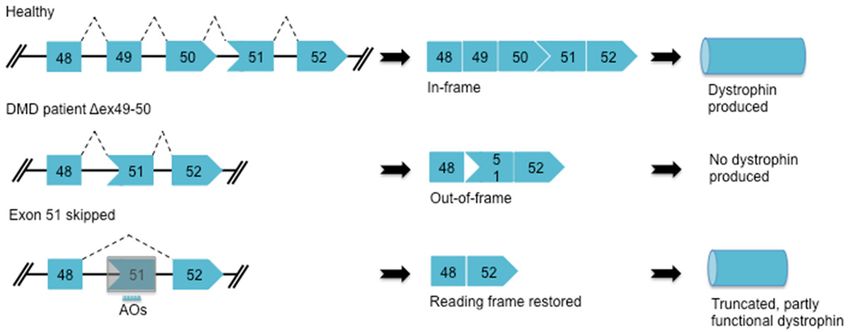
Figure 1. Antisense-induced exon skipping in DMD. Deletion of exon 49 and 50 in the DMD gene creates a frame-
shift mutation which results in a premature stop codon and no dystrophin produced. In the case shown, AOs can
specifically bind to exon 51 and interfere with the splicing machinery to exclude exon 51 from the mature mRNA,
thereby restoring the reading frame and producing truncated but partly functional dystrophin.
ne instability and tearing [22]. Cardiomyocyte other interventions such as ventricular assist
remodeling occurs secondary to myocardial devices (VADs) or cardiac transplantation [9,
wasting, which leads to ventricular enlarge- 47, 82-92]. Treatment with corticosteroids has
ment and fibrosis [68]. As previously men- been shown to improve cardiac function. DMD
tioned, affected hearts do not always show patients who received steroids such as pred-
signs of ventricular dilation. Another conse- nisolone/prednisone or deflazacort had signifi-
quence of myocardial tearing and fragmenta- cantly delayed onset of cardiomyopathy, less
tion is the dysregulation of ion influx/efflux in ventricular dilation and systolic dysfunction
the heart [69, 70]. Notably, damages to the than those who did not. However, patients
myocardial membrane disrupt Ca2+ homeosta- using corticosteroids can experience some
sis. Since Ca2+ acts as a second messenger in long-term complications such as weight gain,
many cellular pathways, Ca2+ dysregulation re- bone fractures, cataracts, etc. [9, 10, 93-96],
sults in multiple downstream abnormalities which limits their use for therapy. ACEIs and
within myocardial tissue. One significant conse- ARBs have proven effective in reducing left ven-
quence of Ca2+ dysregulation includes increa- tricular hypertrophy and fibrosis. Furthermore,
sed reactive oxygen species (ROS) production initiation of beta-adrenergic receptor blocker
and mitochondrial dysfunction. Elevated Ca2+ treatment along with ACEIs has been demon-
levels within cardiomyocytes activate the mito- strated to improve left ventricular systolic func-
chondria to produce ROS which leads to apop- tion in DMD patients [88, 91, 97]. However,
tosis and further muscle wasting [69-79]. An most of these studies have their inherent limi-
important second messenger affected by Ca2+ tations, which makes it challenging for data
dysregulation is nitric oxide (NO) which has interpretation as well as treatment application
roles in blood flow and vasoregulation [80, 81]. in clinical settings.
Increased intracellular Ca2+ concentrations
also enhance the risk of Ca-dependent arrhyth- Antisense oligonucleotides for the treatment
mias and cellular Ca2+ overload in DMD patients of DMD
[69].
At present, there is no cure for DMD. Current
Cardiomyopathy in DMD patients is currently treatments are mostly palliative, aiming at alle-
not curative. Therapies commonly used include: viating the symptoms of the disease [11, 14].
corticosteroids, angiotensin-converting enzyme Several promising approaches have been in-
inhibitors (ACEIs), angiotensin II receptor block- vestigated such as utrophin up-regulation, viral
ers (ARBs), beta-adrenergic receptor blockers, gene therapy, cell-based therapy, antisense oli-
mineralocorticoid receptor antagonists and gonucleotides (AOs) for exon skipping and,
1204 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
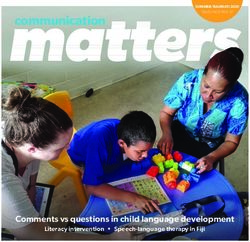
Figure 2. Chemical structures commonly used in antisense therapy. (A) RNA, (B) 2’-OMe-phosphorothioate, (C) Tricy-
clo-DNA, (D) Phosphorodiamidate morpholino oligomers. X or Y can be a peptide; Y can be an octaguanidine moiety
(E) as seen in Vivo-morpholino.
most recently, CRISPR-Cas9-mediated gene sistance to nuclease degradation, but also
editing [69]. In this review, we will discuss the enhance their pharmacological properties. Al-
use of AOs in the treatment of DMD with a spe- terations at the 2’ position of the ribose sugar
cific focus on treating the heart. have yielded a class of AOs with improved safe-
ty and efficacy profiles. 2’-O-methyl (2’-OMe)
AOs are short, synthetic nucleic acid sequenc- and 2’-O-methoxyethyl (2’-MOE) alkyl substitu-
es which bind to complementary target mRNA ents are the most studied members of this
sequences and lead to either endonuclease- group. In addition, the use of a phosphorothio-
mediated transcript knockdown or splice mod- ate backbone which contains a sulfur in a non-
ulation [98, 99]. AO-mediated exon skipping bridging location on the phosphate backbone
can correct the reading frame by removing an significantly improves AO nuclease resistance
out-of-frame exon or exons from the DMD pre- and binding affinity to serum proteins [98, 107-
mRNA, producing a truncated but partly func- 109]. Antisense chemistries that contain both
tional dystrophin protein [100-102] (Figure 1). a phosphorothioate backbone and a 2’-alkyl
The first generation of AOs has the unmodified substituent, such as 2’-OMe-phosphorothioate
phosphoribose backbone, making them highly (2’OMePS) AOs, have shown several favorable
susceptible to degradation by nucleases [103, properties compared to their unmodified coun-
104] (Figure 2). Due to their short half-life, first terparts [105, 110-113]. The phosphodiester
generation AOs rarely achieve sufficient intra- backbone can also be replaced with a polyam-
cellular concentrations to have a therapeutic ide structure made up of repeating N-(2-
effect [105, 106]. Second and third generation aminoethyl) glycine units, which has given rise
AOs contain chemically modified structures. to another class of AOs termed peptide nucleic
These modifications not only increase AO re- acids (PNAs) [114]. This new class of AO can
1205 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
sterically block splicing factors, inhibit ribo- and multi-vesicular bodies (MVBs), and lyso-
some recruitment and bind non-coding RNAs, somes. Most AOs are initially delivered to early
thereby further expanding therapeutic potential endosomes. Subsequently, they can be traf-
[69]. ficked to lysosomes for degradation or seques-
tered in late endosomes/MVBs. Antisense dru-
Among these next-generation chemistries, ph- gs trapped within endomembrane compart-
osphorodiamidate morpholino oligomers (PM- ments are pharmacologically inactive as they
Os) represent the most advanced use of anti- remain separated from their target sites by
sense therapy for DMD. PMOs have the deoxy- membrane barriers [106, 129]. Nevertheless,
ribose/ribose moiety replaced by a morpholine a small portion of AOs escapes endosomes and
ring, and the charged phosphodiester inter- only then can they reach their targets and
subunit linkage replaced by an uncharged become pharmacologically active. The concept
phosphorodiamidate linkage, making PMOs of endosomal escape has been widely accept-
nuclease-resistant and charge-neutral [115, ed as the most important barrier to the effec-
116]. One of the challenges with using nucleic tive use of antisense drugs [127, 130]. Im-
acid-based molecules as therapeutics is their portantly for developing heart-effective AOs,
stability and potential toxicity in cells. The the research found that AOs (particularly PMOs)
advantage of being charge-neutral, as in the tend to be trapped in endosomes in cardiomyo-
case of PMOs, is that this imparts an even cytes more than in skeletal muscle cells [131].
greater resistance to nucleases, which typically Since cardiomyopathy is the leading cause of
target charged molecules. Additionally, due to death in DMD patients, researchers have
the lack of charge, PMOs are safer since they looked into different approaches to enhance
are unlikely to activate Toll-like receptors, a delivery of AOs to cardiac tissues. The next sec-
class of receptors involved in producing innate tion will discuss some of the most promising
immune responses against pathogenic materi- approaches to improving AO efficacy for treat-
al [117]. In fact, a PMO targeting DMD exon 51, ing the heart.
called eteplirsen or Exondys 51 (Sarepta
Therapeutics, Cambridge, MA, USA), was condi- Strategies to improve the efficacy of antisense
tionally approved by the U.S. Food and Drug drugs for the treatment of cardiomyopathy in
Administration (FDA) in 2016, and several DMD patients
PMOs targeting other DMD exons, including
golodirsen or SRP-4053 (Sarepta Therapeutics) Tricyclo-DNA
and NS-065/NCNP-01 (NS Pharma, Paramus,
NJ, USA) are currently undergoing clinical trials In the late nineties, a novel class of AOs known
[118-121]. as tricyclo-DNAs (tcDNAs) was shown to display
unique pharmacological properties. tcDNA is a
Although AOs effectively rescue dystrophin conformationally-constrained DNA analog that
expression in skeletal muscles, they are highly deviates from the natural DNA structure by the
inefficient in cardiac muscles [122, 123]. presence of an ethylene bridge connecting C3’
Failure to restore dystrophin expression in the and C5’ [132-134]. tcDNA shows enhanced
heart in the presence of rescued dystrophin in RNA affinity and nuclease resistance, as well
skeletal muscles can exacerbate cardiac issues as the inability to elicit RNase H activity [135-
due to increased patient voluntary activity 138]. Furthermore, tcDNAs can spontaneously
[124, 125]. The major barrier to effective use of form defined nanoparticles which potentia-
AOs in therapy is the delivery of antisense drugs lly improves delivery and cellular uptake com-
to their intracellular targets. Upon reaching the pared to other antisense chemistries [139-
cell surface, AOs are internalized by endocyto- 141].
sis. A variety of cell-surface receptors have
been suggested to bind AOs and facilitate their In a study by Goyenvalle and colleagues, a
entry into the cell including integrins, scavenger mouse model carrying a nonsense mutation in
receptors and Toll-like receptors [126-128]. exon 23 of the Dmd gene (hereafter referred to
Regardless of the endocytosis route taken, AOs as mdx mice) was injected intravenously with a
entering a cell will encounter an intricate net- 15 nucleotide long (15-mer) tcDNA-AO that tar-
work of membrane compartments that include gets the skipping of Dmd exon 23 [139].
early and recycled endosomes, late endosomes Treatment with 200 mg/kg/week of the drug
1206 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
for 12 weeks rescued up to 40% of wild type experiments are mentioned in this paper, but a
(WT) dystrophin expression in the heart. selected few will be discussed for each
Additionally, tcDNA-treated mice showed signif- approach.
icantly higher levels of dystrophin rescue, espe-
cially in the diaphragm and the heart, com- The (RXR)4 peptide (with R standing for arginine
pared to those treated with PMO and 2’-OMe and X standing for aminohexanoic acid) was the
AOs at an equimolar dosage. Similar results first arginine-rich CPP tested in the mdx model
were observed in a dystrophin/utrophin double of DMD [146]. In a study by Yin and colleagues,
knockout mouse model where treatment with (RXR)4 peptides were conjugated to PMOs tar-
weekly intravenous (IV) injections of 200 mg/ geting Dmd exon 23. A single IV injection at 25
kg of tcDNA over a period of 5-20 weeks mg/kg via tail vein resulted in ~50% exon 23
restored 53% of WT dystrophin levels in the skipping in the heart of treated mice. A wide-
heart. Treatment with tcDNA also ameliorated spread, uniform distribution of dystrophin-posi-
cardiac systolic function as demonstrated by tive fibers was also observed in cardiac tissue
improved ventricular ejection fractions and as shown by immunostaining. Western blot
shortening fractions in echocardiography. analysis demonstrated dystrophin restoration
at levels between 10 and 20% of that found in
One of the advantages of tcDNA is its increased the WT mouse heart. Even at lower doses
RNA binding affinity. Due to this feature, shorter administered (weekly injections at 6 mg/kg for
tcDNAs can be designed, reducing the mass of 3 weeks), dystrophin restoration was still
AOs administered and potential AO-induced observed in cardiac tissue as shown by immu-
toxicity while retaining their therapeutic effect. nostaining and Western blotting.
To investigate the efficacy of shorter tcDNAs,
mdx mice were injected intravenously with a Subsequently, another arginine-rich peptide,
13-mer tcDNA targeting Dmd exon 23 at 200 named the B-peptide, demonstrated high lev-
mg/kg/week for 12 weeks. The 13-mer tcDNA els of exon skipping in various muscles includ-
induced particularly high levels of exon skip- ing the heart. The B-peptide contains arginine,
ping and restored dystrophin in the heart as aminohexanoic acid and beta alanine (abbrevi-
shown by RT-PCR, Western blotting and immu- ated B) in an (RXRRBR)2 sequence [147-149]. A
nostaining. The safety profile of the treatment single IV injection at 30 mg/kg of B-peptide-
also showed that tcDNAs were well-tolerated, conjugated PMO (PPMO) restored 94% of dys-
with only minimal renal toxicity and liver inflam- trophin expression in cardiac muscle fibers of
mation observed [138]. Although tcDNAs have treated mdx mice by immunohistochemistry,
the potential to rescue dystrophin in cardiac tis- 50% of WT dystrophin levels by Western blot,
sue, treatment with these AOs requires high and 63% exon 23 skipping by RT-PCR. Repeated
dosage and multiple dose administrations. treatment for 3 months at the same dose at
biweekly intervals further improved dystrophin
Peptides restoration in cardiac muscle. Skipped tran-
script levels increased to 72%. Immunohis-
Among the various delivery systems studied, tochemistry and Western blot demonstrated
cell-penetrating peptides (CPPs) have gained dystrophin rescue at levels comparable to that
the most considerable interest. CPPs are com- in WT hearts. Dystrophin restoration was also
posed of cationic and/or amphipathic amino observed in the muscles of the atria and large
acids that are capable of delivering a wide vessels such as the aorta or vena cava and the
range of nucleic acid-based molecules both in pulmonary arteries. PPMO treatment signifi-
vitro and in vivo [142-144]. These peptides cantly improved cardiac function and prevent-
either possess natural translocating properties ed cardiac failure under dobutamine stress
or were engineered by combining different pro- [150]. A PPMO cocktail was also shown to
tein domains to have these properties [145]. restore dystrophin expression in the myocardi-
Many studies have investigated peptide-conju- um and cardiac Purkinje fibers, and improve
gated AOs for the potential treatment of DMD. cardiac conduction abnormalities in a canine
This review will discuss some of the most prom- model of DMD [151].
ising approaches, namely: arginine-rich pep-
tides, B peptides, PNA/PMO internalization Another promising class of CPPs is the Pips.
peptides (Pips), and phage peptides. Not all Pips are a novel series of transduction peptides
1207 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
developed from mutagenesis and functional also evaluated and no significant changes were
studies of a derivative of Penetratin, with the detected for liver and kidney damage. This
six arginine residues added to the N terminus result is encouraging since the phage peptides
of the CPP (R6Pen) [152]. Penetratin is origi- could be used as an alternative to arginine-rich
nally derived from the homeobox peptide of peptides, which have shown toxicity in higher
Drosophila Antennapedia. The CPPs in the Pip animals [156-158].
series are characterized by a central hydropho-
bic motif anchored on each side by arginine- Octaguanidine morpholino
rich sequences similar to that of the B-peptide
which contains arginine, aminohexanoic acid, In an effort to improve the efficacy of AO sys-
and beta-alanine residues. Among the highly temic delivery and to reduce the immunogenic-
efficient members of this series are Pip5 and ity of cell penetrating peptides, dendrimeric
Pip6, both of which have demonstrated high octaguanidine moieties have been conjugated
levels of dystrophin restoration in various mus- to PMOs to form a new class of AOs named
cles including the heart [153, 154]. A single IV Vivo-Morpholinos or vPMOs [150, 159].
injection of 25 mg/kg of Pip5e-PMO (a member
The guanidine groups in vPMOs work similarly
of the Pip5 family) induced almost complete
to the arginine-rich CPPs found conjugated to
exon skipping in cardiac tissue where full length
PMOs. As such, vPMOs have been shown to
uncorrected transcript was barely detectable. induce high levels of dystrophin expression es-
Immunohistochemistry data revealed more pecially in the heart [149]. Additionally, the
than 90% of dystrophin-positive fibers in cardi- combination of a synthetic scaffold and multi-
ac muscle. Dystrophin restoration was further ple unnatural side chains makes vPMOs unlike-
confirmed by Western blot which revealed more ly to elicit an immune response, thus allowing
than 50% of WT dystrophin levels in the heart for multiple administrations to maintain ade-
[153]. Modifications to the central hydrophobic quate levels of dystrophin in the body [160].
core of the Pip5 peptide gave rise to a novel
derivative of the Pip series, consecutively vPMOs have been shown to rescue cardiac dys-
named Pip6. When directly compared to Pip5e- trophin expression in vivo [161]. A single IV
PMO treatment, a member of the Pip6 family injection of a vPMO targeting mouse Dmd exon
exhibited significantly higher dystrophin resto- 23 (Vivo-ME23) at 6 mg/kg resulted in a strong
ration in the heart of treated mice at very low dystrophin signal in a significant number of car-
doses (12.5 mg/kg). The Pip6 series have also diomyocytes in mdx mice. Repeated treatment
been demonstrated to prevent exercise- at the same dose for five times biweekly res-
induced cardiomyopathy following Pip-PMO cued dystrophin expression in more than 40%
treatment in dystrophic mice [154]. of cardiomyocytes as observed by immunos-
taining. Western blot showed dystrophin rescue
While the above-mentioned CPPs work well for to approximately 10% of normal levels in cardi-
neutral AOs like PMOs, it is challenging to con- ac muscles. vPMOs have also been shown to
jugate positively charged peptides to negative- restore dystrophin expression in a canine mo-
ly-charged AOs such as 2’OMePS due to the del of DMD, however, no systemic injection was
presence of strong electrostatic interactions. In performed so whether vPMOs can rescue dys-
an effort to find uncharged CPPs, Jirka and trophin in canine cardiac tissues remains to be
colleagues screened a phage display peptide determined [162]. Regardless, these encourag-
library and identified a 7-mer peptide (P4) that ing results represent an important step forward
significantly enhanced AO uptake in cardiac tis- in our effort to overcome the challenges associ-
sue [155]. Dystrophic mdx mice were injected ated with the delivery of AOs to the heart.
subcutaneously with 200 mg/kg/week doses
of 2’OMePS-P4 conjugate targeting mouse Ultrasound and microbubbles
Dmd exon 23 for 6 weeks. Treatment with pep-
tide-conjugated AOs resulted in enhanced exon Another promising approach for improving AO
skipping efficacy with a significant difference in delivery to cardiac tissue is the use of ultra-
cardiac tissue compared to naked AOs, possi- sound in combination with contrast-enhancing
bly due to improved uptake in cardiac muscle. microbubbles [163]. Microbubbles are used to
The safety profile of the peptide conjugate was carry the drugs to an area of interest, then
1208 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
ultrasound is applied to burst the microbub- ZM2, have been shown to restore dystrophin
bles, resulting in tissue-specific delivery of the expression in the heart of mdx mice [172, 173].
therapeutic materials [164-167]. Ultrasound
exposure improves the efficacy of intracellular T1 nanoparticles are a type of cationic core-
delivery due to a phenomenon known as sono- shell nanospheres, made up of a core of poly-
poration or cellular sonification. This effect cre- methylmethacrylate (PMMA) and surrounded
ates transient pores in the cellular plasma by a shell of cationic groups, which facilitates
membrane by a process known as inertial cavi- the binding of charged AOs. In a study by
tation, thus allowing bioactive materials to Rimessi and colleagues, T1 nanoparticles were
enter the cells. Inertial cavitation is enhanced demonstrated to deliver 2’OMePS AOs and
by using microbubbles of contrast agents [164, induce dystrophin rescue in body-wide striated
muscles. AOs targeting the boundary sequenc-
167-170]. AOs can be mixed with or incorporat-
es of exon and intron 23 of mouse Dmd (M23D)
ed into microbubbles in a number of ways such
were conjugated with T1 nanoparticles, and
as binding to the microbubble shell or using
delivered by weekly intraperitoneal (IP) injec-
site-specific ligands. The combination of ultra-
tions at 2.7 mg/kg to mdx mice [172]. T1
sound and microbubbles not only improves
nanoparticles showed a wide distribution in the
intracellular delivery but also reduces the
body, including the heart. At one week post-
amount of drugs used systemically thereby le-
injection, immunohistochemical analysis of
ssening the potential toxicity and side effects treated mice showed the presence of dystro-
of treatment. phin-positive cardiomyocytes in various areas
of the heart. Dystrophin was however undetect-
In order to investigate the microbubble proper-
able in cardiac tissues 6 weeks after the last
ties that are important for influencing drug
injection. Total and skipped dystrophin tran-
delivery efficacy in vivo, PMOs targeting Dmd
script levels in the hearts of treated mice were
exon 23 of the mdx mouse were injected sys-
also significantly increased with 80% and 16%
temically at 16 mg/kg via the tail vein [171].
more transcripts, respectively. Although dystro-
PMOs were incorporated into three different
phin was undetected in the heart by Western
commercially available microbubbles: Sona-
blot, the results were positive considering a sig-
zoid, Optison, and SonoVue. Ultrasound was nificantly reduced dose compared to previous
then applied to the heart for two minutes after studies. From a safety aspect, T1 nanoparticles
injections. Treated hearts were collected 24 may cause adverse effects due to their slow
hours or one-week post injection. Of the three biodegradability, indicating a possibility of
microbubbles tested, Sonazoid and Optison accumulative toxicity for long-term treatments
induced significant amounts of dystrophin-pos- [172]. Also, T1 nanoparticles can form small
itive fibers in cardiac tissues. Treatments with aggregates and are therefore not suitable for IV
PMOs only (no ultrasound or microbubbles) injections.
were ineffective in terms of restoring dystro-
phin in cardiomyocytes. Microbubbles were To improve the efficacy of T1 nanoparticles, a
also found to increase AO delivery to the heart more efficient class of nanoparticles termed
in a dose-dependent manner. Histological anal- ZM2 was designed [173]. ZM2 nanoparticles
ysis showed no signs of tissue damage or are composed of a PMMA core and a random
observable morphological differences between copolymer shell consisting of units derived
samples treated with ultrasound and microbub- from N-isopropylacrylamide+ (NIPAM) and reac-
bles and non-treated controls. Additionally, tive methacrylate-bearing cationic groups. mdx
microbubble stability was determined to be the mice were injected IP weekly for 7 weeks at 7.5
major factor affecting the efficiency of thera- mg/kg with M23D AOs loaded onto ZM2
peutic drug delivery. nanoparticles. Immunohistochemical findings
showed 3% by manual count and 6% by semi-
Nanoparticles automated count of dystrophin-positive signal
in the heart. Dystrophin was also detectable,
In order to improve AO stability and enable the though faintly, in the heart of ZM2-M23D treat-
use of lower AOs concentrations in vivo, AO ed mice via Western blot. However, dystrophin
delivery using nanoparticles was developed was not detectable in the heart at 3 months
and demonstrated to be another promising post-injection as demonstrated in a follow-up
approach. Two classes of nanoparticles, T1 and study.
1209 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
Polymers Conclusion
Different series of polymers were investigated To summarize, with the exception of tricyclo-
for their ability to improve the delivery of AOs in DNAs, naked AOs are generally ineffective in
vitro and in vivo. The first class is a series of low treating the heart. Conjugation to CPPs, espe-
molecular weight polyethylenimine (LPEI) conju- cially arginine-rich peptides and the Pip series,
gated pluronic copolymers (PCMs) [174]. Am- appears to be a promising approach to improve
phiphilic pluronic, poly (ethylene oxide)-b-poly AO uptake and dystrophin restoration in cardi-
(propylene oxide)-b-poly (ethylene oxide) (PEO- ac tissue. However, the practicality of CPPs in
PPO-PEO triblock copolymer) has been used the clinical setting remains to be determined
widely as a pharmaceutical adjuvant and a free largely due to concerns over our complex
adjuvant for gene delivery. Depending on the immune system. Phage peptides and octagua-
molecular weight, hydrophilic-lipophilic balance nidine moieties were developed in an effort to
(HLB), and other characteristics of the pluron- reduce the immunogenicity of arginine-rich
ics, PCMs can have different AO delivery effi- peptides, however, they have been less suc-
ciencies and toxicities. In a study by Wang and cessful in rescuing dystrophin in systemic deliv-
colleagues, mdx mice were injected intrave- ery of antisense drugs to the heart. Other non-
nously with 0.4 mg of PCMs and 2 mg of PMOs covalent conjugation approaches such as the
targeting the boundary sequences of exon and use of nanoparticles, polymers, or ultrasound
intron 23 of mouse Dmd gene (PMOE23), or 2 and microbubbles are promising strategies to
mg of PMOE23 only as the control. Two weeks enhance the efficacy of AOs in cardiac tissue,
after injection, dystrophin was not detectable especially for charged antisense chemistries.
in cardiac muscle of control mice, while immu- With a growing number of AO-based approach-
nohistochemistry showed membrane-localized es being investigated, antisense therapy holds
dystrophin in more than 5% of cardiomyocytes the potential to improve the treatments for
in some areas of the heart from treated mice. DMD patients, with special focus on cardiac
Treatment also demonstrated no detectable aspects of the disease.
toxicity in muscles, liver, and kidneys after sys-
temic administration. Tricyclo-DNA clearly appears as a promising
chemistry for the antisense therapy of DMD-
Another class of amphiphilic polymers, termed associated cardiomyopathy due to its unique
Z polymers, is constructed from Tween 85 and pharmacological properties and high therapeu-
LPEI [175]. Based on preliminary results, two Z tic potential. Besides their ability to improve
polymers Z7 and Z8 were selected for systemic delivery and uptake into cardiac tissue, tcDNAs
injection. Dystrophic mdx mice were treated by can also cross the blood-brain barrier at low
IV injection with 1 mg Z7/1 mg PMO complex, or levels after systemic administration [139].
0.5 mg Z8/1 mg PMO conjugate, or 1 mg PMO Along with other distinctive properties, this out-
as a control. Dystrophin expression was not standing feature opens up more therapeutic
detected in the PMO-only group, however, options for other neuromuscular and neurode-
Z8-PMO treated mice demonstrated mem- generative disorders such as spinal muscular
brane-localized dystrophin-positive fibers in atrophy and Huntington’s disease [135].
some areas of the heart. No adverse effects Although the safety profile of tcDNAs has been
were observed in systemic delivery under the evaluated, observed toxicities were ascribed
experimental conditions. The mechanism/s by more to the phosphorothioate linkages rather
which amphiphilic polymers improve gene than the tcDNA chemistry itself [138]. More
transfer is/are not fully understood. Their hydro- extensive toxicological studies are recommend-
phobic interaction with cell membranes could ed to assess the full safety profile of this prom-
reduce membrane viscosity and facilitate the ising chemistry. Given its positive performance
entry of AOs [173]. Amphiphilic polymers could in the preclinical phase, the evaluation of tcD-
also prevent nonspecific binding of AOs to NAs in human clinical trials seems to be the
charged extracellular components, thus most logical next step. Similar to other chemis-
increasing the effective concentrations of ther- tries, the outcome essentially depends on how
apeutic drugs. well tcDNAs will be tolerated in patients.
1210 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
An active body of research on DMD has signifi- [3] Mendell JR, Shilling C, Leslie ND, Flanigan KM,
cantly broadened our knowledge on the pathol- Al-Dahhak R, Gastier-Foster J, Kneile K, Dunn
ogy as well as potential therapeutic treatments DM, Duval B, Aoyagi A, Hamil C, Mahmoud M,
Roush K, Bird L, Rankin C, Lilly H, Street N,
for the disease. To this day, DMD is still an
Chandrasekar R, Weiss RB. Evidence-based
invariably fatal disease that affects the whole path to newborn screening for Duchenne mus-
body. It is, therefore, essential to focus on treat- cular dystrophy. Ann Neurol 2012; 71: 304-
ments for individual systems such as the heart. 313.
Advances in the understanding of antisense [4] Moser H. Duchenne muscular dystrophy:
therapy have provided a strong foundation for pathogenetic aspects and genetic prevention.
the transition of AOs drugs from the lab bench Hum Genet 1984; 66: 17-40.
to the clinic. However, delivery and uptake in [5] Duchenne. The pathology of paralysis with
muscular degeneration (paralysie myosclero-
cardiac tissue remain the key limiting factor in
tique), or paralysis with apparent hypertrophy.
the bioavailability of AO-based therapies for the Br Med J 1867; 2: 541-542.
treatment of DMD. Perhaps more basic [6] Hoffman EF, Kunkel LM. Dystrophin abnormali-
research into understanding the underlying ties in Duchenne/becker muscular review dys-
mechanism of these processes is needed to trophy genes. Cell 1989; 2: 1019-1029.
overcome this major obstacle. Up to this point, [7] Mercuri E, Muntoni F. Muscular dystrophies.
clinical trials have focused mostly on the effi- Lancet 2013; 381: 845-860.
cacy of AOs treatments on skeletal muscle, [8] Tsuda T. Clinical manifestations and overall
without much emphasis on the heart. Given management strategies for Duchenne muscu-
lar dystrophy. Methods Mol Biol 2018; 1687:
how cardiomyopathy is currently the leading
19-28.
cause of death in patients with DMD, an [9] Bushby K, Finkel R, Birnkrant DJ, Case LE, Cle-
increased focus on treatments for the heart is mens PR, Cripe L, Kaul A, Kinnett K, McDonald
very much needed. In 2017, a clinical trial C, Pandya S, Poysky J, Shapiro F, Tomezsko J,
investigating the efficacy of a peptide-conjugat- Constantin C. Diagnosis and management of
ed version of eteplirsen was initiated. The trial Duchenne muscular dystrophy, part 1: diagno-
is expected to be completed in January 2019. sis, and pharmacological and psychosocial
With the promising results shown by peptide management. Lancet Neurol 2010; 9: 77-93.
[10] Strehle EM, Straub V. Recent advances in the
conjugated AOs in pre-clinical studies, it would
management of Duchenne muscular dystro-
be exciting to see the therapeutic outcome of phy. Arch Dis Child 2015; 100: 1173-1177.
the trial, particularly the cardiac aspects of it. [11] Manzur AY, Kinali M, Muntoni F. Update on the
Hopefully, these efforts will facilitate the prog- management of Duchenne muscular dystro-
ress of therapeutic development so that one phy. Arch Dis Child 2008; 93: 986-990.
day DMD will no longer be as devastating a dis- [12] Eagle M, Baudouin SV, Chandler C, Giddings
ease as it is now. DR, Bullock R, Bushby K. Survival in Duchenne
muscular dystrophy: improvements in life ex-
Disclosure of conflict of interest pectancy since 1967 and the impact of home
nocturnal ventilation. Neuromuscul Disord
None. 2002; 12: 926-929.
[13] Passamano L, Taglia A, Palladino A, Viggiano E,
Address correspondence to: Dr. Toshifumi Yokota, D’Ambrosio P, Scutifero M, Cecio MR, Torre V,
De Luca F, Picillo E, Paciello O, Piluso G, Nigro
Department of Medical Genetics, Faculty of
G, Politano L. Improvement of survival in Duch-
Medicine and Dentistry, University of Alberta, 8812- enne muscular dystrophy: retrospective analy-
112 St., Edmonton, AB T6G 2H7, Canada. Tel: sis of 835 patients. Acta Myol 2012; 31: 121-
+1-780-492-1102; E-mail: toshifum@ualberta.ca 125.
[14] Mah JK. Current and emerging treatment strat-
References egies for Duchenne muscular dystrophy. Neu-
ropsychiatr Dis Treat 2016; 12: 1795-1807.
[1] Nakamura A, Takeda S. Mammalian models of [15] Ervasti JM. Dystrophin, its interactions with
Duchenne muscular dystrophy: pathological other proteins, and implications for muscular
characteristics and therapeutic applications. J dystrophy. Biochim Biophys Acta 2007; 1772:
Biomed Biotechnol 2011; 2011: 184393. 108-117.
[2] Emery AE. Population frequencies of inherited [16] van Deutekom JC, van Ommen GJ. Advances in
neuromuscular diseases-A world survey. Neu- Duchenne muscular dystrophy gene therapy.
romuscul Disord 1991; 1: 19-29. Nat Rev Genet 2003; 4: 774-783.
1211 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
[17] Campbell KP. Three muscular dystrophies: loss [33] Pillers DA, Bulman DE, Weleber RG, Siges-
of cytoskeleton-extracellular matrix linkage. mund DA, Musarella MA, Powell BR, Murphey
Cell 1995; 80: 675-679. WH, Westall C, Panton C, Becker LE, Worton
[18] Whitmore C, Morgan J. What do mouse models RG, Ray PN. Dystrophin expression in the hu-
of muscular dystrophy tell us about the DAPC man retina is required for normal function as
and its components? Int J Exp Pathol 2014; defined by electroretinography. Nat Genet
95: 365-377. 1993; 4: 82-86.
[19] Ervasti JM, Campbell KP. A role for the dystro- [34] Takeshima Y, Yagi M, Okizuka Y, Awano H,
phin-glycoprotein complex as a transmem- Zhang Z, Yamauchi Y, Nishio H, Matsuo M. Mu-
brane linker between laminin and actin. J Cell tation spectrum of the dystrophin gene in 442
Biol 1993; 122: 809-823. Duchenne/becker muscular dystrophy cases
[20] Ervasti JM, Campbell KP. Membrane organiza- from one Japanese referral center. J Hum Gen-
tion of the dystrophin-glycoprotein complex. et 2010; 55: 379-388.
Cell 1991; 66: 1121-1131. [35] Buzin CH, Feng J, Yan J, Scaringe W, Liu Q, Den
[21] Lapidos KA, Kakkar R, McNally EM. The dystro- Dunnen J, Mendell JR, Sommer SS. Mutation
phin glycoprotein complex: signaling strength rates in the dystrophin gene: a hotspot of mu-
and integrity for the sarcolemma. Circ Res tation at a CpG dinucleotide. Hum Mutat 2005;
2004; 94: 1023-1031. 25: 177-188.
[22] Petrof BJ, Shrager JB, Stedman HH, Kelly AM, [36] Nachman MW, Crowell SL. Contrasting evolu-
Sweeney HL. Dystrophin protects the sarco- tionary histories of two introns of the Duch-
lemma from stresses developed during mus- enne muscular dystrophy gene, Dmd, in hu-
cle contraction. Proc Natl Acad Sci U S A 1993; mans. Genetics 2000; 155: 1855-1864.
90: 3710-3714. [37] Yokota T, Pistilli E, Duddy W, Nagaraju K. Poten-
[23] Nichols B, Takeda S, Yokota T. Nonmechanical tial of oligonucleotide-mediated exon-skipping
roles of dystrophin and associated proteins in therapy for Duchenne muscular dystrophy. Ex-
exercise, neuromuscular junctions, and brains. pert Opin Biol Ther 2007; 7: 831-842.
Brain Sci 2015; 5: 275-98. [38] White S, Kalf M, Liu Q, Villerius M, Engelsma D,
[24] Hoffman EP, Brown RH, Kunkel LM. Dystro- Kriek M, Vollebregt E, Bakker B, van Ommen
phin: the protein product of the Duchenne GJ, Breuning MH, den Dunnen JT. Comprehen-
muscular dystrophy locus. Cell 1987; 51: 919- sive detection of genomic duplications and de-
928. letions in the DMD gene, by use of multiplex
[25] Koenig M, Hoffman EP, Bertelson CJ, Monaco amplifiable probe hybridization. Am J Hum
AP, Feener C, Kunkel LM. Complete cloning of Genet 2002; 71: 365-374.
the Duchenne muscular dystrophy (DMD) [39] Ferlini A, Neri M, Gualandi F. The medical ge-
cDNA and preliminary genomic organization of netics of dystrophinopathies: molecular genet-
the DMD gene in normal and affected individu- ic diagnosis and its impact on clinical practice.
als. Cell 1987; 50: 509-517. Neuromuscul Disord 2013; 23: 4-14.
[26] Roberts RG, Coffey AJ, Bobrow M, Bentley DR. [40] Flanigan KM, Dunn DM, Von Niederhausern A,
Exon structure of the human dystrophin gene. Soltanzadeh P, Gappmaier E, Howard MT,
Genomics 1993; 16: 536-538. Sampson JB, Mendell JR, Wall C, King WM,
[27] Tsuda T, Fitzgerald K. Dystrophic cardiomyopa- Pestronk A, Florence JM, Connolly AM,
thy: complex pathobiological processes to gen- Mathews KD, Stephan CM, Laubenthal KS,
erate clinical phenotype. J Cardiovasc Dev Dis Wong BL, Morehart PJ, Meyer A, Finkel RS,
2017; 4: 14. Bonnemann CG, Medne L, Day JW, Dalton JC,
[28] Kamdar F, Garry DJ. Dystrophin-deficient car- Margolis MK, Hinton VJ, Weiss RB, Bromberg
diomyopathy. J Am Coll Cardiol 2016; 67: M, Swoboda K, Kerr L, Gurvich O, Tuohy T, Tay-
2533-2546. lor L, Zhao L, Hart K, Moural C, Hak K, Duval B,
[29] Ahn AH, Kunkel LM. The structural and func- Hamil C, Mahmoud M, Aoyagi A, Viollet L, Gai-
tional diversity of dystrophin. Nat Genet 1993; ley S, Lopate G, Golumbek P, Schierbecker J,
3: 283-291. Malkus B, Siener C, Baldwin K, Glanzman AM,
[30] Mehler MF. Brain dystrophin, neurogenetics Flickinger J, Naughton CE. Mutational spec-
and mental retardation. Brain Res Rev 2000; trum of DMD mutations in dystrophinopathy
32: 277-307. patients: application of modern diagnostic
[31] Chelly J, Hamard G, Koulakoff A, Kaplan JC, techniques to a large cohort. Hum Mutat
Kahn A, Berwald-Netter Y. Dystrophin gene 2009; 30: 1657-1666.
transcribed from different promoters in neuro- [41] Tuffery-Giraud S, Béroud C, Leturcq F, Yaou R
nal and glial cells. Nature 1990; 344: 64-65. Ben, Hamroun D, Michel-Calemard L, Moizard
[32] Lidov HG, Selig S, Kunkel LM. Dp140: a novel MP, Bernard R, Cossée M, Boisseau P, Blayau
140 kDa CNS transcript from the dystrophin M, Creveaux I, Guiochon-Mantel A, De Martin-
locus. Hum Mol Genet 1995; 4: 329-335. ville B, Philippe C, Monnier N, Bieth E, Van Kien
1212 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
PK, Desmet FO, Humbertclaude V, Kaplan JC, [51] Ashwath ML, Jacobs IB, Crowe CA, Ashwath
Chelly J, Claustres M. Genotype-phenotype RC, Super DM, Bahler RC. Left ventricular dys-
analysis in 2,405 patients with a dystrophinop- function in Duchenne muscular dystrophy and
athy using the UMD-DMD database: a model of genotype. Am J Cardiol 2014; 114: 284-289.
nationwide knowledgebase. Hum Mutat 2009; [52] Magri F, Govoni A, D’Angelo MG, Del Bo R, Ghe-
30: 934-945. zzi S, Sandra G, Turconi AC, Sciacco M, Ciscato
[42] Hoffman EP, Kunkel LM, Angelini C, Clarke A, P, Bordoni A, Tedeschi S, Fortunato F, Lucchini
Johnson M, Harris JB. Improved diagnosis of V, Bonato S, Lamperti C, Coviello D, Torrente Y,
Becker muscular dystrophy by dystrophin test- Corti S, Moggio M, Bresolin N, Comi G Pietro.
ing. Neurology 1989; 39: 1011-1017. Genotype and phenotype characterization in a
[43] Arahata K, Hoffman EP, Kunkel LM, Ishiura S, large dystrophinopathic cohort with extended
Tsukahara T, Ishihara T, Sunohara N, Nonaka I, follow-up. J Neurol 2011; 258: 1610-1623.
Ozawa E, Sugita H. Dystrophin diagnosis: com- [53] Spurney CF. Cardiomyopathy of Duchenne
parison of dystrophin abnormalities by immu- muscular dystrophy: current understanding
nofluorescence and immunoblot analyses. and future directions. Muscle Nerve 2011; 44:
Proc Natl Acad Sci U S A 1989; 86: 7154-7158. 8-19.
[44] Neri M, Torelli S, Brown S, Ugo I, Sabatelli P, [54] Thomas TO, Morgan TM, Burnette WB,
Merlini L, Spitali P, Rimessi P, Gualandi F, Markham LW. Correlation of heart rate and
Sewry C, Ferlini A, Muntoni F. Dystrophin levels cardiac dysfunction in Duchenne muscular
as low as 30% are sufficient to avoid muscular dystrophy. Pediatr Cardiol 2012; 33: 1175-
dystrophy in the human. Neuromuscul Disord 1179.
2007; 17: 913-918. [55] Miller G, D’Orsogna L, O’Shea JP. Autonomic
[45] Melacini P, Fanin M, Danieli GA, Villanova C, function and the sinus tachycardia of Duch-
Martinello F, Miorin M, Freda MP, Miorelli M, enne muscular dystrophy. Brain Dev 1989; 11:
247-250.
Mostacciuolo ML, Fasoli G, Angelini C, Dalla
[56] Lanza GA, Russo A Dello, Giglio V, De Luca L,
Volta S. Myocardial involvement is very fre-
Messano L, Santini C, Ricci E, Damiani A, Fu-
quent among patients affected with subclinical
magalli G, De Martino G, Mangiola F, Bellocci F.
Becker’s muscular dystrophy. Circulation
Impairment of cardiac autonomic function in
1996; 94: 3168-3175.
patients with Duchenne muscular dystrophy:
[46] Nigro G, Comi LI, Politano L, Bain RJ. The inci-
relationship to myocardial and respiratory
dence and evolution of cardiomyopathy in
function. Am Heart J 2001; 141: 808-812.
Duchenne muscular dystrophy. Int J Cardiol
[57] Kedem J, Sonn J, Scheinowitz M, Weiss HR. Re-
1990; 26: 271-277.
lationship between local oxygen consumption
[47] McNally EM, Kaltman JR, Benson D, Canter CE,
and local and external cardiac work: effect of
Cripe LH, Duan D, Finder JD, Hoffman EP, tachycardia. Cardiovasc Res 1989; 23: 1043-
Judge DP, Kertesz N, Kinnett K, Kirsch R, 1052.
Metzger JM, Pearson GD, Rafael-Fortney JA, [58] Chiang DY, Allen HD, Kim JJ, Valdes SO, Wang
Raman SV, Spurney CF, Targum SL, Wagner Y, Pignatelli RH, Lotze TE, Miyake CY. Relation
KR, Markham LW. Contemporary cardiac is- of cardiac dysfunction to rhythm abnormalities
sues in Duchenne muscular dystrophy. Work- in patients with Duchenne or becker muscular
ing group of the national heart, lung, and blood dystrophies. Am J Cardiol 2016; 117: 1349-
institute in collaboration with parent project 1354.
muscular dystrophy. Circulation 2015; 131: [59] Ramaciotti C, Heistein LC, Coursey M, Lemler
1590-1598. MS, Eapen RS, Iannaccone ST, Scott WA. Left
[48] Wang M, Birnkrant DJ, Super DM, Jacobs IB, ventricular function and response to enalapril
Bahler RC. Progressive left ventricular dysfunc- in patients with Duchenne muscular dystrophy
tion and long-term outcomes in patients with during the second decade of life. Am J Cardiol
Duchenne muscular dystrophy receiving car- 2006; 98: 825-827.
diopulmonary therapies. Open Hear 2018; 5: [60] Su JA, Ramos-Platt L, Menteer JD. Left ventric-
e000783. ular tonic contraction as a novel biomarker of
[49] Jefferies JL, Eidem BW, Belmont JW, Craigen cardiomyopathy in Duchenne muscular dystro-
WJ, Ware SM, Fernbach SD, Neish SR, Smith phy. Pediatr Cardiol 2016; 37: 678-685.
EOB, Towbin JA. Genetic predictors and remod- [61] Silva MC, Meira ZM, Gurgel Giannetti J, da Sil-
eling of dilated cardiomyopathy in muscular va MM, Campos AF, Barbosa Mde M, Starling
dystrophy. Circulation 2005; 112: 2799-2804. Filho GM, Ferreira Rde A, Zatz M, Rochitte CE.
[50] Nigro G, Politano L, Nigro V, Petretta VR, Comi Myocardial delayed enhancement by magnetic
LI. Mutation of dystrophin gene and cardiomy- resonance imaging in patients with muscular
opathy. Neuromuscul Disord 1994; 4: 371- dystrophy. J Am Coll Cardiol 2007; 49: 1874-
379. 1879.
1213 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
[62] Silva MC, Magalhães TA, Meira ZM, Rassi CH, tion in Duchenne muscular dystrophy and the
Andrade AC, Gutierrez PS, Azevedo CF, Gurgel- role of second messengers. Med Res Rev
Giannetti J, Vainzof M, Zatz M, Kalil-Filho R, 2013; 33: 1174-1213.
Rochitte CE. Myocardial fibrosis progression in [74] Berridge MJ, Lipp P, Bootman MD. The versatil-
Duchenne and becker muscular dystrophy: a ity and universality of calcium signalling. Nat
randomized clinical trial. JAMA Cardiol 2017; Rev Mol Cell Biol 2000; 1: 11-21.
2: 190-199. [75] Vallejo-Illarramendi A, Toral-Ojeda I, Aldanondo
[63] Mavrogeni SI, Markousis-Mavrogenis G, Pa- G, López de Munain A. Dysregulation of calci-
pavasiliou A, Papadopoulos G, Kolovou G. um homeostasis in muscular dystrophies. Ex-
Cardiac involvement in Duchenne muscular pert Rev Mol Med 2014; 16: e16.
dystrophy and related dystrophinopathies. [76] Zorov DB, Juhaszova M, Sollott SJ. Mitochon-
Methods Mol Biol 2018; 1687: 31-42. drial reactive oxygen species (ROS) and ROS-
[64] Urasawa N, Wada MR, Machida N, Yuasa K, induced ROS release. Physiol Rev 2014; 94:
Shimatsu Y, Wakao Y, Yuasa S, Sano T, Nonaka 909-950.
I, Nakamura A, Takeda S. Selective vacuolar [77] Gorski PA, Ceholski DK, Hajjar RJ. Altered myo-
degeneration in dystrophin-deficient canine cardial calcium cycling and energetics in heart
Purkinje fibers despite preservation of dystro- failure - a rational approach for disease treat-
phin-associated proteins with overexpression ment. Cell Metab 2015; 21: 183-194.
of Dp71. Circulation 2008; 117: 2437-2448. [78] Fong P, Turner PR, Denetclaw WF, Steinhardt
[65] Nomura H, Hizawa K. Histopathological study RA. Increased activity of calcium leak channels
of the conduction system of the heart in Duch- in myotubes of Duchenne human and mdx
enne progressive muscular dystrophy. Acta mouse origin. Science 1990; 250: 673-676.
Pathol Jpn 1982; 32: 1027-33. [79] Franco A, Lansman JB. Calcium entry through
[66] Yanagisawa A, Miyagawa M, Yotsukura M, stretch-inactivated ion channels in mdx myo-
Tsuya T, Shirato C, Ishihara T, Aoyagi T, Ishika- tubes. Nature 1990; 344: 670-673.
wa K. The prevalence and prognostic signifi- [80] Reid MB. Role of nitric oxide in skeletal mus-
cance of arrhythmias in Duchenne type mus- cle: synthesis, distribution and functional im-
cular dystrophy. Am Heart J 1992; 124: portance. Acta Physiol Scand 1998; 162: 401-
1244-50. 409.
[67] Wallace GQ, McNally EM. Mechanisms of mus- [81] Stamler JS, Meissner G. Physiology of nitric ox-
cle degeneration, regeneration, and repair in ide in skeletal muscle. Physiol Rev 2001; 81:
the muscular dystrophies. Annu Rev Physiol 209-237.
2009; 71: 37-57. [82] Raman SV, Hor KN, Mazur W, Halnon NJ, Kissel
[68] Konstam MA, Kramer DG, Patel AR, Maron MS, JT, He X, Tran T, Smart S, McCarthy B, Taylor
Udelson JE. Left ventricular remodeling in MD, Jefferies JL, Rafael-Fortney JA, Lowe J,
heart failure: current concepts in clinical sig- Roble SL, Cripe LH. Eplerenone for early car-
nificance and assessment. JACC Cardiovasc diomyopathy in Duchenne muscular dystrophy:
Imaging 2011; 4: 98-108. a randomised, double-blind, placebo-con-
[69] van Westering T, Betts C, Wood M. Current un- trolled trial. Lancet Neurol 2015; 14: 153-161.
derstanding of molecular pathology and treat- [83] Mendell JR, Moxley RT, Griggs RC, Brooke MH,
ment of cardiomyopathy in Duchenne muscu- Fenichel GM, Miller JP, King W, Signore L, Pan-
lar dystrophy. Molecules 2015; 20: 8823-8855. dya S, Florence J, Schierbecker J, Robison J,
[70] Shirokova N, Niggli E. Cardiac phenotype of Kaiser K, Mandel S, Arfken C, Gilder B. Ran-
Duchenne muscular dystrophy: insights from domized, double-blind six-month trial of pred-
cellular studies. J Mol Cell Cardiol 2013; 58: nisone in Duchenne’s muscular dystrophy. N
217-224. Engl J Med 1989; 320: 1592-1597.
[71] Fanchaouy M, Polakova E, Jung C, Ogrodnik J, [84] Dec GW. Steroid therapy effectively delays
Shirokova N, Niggli E. Pathways of abnormal Duchenne’s cardiomyopathy. J Am Coll Cardiol
stress-induced Ca2+ influx into dystrophic mdx 2013; 61: 955-956.
cardiomyocytes. Cell Calcium 2009; 46: 114- [85] Wu RS, Gupta S, Brown RN, Yancy CW, Wald
121. JW, Kaiser P, Kirklin NM, Patel PC, Markham
[72] Nakayama H, Chen X, Baines CP, Klevitsky R, DW, Drazner MH, Garry DJ, Mammen PP. Clini-
Zhang X, Zhang H, Jaleel N, Chua BHL, Hewett cal outcomes after cardiac transplantation in
TE, Robbins J, Houser SR, Molkentin JD. Ca2+- muscular dystrophy patients. J Heart Lung
and mitochondrial-dependent cardiomyocyte Transplant 2010; 29: 432-438.
necrosis as a primary mediator of heart failure. [86] Ryan TD, Jefferies JL, Sawnani H, Wong BL,
J Clin Invest 2007; 117: 2431-2444. Gardner A, Del Corral M, Lorts A, Morales DL.
[73] Mosqueira M, Zeiger U, Förderer M, Brinkmeier Implantation of the HeartMate II and Heart-
H, Fink RH. Cardiac and respiratory dysfunc- Ware left ventricular assist devices in patients
1214 Am J Transl Res 2019;11(3):1202-1218Antisense therapy for DMD cardiomyopathy
with Duchenne muscular dystrophy: lessons prednisone therapy in Duchenne muscular
learned from the first applications. ASAIO J dystrophy. Neurology 1991; 41: 1874-1877.
2014; 60: 246-248. [97] McMurray JJ, Östergren J, Swedberg K, Grang-
[87] Stoller D, Araj F, Amin A, Fitzsimmons C, Mor- er CB, Held P, Michelson EL, Olofsson B, Yusuf
lend R, Thibodeau JT, Ramaciotti C, Drazner S, Pfeffer MA. Effects of candesartan in pa-
MH, Meyer DM, Mammen PPA. Implantation of tients with chronic heart failure and reduced
a left ventricular assist device to provide long- left-ventricular systolic function taking angio-
term support for end-stage Duchenne muscu- tensin-converting-enzyme inhibitors: the cha-
lar dystrophy-associated cardiomyopathy. ESC rm-added trial. Lancet 2003; 362: 767-771.
Hear Fail 2017; 4: 379-383. [98] Wu H, Lima WF, Zhang H, Fan A, Sun H, Crooke
[88] Duboc D, Meune C, Pierre B, Wahbi K, Eymard ST. Determination of the role of the human
B, Toutain A, Berard C, Vaksmann G, Weber S, RNase H1 in the pharmacology of dna-like an-
Bécane HM. Perindopril preventive treatment tisense drugs. J Biol Chem 2004; 279: 17181-
on mortality in Duchenne muscular dystrophy: 9.
10 years’ follow-up. Am Heart J 2007; 154: [99] Lee J, Yokota T. Antisense therapy in neurology.
596-602. J Pers Med 2013; 3: 144-176.
[89] Viollet L, Thrush PT, Flanigan KM, Mendell JR, [100] Kole R, Krieg AM. Exon skipping therapy for
Allen HD. Effects of angiotensin-converting en- Duchenne muscular dystrophy. Adv Drug Deliv
zyme inhibitors and/or beta blockers on the Rev 2015; 87: 104-107.
cardiomyopathy in Duchenne muscular dystro- [101] Guncay A, Yokota T. Antisense oligonucleotide
phy. Am J Cardiol 2012; 110: 98-102. drugs for Duchenne muscular dystrophy: how
[90] Allen HD, Flanigan KM, Thrush PT, Dvorchik I, far have we come and what does the future
Yin H, Canter C, Connolly AM, Parrish M, Mc- hold? Future Med Chem 2015; 7: 1631-1635.
Donald CM, Braunlin E, Colan SD, Day J, Dar- [102] Nguyen Q, Yokota T. Immortalized muscle cell
model to test the exon skipping efficacy for
ras B, Mendell JR. A randomized, double-blind
Duchenne muscular dystrophy. J Pers Med
trial of lisinopril and losartan for the treatment
2017; 7: E13.
of cardiomyopathy in Duchenne muscular dys-
[103] Dias N, Stein CA. Antisense oligonucleotides:
trophy. PLoS Curr 2013; 5.
basic concepts and mechanisms. Mol Cancer
[91] Kajimoto H, Ishigaki K, Okumura K, Tomimatsu
Ther 2002; 1: 347-355.
H, Nakazawa M, Saito K, Osawa M, Nakanishi
[104] Eder PS, DeVine RJ, Dagle JM, Walder JA. Sub-
T. Beta-blocker therapy for cardiac dysfunction
strate specificity and kinetics of degradation of
in patients with muscular dystrophy. Circ J
antisense oligonucleotides by a 3’ exonucle-
2006; 70: 991-994.
ase in plasma. Antisense Res Dev 1991; 1:
[92] Matsumura T, Tamura T, Kuru S, Kikuchi Y,
141-151.
Kawai M. Carvedilol can prevent cardiac events [105] Geary RS, Norris D, Yu R, Bennett CF. Pharma-
in Duchenne muscular dystrophy. Intern Med cokinetics, biodistribution and cell uptake of
2010; 49: 1357-1363. antisense oligonucleotides. Adv Drug Deliv Rev
[93] Schram G, Fournier A, Leduc H, Dahdah N, 2015; 87: 46-51.
Therien J, Vanasse M, Khairy P. All-cause mor- [106] Juliano RL, Carver K. Cellular uptake and intra-
tality and cardiovascular outcomes with pro- cellular trafficking of oligonucleotides. Adv
phylactic steroid therapy in Duchenne muscu- Drug Deliv Rev 2015; 87: 35-45.
lar dystrophy. J Am Coll Cardiol 2013; 61: [107] De Clercq E, Eckstein E, Merigan TC. Interferon
948-954. induction increased through chemical modifi-
[94] Buyse GM, Goemans N, Van Den Hauwe M, cation of a synthetic polyribonucleotide. Sci-
Meier T. Effects of glucocorticoids and ideben- ence 1969; 165: 1137-1139.
one on respiratory function in patients with [108] Rifai A, Brysch W, Fadden K, Clark J, Schlingen-
Duchenne muscular dystrophy. Pediatr Pulm- siepen KH. Clearance kinetics, biodistribution,
onol 2013; 48: 912-920. and organ saturability of phosphorothioate oli-
[95] Tandon A, Villa CR, Hor KN, Jefferies JL, Gao Z, godeoxynucleotides in mice. Am J Pathol
Towbin JA, Wong BL, Mazur W, Fleck RJ, Sticka 1996; 149: 717-725.
JJ, Benson DW, Taylor MD. Myocardial fibrosis [109] Watanabe TA, Geary RS, Levin AA. Plasma pro-
burden predicts left ventricular ejection frac- tein binding of an antisense oligonucleotide
tion and is associated with age and steroid targeting human ICAM-1 (ISIS 2302). Oligonu-
treatment duration in Duchenne muscular dys- cleotides 2006; 16: 169-180.
trophy. J Am Heart Assoc 2015; 4: e001338. [110] Freier S, Altmann KH. The ups and downs of
[96] Fenichel GM, Florence JM, Pestronk A, Mendell nucleic acid duplex stability: structure-stability
JR, Moxley RT, Griggs RC, Brooke MH, Miller JP, studies on chemically-modified DNA: RNA du-
Robison J, King W, Signore L, Pandya S, Schier- plexes. Nucleic Acids Res 1997; 25: 4429-
becker J, Wilson B. Long-term benefit from 4443.
1215 Am J Transl Res 2019;11(3):1202-1218You can also read