Roxadustat for Treating Anemia in Patients with CKD Not on Dialysis: Results from a Randomized Phase 3 Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL RESEARCH www.jasn.org
Roxadustat for Treating Anemia in Patients with CKD
Not on Dialysis: Results from a Randomized Phase 3
Study
Steven Fishbane,1 Mohamed A. El-Shahawy,2 Roberto Pecoits-Filho,3,4 Bui Pham Van,5
Mark T. Houser,6 Lars Frison,7 Dustin J. Little,6 Nicolas J. Guzman,6 and Pablo E. Pergola8
Due to the number of contributing authors, the affiliations are listed at the end of this article.
ABSTRACT
Background Current anemia therapies for patients with non–dialysis-dependent CKD may require injec-
tion and medical visits. Roxadustat, an oral hypoxia-inducible factor prolyl hydroxylase inhibitor, stimu-
lates erythropoiesis and improves iron homeostasis.
Methods In this double-blind phase 3 study, we randomized patients with non–dialysis-dependent CKD
stages 3–5 and hemoglobin ,10.0 g/dl (1:1) to thrice-weekly 70-mg oral roxadustat or placebo. Doses
were titrated throughout the study based on hemoglobin levels. The primary efficacy end point was mean
change from baseline in hemoglobin averaged over weeks 28–52 versus placebo, irrespective of rescue
therapy use. We assessed patients for adverse events.
Results The study included 2781 patients, 1393 who received roxadustat and 1388 who received placebo.
Mean baseline hemoglobin was 9.1 g/dl for both groups. The mean change in hemoglobin from baseline
was 1.75 g/dl (95% confidence interval [95% CI], 1.68 to 1.81) with roxadustat versus 0.40 g/dl (95% CI, 0.33
to 0.47) with placebo, (P,0.001). Among 411 patients with baseline elevated high-sensitivity C-reactive
protein, mean change in hemoglobin from baseline was 1.75 g/dl (95% CI, 1.58 to 1.92) with roxadustat
versus 0.62 g/dl (95% CI, 0.44 to 0.80) with placebo, (P,0.001). Roxadustat reduced the risk of red blood
cell transfusion by 63% (hazard ratio, 0.37; 95% CI, 0.30 to 0.44). The most common adverse events with
roxadustat and placebo, respectively, were ESKD (21.0% versus 20.5%), urinary tract infection (12.8%
versus 8.0%), pneumonia (11.9% versus 9.4%), and hypertension (11.5% versus 9.1%).
Conclusions Roxadustat effectively increased hemoglobin in patients with non–dialysis-dependent CKD
and reduced the need for red blood cell transfusion, with an adverse event profile comparable to that of
placebo.
Clinical Trial registry name and registration number: Safety and Efficacy Study of Roxadustat to Treat
Anemia in Patients With CKD, Not on Dialysis, NCT02174627
JASN 32: ccc–ccc, 2021. doi: https://doi.org/10.1681/ASN.2020081150
Anemia is frequently experienced by patients with
non–dialysis-dependent CKD (NDD-CKD) and its
prevalence increases with advancing CKD stage.1–5 Received August 9, 2020. Accepted December 1, 2020.
Anemia of CKD is associated with reduced quality Published online ahead of print. Publication date available at
of life and an increased risk of mortality and www.jasn.org.
hospitalization.6–11
Correspondence: Prof. Steven Fishbane, Department of Medi-
The recommended therapies for anemia in pa- cine, Donald and Barbara Zucker School of Medicine at Hofstra/
tients with NDD-CKD include erythropoiesis- Northwell, 100 Community Drive, 2nd Floor, Great Neck, NY
11021. Email: sfishbane@northwell.edu
stimulating agents (ESAs), oral or intravenous
(iv) iron, and red blood cell (RBC) transfusion.12 Copyright © 2021 by the American Society of Nephrology
JASN 32: ccc–ccc, 2021 ISSN : 1046-6673/3203-ccc 1CLINICAL RESEARCH www.jasn.org
However, these therapies may require injection and medi-
Significance Statement
cal office visits, and may be associated with adverse
outcomes.12–15 RBC transfusion is associated with risks in- Anemia is untreated in many patients with non–dialysis-dependent
cluding infection and allosensitization,15,16 and costs; thus, a CKD. Barriers to the use of current anemia therapies among such
patients include parenteral administration that may require a
treatment objective for anemia is to avoid RBC transfu-
medical visit, a requirement for iron repletion, and potentially in-
sion.12,17,18 ESAs are an established therapy for anemia in pa- creased risk of cardiovascular events. In a phase 3 placebo-
tients with NDD-CKD, and although effective at increasing controlled international study, the authors compared roxadustat,
hemoglobin (Hb) and reducing the need for RBC transfusion, an oral hypoxia-inducible factor prolyl hydroxylase inhibitor, with
safety concerns noted with ESAs have stimulated the develop- placebo for the treatment of anemia of non–dialysis-dependent
CKD. They report that roxadustat was statistically superior to pla-
ment of alternative treatments for anemia.19–21 According to
cebo in increasing hemoglobin and reduced the need for red blood
US product labels and international clinical practice guide- cell transfusion. The drug also was generally well tolerated and had
lines, ESAs can be considered in patients with Hb ,10 g/dl an adverse event profile comparable to placebo. These findings
at risk of RBC transfusions.12,17,18 ESA US product labels state indicate that roxadustat may be clinically useful for the oral man-
that dosing should be reduced or interrupted when Hb ex- agement of anemia in patients with non–dialysis-dependent CKD.
ceeds 10 g/dl, and that supplemental iron should be admin-
istered among patients with ferritin ,100 mg/L or transferrin METHODS
saturation (TSAT) ,20%.22,23 Oral iron, however, is associ-
ated with gastrointestinal side effects and barriers exist to Trial Design and Oversight
administration of iv iron in NDD-CKD.13,24 These limitations This phase 3, multicenter, randomized, double-blind,
of established therapies may contribute to estimates from in- placebo-controlled study (NCT02174627) was performed in
ternational analyses that approximately 50%–90% of patients 385 centers across 25 countries worldwide. The study com-
with anemia of NDD-CKD are untreated.4,5,11,25–30 In partic- prised a screening period of up to 6 weeks, a treatment period
ular, analyses estimate that ESA use among patients with of variable duration up to 4 years, and an end of study (EOS)
anemia of NDD-CKD in the real world ranges from 11% follow-up visit (Figure 1). Treatment end date was defined on
to 35%.11,28–30 Accordingly, research has focused on devel- the basis of accrual of a predefined number of adjudicated
oping alternative therapies for patients with anemia of cardiovascular events for a separate pooled analysis (to pro-
NDD-CKD on the basis of the physiologic pathways of vide adequate power) of three phase 3, placebo-controlled
erythropoiesis. roxadustat studies in NDD-CKD conducted by different spon-
Hypoxia-inducible factor prolyl hydroxylase (HIF-PH) in- sors (NCT02174627, NCT01887600, NCT01750190).
hibitors are a new class of drug for anemia of CKD following The final study protocol and informed consent form, and
recent Nobel Prize–winning research delineating response any amendments to them, were approved by an Independent
mechanisms to hypoxia.31 Roxadustat was the first-in-class Ethics Committee or Institutional Review Board in each par-
HIF-PH inhibitor to be approved by a regulatory agency to ticipating center. All patients provided written, informed con-
treat anemia in patients with dialysis-dependent CKD in Japan sent. This study was performed in accordance with the ethical
and China and in patients with NDD-CKD in China. 32 principles of the Declaration of Helsinki and the International
Hypoxia-inducible factor (HIF) is a transcription factor that Council for Harmonisation Good Clinical Practice (GCP).
regulates expression of genes stimulating erythropoiesis. In
normoxia, HIF-PH is active and promotes degradation of Patients
HIF-a.33–35 Roxadustat reversibly stabilizes HIF-a, which Eligible patients were aged $18 years; had eGFR ,60 ml/min
promotes a coordinated erythropoietic response by activat- per 1.73 m2, corresponding to stages 3–5 CKD; were not on
ing a number of genes, including those encoding endoge- dialysis; and had a mean of two values of Hb ,10 g/dl mea-
nous erythropoietin, enzymes of heme biosynthesis, and sured at least 7 days apart during the screening period; and
proteins that promote bone marrow iron availability via ferritin $50 mg/L and TSAT $15%. Full inclusion and exclu-
improved absorption and transport.35,36 HIF-PH inhibitors sion criteria are provided in the Supplemental Material.
are taken orally and routinely self-administered. In phase 2
and smaller, single-nation phase 3 studies among patients Treatment
with NDD-CKD and anemia, roxadustat increased and Eligible patients were randomly assigned in a 1:1 ratio to re-
maintained Hb levels, 37–39 with similar adverse events ceive roxadustat or placebo in a double-blind manner, which
(AEs) compared with placebo.37,38 The roxadustat clinical was performed centrally using an Interactive Web Response
development program comprises both placebo- and active- System/Interactive Voice Response System. Randomization
controlled phase 3 clinical studies designed to assess the codes were computer generated by AstraZeneca Research &
efficacy and safety of roxadustat in NDD-CKD. Here, we Development using GRand and a block randomization sched-
report the results of OLYMPUS, a global phase 3 study of ule comprising a block size of 4. Randomization was stratified
the efficacy and safety of roxadustat in 2781 patients with by country to ensure a balanced global distribution. The in-
anemia of NDD-CKD. vestigator, study site staff, and patient were blinded to study
2 JASN JASN 32: ccc–ccc, 2021www.jasn.org CLINICAL RESEARCH
HbCLINICAL RESEARCH www.jasn.org
$2.0 g/dl (if #8.0 g/dl at baseline); (2) mean change from Material). Superiority of roxadustat compared with placebo
baseline in Hb averaged over weeks 28–52 among patients was declared if the lower bound of the two-sided 95% confi-
with baseline high-sensitivity C-reactive protein (hsCRP; as- dence interval (95% CI) of the difference between roxadustat
sessed among patients who consented to biobank samples) and placebo exceeded 0 g/dl. Overall, 14.3% and 21.2% of
greater than the upper limit of normal (ULN; 5 mg/L); (3) roxadustat and placebo datapoints, respectively, were imputed
proportion of total time of interpolated Hb values $10 g/dl for the primary efficacy analysis of mean change from baseline
from weeks 28–52; (4) proportion of total time of interpolated in Hb (ITT analysis set) and 200 datasets with simulated data
Hb values within 10–12 g/dl from weeks 28–52; (5) mean were generated accordingly (Supplemental Material). Sub-
change from baseline in serum LDL cholesterol (LDL-C) to group analyses were also performed using the ITT analysis
week 24; (6) need for first rescue therapy (composite) of any of set (Supplemental Material).
iv iron, RBC transfusion, or ESA; (7) need for first RBC trans- For the secondary efficacy end points, a fixed sequence
fusion as rescue therapy; (8) mean change from baseline in approach adjusted for multiple testing; formal statistical hy-
SF-36 Vitality subscore averaged over weeks 12–28; (9) annual pothesis testing was stopped once a test was accompanied by a
rate of change in eGFR starting from week 4, using all post- P value $0.05. Secondary and key exploratory efficacy end
baseline eGFR values before initiation of dialysis/kidney trans- points were analyzed using Cochran–Mantel–Haenszel tests,
plant; and (10) mean change from baseline in SF-36 Physical Cox proportional hazard regression models, ANCOVA, and
Functioning subscore averaged over weeks 12–28. mixed-effect model repeated measures; full details of the sta-
Key exploratory efficacy end points included: change in tistical methods and analysis sets are listed in Supplemental
hepcidin (assessed from available biobank samples) from Tables 1 and 2. Need for first rescue therapy end points are
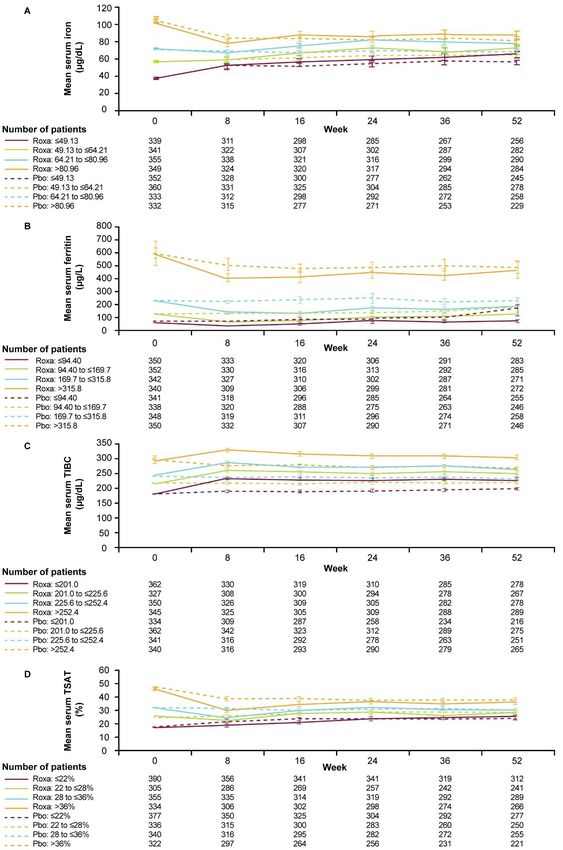
baseline to week 24; change from baseline in serum iron pro- presented as the number (%) of patients with the event and
files (iron, ferritin, total iron binding capacity [TIBC], and event rates per 100 patient-years at risk (total number of years
TSAT) averaged over week 24 to end of treatment (EOT); at risk).
and change from baseline in sitting systolic BP (SBP) and di- Details of the assessment of treatment compliance are pro-
astolic BP (DBP). TSATwas calculated as: TSAT (%) 5 (serum vided in the Supplemental Material.
iron level 3 100)/(TIBC). AEs were analyzed using the ITT analysis set, with patients
The primary safety objective was to contribute adjudicated censored at their individual EOS visit regardless of study drug
cardiovascular safety data to a separate pooled safety analysis discontinuation, at the date of withdrawal of consent or last
across the NDD-CKD studies in the roxadustat phase 3 pro- study contact if the patient withdrew consent, or at the date
gram. Safety analyses included assessment of the incidence of of death, whichever was earliest. Patients with more than one
AEs. AEs were coded using the Medical Dictionary for Regu- event for the same AE category/preferred term were counted
latory Activities version 20.0. For patients who withdrew con- once in that category/preferred term. The AE exposure-
sent, public record searches were used to confirm vital status adjusted event rate (per 100 patient-years) was calculated as
(alive or dead), as appropriate, in accordance with local follows:
regulations. [Number of patients with AEs/(the total number of
days at risk for that AE across all patients in given
Statistical Analyses group/365.25)] 3 100.
To contribute an adequate number of adjudicated cardiovas- All data were analyzed using SAS software version 9.4 (SAS
cular safety events to the separate pooled analysis of phase Institute, Cary, NC).
3 NDD-CKD studies (including approximately 4000 patients
overall), approximately 2600 patients were planned to be ran-
domized in OLYMPUS. The intent-to-treat (ITT) population RESULTS
comprised all patients who were randomized to study treat-
ment throughout the duration of the study, irrespective of Patients
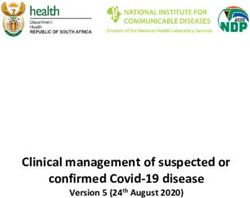
their protocol adherence and continued participation in the Overall, 5222 patients were screened. Of these, 2441 (46.7%)
study. The full analysis set (FAS) included patients from the were not randomized, most commonly due to patients not
ITT analysis set who received study drug and had baseline Hb meeting all inclusion/exclusion criteria (n52336 [95.7%];
and $1 postdose Hb assessments. The on-treatment (OT) Figure 2). From June 26, 2014 to May 11, 2017, 2781 patients
128 analysis set comprised all patients who received $1 were randomized to roxadustat (n51393) or placebo
dose of randomized study treatment and was censored (n51388). Twenty patients were excluded due to incorrect
28 days after last intake of study treatment. randomization (n54) or significant GCP violations (n516)
The primary efficacy end point was analyzed in the ITT in obtaining or recording the data that might affect the validity
analysis set using missing at random–based multiple imputa- of the data; therefore, the ITT population comprised 1384 and
tion analysis of covariance (ANCOVA), containing terms for 1377 patients receiving roxadustat and placebo, respectively
treatment, baseline Hb measurement, baseline eGFR, geo- (Figure 2). The FAS included 2728 patients (roxadustat
graphic region, and cardiovascular history (Supplemental n51371; placebo n51357) and the OT128 population
4 JASN JASN 32: ccc–ccc, 2021www.jasn.org CLINICAL RESEARCH
Patients screened (n=5222) Not randomized (n=2441)
Did not meet full eligibility criteria (n=2336)
Death (n=16)
Randomized Patients randomized (n=2781)
Patient decision (n=89)
Allocation
Allocated to roxadustat Allocated to placebo Excluded from analysisa (n=11)
Excluded from analysisa (n=9) (n=1393) (n=1388) Did not receive treatment (n=1)
Received treatment Received treatment Withdrew from study (n=130)
(n=1384) (n=1376) Patient decision (n=128)
Withdrew from study (n=84) Incorrect enrollment (n=1)
Patient decision (n=84) Missing (n=1)
Discontinued treatment (n=801)
Discontinued treatment (n=499) Patient decision (n=390)
Follow-up
Patient decision (n=250) Adverse event (n=52)
Adverse event (n=79) Completed treatment Completed treatment Protocol non-compliance (n=13)
Protocol non-compliance (n=12) (n=885) (n=575) Study-specific discontinuation
Study-specific discontinuation criteria (n=252)
criteria (n=76) Other (n=93)
Other (n=82) Missing (n=1)
Completed study Completed study
(n=1300) (n=1247)
Figure 2. Patient disposition. aBecause of GCP violations. Study-specific discontinuation criteria included patients who required di-
alysis initiation and ESA rescue therapy. When possible, patients who discontinued treatment were followed for concomitant medi-
cations, AEs, vital status, and hospitalization.
included 2760 patients (roxadustat n51384; placebo 0.29 to 0.45; nominal P,0.001). Withdrawal of consent was more
n51376). The predominant reason for exclusion from the common in placebo- than roxadustat-treated patients (n5128
FAS was the absence of postdose Hb data (n532). [9.3%] versus n584 [6.1%], respectively). Vital status at the end
Baseline demographic and clinical characteristics were sim- of the study was confirmed for 2756 of 2781 patients (99.1%),
ilar between the treatment groups (Table 1). Mean baseline Hb with ten (0.7%) roxadustat- and 15 (1.0%) placebo-treated
overall was 9.1 g/dl and mean eGFR was 19.7 and 20.0 ml/min patients having unknown vital status at the end of the study.
per 1.73 m2 in the roxadustat and placebo groups, respec-
tively. At baseline, approximately 58% of patients had ferritin Dosing
.100 mg/L and TSAT .20% (Table 1). Iron supplements were Duration of exposure was longer with roxadustat than placebo
taken by 1777 of 2761 (64.4%) patients during the study, in- (mean [SD] 19.62 [10.39] versus 15.24 [10.48] months, re-
cluding oral bivalent (n51283 of 2761 [46.5%]) and oral tri- spectively; median [interquartile range] 20.80 [11.38–27.55]
valent (n5188 of 2761 [6.8%]) iron (Supplemental Table 3). versus 14.57 [5.52–23.51] months, respectively). The most
Overall, 1300 patients discontinued study drug prema- common roxadustat doses were in the range of 40–100 mg
turely. Fewer patients in the roxadustat group (n5499 of orally three times weekly (Supplemental Table 4). Mean
1384 [36.1%]) discontinued study drug versus the placebo (SD) weekly dose, calculated as the total cumulative dose/ac-
group (n5801 of 1376 [58.2%]); the difference was observed tual treatment duration (in weeks), of roxadustat was 207.6
early and maintained throughout the study (Figure 3, (116.7) mg, with a median (interquartile range) of 182.3
Supplemental Figure 1). Post hoc analyses showed a 51% lower (124.1–267.3) mg. During treatment, 1204 (87.0%) patients
risk of study drug discontinuation with roxadustat versus pla- in the roxadustat group compared with 577 (41.9%) patients
cebo (hazard ratio [HR] 0.49; 95% CI, 0.44 to 0.55; nominal in the placebo group had at least one dose reduction, whereas
P,0.001). In post hoc analyses, factors associated with study approximately 90% of all patients had at least one dose in-
drug discontinuation were baseline eGFR ,15 ml/min per crease (Supplemental Table 5). Compliance ($75%) to treat-
1.73 m2 and initiation of dialysis after randomization. Fewer ment was observed in 1330 (96.1%) patients with roxadustat
patients in the roxadustat arm discontinued study drug versus and 1330 (96.7%) patients with placebo.
placebo among those with baseline eGFR ,15 ml/min per
1.73 m 2 (n5250 of 591 [42.3%] versus n5421 of 597 Primary Efficacy End Point
[70.5%]; HR 0.42; 95% CI, 0.36 to 0.49; nominal P,0.001) The adjusted least-squares mean (LSM) change from baseline
and those initiating dialysis while on study drug (n5174 of in Hb averaged over weeks 28–52 was significantly greater with
457 [38.1%] versus n5185 of 272 [68.0%]; HR 0.36; 95% CI, roxadustat versus placebo (11.75 g/dl [95% CI, 1.68 to 1.81]
JASN 32: ccc–ccc, 2021 Roxadustat in Nondialysis CKD 5CLINICAL RESEARCH www.jasn.org Table 1. Baseline demographic and clinical characteristics (ITT analysis set) Characteristic Roxadustat (n51384) Placebo (n51377) Age, yr Mean (SD) 60.9 (14.7) 62.4 (14.1) Sex, n (%) Female 820 (59.2) 774 (56.2) Race, n (%) White 623 (45.0) 611 (44.4) Black 112 (8.1) 115 (8.4) Asian 544 (39.3) 538 (39.1) Native Hawaiian or Pacific Islander 0 2 (0.1) American Indian or Alaska Native 24 (1.7) 29 (2.1) Other 81 (5.9) 82 (6.0) Geographic region, n (%) USA 343 (24.8) 340 (24.7) Canada 26 (1.9) 24 (1.7) Latin America 206 (14.9) 205 (14.9) Asia 522 (37.7) 521 (37.8) Europe 287 (20.7) 287 (20.8) Weight, kg Mean (SD) 69.9 (18.5) 70.6 (18.8) BMI, kg/m2 Mean (SD) 26.7 (6.0) 26.9 (6.1) Comorbidities, n (%) Hypertension 1274 (92.1) 1280 (93.0) Type 2 diabetes mellitus 737 (53.3) 771 (56.0) Dyslipidemia 683 (49.3) 691 (50.2) Coronary artery disease 160 (11.6) 178 (12.9) Cardiac failure congestive 151 (10.9) 155 (11.3) Hb, g/dl Mean (SD) 9.1 (0.7) 9.1 (0.7) Hb, g/dl, n (%) #8 129 (9.3) 131 (9.5) .8 to #9 386 (27.9) 402 (29.2) .9 869 (62.8) 844 (61.3) eGFRa, ml/min per 1.73 m2 Mean (SD) 19.7 (11.7) 20.0 (11.7) eGFR, ml/min per 1.73 m2, n (%) ,10 291 (21.0) 283 (20.6) 10 to ,15 300 (21.7) 315 (22.9) 15 to ,30 534 (38.6) 520 (37.8) 30 to ,45 201 (14.5) 196 (14.2) 45 to ,60 55 (4.0) 59 (4.3) $60 3 (0.2) 4 (0.3) LDL-C, mg/dl Mean (SD) 94.4 (43.4) 92.4 (42.0) Ferritin .100 mg/L and TSAT .20%, n (%) 809 (58.5) 799 (58.0) hsCRP, mg/dl Meanb (SD) 0.7 (1.5) 0.7 (1.8) hsCRP .ULNb, n (%) 227 (16.4) 209 (15.2) SBP, mmHg Mean (SD) 134.4 (13.3) 135.5 (12.7) DBP, mmHg Mean (SD) 74.5 (9.1) 74.1 (9.3) Most likely cause of CKD, n (%)c Diabetic nephropathy 614 (44.9) 602 (44.2) Ischemic/hypertensive nephropathy 207 (15.2) 192 (14.1) Chronic GN 169 (12.4) 155 (11.4) 6 JASN JASN 32: ccc–ccc, 2021
www.jasn.org CLINICAL RESEARCH
Table 1. Continued
Characteristic Roxadustat (n51384) Placebo (n51377)
Other primary or secondary GN 75 (5.5) 82 (6.0)
Cystic kidney disease 74 (5.4) 62 (4.6)
Chronic interstitial nephritis 36 (2.6) 27 (2.0)
Chronic pyelonephritis (infectious) 30 (2.2) 44 (3.2)
FSGS 28 (2.0) 17 (1.2)
IgA nephropathy 19 (1.4) 23 (1.7)
Obstructive nephropathy 17 (1.2) 24 (1.8)
Membranous nephropathy 13 (1.0) 10 (0.7)
Lupus nephritis 7 (0.5) 2 (0.1)
Renal artery stenosis 2 (0.1) 1 (,0.1)
Minimal change 2 (0.1) 6 (0.4)
Obstructive uropathy 1 (,0.1) 0
Not specified 25 (1.8) 15 (1.1)
Unknown 124 (9.1) 137 (10.1)
Other 92 (6.7) 117 (8.6)
Missing 18 16
BMI, body mass index.
a
Calculated using the four-variable Modification of Diet in Renal Disease equation.
b
hsCRP quantified from stored biomarker samples obtained at randomization (n5753 for roxadustat, n5717 for placebo); ULN is 5 mg/l (0.5 mg/dl).
c
Percentages were on the basis of the number of patients with nonmissing data (n51366 for roxadustat, n51361 for placebo).
versus 10.40 g/dl [95% CI, 0.33 to 0.47], respectively; differ- (8.5%) during the first 24 weeks of treatment (relative risk
ence 11.35 g/dl; 95% CI, 1.27 to 1.43; P,0.001) (Figure 4A). 9.12; 95% CI, 7.63 to 10.89; P,0.001) (Figure 4D). Among
An initial separation of Hb levels for roxadustat versus placebo 411 patients with baseline hsCRP .ULN, the adjusted LSM
was observed after randomization and sustained until EOT change from baseline in Hb averaged over weeks 28–52 was
(Figure 4C). significantly greater with roxadustat versus placebo (11.75 g/dl
[95% CI, 1.58 to 1.92] versus 10.62 g/dl [95% CI, 0.44 to 0.80],
Secondary Efficacy End Points respectively; difference 11.13 g/dl; 95% CI, 0.91 to 1.35;
A significantly greater proportion of patients receiving roxa- P,0.001) (Figure 4E). The proportions of total time of inter-
dustat (77.0%) achieved an Hb response versus placebo polated Hb values $10 g/dl and 10–12 g/dl from weeks 28 to 52
100
Cumulative percentage (%)
80
60
40
Events/N KM%
Placebo (eGFRCLINICAL RESEARCH www.jasn.org
A B Iron replete Non-iron replete
Pwww.jasn.org CLINICAL RESEARCH
were significantly greater with roxadustat versus placebo with roxadustat and increased with placebo (adjusted LSM
(P,0.001) (Table 2). [SD] change from baseline 235.94 [116.69] ng/ml versus
Mean LDL-C levels at baseline were similar for roxadustat 19.42 [115.78] ng/ml, respectively) (Table 3). Adjusted LSM
(94.50 mg/dl) and placebo (92.52 mg/dl). The adjusted LSM changes in serum iron, ferritin, TIBC, and TSAT from baseline
change in LDL-C from baseline to week 24 was significantly averaged over week 24 to EOT were as follows: serum iron was
greater with roxadustat versus placebo (214.58 mg/dl versus increased with roxadustat and reduced with placebo (16.63
20.70 mg/dl, respectively; difference 213.88 mg/dl; 95% CI, versus 21.07 mg/dl, respectively; difference 7.70 mg/dl; 95%
216.37 to 211.39; P,0.001) (Table 2). CI, 5.82 to 9.58) (Figure 7A, Table 3); serum ferritin was re-
Fewer roxadustat- versus placebo-treated patients received duced with roxadustat and increased with placebo (237.10
$1 rescue therapy for the overall composite, and for each indi- versus 117.45 mg/l, respectively; difference 254.55 mg/l;
vidual component (RBC transfusion, iv iron, or ESA; Figure 5). 95% CI, 271.68 to 237.42) (Figure 7B, Table 3); serum
Event rates for use of first rescue therapy and first rescue RBC TIBC was increased with roxadustat and reduced with placebo
transfusion were lower with roxadustat than placebo (Figure 5, (130.79 versus 23.82 mg/dl, respectively; difference 34.61 mg/dl;
Table 2). Roxadustat achieved risk reductions versus placebo of 95% CI, 31.29 to 37.93) (Figure 7C, Table 3); and there was
74% for rescue therapy overall, 63% for RBC transfusion, 59% no difference in change from baseline in TSAT (20.83%
for iv iron, and 87% for ESA (all P,0.001) (Figure 5). versus 20.26%, respectively; difference 20.57%; 95% CI, 21.31
Adjusted LSM change from baseline in SF-36 Vitality to 0.18) (Figure 7D, Table 3). Iron profile parameters analyzed
subscore was 1.59 with roxadustat and 1.15 with placebo according to baseline quartile are shown in Supplemental
(difference 10.44; 95% CI, 20.11 to 0.99; P50.120) and Figure 2. The largest reductions in serum ferritin with roxadu-
in SF-36 Physical Functioning subscore was 0.14 with roxadu- stat treatment were seen in those patients with the highest
stat and 20.39 with placebo (difference 10.52; 95% CI, 0.0 to baseline values.
1.05; nominal P50.051; Supplemental Table 6). Adjusted LSM changes in SBP were similar with roxadustat and
Annual rate of change in eGFR starting from week 4 was placebo (1.24 mmHg versus 2.06 mmHg, respectively; difference
23.70 ml/min per 1.73 m2 with roxadustat and 23.19 ml/min 20.82 mmHg; 95% CI, 21.73 to 0.09). The adjusted LSM changes
per 1.73 m 2 with placebo (difference 20.51 ml/min per in DBP were 10.51 mmHg with roxadustat and 20.32 mmHg
1.73 m 2 ; 95% CI, 21.00 to 20.01; nominal P50.046; with placebo (difference 10.82 mmHg; 95% CI, 0.31 to 1.34).
Supplemental Table 6).
Safety
Subgroup Analysis of the Primary Efficacy End Point Interpretation of AEs was on the basis of the ITT analysis set.
Results from the subgroup analyses were consistent with the The proportions of patients with any AE were similar between
main analysis, including across baseline eGFR and Hb cate- the roxadustat and placebo groups (89.8% versus 88.3%, re-
gories (Figure 6). Hb improvement with roxadustat versus spectively) (Table 4). The most commonly reported AEs by
placebo was similar among the 42% of patients with ferritin preferred term were ESKD, urinary tract infection (UTI),
#100 mg/L and/or TSAT #20% (11.76 g/dl versus 10.43 g/dl, pneumonia, and hypertension (Table 5). Most AEs by pre-
respectively) compared with patients with values above ferred term had similar time at risk–adjusted event rates for
those thresholds (11.71 g/dl versus 10.39 g/dl, respectively) both treatment groups; the only AE with an event rate differ-
(both P,0.001; Figure 4B). ence of .2.0 events per 100 patient-years between roxadustat
and placebo was UTI (6.8 versus 4.2 events per 100 patient-
Exploratory End Points years, respectively) (Table 5).
Mean (SD) baseline hepcidin was 163.16 (116.94) ng/ml for The frequency of serious AEs was similar for roxadustat
roxadustat and 155.45 (111.83) ng/ml for placebo (Table 3). and placebo (57.4% versus 54.4%, respectively) (Table 4).
Compared with baseline, hepcidin at week 24 was reduced The most commonly reported serious AEs by preferred term
cardiovascular/cerebrovascular/thromboembolic history, and geographic region (USA versus ex-USA) as predictor variables. Observed
values up to the EOT visit if treatment was completed; the EOS visit if patient discontinued treatment; or date of withdrawal of consent, last
contact, or death if patient withdrew consent, was lost to follow-up, or died; and imputed values up to death of patient were used to derive the
mean from weeks 28 to 52. (B) ITT analysis set. Iron replete defined as ferritin .100 mg/l and TSAT .20%. (C) ITT analysis set. Week 0 on
the x axis refers to the baseline value. (D) FAS. Hb response was defined as Hb $11.0 g/dl and Hb increase from baseline by $1.0 g/dl
for patients with baseline Hb .8.0 g/dl, or Hb increase from baseline by $2.0 g/dl for those with baseline Hb #8.0 g/dl, at two con-
secutive visits (with available data) separated by at least 5 days during the first 24 weeks of treatment without having received rescue
therapy before Hb response. Statistical analysis was on the basis of the Cochran–Mantel–Haenszel test, adjusting for baseline Hb
(#8, .8 g/dl), baseline eGFR (#30, .30 ml/min per 1.73 m2), cardiovascular/cerebrovascular/thromboembolic history, and geographic
region (USA versus ex-USA). Patients who had discontinued study drug or taken rescue medication before response were considered
nonresponders. (E) ITT analysis set. hsCRP was quantified from available stored biomarker samples obtained at randomization. ULN is
5 mg/l (0.5 mg/dl). Data were analyzed analogously to the primary analysis.
JASN 32: ccc–ccc, 2021 Roxadustat in Nondialysis CKD 9CLINICAL RESEARCH www.jasn.org
A Time-to-first rescue therapy
0.6 Roxadustat (n=1384)
HR 0.26
Placebo (n=1376)
95% CI (0.23, 0.31)
Pwww.jasn.org CLINICAL RESEARCH
Table 2. Secondary efficacy end points
Roxadustat (n51384) Placebo (n51377)
Number (%)/Adjusted Relative Risk/HR/
Number (%)/Adjusted LSM P
End Point LSM (95% CI)/Event Rate Difference in LSM
N (95% CI)/Event Rate per 100 PY n Value
per 100 PY (Total Number Changes (95% CI)a
(Total Number of Yr at Risk)a
of Yr at Risk)a
1. Proportion with Hb response 1371 1055 (77.0) 1357 112 (8.5) 9.12 (7.63 to 10.89) ,0.001
during the first 24 wk of
treatment, %
2. Change from baseline in Hb 213 1.75 (1.58 to 1.92) 198 0.62 (0.44 to 0.80) 1.13 (0.91 to 1.35) ,0.001
averaged over wk 28–52 in
patients with baseline hsCRP
.ULN, g/l
3. Proportion of total time of 1220 0.82 (0.80 to 0.85) 1145 0.33 (0.31 to 0.35) 0.50 (0.47 to 0.52) ,0.001
interpolated Hb values $10
g/dl over wk 28–52, %
4. Proportion of total time of 1220 0.70 (0.68 to 0.72) 1145 0.28 (0.26 to 0.30) 0.42 (0.40 to 0.45) ,0.001
interpolated Hb values
10–12 g/dl over wk 28–52, %
5. Mean change in LDL-C from 1147 214.58 (–16.67 to –12.49) 1133 20.70 (–2.78 to 1.37) 213.88 (–16.37 to ,0.001
baseline to wk 24, mg/dl –11.39)
6. Event rate for first rescue 254 11.90 (2134.88) 574 39.76 (1443.49) 0.26 (0.23 to 0.31) ,0.001
therapy (composite)
7. Event rate for first rescue RBC 176 7.98 (2206.74) 320 19.61 (1631.69) 0.37 (0.30 to 0.44) ,0.001
transfusion
Hb response was defined as Hb $11.0 g/dl and Hb increase from baseline by $1.0 g/dl for patients with baseline Hb .8.0 g/dl, or Hb increase from baseline by
$2.0 g/dl for patients with baseline Hb #8.0 g/dl, at two consecutive visits (with available data) separated by at least 5 d during the first 24 wk of treatment without
having received rescue therapy (RBC transfusion, ESA, or iv iron) before Hb response. PY, patient yr at risk.
a
No. of patients (%) and relative risk (95% CI) are presented for secondary end point 1; adjusted LSM change (95% CI) and difference in LSM changes (95% CI) are
presented for secondary end points 2, 3, 4, and 5; and event rate per 100 patient-yr at risk (total number of yr at risk) and HR (95% CI) are presented for secondary end
points 6 and 7.
were ESKD, pneumonia, and azotemia, although cardiovascu- initiation of dialysis was 10.3% with roxadustat and 6.8%
lar AEs were also observed in this category (Supplemental with placebo (Supplemental Table 9).
Table 7).
In an overview of cardiovascular AEs, the proportion of
roxadustat- and placebo-treated patients with AEs was DISCUSSION
22.8% versus 21.3%, respectively, and with serious AEs was
12.6% versus 11.4%, respectively, in the cardiac disorders sys- The clinical development program for roxadustat for patients
tem organ class (Table 4). The complete listing of serious AEs with anemia of NDD-CKD includes placebo-controlled trials
in the cardiac disorders system organ class is provided in and trials comparing roxadustat with ESA treatment. In this
Supplemental Table 8. large, global, phase 3 study of patients with anemia of NDD-
The likelihood of death was ascertained in two popula- CKD, roxadustat was superior to placebo in increasing Hb.
tions: one that included only patients remaining in the trial Compared with placebo, roxadustat reduced the need for
(excluding deaths after withdrawal of consent) and one that RBC transfusions, iv iron, and ESAs. RBC transfusions are
included public record searches to increase ascertainment of common in patients with NDD-CKD and anemia, have in-
as many deaths as possible during the study period, includ- creased in frequency after US label changes, and carry poten-
ing deaths that occurred after withdrawal of consent but tial risks including infection and allosensitization.12,15,16,40
before EOS (Table 4). Mortality rates for the roxadustat Roxadustat treatment led to a 63% relative risk reduction
and placebo groups with more complete ascertainment compared with placebo, and an absolute risk reduction of
were 9.6 and 8.4 events per 100 patient-years, respectively 11.63 transfusions per 100 patient-years. Similar Hb improve-
(Table 4). ments with roxadustat were observed among all patient
The overall mean (SD) change from baseline in serum po- subpopulations assessed including patients with elevated or
tassium was similar between the roxadustat and placebo normal baseline hsCRP levels. Studies have demonstrated an
groups (10.05 [0.522] mmol/l versus 10.01 [0.541] mmol/ inverse association between the inflammatory marker hsCRP
l, respectively). The proportion of patients with postbaseline and ESA responsiveness.41,42 Similar Hb improvements were
serum potassium concentrations $6.5 mmol/l before observed with roxadustat treatment regardless of baseline iron
JASN 32: ccc–ccc, 2021 Roxadustat in Nondialysis CKD 11CLINICAL RESEARCH www.jasn.org
Roxadustat Placebo LS mean treatment
N N difference (95% Cl)
Age 9 g/dl 869 844 1.26 (1.16, 1.36)
eGFRwww.jasn.org CLINICAL RESEARCH
A 90 Roxadustat (n=1384) Placebo (n=1377)
Mean serum iron (μg/dl)
80
70
60
50
40
30
20
10
0
0 8 16 24 36 52
Week
Roxadustat n= 1384 1295 1246 1220 1147 1112
Placebo n= 1377 1292 1200 1144 1072 1010
B 300 Roxadustat (n=1384) Placebo (n=1377)
Mean serum ferritin (μg/l)
250
200
150
100
50
0
0 8 16 24 36 52
Week
Roxadustat n= 1384 1299 1252 1220 1151 1110
Placebo n= 1377 1289 1202 1146 1073 1005
C 300 Roxadustat (n=1384) Placebo (n=1377)
250
Mean TIBC (μg/dl)
200
150
100
50
0
0 8 16 24 36 52
Week
Roxadustat n= 1384 1289 1233 1218 1133 1112
Placebo n= 1377 1283 1195 1138 1065 1007
D 35 Roxadustat (n=1384) Placebo (n=1377)
30
Mean TSAT (%)
25
20
15
10
5
0
0 8 16 24 36 52
Week
Roxadustat n= 1384 1283 1226 1215 1127 1108
Placebo n= 1375 1279 1185 1125 1055 1003
Figure 7. Serum iron parameters by visit. (A) Iron; (B) ferritin; (C) TIBC; (D) TSAT (ITT analysis set). Error bars are 95% CIs. Baseline is
defined as the last measurement before randomization. 95% CI of the mean is on the basis of the normal distribution.
JASN 32: ccc–ccc, 2021 Roxadustat in Nondialysis CKD 13CLINICAL RESEARCH www.jasn.org
Table 4. AEs summary (ITT analysis set)a
Roxadustat (n51384) Placebo (n51377)
AE Category Patients with Event Rate Patients with Event Rate
% %
Event (per 100 PY)b Event (per 100 PY)b
Any AE 1243 89.8 182.9 1216 88.3 171.9
Any serious AE (including events with an outcome of 795 57.4 42.1 749 54.4 40.0
death)
Any AE with an outcome of death 262 18.9 9.3 213 15.5 7.8
All-cause mortalityc 284 20.5 9.6 245 17.8 8.4
Any AE in the cardiac disorders SOCd 316 22.8 12.7 293 21.3 12.0
Any serious AE in the cardiac disorders SOCd 174 12.6 6.5 157 11.4 6.0
Patients with multiple events in the same category were counted only once in that category. Patients with events in more than one category were counted once in
each of those categories. PY, patient yr at risk; SOC, system organ class.
a
Included AEs with an onset date on or after the date of randomization and up to and including the EOS visit; or date of last contact or withdrawal of consent, if
before the EOS visit.
b
Calculated as [No. of patients with AEs divided by (the total number of days at risk for that AE across all patients in given group divided by 365.25)] 3 100.
c
Includes deaths from public record searches.
d
Analyses performed post hoc.
increased serum iron levels and serum TIBC. The observed OLYMPUS was neither individually powered to assess nor
reduction in serum ferritin with roxadustat has been report- prospectively planned as a standalone study to determine car-
ed previously,37–39,44 and in this study was most prominent diovascular safety and mortality risk with roxadustat. The
in patients with the highest baseline values. Overall, the findings will be further assessed in the fully powered analysis
reduction in hepcidin, increased serum iron, and, in partic- of the pooled population of the phase 3, placebo-controlled
ular, increased TIBC with roxadustat support improved roxadustat NDD-CKD studies.
absorption, mobilization, and utilization of iron for eryth- Some safety data were difficult to interpret in the setting
ropoiesis in roxadustat-treated patients, particularly in the of differential study drug discontinuation. For example, a
setting of the increase in Hb from baseline regardless of numerically greater number of patients with roxadustat
baseline iron repletion status and the observed decreased than placebo had $1 postbaseline serum potassium con-
need for iv iron. centration of $6.5 mmol/l. Because patients who discon-
Observational studies have shown that patients with ane- tinued study drug prematurely and remained in the study
mia of NDD-CKD frequently have a high incidence of adverse with modified follow-up often did not continue central lab-
clinical outcomes.9 In OLYMPUS, the safety profile of roxa- oratory testing, OT data were used to assess serum potas-
dustat was comparable to placebo, as was seen in previous sium outlier values. However, these data are confounded by
placebo-controlled roxadustat studies.37–39 More patients re- patients at higher risk for hyperkalemia being more likely to
ceiving roxadustat who had low eGFR or initiated dialysis, remain on roxadustat than placebo. Notably, placebo-
which are associated with higher risk of death and cardiovas- treated patients with baseline eGFR ,15 ml/min per
cular events,6–8 remained on roxadustat versus placebo. To 1.73 m2, which is associated with an approximate twofold
minimize potential bias due to differential dropout, the ITT and fivefold increased risk of hyperkalemia versus eGFR
analysis set and time at risk–adjusted event rates were utilized. 15–29 ml/min per 1.73 m2 and 30–59 ml/min per 1.73 m2,
Event rates of UTI and pneumonia appeared higher for rox- respectively,45 were approximately 2.5-times more likely to
adustat than placebo, although there is no clear biologic mech- prematurely discontinue study drug versus roxadustat-
anism for these observations. treated patients. Therefore, and given the overall severe
Because cardiovascular risk is increased in this patient pop- CKD of the studied population, mean changes in serum
ulation, event rates for AEs and serious AEs in the cardiac potassium between treatments are meaningful to assess
disorders system organ class were assessed. Analysis of cardio- the potential effects of roxadustat. Overall, mean changes
vascular events is limited by the size of the study and will be in serum potassium from baseline between treatments did
analyzed using a pooled analysis of multiple roxadustat stud- not differ, suggesting that roxadustat does not affect serum
ies; however, rates were generally comparable for roxadustat potassium. Similarly, numeric decreases and increases of
and placebo, both overall and for individual cardiac serious ,1 mmHg for roxadustat versus placebo in SBP and DBP,
AEs. Importantly, OLYMPUS allowed for a prospective and respectively, suggest that roxadustat does not meaningfully
complete ascertainment of patient mortality using public affect BP values.
record searches, even after withdrawal of consent, and vital For clinical trials among patients with anemia of NDD-
status was confirmed in .99% of patients. These results CKD, such as the Trial to Reduce Cardiovascular Events with
showed that mortality rates between roxadustat and placebo AranespÒ Therapy (TREAT), the use of a placebo control has
were 9.6 and 8.4 events per 100 patient-years, respectively. been considered to provide greater evidentiary power than use
14 JASN JASN 32: ccc–ccc, 2021www.jasn.org CLINICAL RESEARCH
Table 5. Most common AEs ($5%) by preferred term (ITT analysis set)a
Roxadustat (n51384) Placebo (n51377)
Preferred Term Event Rate Event Rate
Patients with Event % Patients with Event %
(per 100 PY)b (per 100 PY)b
ESKD 290 21.0 11.7 282 20.5 11.8
UTI 177 12.8 6.8 110 8.0 4.2
Pneumonia 165 11.9 6.2 130 9.4 4.9
Hypertension 159 11.5 6.1 125 9.1 4.8
Edema peripheral 149 10.8 5.7 111 8.1 4.3
Diarrhea 144 10.4 5.5 119 8.6 4.6
Nausea 125 9.0 4.8 104 7.6 4.1
Hyperkalemia 118 8.5 4.4 95 6.9 3.6
Cough 105 7.6 3.9 69 5.0 2.6
Viral upper respiratory tract infection 101 7.3 3.8 106 7.7 4.1
Upper respiratory tract infection 96 6.9 3.6 76 5.5 2.9
Headache 94 6.8 3.5 82 6.0 3.1
Constipation 92 6.6 3.4 88 6.4 3.4
Hypoglycemia 91 6.6 3.4 73 5.3 2.8
Gastritis 81 5.9 3.0 72 5.2 2.7
Azotemia 80 5.8 2.9 73 5.3 2.7
Dyspnea 78 5.6 2.9 74 5.4 2.8
Bronchitis 78 5.6 2.9 73 5.3 2.8
Vomiting 78 5.6 2.9 69 5.0 2.6
Dizziness 77 5.6 2.9 87 6.3 3.4
AKI 75 5.4 2.7 47 3.4 1.7
Asthenia 74 5.3 2.7 75 5.4 2.8
Arthralgia 73 5.3 2.7 54 3.9 2.0
Back pain 72 5.2 2.6 57 4.1 2.1
Pruritus 68 4.9 2.5 80 5.8 3.1
Edema 66 4.8 2.4 69 5.0 2.6
Percentages were on the basis of the No. of patients in the ITT analysis set in that treatment arm. PY, patient yr at risk.
a
Included AEs with an onset date on or after the date of randomization and up to and including the EOS visit; or date of last contact or withdrawal of consent, if
before the EOS visit.
b
Calculated as [No. of patients with AEs divided by (the total No. of days at risk for that AE across all patients in given group divided by 365.25)] 3 100.
of an active control and to allow valid assessment of safety and DOLOMITES, 616 patients with NDD-CKD stages 3–5 and
efficacy.17,46 For studying efficacy, the placebo control means anemia were randomized to receive roxadustat (n5323) or
that roxadustat was assessed against a comparator not expec- darbepoetin alfa (n5293). Among these patients, roxadustat
ted to increase Hb or prevent RBC transfusion. For studying was noninferior to darbepoetin alfa in the correction of Hb
safety, the use of placebo allows a rigorous assessment of non- levels (Hb response rates: roxadustat 89.5% versus darbepoe-
inferiority for cardiovascular safety via separate pooled anal- tin alfa 78.0%; difference: 11.5%; 95% CI, 5.7% to 17.4%)
yses of the phase 3 NDD-CKD studies, and comparison with a during the first 24 weeks of treatment and safety profiles
therapy without known AEs. Although ESA is also a valid were comparable.
comparator, interpretation of safety against an active compar- Another reason that placebo might be considered is that
ator with reported cardiovascular safety concerns when dosed several reports estimate that many patients with anemia of
to achieve normal or near normal Hb levels19–21 can be com- NDD-CKD in the real world are untreated4,5,11,25–30 and
plex. Boxed warnings in the US product labels of approved ESA use is relatively uncommon in treated patients.11,28–30
ESAs state that no trial has identified an Hb target level, ESA In particular, a US study from 2018 showed that approxi-
dose, or dosing strategy that does not increase the risks of mately 11%–13% of patients with anemia of NDD-CKD
death and other cardiovascular events.22,23 The lack of an ac- received an ESA; of these, ,5% received ESA treatment
tive comparator in OLYMPUS precludes direct comparison of consistently.28 This likely reflects problems with affordabil-
roxadustat with ESAs. However, the roxadustat clinical devel- ity, physical access to injectable therapy, and interpretation
opment program comprises several placebo- and active- of current guideline recommendations including the rec-
controlled phase 3 clinical studies, and the efficacy and safety ommendation that ESAs are used intermittently and to pre-
of roxadustat compared with ESA among patients with anemia vent RBC transfusions, given their risk of cardiovascular
of NDD-CKD have been evaluated in the completed phase 3, events.19–21 The high discontinuation rate and need for res-
active-controlled DOLOMITES study (NCT02021318). In cue therapy in the placebo arm in OLYMPUS support
JASN 32: ccc–ccc, 2021 Roxadustat in Nondialysis CKD 15CLINICAL RESEARCH www.jasn.org
the need for effective anemia treatment in patients with OLYMPUS had limitations. Study personnel at local study
NDD-CKD. sites could not be blinded to Hb values; therefore, Hb increases
The OLYMPUS study has several strengths that further our could have in some cases been considered by patients and
knowledge of roxadustat from the previous phase 3 NDD- physicians to be suggestive of treatment allocation and poten-
CKD study conducted in China.38 The OLYMPUS study had tially affected continuation in the study or reporting of AEs.
a longer follow-up period than that previously assessed and No assessment of site personnel or patients was performed to
enrolled a larger and more diverse patient population, which is examine perception of treatment allocation. Median expo-
important for the generalizability of the data. This large pa- sures of 20.80 and 14.57 months in the roxadustat and placebo
tient population allowed for the analysis of patient subgroups, groups, respectively, do not allow for the assessment of rox-
such as by baseline eGFR and Hb categories and iron repletion adustat in this population over a time period longer than the
status, and additional secondary analyses than were possible maximum treatment duration of 4 years.
in earlier studies. Another strength of OLYMPUS is that, In conclusion, oral roxadustat was more effective than
compared with the Correction of Hemogloblin and Out- placebo in correcting anemia, reduced the risk of RBC trans-
comes in Renal Insufficiency (CHOIR) and TREAT ESA fusions, and had comparable safety to placebo in this interna-
studies,20,21 OLYMPUS enrolled a broader, real-world pa- tional, double-blind, phase 3 study. Roxadustat was effective
tient population. For instance, baseline Hb and eGFR were in a broad range of patients with NDD-CKD, including pa-
lower in patients in OLYMPUS (mean: 9.1 g/dl and approx- tients with inflammation, and patients with more advanced
imately 20 ml/min per 1.73 m 2 ) compared with CHOIR CKD (lower baseline eGFR), more severe anemia (lower base-
(mean: 10.1 g/dl and 27 ml/min per 1.73 m2) and TREAT line Hb levels), and lower iron stores (low baseline ferritin and
(median: 10.5 g/dl and 34 ml/min per 1.73 m2).20,21 Evi- TSAT) than those included in historical NDD-CKD trials with
dence from the CKD Outcomes and Practice Patterns Study ESAs. The findings support anemia treatment using roxadu-
suggests that up to 45% of patients with NDD-CKD and stat, an oral medication that can be administered in the home
Hb ,10 g/dl have stage 5 CKD, confirming the clinical ap- setting and without requirement for routine iv iron supple-
plicability of the OLYMPUS study.4 mentation, which may simplify anemia treatment for patients
Although the inclusion of patients with severe disease was with NDD-CKD.
an advantage of OLYMPUS, it also affected data interpreta-
tion. The rate of study drug discontinuation was relatively high
in both treatment arms but higher in the placebo group. AEs DISCLOSURES
were an uncommon reason for study drug discontinuation in
both treatment groups. Post hoc analyses identified low eGFR M.A. El-Shahawy reports ownership interest in Paramount Hope Dialysis
and initiation of dialysis after randomization as contributors Center, East LA Dialysis Center; research funding from AstraZeneca, Pfizer,
to study drug discontinuation overall and to differences in Bayer, UCB, and Sanofi; honoraria from AstraZeneca; being a scientific advi-
sor or membership from AstraZeneca and Bayer; and speakers bureau from
study drug discontinuation by treatment group. Although AstraZeneca. S. Fishbane reports receiving research support and consulting
the study allowed continuation of roxadustat after dialysis ini- fees from AstraZeneca; consultancy agreements from Akebia, Cara Therapeu-
tiation, study drug discontinuations may have been driven by tics, and FibroGen; research funding from Cara, Gilead, and Merck; and hon-
administrative challenges relating to standardized processes of oraria from Akebia and AstraZeneca. L. Frison, N.J. Guzman, and D.J. Little
anemia treatment at dialysis centers, avoidance of the added are employees of AstraZeneca. N.J. Guzman and D.J. Little also report owner-
ship interest in AstraZeneca. M.T. Houser is employed by and has ownership
complexity of experimental drug administration, and patients interest in AstraZeneca. R. Pecoits-Filho reports receiving consulting fees paid
who may require hospitalization and have other medical com- to his employer from Akebia and AstraZeneca for participation in advisory
plexities making strict adherence to the protocol difficult. boards and educational events, and research grants from Fresenius Medical
Similar to TREAT,21 patients in OLYMPUS who discontin- Care. R. Pecoits-Filho also reports consultancy agreements with Rethrophin;
ued study drug (but did not withdraw from study) were being a scientific advisor or member with the Kidney Disease: Improving
Global Outcomes Executive Board, International Society of Nephrology Ex-
followed for as long as possible and remained in the ITT ecutive Board, and Standardised Outcomes in Nephrology Executive Com-
analysis until study closure/withdrawal, using follow-up mittee; serving on editorial boards for American Journal of Kidney Diseases,
options designed, in part, to minimize withdrawal of con- Blood Purification, Nephrology, Peritoneal Dialysis International, Hemodialysis
sent. The rate of study withdrawal in OLYMPUS was low International, and the Brazilian Journal of Nephrology; and serving on the
speakers bureau with AstraZeneca and Novo Nordisk. P.E. Pergola reports
(7.8%) compared with the ESA studies CHOIR (38%) and
receiving research support and consulting fees from AstraZeneca. P.E. Pergola
PEARL (approximately 24%), 20,47 and vital status at the also reports consultancy agreements with Akebia Therapeutics, Ardelyx,
end of the study was confirmed in .99% of randomized Bayer, Corvidia Therapeutics, Gilead Sciences, Reata Pharmaceuticals, and
patients. However, although the ITT population allowed for a Tricida; reports ownership interest in Unicycive Therapeutics; and reports
more balanced evaluation of safety, this population could also receiving research funding as principal investigator or subinvestigator on mul-
contain reporting bias for AEs due to the higher withdrawal of tiple clinical trials (the contracts are with his practice, not individual); being a
scientific advisor or member with Ardelyx and Unicycive; and serving on the
consent in placebo patients and possible under-reporting of speakers bureau with AstraZeneca. B.P. Van reports receiving research support
some events (e.g., nonserious AEs) in patients with modified and consulting fees from AstraZeneca. B.P. Van also reports honoraria from
post-treatment follow-up. Astellas, AstraZeneca, Boehringer Ingelheim, DiethelmKellerSiberHegner,
16 JASN JASN 32: ccc–ccc, 2021www.jasn.org CLINICAL RESEARCH
Kalbe International, Nanogen (Vietnam), Otsuka, Pfizer, Servier, and Tedis; Treatment compliance.
being a scientific advisor or member with Nguyen Tri Phuong University Supplemental Table 1. Statistical analyses of secondary efficacy end points.
Hospital (Vietnam); and serving on the speakers bureau with Astellas, Astra- Supplemental Table 2. Statistical analyses of exploratory efficacy end points.
Zeneca, Boehringer Ingelheim, DKSH, Kalbe International, Otsuka, Pfizer, Supplemental Table 3. Key medications taken during study treatment.
Sanofi, Servier, and Tedis. Supplemental Table 4. Exposure by dose.
Supplemental Table 5. Proportions of patients with at least one dose re-
duction or increase during treatment.
Supplemental Table 6. Secondary efficacy end points.
FUNDING Supplemental Table 7. Most common serious adverse events ($1%) by
system organ class and preferred term (ITT analysis set)a.
This study was supported by AstraZeneca. Supplemental Table 8. Serious adverse events within the cardiac disorders
system organ class, by preferred term (ITT analysis set)a.
Supplemental Table 9. Serum potassium treatment-emergent laboratory
values (OT128 analysis set).
ACKNOWLEDGMENTS Supplemental Figure 1. Time to premature study drug discontinuation by
treatment arm and baseline eGFR (OT128 analysis set).
The authors thank Dr. Mary Beth DeYoung, Dr. James Sloand, and Dr. Lynda Supplemental Figure 2. Serum iron parameters by visit, according to base-
Szczech for their review of the data and manuscript drafts. Medical writing line quartile. (A) Iron; (B) ferritin; (C) TIBC; (D) TSAT (ITT analysis set).
support was provided by Mr. Shaun W. Foley and Dr. Maria Alfaradhi, and
editorial support was provided by Ms. Rachael Cazaly, all of Core Medica
(London, United Kingdom), supported by AstraZeneca according to Good
Publication Practice guidelines. REFERENCES
The Sponsor was involved in the study design; collection, analysis, and
interpretation of data; and data checking of information provided in the 1. Stauffer ME, Fan T: Prevalence of anemia in chronic kidney disease in
manuscript. However, ultimate responsibility for opinions, conclusions, and the United States. PLoS One 9: e84943, 2014
data interpretation lies with the authors. All authors were involved in the 2. McClellan W, Aronoff SL, Bolton WK, Hood S, Lorber DL, Tang KL, et al.:
drafting and critical revision of the manuscript. All authors approved the final The prevalence of anemia in patients with chronic kidney disease. Curr
version of the manuscript. Roxadustat is being developed in collaboration Med Res Opin 20: 1501–1510, 2004
between FibroGen, Astellas, and AstraZeneca. 3. Jungers PY, Robino C, Choukroun G, Nguyen-Khoa T, Massy ZA,
Dr. Dustin J. Little, Dr. Lars Frison, Dr. Mark T. Houser, Dr. Nicolas Jungers P: Incidence of anaemia, and use of epoetin therapy in pre-
J. Guzman, Dr. Steven Fishbane, and Dr. Bui Pham Van contributed to the dialysis patients: A prospective study in 403 patients. Nephrol Dial
study design; Dr. Steven Fishbane, Dr. Bui Pham Van, Dr. Mohamed A. El- Transplant 17: 1621–1627, 2002
Shahawy, Dr. Roberto Pecoits-Filho, and Dr. Pablo E. Pergola collected data for 4. Wong MMY, Tu C, Li Y, Perlman RL, Pecoits-Filho R, Lopes AA, et al.;
the study; and all authors contributed to the analysis and interpretation of the CKDopps Investigators: Anemia and iron deficiency among chronic
data, critically reviewed the manuscript, approved the final version, and accept kidney disease Stages 3-5ND patients in the Chronic Kidney Disease
accountability for the overall work. Outcomes and Practice Patterns Study: Often unmeasured, variably
treated. Clin Kidney J 13: 613–624, 2019
5. Cases-Amenós A, Martínez-Castelao A, Fort-Ros J, Bonal-Bastons J,
Ruiz MP, Vallés-Prats M, et al.: Prevalence of anaemia and its clinical
DATA SHARING STATEMENT management in patients with stages 3-5 chronic kidney disease not on
dialysis in Catalonia: MICENAS I study. Nefrologia 34: 189–198, 2014
Data underlying the findings described in this manuscript can be requested in 6. Thorp ML, Johnson ES, Yang X, Petrik AF, Platt R, Smith DH: Effect of
accordance with AstraZeneca’s data sharing policy, described at https:// anaemia on mortality, cardiovascular hospitalizations and end-stage
astrazenecagroup-dt.pharmacm.com/DT/Home by accessing www.vivli.org. renal disease among patients with chronic kidney disease. Nephrol-
ogy (Carlton) 14: 240–246, 2009
7. Locatelli F, Pisoni RL, Combe C, Bommer J, Andreucci VE, Piera L, et al.:
Anaemia in haemodialysis patients of five European countries: Asso-
SUPPLEMENTAL MATERIAL ciation with morbidity and mortality in the Dialysis Outcomes and
Practice Patterns Study (DOPPS). Nephrol Dial Transplant 19: 121–132,
This article contains the following supplemental material online at http:// 2004
jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2020081150/-/ 8. Robinson BM, Joffe MM, Berns JS, Pisoni RL, Port FK, Feldman HI:
DCSupplemental. Anemia and mortality in hemodialysis patients: Accounting for mor-
Contents. bidity and treatment variables updated over time. Kidney Int 68:
Study locations and investigators. 2323–2330, 2005
Inclusion criteria. 9. Toft G, Heide-Jørgensen U, van Haalen H, James G, Hedman K, Birn H,
Exclusion criteria. et al.: Anemia and clinical outcomes in patients with non-dialysis de-
Dose adjustment algorithm. pendent or dialysis dependent severe chronic kidney disease: A Danish
Dose increases and reductions. population-based study. J Nephrol 33: 147–156, 2020
Dose adjustment for excessive erythropoiesis. 10. van Haalen H, Jackson J, Spinowitz B, Milligan G, Moon R: Impact of
Prohibited medication. chronic kidney disease and anemia on health-related quality of life and
Rescue medication. work productivity: Analysis of multinational real-world data. BMC
Intravenous (iv) iron. Nephrol 21: 88, 2020
RBC transfusion. 11. Hoshino J, Muenz D, Zee J, Sukul N, Speyer E, Guedes M, et al.:
Erythropoiesis-stimulating agents (ESAs). CKDopps Investigators: Associations of hemoglobin levels with health-
Missing at random–based multiple imputation analysis of covariance. related quality of life, physical activity, and clinical outcomes in persons
Efficacy subgroup analyses. with stage 3-5 nondialysis CKD. J Ren Nutr 30: 404–414, 2020
JASN 32: ccc–ccc, 2021 Roxadustat in Nondialysis CKD 17You can also read