Santhera Pharmaceuticals - Developing medicines to meet the needs of patients living with rare diseases Corporate Presentation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Santhera Pharmaceuticals
Developing medicines to meet the needs of
patients living with rare diseases
Corporate Presentation
JAN 2022
Disclaimer This presentation is not and under no circumstances to be construed as a solicitation, offer, or recommendation, to buy or sell securities issued by Santhera Pharmaceuticals Holding AG. Santhera Pharmaceuticals Holding AG makes no representation (either express or implied) that the information and opinions expressed in this presentation are accurate, complete or up to date. Santhera Pharmaceuticals Holding AG disclaims, without limitation, all liability for any loss or damage of any kind, including any direct, indirect or consequential damages, which might be incurred in connection with the information contained in this presentation. This presentation expressly or implicitly contains certain forward-looking statements concerning Santhera Pharmaceuticals Holding AG and its business. Certain of these forward-looking statements can be identified by the use of forward-looking terminology or by discussions of strategy, plans or intentions. Such statements involve certain known and unknown risks, uncertainties and other factors, which could cause the actual results, financial condition, performance or achievements of Santhera Pharmaceuticals Holding AG to be materially different from any expected results, performance or achievements expressed or implied by such forward-looking statements. There can be no guarantee that any of the research and/or development projects described will succeed or that any new products or indications will be brought to market. Similarly, there can be no guarantee that Santhera Pharmaceuticals Holding AG or any future product or indication will achieve any particular level of revenue. In particular, management’s expectations could be affected by, among other things, uncertainties involved in the development of new pharmaceutical products, including unexpected preclinical and clinical trial results; unexpected regulatory actions or delays or government regulation generally; the Santhera Pharmaceuticals Holding AG's ability to obtain or maintain patent or other proprietary intellectual property protection; competition in general; government, industry, and general public pricing and other political pressures. Santhera Pharmaceuticals Holding AG is providing the information in this presentation as of the date of the publication, and does not undertake any obligation to update any forward-looking statements contained herein as a result of new information, future events or otherwise. 2 Corporate Presentation Jan-2022
SIX Swiss Exchange listed company (SANN)
1 Global headquarters near Basel (Switzerland) with internationally experienced leadership team
North American headquarters in Boston (USA) with recent hire of new President, North America
US NDA filing for vamorolone in Duchenne muscular dystrophy start in Q1-2022
2 Positive study supports vamorolone as foundational therapy replacing standard of care
Steroid-like efficacy with differentiated safety profile addresses needs across broad patient segments
Santhera Potential as alternative to steroids in broad range of therapeutic indications
Pharmaceuticals Phase 2a study initiation for lonodelestat in cystic fibrosis in mid-2022
3
Corporate Successful multiple ascending dose study in cystic fibrosis patients completed
Novel anti-inflammatory agent for neutrophil associated pulmonary disorders in general
Snapshot
Recent financing activities
4 Financing CHF 42 million completed Sep. 2021 with runway through mid-2022
Additional funding, including non-dilutive, planned for H1-2022
China licensing USD 20 million upfront & early regulatory milestones combined
Top shareholders: Idorsia, Highbridge Capital, HNWI/Family offices
3 Corporate Presentation Jan-2022
Santhera pipeline offers an attractive investment opportunity
Two assets with broad therapeutic potential and opportunities beyond current active programs
Lonodelestat targeting
Vamorolone foundational therapy in Duchenne MD inflammation in cystic fibrosis
• Positive pivotal data in Phase 2b trial • Positive MAD Phase 1b trial in CF
• Upcoming regulatory filings US (NDA Q1-2022*), EU (MAA Q2-2022) • Safe dose regimen; effect on biomarker
• Peak potential > USD 500 million in DMD (US+EU4+UK) • Phase 2a starting mid 2022 in patients not on
CFTR modulator therapy
• Own commercialization in US and EU4+UK
• Potential in other inflammatory lung diseases with
• Geographical partnerships outside US and top 5 European markets neutrophil involvement, both for acute and chronic
• Potential as alternative to steroids in broad range of therapeutic areas application
Worldwide rights for all indications for both assets
4 Corporate Presentation Jan-2022 * NDA rolling submission to start in Q1 2022; CFTR: Cystic Fibrosis Transmembrane Conductance Regulator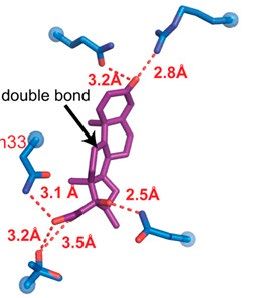
Pipeline offers promising therapeutic options in rare disease areas
Lead asset vamorolone close to NDA filing in DMD in Q1-2022
Molecule Indication IND Ph 1 PoC Pivotal Filing Market Milestones and remarks
Q2-21: Positive pivotal data
Duchenne
VISION-DMD Q4-21: Successful study completion
muscular dystrophy Q1-22: Start US NDA rolling submission
Vamorolone
Q4-21: IND authorization obtained
• dissociative steroid Becker
Q1-22: Start Ph 2a
• oral suspension muscular dystrophy FDA grant to partner
Steroid alternative in multiple
New IND applications in planning
pediatric rare indications
Q1-21: Successful Phase 1 MAD
Cystic fibrosis Q2-22: Start of Phase 2a
Lonodelestat (non-user of CFTR therapy)
• hNE inhibitor
• via nebulizer Multiple respiratory conditions
New IND applications in planning
with high hNE activity
Vamorolone worldwide license from ReveraGen in Sep 2020; Lonodelestat worldwide license from Polyphor (now Spexis) in Feb 2018; Lonodelestat was formerly known as POL6014
hNE: Human Neutrophil Elastase; PoC: Proof of Concept; SEAL: Simultaneous expression of artificial linkers; IND: Investigational new
drug; MAD: Multiple ascending dose; CFTR: Cystic Fibrosis Transmembrane Conductance Regulator; NDA: New Drug Application;
5 Corporate Presentation Jan-2022 FDA: Food and Drug Administration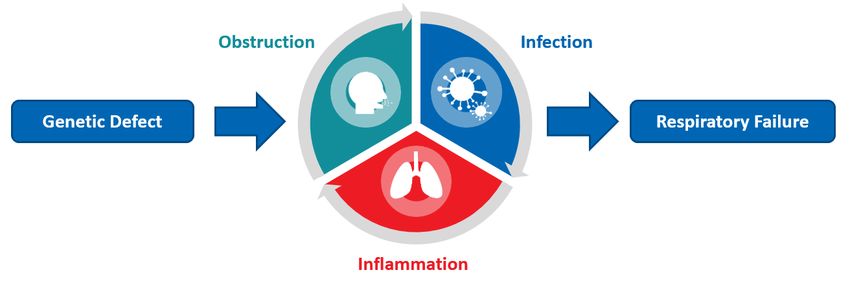
Vamorolone in Duchenne muscular dystrophy
and potentially other inflammatory disorders
6
DMD offers attractive opportunity in well-defined orphan disease market
DMD market with few current treatment
options, projected to be worth Small teams
needed to cover DMD Centers HCPs
> USD 4 billion by 2023*
entire market in
US ~160 ~450
EU and US
• Approx. 30,000 – 35,000 patients in US and
EU4+UK ~180 ~750
Europe combined
• Well defined standard of care with corticosteroids
as lead chronic treatment in established guidelines • Exon skippers and read through therapies
Current approved serve niche segments based on genetic
• Patients diagnosed at early age and accessible
mutation
therapies
• Limited number of specialized centers
command high • Gene therapies deliver micro-dystrophin
• Well organized and influential patient advocacy price with intrinsic partially restoring function with re-dosing
groups limitations to challenges
• Newer therapies likely to be used in combination serve addressable • Deflazacort (corticosteroid) is approved in
with corticosteroids market US, achieves attractive margins
7 Corporate Presentation Jan-2022 * Grand View Research Inc., Research & Markets, Decision ResourcesCorticosteroids delay disease progression by 2 – 3 years4,6
Established endpoints and consistent evidence base from several clinical studies
age (years)
Corticosteroids are a standard of care
0 5 10 15 20 25 30
Impaired ability to
hop, run, jump, rise from floor • DMD progression is sequential, non-linear and
Loss of rise from floor
irreversible1-4
Loss of stair climb
Loss of ambulation • Early initiation of corticosteroids preserves
Loss of upper limb
overhead reach muscle function and strength, delaying time to
Loss of upper limb
hand to mouth loss of functional milestones by 2 – 3 years4,6
Non-invasive ventilation
(nocturnal)
Non-invasive ventilation • Steroid treatment associated with a reduction
(diurnal)
Death
in all-cause mortality, new onset and
progressive cardiomyopathy5
1. Birnkrant et al. (2018) Lancet Neurology, 1474; 2. Cowen et al. BMC; Neurology (2019) 19:84; 3. Asher et al. (2020) Exp.
Opin. Bio. Therapy, 20:3, 263; 4. McDonald CM et al., Lancet 2018, 3391 (10119):451-461; 5. Schram et al; PCL Cochrane
Database of Systematic Reviews (2013), 61(9);948-54; 6. Matthews et al Cochrane Database of Systematic Reviews (2016)
8 Corporate Presentation Jan-2022 DOI: 10.1002/14651858.CD003725.pubCorticosteroid treatment is associated with well-defined toxicities
…up to 65% of patients discontinue treatment early due to adverse events3-5
37% Growth failure/delay2,3 65% Weight gain3
37% Behavioral changes3 31% Excessive hair growth2,3
30% Bone changes or fractures2,3 19% Cataracts2
55% Cushingoid appearance3
1. Cowen L, et al. BMC Neurol. 2019;19:84; 2. Wong B, et al. Treatment Pediatr. 2017;182:296–303;
9 Corporate Presentation Jan-2022 3. Bello L, et al. Neurology. 2015;85:1048–1055;Corticosteroid use is limited due to known side effect profile
Use of corticosteroids in DMD is high, particularly in ambulatory patients but declines with age4
Reasons for Discontinuing Steroid Treatment4
Problems with side effects
Not enough benefits
Did not like use of long term medication
65.2
CS non-user Other
CS user
Reasons for not Initiating Steroid Treatment4
Worried about side effects
Doctor never presribed/recommended
25.4
Other
Worried about not getting enough benefit
Does not like use of long term medication
Age 3 and under
10 Corporate Presentation Jan-2022 1: McDonald Lancet 2017; 2: Goemans Lancet 2018; 3:McDonald Mucle&Nerve 2020 ; 4: Cowen BMC Neurology 2019;Vamorolone retains benefits of steroids with fewer side effects1-3
Glucocorticoid Receptor
Ligand Binding Domain
Like corticosteroids4-5
• inhibition of NF-кB pro-inflammatory transcription factors
Retained efficacy due to potent anti-inflammatory action
Vamorolone
Unlike corticosteroids4-5
• Not a substrate of hydroxysteroid dehydrogenase
• Less activation of genes responsible for side effects
• Potent mineralocorticoid antagonist (eplerenone-like)
• Membrane stabilizer
Double bond in vamorolone chemical structure
attenuates GC receptor binding and ultimately Potential for significant reduction of steroid-associated side effects
leads to less activation of genes responsible for
side effects4-5
NF-кB=nuclear factor kappa B., 1. Smith et al. PLOS Medicine. (2020); 2. Dang et al. MDA Abstr. #47 (2021) 3. Guglieri M Poster EP 524
11 Corporate Presentation Jan-2022 WMS 2021, 4. Heier CR, et al. EMBO Mol Med. 2013;5:1569-1585, 5. Liu X, Proc Natl Acad Sci U S A. 2020 Sep 29;117(39):24285-24293Tested in a comprehensive clinical development program
200 patient-years exposure in 160 DMD boys treated with vamorolone for up to 2.5 years1
2015 2016 2017 2018 2019 2020 2021 2022 2023 2024
Ph 1 (N=86) Ph 2a (N=48) Pivotal VISION-DMD (N=121) age 4 –Pivotal VISION-DMD: Study design
Randomized, double-blind, placebo and active control trial in 121 steroid-naive patients, aged 4 –Primary endpoint met with high statistical significance at 24 weeks
Secondary endpoints with statistical significance and clinically relevant treatment differences (4 out of 5)
Rank Endpoint Comparison vs placebo Difference P-value
Primary TTSTAND velocity vam 6mg/kg/d 0.06 rises/s 0.002
TTSTAND velocity vam 2mg/kg/d 0.04 rises/s 0.017
6MWT vam 6mg/kg/d 42 m 0.003
Pre-Specified
6MWT vam 2mg/kg/d 37 m 0.009
Secondary
TTRW velocity vam 6mg/kg/d 0.24 m/s 0.002
TTRW velocity vam 2mg/kg/d 0.13 m/s 0.103
TTCLIMB velocity vam 6mg/kg/d 0.07 tasks/sPrimary endpoint met with clinically relevant treatment difference
Treatment difference of 0.05 rises/sec predictive of delay of 2 – 3 years in time to loss of ambulation1
TTSTAND velocity (rises/sec)2
0.08
0.06
Change from Baseline (SEM)
0.04
0.02 p=0.002
0.00 23% improvement in time to rise after
0 6 12 24 6 months of treatment with VAM 6mg/kg/d
-0.02
Weeks Rise time (sec) 2 BL w 24 % Change
-0.04 VAM 6 mg/kg/d 6.0 4.6 - 23%
Placebo(N=28) VAM 6 mg/kg/d (N=28) Placebo 5.4 5.5 + 2%
1. McDonald et al. PPDM Conf. 2021 Poster #16, 2. mITT-1: modified intention to treat population from period 1, MMRM
15 Corporate Presentation Jan-2022 estimates of changes from baseline, 3. Press Release June 1st 2021, descriptive statisticsNo significant difference for vamorolone vs prednisone across endpoints
Percentual change from baseline comparing groups at week 24
35
PLA VAM 2 VAM 6 PDN
Percentual change from baseline 30
25
20
15
10
5
0
-5
-10
TTSTAND velocity 6MWT distance NSAA score TTRW velocity
PDN: Prednisone 0.75 mg/kg/d; VAM: Vamorolone at 2 and 6 mg/kg/d; PLA: Placebo; Time to Stand (TTSTAND), 6 Minute Walk Test
16 Corporate Presentation Jan-2022 (6MWT), Time to Run/Walk 10m (TTRW), Time to Climb 4 Stairs (TTCLIMB), North Star Ambulatory Assessment (NSAA).No loss of efficacy when switching from prednisone to vamorolone
Durable treatment effect maintained over 48 weeks with vamorolone 6 mg/kg/d1
TTSTAND velocity (rises/sec) 1
0.08
Period 1 Period 2 • During treatment period 1, patients on
vamorolone 6 mg/kg/d showed same change
0.06
in TTSTAND velocity as patients on
Change from Baseline (SEM)
prednisone before switching to vamorolone
0.04
6 mg/kg/d
• During treatment period 2, both groups
0.02 showed same maintenance of effect
• Historical data consistently show that there is
0.00 no further improvement with prolonged
0 24 48
steroid treatment after the initial improvement
in TTSTAND2
-0.02
Weeks
Placebo (N=28) VAM 6 mg/kg/d (N=28) PDN - VAM 6 mg/kg/d (N=15)
1. Data on File VAM-2021-002, mITT-2: modified intention to treat population from period 1 and 2, MMRM estimates of changes
17 Corporate Presentation Jan-2022 from baseline. PDN –prednisone 0.75mg/kg/day: PCB: Placebo, PDN-VAM: prednisone 0.75 mg/kg/d in Period 1 transitioned to
vamorolone 6mg/kg/d in Period 2 group after a 4-week tapering period; 2. McDonald et al. Poster PPMD Annual Conference 2021Adverse events decreased after switching from prednisone to vamorolone
Number of new or worsening adverse events (AE) or adverse events of special interest (AESI)
Analysis in population of 30 patients on prednisone switching to either vamorolone 2 or 6 mg/kg/d with 15 patients per dose i.e. same 30 patients combined
120 25 Data from same switching patients
• Prednisone Period 1 (N=30)
100
- 23% • Vamorolone Period 2 (N=30)
- 32% 20
80 No adverse events reported with vamorolone for
Number of AESI’s
15 • Hirsutism
• Cataracts
Number
60 • Severe/serious skin related issues
- 60%
- 49% 10 - 30%
40
5
20
0 0
All AEs AESIs Infections Behaviour Gastrointestinal Cushingoid Skin/hair changes Diabetes-related Weight gain Hypertension
problems symptoms features labs
PDN 0.75mg/kg VAM 2+6 mg/kg
PDN 0.75 mg/kg + 6 mg/kg
VAM2 &
AE: adverse events; AESI: adverse events of special interest; SAE: serious adverse events. PDN: prednisone 0.75 mg/g/d; All
doses daily; Safety Population 2 (SAF-2). Data for prednisone 0.75mg/kg/d from Period 1 and vamorolone 2 + 6mg/kg/d from
18 Corporate Presentation Jan-2022
Period 2 (N=30)Vamorolone allows for normal bone development and growth
Comparison to prednisone upon switching to vamorolone and analyses of long-term use
Switching from prednisone to vamorolone recovers Long-term use of vamorolone did not stunt growth
normal growth trajectory unlike other corticosteroids used in DMD
0.3 Change in Height z-score1
VAM 2 + 6 mg/kg/d (N=23)
0.2
VAM 2 + 6 mg/kg/d (N=56)
Change from Baseline (SEM)
0.1
p = 8.94 x10-7
0
0 24 48
Corticosteroids from CINRG DNHS study (N=75)
-0.1
Weeks
PDN - VAM 2 + 6 mg/kg/d (N=30)
-0.2
Modelling of height trajectory from long-term vamorolone data and
corticosteroids from CINRG Natural History Data2
1. Safety Population 2 (SAF-2); PDN – Prednisone 0.75 mg/kg/d; PDN-VAM: growth trajectory (z-score) compared for
prednisone in Period 1 and vamorolone (2 + 6 mg/kg/d) in Period 2; All doses daily; MMRM estimates of changes from
19 Corporate Presentation Jan-2022 baseline 2. Mah et al; ePoster LB.08 WMS 2021Summary of key findings from VISION-DMD pivotal trial
Placebo controlled treatment followed by randomized vamorolone treatment at 2 doses
Treatment Period 1 Treatment Period 2
Baseline to week 24 Week 24 to week 48
Placebo controlled Vamorolone treatment
Vamorolone at 2 doses vs placebo and prednisone Continued use of vamorolone
• Persistence of the treatment effect
• Primary endpoint vs placebo met (TTSTAND Velocity)
• Well tolerated safety profile
• Strong efficacy across secondary endpoints
• Similar efficacy as prednisone Switching from prednisone to vamorolone
• Maintenance of efficacy
• Well tolerated safety profile
• Reduction of adverse events (typically associated with corticosteroids)
• Recovery of normal growth trajectory
Vamorolone shows comparable efficacy to prednisone with improved safety profile
20 Corporate Presentation Jan-2022Vamorolone program in DMD ready to file Pre-NDA meeting with FDA confirmed filing based on current data package for efficacy and safety FDA filing starts in Q1-2022* followed by EMA filing in Q2-2022 based on pivotal placebo-controlled VISION-DMD study • Positive primary (p
Lonodelestat in cystic fibrosis and potentially
other inflammatory pulmonary disorders
22Cystic fibrosis is a rare genetic lung disorder with unmet medical need
Genetics Cause Patients Symptoms Medical need
Autosomal recessive Mutations in the CF More than 80,000 Persistent lung No approved
disorder diagnosed at transmembrane patients in US and infections, chronic treatment specifically
young age conductance regulator Europe combined inflammation and loss addressing
(CFTR) gene of respiratory function inflammation in CF
Need to break vicious cycle
of airway obstruction,
respiratory failure and
resulting chronic
inflammation
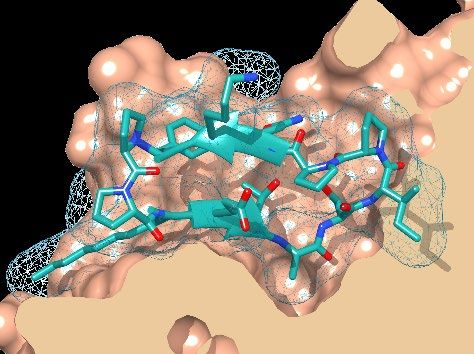
23 Corporate Presentation Jan-2022 De Rose, V, Eur Resp J (2002) 19;333; Mogayzel, PJ, et. al. Am J Respir Crit Care Med (2013) 187(7):680Lonodelestat targets elastase, a protease responsible for lung damage
Pathological levels of neutrophil elastase (NE) during inflammation
destroy lung tissue over time
Lonodelestat is a highly potent, reversible and selective NE inhibitor
• Effective in pico-molar range (Ki 0.05nM) inhibiting Lonodelestat bound to elastase
free and membrane bound NE
• Demonstrated efficacy in various in vivo models
for lung diseases (inhaled/intranasal)
Lung
Lonodelestat (μM)
x 1,000
Administration via inhalation using Pari eFlow® Systemic
• CE marked medical device since 2005,
widely used, also in CF
• High prolonged exposure in lung but desired
low systemic exposure after inhalation Mean levels (±SD) of lonodelestat after inhalation of single ascending
doses in subjects with CF (SAD study, Barth et al. J. Cyst Fibr. 2020)
24 Corporate Presentation Jan-2022Effect on inflammatory biomarker at a safe dose established in Phase 1
Single and multiple ascending dose (SAD & MAD) studies supported by the Cystic Fibrosis Foundation and
successfully completed with lonodelestat
Phase 1 SAD in healthy volunteers (Barth et al. 2020)
Linear dose relationship and well tolerated doses up to 480 mg
per day via inhalation (N=48)
Phase 1 SAD in patients with CF (Barth et al. 2020)
Good tolerability at doses of 80/160/320 mg QD, achieving high
concentrations in sputum and complete inhibition of elastase (N=24)
Phase 1 MAD in patients with CF (press release 3/2021)
Good tolerability and transient, near complete inhibition of elastase Absolute values in μM of active NE in sputum after inhalation of lonodelestat
(mean ± SD values, N=6 per group).
activity with daily inhalation of 40/80/160 mg QD, 80 mg BID over a
period of 2 – 4 weeks (N=32)
25 Corporate Presentation Jan-2022 Barth et al. J. Cyst Fibr. (2020), 19:299Successful Phase 1 program paves way for further clinic development
Key achievements in CF development program Next steps in CF
• Safe dose regimen identified • Preparation of Phase 2a program in patients
• Effect on inflammatory biomarker established currently non-eligible for CFTR modulator
therapy with a dose of 2 x 40 mg daily
• High local targeting through inhalation demonstrated
Opportunities beyond CF
Opportunities beyond CF
• Acute lung injury / ARDS
• Excessive neutrophil activity in range of pulmonary • Pulmonary arterial hypertension
diseases provides rationale for pipeline expansion • Primary ciliary dyskinesia
• Non-cystic fibrosis bronchiectasis
• Identified opportunities in both acute and chronic
• Alpha-1 antitrypsin deficiency
indications • Chronic obstructive pulmonary disease
• Two different acute indications under discussion • Pulmonary fibrosis following cancer therapy
for entry into clinical program • ...and other disorders associated
with excessive elastase activity
26 Corporate Presentation Jan-2022 ARDS: Acute respiratory distress syndrome; CFTR: Cystic Fibrosis Transmembrane Conductance RegulatorFinancial overview
• Cash runway through mid-2022
• CHF 21 million cash & cash equivalents and CHF 8 million available facility at Dec 31, 2021
• CHF 42 million (net proceeds) financing completed September 2021
• Comprising CHF 20 million share issue; CHF 15 million Bond issue; CHF 10 million loan facility
• Debt obligations at Dec 31, 2021
• CHF 20 million Convertible Bond 7.5% 21/24 maturing Aug 2024
• CHF 15 million new Convertible Bond 7.5% 21/24 maturing Aug 2024 to settle CHF 15.1 million
Convertible Bond 5% 17/22 maturing Feb 2022
• CHF 2 million exchangeable loan facility
• Share capital and market capitalization
• 54.6 million (incl. treasury) shares issued at Dec 31, 2021
• Available capital increase 20 million in ordinary and 49 million in conditional and authorized shares
• CHF 73 million market capitalization Dec 31, 2021
27 Corporate Presentation Jan-2022 All amounts Consolidated IFRSSanthera Pharmaceuticals
Developing medicines to meet the needs of
patients living with rare diseases
Jan 2022You can also read