New Determinants for Gallstone Disease? - Daniel Mønsted Shabanzadeh
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PHD THESIS DANISH MEDICAL JOURNAL
New Determinants for Gallstone Disease?
Daniel Mønsted Shabanzadeh
analyzed the composition of surgically removed gallstones indi-
This review has been accepted as a thesis together with four previously published cate that cholesterol gallstones have been the dominating cause
papers by University of Copenhagen 30th of June 2017 and defended on 24th of No- of clinical gallstone disease for long. Studies from the 1970’ies in-
vember 2017 cluding x-ray and chromatography analyses of gallstones show
Tutors: Lars Tue Sørensen and Torben Jørgensen that cholesterol constituted 89% of the weighted occurrence in
Swedish populations(11, 12). In a study from 1987-88, cholesterol
Official opponents: Henry Völzke and Søren Paaske Johnsen stones with a cholesterol content above 70% or mixed stones
Correspondence: Daniel Mønsted Shabanzadeh, Digestive Disease Center, Bispebjerg
with cholesterol contents of 20-69% at chromatography ac-
Hospital, Bispebjerg Bakke 23, 2400 Copenhagen NV counted for 77% of gallstones identified at cholecystectomy or
autopsy in a Danish population(13). In a more recent study in a
E-mail: daniel.moensted.shabanzadeh@regionh.dk German clinical population, cholesterol was the main constituent
in 93.3% and pigment was in 5.5% of gallstones at spectrome-
try(14). Due to the dominance of cholesterol gallstones in the
Dan Med J 2018;65(2):B5438 western countries, most of the determinants for gallstone disease
identified in epidemiological studies are assumed to apply to cho-
lesterol or mixed stones(10).
THE FOUR STUDIES INCLUDED IN THIS THESIS
Pigment stones contain calcium bilirubinate as the main
I. Shabanzadeh DM, Sorensen LT, Jorgensen T. Determinants
component and can further be divided into black and brown
for gallstone formation - a new data cohort study and a sys-
stones(15). Black pigment stones may be associated with physio-
tematic review with meta-analysis. Scand J Gastroenterol
logical conditions including hemolysis and increased production
2016;51:1239-48.(1)
of unconjugated bilirubin(16) such as clinical conditions of hepatic
II. Shabanzadeh DM, Holmboe SA, Sorensen LT, Linneberg A,
origin like cirrhosis(17) or of pre-hepatic origin like spherocytosis,
Andersson A-M, Jorgensen T. Are incident gallstones associ-
sickle cell disease, thalassemia, and malaria(15). Higher preva-
ated to sex-dependent changes with age? A cohort study.
lence of black pigment than cholesterol gallstones are found in
Andrology 2017;5:931-8.(2)
developing countries and in Asian populations(18-23). Although
III. Shabanzadeh DM, Jorgensen T, Linneberg A, Sorensen LT,
black pigment gallstones still are highly prevalent in Asia, the
Skaaby T. Vitamin D and gallstone disease-A population-
prevalence of cholesterol gallstones has been ever rising since the
based study. Endocrine 2016;54:818-25.(3)
late 1960’ies – a trend ascribed to a westernized lifestyle(22).
IV. Shabanzadeh DM, Skaaby T, Sorensen LT, Eugen-Olsen J,
Brown pigment stones are found in the hepatic ducts and be-
Jorgensen T. Metabolic biomarkers and gallstone disease - a
lieved to be caused by biliary stasis and cholangitis(24-27) due to
population-based study. Scand J Gastroenterol
anaerobic and aerobic bacterial infection, parasitic infestations,
2017;52:1270-7.(4)
or bile seeking worms(15). They contain more cholesterol and
fatty acids than black pigment stones(25, 26, 28). Brown pigment
BACKGROUND
stones are uncommon in Western countries and reported with
Gallstones are abnormal stone masses formed in the gallbladder
higher prevalence in Asia(18, 29, 30).
or the intrahepatic bile ducts and infrequently also migrate to the
The true presence or absence of gallstones can only be con-
common bile duct or the intestines(5, 6). The presence of gall-
firmed through surgery or autopsy. However, non-invasive radio-
stones in humans has been identified in the mummy of an Egyp-
logical examinations have been developed in order to examine
tian priestess dated back to about 1500 BCE(7). The first observa-
patients with suspected gallstone disease(31). Oral cholecys-
tion of gallstones in humans was reported by the Florentine
tography was the examination of choice in the pre-ultrasound
physician Antonio Benivenius towards the end of the fifteenths
era, but somewhat unpractical since it required two days prepara-
century at an autopsy of a lady that had deceased with abdominal
tion, ingestion of tablets, exposure to radiation, and the cholecys-
pain(8). Historical writings and autopsy findings indicate that
togram was often inconclusive due to failed visualization of the
Catherine the Great of Russia and the emperor Alexander the
gallbladder(32, 33). When comparing detection of gallstones at
Great both suffered from gallstone disease with death of the lat-
surgery with radiology, sensitivity and specificity for oral cholecys-
ter ascribed to acute cholecystitis(7).
tography is 90% and 95%, computed tomography is 79% and 99%,
Gallstones are classified by their composition of major con-
and for ultrasound is 97% and 95%, respectively(31). The superi-
stituents into pure cholesterol stones, pure pigment stones or
ority of gallstone detection with ultrasound has been reproduced
mixed stones(9). Cholesterol gallstones have been estimated to
in the morbidly obese patients with sensitivity 91% and specificity
account for 75-90% of gallstones prevalence in Western coun-
100%(34). Inter-observer agreement for both detection and ex-
tries(10). A number of studies throughout the decades that have
clusion of gallstone disease is good (Kappa scores 0.78 and 0.73,
DANISH MEDICAL JOURNAL 1respectively) (35). Due to the many advantages, ultrasound exam- ered only secondary to gallstone formation but could change gall-
ination has become the preferred non-invasive examination for stone size, appearance, and composition with a coating of calcium
gallstone disease. and pigment causing formation of mixed or pigment gallstones.
Gallstone disease prevalence was traditionally determined Bile cholesterol and its crystallization were central to all of
through autopsy studies, but the selective approach of autopsies these primary theories. The chemical properties of bile and the
performed caused biased estimates(36). Truer estimations of gall- transport function of the gallbladder mucosa earned much focus
stone disease prevalence in larger populations became possible in the research performed during the following decades. It be-
with the introduction of real-time ultrasound throughout 1980- came evident that bile salts and phospholipids were necessary to
90’ies which caused a wave of general population screening stud- keep cholesterol soluble(44-46). A cholesterol-rich diet was found
ies(10, 37). Gallstone disease prevalence was found to have a sig- correlated with cholesterol gallstone formation in animal models
nificant ethno-geographic variation with the highest in the Native – such as in prairie dogs(47) – and increased cholesterol excretion
American Indian populations and the lowest in Black Africans(10, to bile was observed in humans with cholesterol gallstones(48,
37). In Western cultured countries of Europe and the US, interme- 49). Through continuous chemical experiments with bile, the pri-
diate high overall prevalence of about 10-20% have been found mary focus became the solubility of bile cholesterol relative to
with the highest prevalence in Northern Europe. Female sex and the other two bile constituents including phospholipids and bile
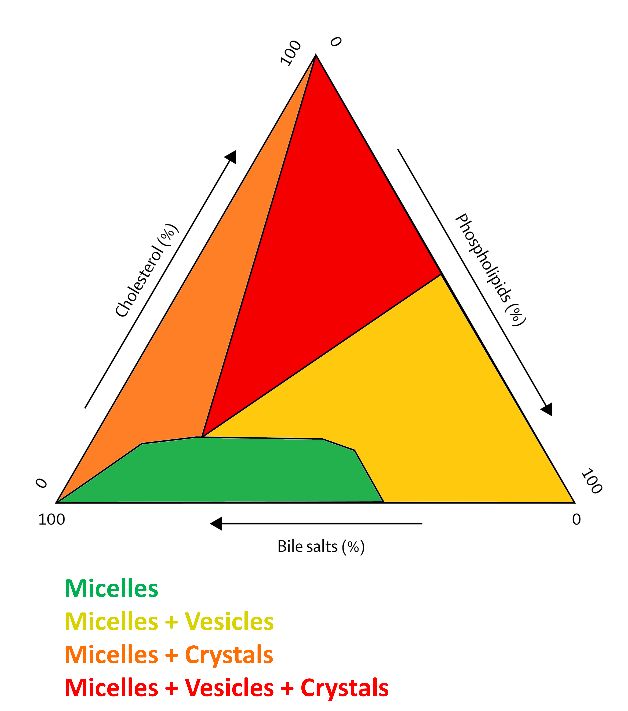
higher age were significantly associated with gallstone disease in salts produced by hepatocytes. Based on in vitro studies, a ter-
all countries(37, 38). nary diagram was developed, which defined the physical state of
bile cholesterol into an ascending order on its way to cholesterol
Mechanisms of gallstone formation crystallization which included 1. micelles (liquid), 2. vesicles (liq-
The very first theories about gallstone formation were based on uid crystals), and 3. crystals(50) (Figure 1). The ternary diagram
chemical studies of ox bile. Thudichum (1863) left ox bile to de- has since been reproduced in several experimental models includ-
compose for years and suggested the acidified bile as the neces- ing human bile(51-53) and constitutes the theory of bile choles-
sary environment for gallstone formation(39). He found that hu- terol supersaturation, which still is believed to be the leading
man bile was rich in cholesterol and he theorized that the acid of mechanism for cholesterol gallstone formation.
putrefaction would set free cholesterol to crystallize and deposit
upon any particle that would happen to be within easy dis-
tance(39). During the following decades, the composition and ap-
pearance of the human gallstone and its central nucleus were
studied and more complex theories of gallstone formation were
suggested. In 1892, Naunyn theorized cholesterol gallstone for-
mation to be a disease of the gallbladder caused by a local bacte-
rial infection(40). This gallbladder wall infection would cause a
desquamation of epithelium with the waste serving as the pri-
mary source of bile cholesterol and forming a pultaceous mass
with primary cholesterol crystallization occurring from the central
nucleus or secondarily occurring through an infiltration of bile
cholesterol. Bile stasis was also emphasized as part of the gall-
stone formation process(40). During the coming century, conflict-
ing mechanisms were suggested. Boysen (1900) and Rovsing
(1924) emphasized the pigment gallstone formation and the im-
portance of the black pigmented nucleus. They thought pigment
stones were the product of a disease in the hepatic ducts under
aseptic conditions which was in conflict with Naunyn’s theory of
infection. Once the pigment nucleus reached the gallbladder, the
stone would grow through infiltration and crystallization of cho-
lesterol in layers, through a process where the pigment nucleus
was possibly dissolved which would explain the presence of cho- Figure 1: The ternary diagram defining the physical state of bile
lesterol stones with little or no pigment(41, 42). Aschoff and Bac- cholesterol
meister (1909) addressed the existing controversies through re-
view of literature and through performing a number of clarifying The enterohepatic circulation of bile salts also involves im-
experimental studies with human bile. They concluded that bile portant mechanisms contributing to cholesterol gallstone for-
stasis was the most important mechanism of gallstone for- mation. Hepatic bile salts such as cholate and chenodeoxycholate
mation(43). Bile stasis was defined as a mechanical obstruction of are synthesized from cholesterol in hepatocytes under normal
the physiological bile drainage such as tight female clothing, preg- physiological conditions(6). Secondary bile salts such as deoxy-
nancy, altered anatomy, or intra-abdominal pathologies such as cholate and lithocholate are produced by fecal microbiota con-
appendicitis or tumors. The stasis would cause a higher bile pres- taining the enzyme 7α-dehydroxylase, through a degradation pro-
sure, with changes in the gallbladder wall including a thickened cess of hepatic bile salts in the large bowel, where they are
muscular layer, deposition of lipids, and an infiltration of lympho- reabsorbed to the bile pool with the enterohepatic circulation(6).
cytes. Bile cholesterol was considered a product of liver metabo- Both secondary bile salts and the fecal microbiota producing
lism which also could be enhanced through a number of altered them are found in high amounts in persons with gallstone disease
physiological conditions. Infection of the gallbladder was consid- compared with gallstone free controls(54-58). When compared to
DANISH MEDICAL JOURNAL 2the primary hepatic bile salts, the secondary bile salts have in- and at follow-up. Only a few cohort studies have explored inci-
verse functions in the formation of gallstones through being hy- dent gallstone disease through ultrasound examinations of gen-
drophobic, increasing bile cholesterol saturation, increasing cho- eral populations, and only few determinants have been identi-
lesterol in vesicles, and thereby promoting cholesterol fied(79, 95-100). Such studies are needed in order to identify
crystallization in gallbladder bile(59). A slower orocecal transit determinants of gallstone disease in order to improve future pre-
and slower large bowel transit are contributing mechanisms to an vention or treatment of this highly prevalent disease.
increased absorption of fecal secondary bile salts to the enterohe-
patic circulation during gallstone disease formation(56, 60). Definitions of gallstone disease in thesis
Impaired gallbladder motor function is the third mechanism For the remaining part of this PhD thesis, the term screen-de-
contributing to the formation of cholesterol gallstones(61). Under tected gallstones refers to ultrasound detected gallstones when
normal physiological conditions, gallbladder contractions are screening an entire population, cholecystectomy refers to the sur-
stimulated by cholecystokinin, a hormone released by the duode- gical removal of the gallbladder already performed at the time of
num as a response to food ingestion. Whether impaired gallblad- screening, and screen-detected gallstone disease is defined as the
der motor function causes bile stasis and cholesterol crystalliza- composite definition for gallstones and cholecystectomy. Clinical
tion or whether it is a secondary process to cholesterol gallstone disease as defined above is characterized by not being a
crystallization in gallbladder wall is debatable(61). result of a systematic screening for gallstones of an entire popula-
tion. Gallstone disease detected in cohort studies will be defined
The quest for gallstone disease determinants as incident and if detected in cross-sectional studies will be de-
The “female, fat, fair, fertile, and forty year old,” patient that fined as prevalent.
sometimes also is “flatulent” and “flabby” has been the subject of
the five or seven “F” clinical stereotype for gallstone disease. AIMS
However, this clinical aphorism is not based on empirical re- The overall aim of the PhD thesis was to investigate new determi-
search. Following the initial autopsy studies for assessment of nants for screen-detected gallstone disease assessed through ul-
gallstone disease prevalence, case-control studies were some of trasound examination in a Danish general population sample.
the first to explore possible differences in risk factors for gallstone Specifically, the thesis explored the following objectives:
carriers (cases) and non-carriers (controls)(62-65). However, most
of these studies suffer from inadequate sample size, and compa- • determinants of incident gallstone disease in the study popu-
rability was hampered by unrepresentative controls, causing se- lation and in other cohort studies of general populations in-
lection biased and confounded estimates of association(38). The cluding ultrasound screening
Framingham Heart Study began in 1948 and started a new tradi- • whether sex-dependent changes in determinants over a dec-
tion for studying cardiovascular disease etiology through an epi- ade determined incident gallstone disease
demiological approach in larger general populations. A decade • whether circulating levels of vitamin D or determinants
later, the Framingham study also included the study of gallstone thereof were associated with gallstone disease prevalence
disease epidemiology(66). The impact of cardiovascular disease • if genetic susceptibility or metabolic changes of obesity such
determinants for gallstone disease was explored with the wave of as insulin resistance, systemic inflammation, or vascular dys-
ultrasound screening studies, and gallstone disease was found as- function were associated with gallstone disease prevalence
sociated with obesity, diabetes, pregnancies, familial aggregation,
oral contraceptives, dietary habits, smoking, alcohol or coffee ab- HYPOTHESIS
stinence, and serum lipids – just to mention a few(65, 67-77). Alt- The hypothesis that generated the objectives of this PhD thesis
hough numerous studies were published, they were all limited by included:
their cross-sectional design with the inability to establish causal
temporal associations. • that cardiovascular disease determinants including factors of
More recent cohort studies have included large populations metabolism and lifestyle also determined incident gallstone
with assessment of clinical gallstone disease such as self-re- disease
ported, hospitals admissions, or cholecystectomy. However, when • that female predominance of gallstone disease is caused by
studying the natural history of gallstone disease, only a small frac- sex-dependent changes in metabolism, pregnancies, and life-
tion of gallstone carriers will experience a clinical detection of style with advancing age
their gallstones during long-term follow-up(78-82). Thereby, only • that the high prevalence of gallstone disease in northern Eu-
assessing clinical gallstone disease will include a selected part of ropean countries is caused by lower in vivo production of vit-
the gallstone disease population and the majority will be misclas- amin D due to lower sun exposure
sified as not having gallstone disease. Further, these studies are • that the metabolic changes and genetic susceptibility of obe-
unable to distinguish determinants for gallstone formation from sity are associated with gallstone disease
determinants for clinical gallstone disease. Studies assessing clini-
cal gallstone disease as outcome have identified temporal associ- MATERIAL AND METHODS
ations for cardiovascular disease determinants such as obesity, di- A random sample from the general population, comprising 4807
abetes, oral contraceptives, hormone replacement therapy, persons, aged 30–60 years, and living in 11 municipalities in the
dietary habits, smoking, alcohol and coffee abstinence, and physi- western part of the urban Copenhagen was studied. The sample
cal activity(65, 83-94). However, some identified associations was drawn from the Civil registration system in October 1982.
from these studies may be biased through the selective approach The study was part of the international collaboration MONICA
of assessing clinical gallstone disease. (Multinational mONItoring of trends and determinants in CArdio-
The superior design in exploring gallstone disease determi- vascular disease) with the aim to examine cardiovascular determi-
nants is the cohort study including larger general populations and nants in the general population. Participants were informed
with ultrasound assessment of gallstone disease both at baseline
DANISH MEDICAL JOURNAL 3about the aim of the study including the screening for cardiovas- hormones, genetic variations, and biomarkers of systemic inflam-
cular disease risk factors, but were not informed about findings of mation and insulin resistance.
gallstone disease or other benign conditions in the gallbladder fol- Logistic regression analyses with gallstone disease as the
lowing ultrasound examination to avoid unnecessary treatment outcome were chosen for inferential statistics since the study
and worrying. Informed consent was obtained from each patient. population was examined and re-examined at fixed time-points.
The study protocol conformed to the ethical guidelines of the Thereby, the study design did not include the effects of long-term
1975 Declaration of Helsinki and was accepted by the local re- follow-up as seen in time-to-event cohort studies where every
search ethic committee(101). participant contributes with different lengths of observation time.
People were invited to examination through mail and non- Sex was adjusted for due to the known sex-differences in gall-
responders were re-invited. Those who still did not respond were stone prevalence or otherwise addressed with separate analyses.
contacted by telephone and, if not reached, a third letter asking Age was adjusted for due to the known association with gallstone
them to take contact by telephone was sent. Examination outside disease prevalence and due to the delayed entry design of the co-
working hours and free transportation were offered if necessary. hort study. Multiple adjusted models were performed in order to
Examinations took place after 12 hours of fasting and included an control the associations under study for confounders identified in
abdominal ultrasound, physical examination (blood pressure, previous studies or identified in the studies included in this PhD
weight, and height), blood samples, and questionnaires about thesis. Models were built including at least 10 outcome cases for
medical history including previous cholecystectomy, lifestyle, and every parameter as a rule of thumb. In multiple models, interac-
socioeconomic factors. Participants were interviewed if errors or tions with sex were tested for and continuous variables were ex-
omissions had occurred in the questionnaire responses. Baseline plored for quadratic and cubic polynomial associations with gall-
examination took place 1982-84 and the cohort was re-examined stone disease.
twice with similar protocols in 1987–1988 and 1993–1994 (Figure
2). Prevalence studies from the baseline examination including a PRESENTATION OF STUDIES
detailed description of the cohort have been published before(69, Study I (1)
101). Parts of the re-examinations have been published as inci- Determinants for gallstone formation – a new data cohort study
dence studies with exploration of the effect of age and sex(96, and a systematic review with meta-analysis
102). Aim
Blood or serum samples from examinations were stored at To identify determinants for incident gallstone disease in a Danish
minus 20°C. New analyses were performed in 2004-11, including cohort and to perform a meta-analysis of results from existing co-
vitamin D, hepatic function, renal function, male reproductive horts.
Figure 2: Participant flow and description of examinations
DANISH MEDICAL JOURNAL 4Methods A cohort study of a general population random sample (N=2366)
Data from a cohort study was used. Gallstone incidence was as- aged 30-60 years. Participants were ultrasound screened for gall-
sessed through repeated ultrasound examinations (baseline ex- stones in 1982-84 and again in 1993-94 (baseline examination and
amination and re-examinations 1 and 2, Figure 2). Body mass in- re-examination 2, Figure 2). Lifestyle data and blood samples
dex (BMI), blood pressure, self-rated health, lifestyle variables, were obtained and re-analyzed in 2004. Changes with age in phys-
blood lipids, and use of female sex hormones were measured at iology (body mass index, blood pressure, blood lipids, self-rated
the baseline examination (Figure 2). Statistical analyses included health), lifestyle (smoking, alcohol and coffee consumption, die-
logistic regression. Based on a prospective protocol, a systematic tary habits, physical activity level), and indices of reproductive
review of the literature was performed identifying all articles function (number of births, oral contraceptive use, hormone re-
dealing with determinants of incident gallstone disease. Meta- placement therapy, male reproductive hormones) were explored
analyses of comparable determinants were performed through in females and males separately. Adjusted logistic regression anal-
fixed effect models. yses were performed.
Results Results
Participants with no gallstones at baseline and with at least one Incident gallstones or cholecystectomy at ultrasound examination
re-examination were followed up completely (mean 11.6 years, N in participants initially free of gallstones at baseline occurred in
= 2848). The overall cumulative incidence of gallstones was 0.60% 9.9% of the study population. In females, increasing alcohol con-
per year. Independent determinants for incident gallstone disease sumption (odds ratio (OR) 0.94, 95% CI [0.90;0.98]) and the cessa-
were high age, female sex, high non-high density lipoprotein tion of hormone replacement therapy (OR 0.29, 95% CI
(non-HDL) cholesterol, and gallbladder polyps. In addition, high [0.10;0.83]) inversely determined incident gallstone disease. In
BMI was associated in men. The systematic review additionally males, increasing levels of sex hormone-binding globulin (SHBG)
identified associations for comorbidities, parity, and dietary fac- (OR 0.97, 95% CI [0.94;0.998]) inversely determined incident gall-
tors. Meta-analyses confirmed the significant associations for inci- stone disease. Other changes with age in physiology, lifestyle, or
dent gallstone disease and high age, female sex, high BMI, and reproductive hormones were not associated with incident gall-
high non-HDL cholesterol. No significant associations were found stone disease. High baseline free testosterone determined inci-
for blood pressure, smoking, alcohol consumption, HDL choles- dent gallstone disease in males (OR 1.15, 95% CI [1.02;1.30]).
terol, or triglycerides in meta-analyses.
Strengths and limitations
Strengths and limitations The uniqueness of this cohort study included the assessment of
The strengths of this cohort study were the multiple ultrasound changing determinants over long-term follow-up and the novelty
examinations during the long-term follow-up period. The limita- of assessing male reproductive hormones. Not assessing serum
tions were the inability to explore temporal associations with female endogenous reproductive hormones or cumulative life-
other important metabolic variables such as fasting blood glu- time exposures to both female and male reproductive hormones
cose, insulin, and glycated hemoglobin which were not measured in this study were the main limitations. These could not be meas-
at baseline examination. Due to the long-term follow-up, time-de- ured due to a lack of data on menopausal status and menstrual
pendent changes of the explorative variables could, potentially, cycle at times of blood sampling. Further, changes in determi-
have an influence on gallstone formation. The latter has been ad- nants were measured as the difference between baseline exami-
dressed in Study II(2). nation and re-examination making the latter an assessment of
The strength of the systematic review was the restricted in- both explorative variable and of outcome. This lack of distinction
clusion of cohort studies performed in general populations as- between induction and latency period could possibly have caused
sessed for screen-detected gallstone disease, thereby avoiding a misclassification bias, which may have limited the interpretation
the various selection bias seen in studies assessing clinical gall- of a temporal association in analyses of changes with age. Fur-
stone disease. Limitations in the meta-analyses included the in- ther, a time-related issue was demonstrated through hormone re-
comparable data between variables reported in the identified placement therapy in females with the identification of the pro-
studies, thereby restricting meta-analyses of adjusted estimates tective effect of cessation of hormone replacement therapy
to include only four studies. Although significant determinants without finding any significant effects of hormone use on incident
identified in the incidence study were confirmed in meta-anal- gallstone disease. If estrogens truly are associated to incident gall-
yses, the statistical heterogeneity was high which may restrict the stone disease, one would suspect current estrogen users to have
generalizability of our findings. Heterogeneity could not be ex- a significant association with incident gallstone disease as well.
plored with sensitivity analyses due to the low number of studies Such diverging results may be caused by left truncation, a bias
included. due to non-inclusion of participants with the outcome of interest
before being able to be included in a study(103).
Study II (2)
Are incident gallstones associated to sex-dependent changes Study III (3)
with age? A cohort study Vitamin D and gallstone disease – A population-based study
Aim Aim
To determine if changes with age in physiology, lifestyle, or repro- To determine whether circulating levels of 25-hydroxyvitamin D
ductive hormones were associated with incident gallstones or were associated to ultrasound proven gallstones or cholecystec-
cholecystectomy. tomy in a general population sample. Determinants of vitamin D
status were also explored.
Methods
DANISH MEDICAL JOURNAL 5Methods MAP2K5(rs2241423) (OR 1.80, 95% CI [1.04;3.41]),
A re-invitation of the 4130 people that were still alive from a ran- NRXN3(rs10146997) (OR 1.26, 95% CI [1.01;1.57]),
dom sample of the population of Copenhagen with ages 41–71 HHEX(rs1111875) (OR 1.29, 95% CI [1.03;1.62]),
years was performed and 2650 participated and had complete ul- FAIM2(rs7138803) (OR 0.66, 95% CI [0.48;0.91]), and apolipopro-
trasound examinations (re-examination 2, Figure 2). Ultrasound tein E4 allele (OR 0.76, 95% CI [0.59;0.98]) were associated with
examinations were performed to assess gallstone status and gallstone disease. Urinary albumin was not associated with gall-
blood samples were drawn to assess 25-hydroxyvitamin D and bi- stone disease. Addition of biomarkers of insulin resistance to mul-
omarkers of renal and hepatic function. Gallstone disease was tivariable models removed the association between BMI and gall-
found in 422 participants. Associations were estimated by logistic stone disease prevalence.
regression models.
Strengths and limitations
Results The novelty of this study was the exploration of inflammatory bi-
Levels of 25-hydroxyvitamin D were not significantly associated omarkers, genetic risk alleles for obesity and diabetes type 2, and
with gallstone disease. Time of birth during low vitamin D expo- gallstone disease. The association between BMI and gallstone dis-
sure was associated with gallstone disease (gallstone prevalence ease seemed to be mediated through insulin resistance. The ina-
18.0 versus 14.4%, OR 1.33, 95% CI [1.07;1.65]). Highest quartile bility to identify temporal associations in this study is the main
of cystatin C was significantly associated with gallstone disease limitation just as with Study III(3). The exploration of the 32 ge-
(gallstone prevalence 22.1 versus 12.0%, OR 1.53, 95% CI netic risk alleles included in this study may have lacked power to
[1.08;2.18]). Serum levels of creatinine and alanine amino trans- show associations with gallstone disease and the identified asso-
ferase were not associated with gallstone disease. Sensitivity ciations would not withhold adjustment for multiple testing.
analyses excluding participants with cholecystectomy did not al-
ter results significantly. DISCUSSION
Principal findings
Strengths and limitations Through an exploration of determinants for screen-detected gall-
The novelty of this study was the exploration of associations for stone disease in a Danish population, the following was identified:
vitamin D, associated biomarkers, and gallstone disease in a large
population sample from Denmark which is a country known to • Age, female sex, BMI, non-HDL cholesterol, and gallbladder
have a high prevalence of seasonal vitamin D insufficiency. The polyps are independent determinants for incident gallstone
most important limitations were the inability to study temporal disease. These significant determinants were confirmed in
associations due to the cross-sectional study design and the use meta-analysis including similar designed cohort studies per-
of time of birth during low vitamin D exposure in utero as a proxy formed in Italy, Sweden, and Taiwan.
for maternal levels of vitamin D during the third trimester of preg- • Changes with age in increasing alcohol consumption and in
nancy. cessation of hormone replacement therapy in females, and
in increasing SHBG in males inversely determine incident
Study IV (4) gallstone disease.
Metabolic biomarkers and gallstone disease – a population- • High free testosterone at baseline determines incident gall-
based study stone disease in males.
Aim • No association between 25-hydroxyvitamin D and gallstone
To examine associations for metabolic biomarkers of obesity such disease prevalence was identified. Time of birth during low
as insulin resistance, vascular dysfunction, systemic inflammation, vitamin D exposure in utero and renal failure were associ-
genetic susceptibility and ultrasound proven gallstone disease or ated with gallstone disease prevalence suggesting that vita-
cholecystectomy in a population-based cross-sectional study. min D might have an impact on gallstone disease.
• Biomarkers of insulin resistance are associated with gall-
Methods stone disease prevalence and seem to mediate the associa-
A total of 2650 participants with complete ultrasound examina- tion between BMI and gallstone disease.
tions were included, of whom 422 had gallstone disease (re-ex- • Biomarkers of systemic inflammation and genetic risk alleles
amination 2, Figure 2). Associations to gallstone disease were es- for obesity or diabetes type 2 seem associated with gallstone
timated by multivariable logistic regression models and expressed disease prevalence.
as OR and 95% CI.
Gallstone disease epidemiology in a Danish cohort
Results The incidence rate of gallstone disease in the study population
Gallstone disease was associated with high fasting glucose (OR was found to be 0.60% per year in Study I(1). Similar designed co-
1.14, 95% CI [1.05;1.24]), high fasting insulin (OR 1.03, 95% CI hort studies performed in Italy and Taiwan report incidence rates
[1.01;1.05]), high homeostasis model assessment (HOMA) insulin of 0.46-0.97% per year(79, 97, 98, 100, 104). In a Swedish study, a
resistance (OR 1.18, 95% CI [1.02;1.36]), the metabolic syndrome higher incidence rate of 1.39% per year was found. This may have
(OR 1.51, 95% CI [1.16;1.96]), high white blood cell count (OR been caused by an older cohort(99). However, higher gallstone
1.07, 95% CI [1.00;1.15]), and high C-reactive protein (OR 1.03, disease prevalence has also been found in northern compared to
95% CI [1.01;1.05]). A non-significant tendency towards an associ- southern Europe(37, 38) which may be caused by a lower expo-
ation to high soluble urokinase plasminogen activator receptor sure to vitamin D in utero as found in Study III(3). The hypothesis
was also found (OR 1.08, 95% CI [0.99;1.18]). The of a relationship between seasonal vitamin D insufficiency caused
MC4R(rs17782313) (OR 1.27, 95% CI [1.02;1.58]),
DANISH MEDICAL JOURNAL 6by lower sun exposure and higher gallstone disease prevalence in bias in observational studies caused by a reduced alcohol use in
Denmark could not be confirmed in Study III(3) of this PhD thesis, patients with abdominal symptoms related to clinical gallstone
but should be explored further in future studies. disease(111). Such a bias is unlikely in Study II(2) and other popu-
Only a few studies have compared gallstone disease preva- lation-based cohort studies due to the exploration of temporal as-
lence between different ethnic populations and only one study sociations and the inclusion of an unselected and non-clinical
has been performed for European populations including cohorts population. A causal association for the protective effects of alco-
from Denmark and northeastern Germany(105). The German co- hol consumption on gallstone formation is supported by a lower-
hort had about twice the odds for gallstone disease when com- ing of bile cholesterol saturation(112-114) and an increase in bile
pared to the Danish, which only partly was explained by higher salt production and excretion to gallbladder bile(115, 116). The
BMI, unfavorable lipid profiles, higher prevalence of diabetes, and inverse association between alcohol consumption and cardiovas-
a more frequent use of oral contraceptives and hormone replace- cular disease(117) further emphasizes the protective effects of al-
ment therapy in German subjects. The study concluded that these cohol consumption on cholesterol metabolism. These benefits
classical cardiovascular disease determinants were unable to fully have been attributed to a cardio-protective rise in blood HDL cho-
explain the higher German prevalence and that other factors in- lesterol(118) which, similar as stated above for alcohol consump-
cluding genetic components should be explored in future stud- tion, also has been associated with an increase in bile salts(119).
ies(105). The inability to explain the large differences in gallstone Further preventive mechanisms of alcohol consumption on gall-
disease prevalence between Hispanics and non-Hispanic blacks or stone formation may include a changed gallbladder motor func-
whites through environmental factors was also the conclusion tion with stimulation of contractions, thereby inhibiting bile stasis
based on the gallstone disease prevalence screening-studies per- and gallstone formation(120). However, the effects of alcohol
formed in the US(106). consumption or chronic alcoholism on gallbladder motor function
More speculative theories have proposed the ethnic pre- are controversial(120-122).
dominance of gallstone disease in northern Europe and in the Na- The effects of chronic and acute alcohol consumption on
tive Indian populations of North and South America to be the proximal bowel transit in humans may be controversial based on
cause of survival advantages in acquiring a low metabolic rate experimental studies(122-124). However, a higher everyday alco-
during periods of cold climates with marginal food supplies. This hol consumption has been associated with a faster self-reported
evolutionary promotion of ‘‘thrifty genes’’ and the factors associ- whole gut transit in the general population(125) and an acute ad-
ated with a Western lifestyle such as diet and a sedentary physi- ministration of alcohol has been shown to suppress impeding
cal activity level are thought to be linked to obesity and develop- Type I pressure waves in the jejunum and to stimulate propulsive
ment of gallstone disease(107). Only a few studies based on Type III pressure waves in the ileum(126), indicating that alcohol
empirical research exploring the genetic epidemiology of gall- consumption speeds up distal bowel transit. The protective ef-
stone disease have been performed. American-Indian genetic ad- fects of alcohol consumption on gallstone formation may thereby
mixture was associated with gallstone disease when comparing also be exerted on the enterohepatic circulation by impeding the
mitochondrial DNA from high prevalence gallstone disease popu- entry of secondary bile acids. The sex differences in the effects of
lations of Chilean Hispanics and Mapuche Indians with the lower rising alcohol exposure identified in Study II(2) are somewhat un-
prevalence population of Chilean Maoris(108). Likewise, when explained, but could also be caused by an inability to detect sig-
comparing 92 ancestry informative single nucleotide polymor- nificant associations due to the lower prevalence of gallstone dis-
phisms in Hispanic American women, American-Indian genetic ad- eased in males.
mixture was associated with cholecystectomy and both European Physical activity level did not determine incident gallstone
and sub-Saharan African genetic admixture was inversely associ- disease (Studies I(1) and II(2)). In support of this finding, an inter-
ated with cholecystectomy(109). Pathways in the human endoge- vention of moderate to vigorous physical activity in pregnant
nous synthesis of bile salts and of cholesterol have been sug- women has also been shown to have no impact on incident gall-
gested as mechanisms for the high American-Indian prevalence of stone disease measured through ultrasound examination in a ran-
gallstone disease(110). No studies have compared the genetic ep- domized controlled trial(127). When exploring the subgroup of
idemiology of gallstone disease in populations from Denmark or the study population that had gallstones and was unaware of its
other northern European countries to Southern European popula- gallstone status, a physical activity including light, moderate, and
tions or to other lower prevalence populations. vigorous levels compared to a sedentary level inversely deter-
mined clinical gallstone disease hospital admissions(128). The cur-
Lifestyle rent evidence therefore indicates that gallstone formation is not
An increase in alcohol consumption inversely determined incident determined by physical activity, but that a sedentary physical ac-
gallstone disease in females in Study II(2) while alcohol consump- tivity level determines clinical gallstone disease in persons with
tion at baseline was not identified a determinant in Study I(1). No gallstone disease. Further supporting this hypothesis, physical ac-
other cohort study has explored associations for change in alcohol tivity has also been inversely associated with clinical gallstone dis-
consumption. Similar designed cohort studies confirm the find- ease in larger cohort studies(93). Physical activity increases
ings of an inverse association for incident gallstone disease, but plasma cholecystokinin, which stimulates gallbladder contrac-
only with baseline alcohol consumption – these studies explored tions(129) and an impaired gallbladder motor function with ejec-
weekly alcohol consumption compared to alcohol abstainers(99) tion fraction below 40% has also been associated with recurrence
and linear trend for wine consumption(97). Clinical gallstone dis- of pain attacks in clinical gallstone disease(130). These mecha-
ease has also been inversely associated with alcohol consump- nisms may explain the protective effects of physical activity on
tion(83, 94). clinical gallstone disease. Due to the current evidence and con-
Inverse associations for alcohol consumption and gallstone flicting results in incident clinical versus screen-detected gallstone
disease have previously been suggested due to the protopathic disease, the impact of objectively measured physical activity
DANISH MEDICAL JOURNAL 7through accelerometers on gallstone formation should be subject a similarly designed cohort study before which assessed low den-
to future studies in order to explore this hypothesis further. sity lipoprotein cholesterol(99). The association may be contro-
Other lifestyle factors were found unrelated to gallstone dis- versial since HDL rather than non-HDL cholesterol has been con-
ease in the studies included in this thesis. The systematic review sidered as the major source for reverse cholesterol transport
of existing literature identified that a similar designed cohort from tissue and into the liver(145). Although transport rates for
study associated incident gallstone disease with tobacco smoking, non-HDL cholesterol are lower, transport of both HDL and non-
consumption of milk and oils, and inverse associations with con- HDL cholesterols to liver and bile has been demonstrated in hu-
sumption of coffee, fish, and whole meal(97). However, associa- mans(146). Further, bile cholesterol saturation has been associ-
tions for tobacco smoking and coffee consumption could not be ated with higher blood non-HDL cholesterol and inversely associ-
confirmed in the meta-analysis of Study I(1). Clinical gallstone dis- ated with higher blood HDL cholesterol in healthy humans(147).
ease has been associated with tobacco smoking(92), consumption Although no association for HDL cholesterol and incident gall-
of fatty acids(87), and inversely associated with coffee consump- stone disease was identified in Study I(1), the association for non-
tion(84, 85). However, bias caused by selected populations, by HDL cholesterol seems biologically feasible. Further supporting
between study heterogeneity in exposure assessment, or by the the identified association of Study I(1), non-HDL cholesterol low-
inability to distinguish gallstone formation from clinical disease ering statins have been inversely associated with screen-detected
just like in the exploration of physical activity above, may explain gallstone disease prevalence and with incident clinical disease in
these discrepancies in study results. observational studies(148, 149).
Biomarkers of insulin resistance were associated with gall-
BMI, cholesterol metabolism, and insulin resistance stone disease prevalence and the association for BMI seemed to
BMI was associated with incident gallstone disease in males, but depend on insulin resistance. This suggests that insulin resistance
the association was found for both females and males in meta- possibly mediates the association between BMI and gallstone dis-
analysis in Study I(1). Similarly designed cohort studies have iden- ease in Study IV(4). The associations for biomarkers of insulin re-
tified associations for incident gallstone disease with BMI(79, 97, sistance such as blood glucose, insulin, impaired glucose toler-
98, 100). BMI has also been identified as a determinant for inci- ance, HOMA, or diabetes, and screen-detected gallstone disease
dent gallstone disease in pregnancy and early post-partum period have previously been found in several cross-sectional and case-
in a cohort study including only pregnant women(131). Meta- control studies(75, 150-153). Diabetes or elevated blood glucose
analysis including studies with incident clinical gallstone disease has also been associated with incident screen-detected gallstone
have also identified associations for BMI and waist circumfer- disease(97, 98, 100), however not consistently(79, 99). Meta-
ence(90). A number of alternative body fat tissue measures have analysis including incident clinical gallstone disease has also been
been associated with gallstone disease prevalence independently associated with diabetes(91).
of BMI, such as waist-to-hip circumference ratio with screen-de- Insulin resistance may increase cholesterol supersaturation
tected gallstone disease and computed tomography measured of bile through a number of mechanisms including stimulation of
visceral or subcutaneous fat with clinical gallstone disease(132, the low density lipoprotein-receptor activity and of the rate limit-
133). ing enzyme for endogenous cholesterol synthesis, the 3-hydroxy-
Spontaneous changes in BMI over a decade had no associa- 3-methyl-glutaryl-coenzyme A reductase (HMG Co-A reduc-
tion with incident gallstone disease in Study II(2). Another similar tase)(154, 155). The most important cholesterol transporter facili-
study identified spontaneous weight gain and not weight loss tating cholesterol excretion into both gallbladder bile and bowel
with incident screen-detected gallstone disease(97), which is in lumen is the ABCG5/8 heterodimer(156), and its expression has
accordance with the known association between BMI and gall- been demonstrated promoted by insulin resistance in mice(157).
stone disease. Other cohort studies have associated weight loss Further, an impaired gallbladder motor function in favor of bile
and weight cycling with clinical gallstone disease when compared stasis has been demonstrated in dynamic ultrasound studies in-
to weight maintainers(134-137). Excessive weight loss during cal- cluding fasting and stimulated gallbladders in persons with obe-
orie restricting diets has also been associated with incident sity, insulin resistance, and induced hyperglycemia or hyperinsu-
screen-detected gallstone disease(138, 139). Patients undergoing linemia(158-161). Slower orocecal transit with the hydrogen
bariatric surgery and with subsequent rapid weight loss have also breath test has also been demonstrated under induced hypergly-
been associated with incident screen-detected gallstone dis- cemia and hyperinsulinemia, and in patients with diabetes(162,
ease(140). Suggested mechanisms for gallstone formation during 163) supporting an effect on the enterohepatic circulation and
rapid weight loss have included an initial increase in bile choles- secondary bile salts. Suggested causes of impaired gallbladder
terol saturation(141-143) and an impaired gallbladder motor function and impaired bowel function under conditions of insulin
function(142, 143). Current evidence therefore suggests that resistance include a suppressing effect of hyperglycemia on the
spontaneous changes in weight or BMI in the general population vagal-cholinergic system which causes reduced gallbladder sensi-
do not seem to be associated with incident gallstone disease con- tivity to cholecystokinin or the effects of autonomous neuropathy
trary to rapid weight loss. The latter risk can be significantly re- in diabetes(61, 159). Fair amounts of experimental and observa-
duced through interventions with ursodeoxycholic acid or high-fat tional evidence thereby support a causal association for gallstone
weight loss diets as demonstrated in randomized controlled tri- formation with BMI and insulin resistance.
als(144). Weight loss as a preventive intervention for incident
gallstone disease has – to the best of the author’s knowledge – Sex-differences in incident gallstone disease
not been tested in a randomized controlled trial yet. Female sex determined(1) and the cessation of hormone replace-
The identified determinant of blood non-HDL cholesterol ment therapy in females inversely determined incident gallstone
with incident gallstone disease in Study I(1) has been identified in disease(2). Although many cross-sectional screening-studies have
DANISH MEDICAL JOURNAL 8associated female sex with gallstone disease prevalence, the asso- are therefore only preliminary. Future cohort studies should ex-
ciation has only been identified in one other cohort study(100). plore hormone analogy further and the impact of lifetime expo-
Association for oral contraceptives or hormone replacement ther- sure to reproductive hormones in both females and males in or-
apy has only been identified for clinical gallstone disease(83, 86, der to detect possible targets for gallstone disease prevention or
88, 89). Number of births was not associated to incident gall- treatment.
stones in Study II(2), but has been found associated with preva-
lent and incident screen-detected gallstone disease before(97, Systemic inflammation
164). A high cumulative incidence of screen-detected gallstone Biomarkers of systemic inflammation such as C-reactive protein
disease including gallbladder sludge of 7.9% at third trimester were associated with gallstone disease prevalence in Study IV(4).
with regression to 4.2% in the post-partum period has been iden- Previous cross-sectional and case-control studies have explored
tified in a cohort study including pregnant women, indicating that the impact of C-reactive protein or white blood cell count on gall-
the higher risk of gallstone disease during pregnancy only is tran- stone disease without identifying any significant associations(153,
sient(131). This temporality of an increased risk during pregnancy 177, 178). The identified associations in Study IV(4) are therefore
and early post-partum period may explain the discrepancies in ex- novel findings. Case-control and cohort studies including clinical
isting studies’ results when only total number of births is explored populations have only associated gallstone disease with immuno-
without including time since birth. logical diseases such as rheumatoid arthritis or incident psoriasis
The female predominance of gallstone disease may be ex- without exploring biomarkers of systemic inflammation(179,
plained by the effects of female reproductive hormones on cho- 180).
lesterol metabolism. The binding of 17β-Estradiol to the nuclear The possible role of the immune system in gallstone for-
estrogen receptor in the liver stimulates excretion of cholesterol mation has only recently been reviewed(181). In animals fed by
into bile increasing cholesterol saturation(165). Estrogens also cholesterol-rich diets, the appearance of cholesterol crystals in
stimulate the activity of HMG-CoA reductase facilitating endoge- gallbladder bile has been associated with local inflammation of
nous cholesterol synthesis(165). A case-control study found a sig- the gallbladder wall(182) with infiltration of inflammatory
nificantly higher urinary estrone in females aged over 50 years cells(183), suggesting that local inflammation is an early event in
and with gallstone disease when compared to controls which also gallstone formation. Further, epithelial cell proliferation and in-
supports the associations for endogenous estrogens and gallstone creasing gallbladder wall thickness caused by cell infiltration ap-
formation(166). Increased bile cholesterol saturation has also pear before stone formation(183, 184) and has been associated
been identified in a randomized controlled trial after interven- with impaired gallbladder motility(183). These observations all
tions of hormone replacement therapy in postmenopausal suggest that local gallbladder inflammation might cause impaired
women(167). Bile cholesterol saturation may thereby be the most gallbladder motor function. Whether the local inflammatory
important mechanism involved in the female predominance of changes seen in the gallbladder during gallstone formation are as-
gallstone disease. Use of oral contraceptives does not seem to in- sociated with the systemic inflammation identified in Study IV(4)
fluence fasting gallbladder volume(168). should be explored in future cohort studies.
A higher baseline free testosterone in males determined inci-
dent gallstone disease and an increase of SHBG in males inversely Genetic susceptibility for gallstone disease
determined incident gallstone disease in Study II(2). Associations The single nucleotide polymorphisms of genes MC4R
for reproductive hormones have only been explored in two case- (rs17782313), MAP2K5 (rs2241423), NRXN3 (rs10146997), HHEX
control studies previously, where luteinizing hormone was identi- (rs1111875) were positively associated, while FAIM2 (rs7138803)
fied to have an inverse association with gallstones in males(169) was inversely associated with gallstone disease prevalence in
and no other associations for female or male reproductive hor- Study IV(4). A study of a Danish population found no association
mones were identified(169, 170). On a population level, there is for single nucleotide polymorphisms FTO (rs9939609) or MC4R
an age-related decline in testosterone levels in males, which is (rs17782313) and incident clinical gallstone disease, but an associ-
paralleled by an age-related increase in SHBG(171). The results of ation was found for increasing number of FTO (rs9939609), MC4R
Study II(2) may, therefore, suggest that male testosterone levels (rs17782313), and TMEM18 (rs6548238)(185). No other studies
determine incident gallstones. have explored associations for single nucleotide polymorphisms
Experimental research has demonstrated that bile choles- for MAP2K5, NRXN3, HHEX, FAIM2 and gallstone disease yet.
terol saturation increases in female rodents with administration These findings are therefore novel to the existing literature and
of testosterone while castration of male rodents decreases it(172, should be explored further in other cohorts in the future. Since
173). These findings indicate analogous effects of female and the understanding of these genes in the regulation of obesity and
male reproductive hormones on bile cholesterol saturation and diabetes type 2 is limited, it is preliminary to suggest biological
analogy is further supported by the similar steroid hormone struc- mechanisms involved in the potential association with gallstone
tures, intracellular pathways through nuclear receptors, and by disease.
regulation of gene expression. A number of studies have also ex- The apolipoprotein E4 allele was found inversely associated
plored the effects of administered female reproductive hormones with gallstone disease prevalence in a dominant model exploring
on gallstone disease in males. Male sex offenders treated with E4 allele homo- and heterozygote, but not associated in a reces-
progesterone had higher clinical gallstone disease preva- sive model exploring the E4 allele homozygote in Study IV(4). In a
lence(174). Further, estrogen treatment of males with prostate previous meta-analysis of observational studies including pre-
cancer when compared to placebo or orchiectomy was associated dominantly Chinese Han populations, the E4 allele was directly as-
with cholecystectomy detected at autopsy(175) and screen-de- sociated with gallstone disease in a dominant model(186). An-
tected gallstone disease(176), respectively. These studies all were other study performed in a Danish population found no
limited by insufficient designs and completion of follow-up and association between apolipoprotein E genotypes and gallstone
DANISH MEDICAL JOURNAL 9disease(187). Meta-analysis performed in mixed ethnic popula- study population(11-13). The epidemic of obesity has been pre-
tions or in subgroup meta-analysis restricted to white populations sent for the past decades and a study population sampled today
also found no significant associations for E4 allele carriers(187). would therefore have a higher BMI(206) which, presumably,
Conflicting results are reported for the E4 association in Spanish would cause higher estimates of both prevalent and incident gall-
and Hispanic populations(188-191). Biologically, the apolipopro- stone disease in absolute numbers. However, these changes
tein E plays a critical role in controlling the response to dietary would have no influence on the relative estimates obtained in the
cholesterol and in cholesterol excretion to bile as demonstrated studies included in this PhD thesis.
in knock-out mice(192). However, no impact on bile cholesterol A number of potential outcome and exposure misclassifica-
excretion has been found for the E4 carrier state in Caucasians tions may be present in the material. At the outcome level, ultra-
with gallstone disease(193). Results from the human studies and sound examinations cannot discriminate cholesterol from pig-
from Study IV(4) seem somewhat conflicting and may indicate ment gallstones. With cholesterol gallstones being the
that the effect of the E4 allele on gallstone disease depends on dominating composition of gallstone disease in Denmark, a bias in
ethnicity. The E4 allele may have an association in Chinese or His- the identification of determinants for gallstone disease is unlikely.
panic populations, but probably only minor or no importance in At the exposure level, the assessment of lifestyle relied on partici-
northern European Caucasian populations such as the Danish. pant self-report, which must be suspected to underreport detri-
This suggested population dependent hypothesis should be ex- mental lifestyle. Participants were uninformed about gallstone
plored further through a meta-analysis of existing studies. disease status following ultrasound examination and the assess-
Only one genome wide association study from 2007 has ment of lifestyle variables may therefore only have caused non-
compared sequenced whole genomes of persons with and with- differential misclassification bias. Such bias are generally thought
out gallstone disease to date. This study only identified associa- to cause estimates towards the null(207), which may have caused
tion for one single nucleotide polymorphism D19H (rs11887534) non-significant associations for tobacco smoking, physical activity
for the gene ABCG8 of the above mentioned cholesterol trans- level, and incident gallstone disease in the studies performed.
porter with gallstone disease in a German population(194). This Newer objective measures of lifestyle factors avoid information
strong association has been replicated in both Danish and other bias due to self-report and, presumably, would also improve the
populations(195, 196). Since then, only studies exploring associa- interpretation of results.
tions for genes linked to other diseases or pathways with possible A general problem when performing population-based stud-
links to gallstone disease based on knowledge or suspicion have ies is non-participation which may cause a selected study popula-
been performed without sequencing whole genomes – such as tion. In the studies of this PhD thesis, participation was 74-85% of
Study IV(4) of this PhD thesis. These studies have identified asso- people invited and alive (Figure 2). After the first re-examination,
ciations for the single nucleotide polymorphism of the bilirubin a follow-up of non-responders was performed and information
conjugating enzyme UGT1A1 (rs6742078) with bilirubin content was obtained in 78% through interview by telephone, postal
of gallstone and with gallstone disease in males(197, 198). A num- questionnaire, or through autopsy reports on deceased. Clinically
ber of other single nucleotide polymorphisms associated with diagnosed gallstone disease in non-responders was no different
cholesterol metabolism and transport have also been found(199, than in responders and no gallstones were found in performed
200). autopsies(96). Selection bias due to non-participation in studies
of this thesis therefore seems unlikely.
METHODOLOGICAL CONSIDERATIONS The inability to explore temporal associations in the cross-
Biobanks are unique for exploration of new determinants based sectional studies III and IV is the most important limitation of the
on knowledge obtained since original examinations were per- studies in this PhD thesis. The identified temporal associations for
formed – the stored serum and blood samples from the included BMI, non-HDL cholesterol, baseline free testosterone, and inverse
cohort’s baseline and re-examinations enabled the exploration of temporal associations for alcohol consumption, SHBG and inci-
new determinants for gallstone disease in the included study pop- dent gallstone disease (studies I and II) may be weak from a statis-
ulation. However, repeated freeze-thaw cycles during long-term tical perspective since 95% CI were close to one. But all of these
storage of biological material may potentially cause denaturation associations were for a low-unit increase of the variable on a con-
or water evaporation. Such a bias could potentially cause both tinuous scale, i.e. increase in 1 kg/m2 for BMI or 1 mmol/L in non-
under- and overestimation of results(201). But analyses of blood HDL cholesterol, and causal associations are therefore still sup-
or serum following multiple freeze-thaw cycles are reported relia- ported by these findings.
ble and reproducible for vitamin D(202), genetic material(203),
reproductive hormones, and a number of biomarkers(201, 204, PERSPECTIVES FOR FUTURE RESEARCH
205). Significant changes have only been identified for selected Cholecystectomy is currently considered the definitive treatment
biomarkers with 30 freeze-thaw cycles or more(201), making the of clinical gallstone disease(208, 209) and laparoscopic cholecys-
risk of such bias negligible in the studies performed for this PhD tectomy is one of the most common surgical procedures per-
thesis. formed in the Nordic countries(210). High rates of approximately
Other potential bias when analyzing biobank material or 6200 and 12900 laparoscopic cholecystectomies are performed
data sampled decades ago may be the inability to identify or ac- every year in Denmark and Sweden, respectively(211, 212). Due
count for changing disease trends in the population that have oc- to the ongoing obesity epidemic, an escalation of both incident
curred since the original examination. Although gallstone compo- and clinical gallstone disease is suspected in the coming years and
sition may differ with the underlying disease or with ethnicity, the need of gallstone disease prevention will evidently be increas-
cholesterol gallstones have been the cause of clinical gallstone ing. Although prevalence and incidence of gallstone disease are
disease in both Denmark and other northern European countries higher in northern compared to southern European populations,
for the past decades including the period of examinations of the
DANISH MEDICAL JOURNAL 10You can also read