SHOWCASING AF PIONEERS OF 2023 - AF ASSOCIATION HEALTHCARE PIONEERS REPORT - www.AFpioneers.org - Arrhythmia Alliance
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

SHOWCASING AF PIONEERS OF 2023 AF ASSOCIATION HEALTHCARE PIONEERS REPORT www.AFpioneers.org

MISSION
AF Association was established in 2007 by Trudie Lobban MBE & Prof A John Camm
following the demand on its sister organisation – Arrhythmia Alliance – from individuals
needing support and information for atrial fibrillation (AF).
AF Association works with medical experts globally to provide information, support,
education and awareness on atrial fibrillation, delivering the latest technologies and
treatments to both patients and healthcare professionals to optimise outcomes for all
those living with AF.
2 www.AFpioneers.org
FOREWORD
Atrial fibrillation (AF) is the most common innovative approaches to detecting,
sustained heart rhythm disorder. It is caused protecting, correcting, and perfecting atrial
by many underlying cardiac conditions and fibrillation management. For example, Giskes
often it appears without any apparent cause. et al (page 5) found that automated atrial
The arrhythmia, however, has deleterious fibrillation self-screening in general practice
consequences if not correctly managed.
The correct management of the condition waiting rooms doubled AF diagnosis rates.
involves control of the rhythm disorder Walker et al (page 6) developed a novel MDT
itself, management of any underlying cause pathway for direct access ILR technology to
and encouragement to improve unhealthy detect AF in patients post embolic stroke
lifestyles. Above all, the risk of stroke must at UHNM. And Gurney and Rankin (page
be assessed so that appropriate protective 7) used Physiologist-led implantable loop
therapy can be instituted. Because of the recorder insertion to detect atrial fibrillation
complexity of this arrhythmia, the Atrial in cryptogenic stroke patients.
Fibrillation Association was founded to help
both patients and doctors to improve the We hope the 2023 AF Pioneers report will
treatment of the condition and contribute to inspire you to explore new approaches to
its investigation to help the discovery of new detecting and managing AF. This is ever more
approaches to its diagnosis and treatment. important because of the rapidly increasing
number of patients who suffer from this
AF Association’s long-standing “DETECT, condition, which although often silent initially
PROTECT, CORRECT, PERFECT” campaign calls may ultimately have devastating effects on
for healthcare professionals to DETECT AF the lives of those who continue, without the
with a simple pulse check, PROTECT against appropriate care.
AF-related stroke with anticoagulation
therapy, and CORRECT the irregular rhythm We are grateful to everyone who submitted
with access to appropriate treatments — their work for looking at ways to improve care
leading to PERFECT the patient care pathway. and quality of life for people living with AF.
Work published in this years AF Association
Healthcare Pioneers Report demonstrates
Mrs Trudie Lobban MBE Professor A John Camm
Founder and CEO Trustee and Co-Founder
AF Association AF Association
Reference 1. AF Association. AF White Paper — Put People First March 2021. https://bit.ly/AFAWhitePaper (date accessed 08/10/21).
www.AFpioneers.org 3
CONTENTS
AUTOMATED ATRIAL FIBRILLATION SELF-SCREENING IN GENERAL PRACTICE
WAITING ROOMS THAT DOUBLED AF DIAGNOSIS RATES (AF SELF-SMART:
5 ATRIAL FIBRILLATION SELF-SCREENING, MANAGEMENT AND GUIDELINE-
RECOMMENDED THERAPY) 1ST PLACE WINNER
THE DEVELOPMENT OF A NOVEL MDT PATHWAY FOR DIRECT ACCESS ILR
6 TECHNOLOGY TO DETECT AF IN PATIENTS POST EMBOLIC STROKE AT UHNM
JOINT 2 ND PLACE
PHYSIOLOGIST-LED IMPLANTABLE LOOP RECORDER INSERTION TO DETECT
7 ATRIAL FIBRILLATION IN CRYPTOGENIC STROKE PATIENTS JOINT 2 ND PLACE
IMPROVING STROKE PREVENTION IN DEVICE-DETECTED ATRIAL FIBRILLATION
THROUGH A MULTIDISCIPLINARY PATHWAY BETWEEN CARDIAC RHYTHM
8 MANAGEMENT TEAM AND STROKE PREVENTION IN ATRIAL FIBRILLATION
(SOS-AF) SERVICE
9 ATRIAL FIBRILLATION VIRTUAL WARD - A GLIMPSE INTO THE FUTURE OF AF CARE
IMPROVING CLINICAL OUTCOMES AND REDUCING HEALTH INEQUALITIES
10 IN REMOTE AND RURAL COMMUNITIES USING A TECHNOLOGY-ENABLED
SOLUTION FOR PAROXYSMAL ATRIAL FIBRILLATION MONITORING
PROTECT AND PERFECT - PREVENTING ATRIAL FIBRILLATION RELATED STROKES
11 ACROSS A PRIMARY CARE NETWORK IN A DEPRIVED BOROUGH
ESTABLISHING HIGHLY SPECIALISED MULTIDISCIPLINARY MANAGEMENT OF
12 PATIENTS UNDERGOING THIRD OR SUBSEQUENT ABLATIONS FOR AF OR ATRIAL
TACHYCARDIAS TRANSFORMS OUTCOMES
PHARMACIST-LED INTERVENTION FOR ATRIAL FIBRILLATION IN LONG-TERM
13 CARE: THE PIVOTALL STUDY
CASE STUDY DEMONSTRATING IMPROVED MONITORING AND PATIENT
14 SAFETY OUTCOMES FOR PATIENTS PRESCRIBED DOACS IN A BOROUGH
IN SOUTH-EAST LONDON
15 CENTRES OF EXCELLENCE
4 www.AFpioneers.org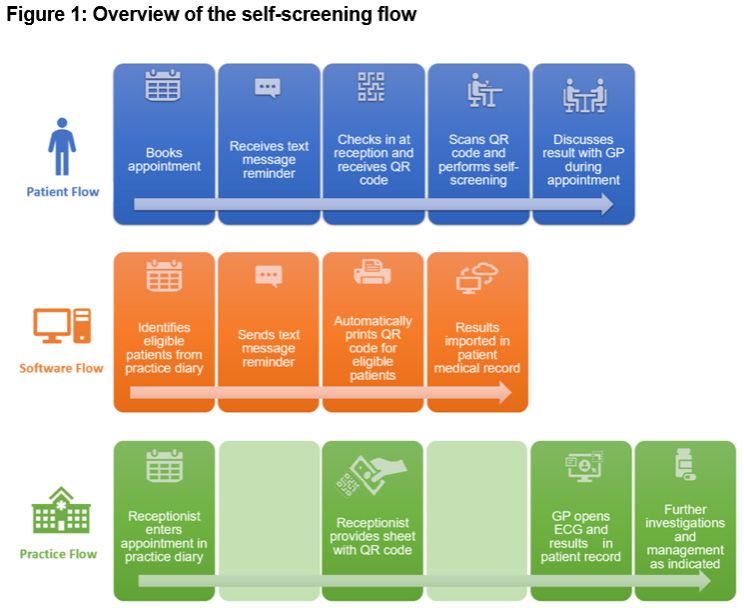
AUTOMATED ATRIAL FIBRILLATION SELF-SCREENING IN GENERAL PRACTICE WAITING
ROOMS THAT DOUBLED AF DIAGNOSIS RATES (AF SELF-SMART: ATRIAL FIBRILLATION
SELF-SCREENING, MANAGEMENT AND GUIDELINE-RECOMMENDED THERAPY)
DR KATRINA GISKES, DR NICOLE LOWRES, DR JESSICA ORCHARD,
MS JIALIN LI, DR KIRSTY MCKENZIE, ASSOC PROF CHARLOTTE HESPE,
PROF BEN FREEDMAN
Heart Research Institute (Australia), University of Notre Dame Australia
INTRODUCTION RESULTS
General Practitioners (GPs) are uniquely placed 1127/2835 (40%) in-scope patients
to screen and initiate management for atrial completed self-screening (range 12-74% per practice). AF was
fibrillation (AF) to reduce avoidable stroke. diagnosed in 49/1127 (4.3%), of whom 90% had CHA2DS2-VA
Current Australian and European guidelines score >2. AF diagnosis doubled during the intervention from
recommend opportunistic AF screening by 10.8 (pre-intervention) to 21.9 per 1000 patients. Screening rates
pulse palpation or electrocardiogram (ECG) increased almost four-fold compared to standard practice. 85% of
rhythm strip among adults aged >65 years. Pulse newly diagnosed high-risk patients (i.e. CHA2DS2-VA >2) received
palpation is a fast and simple method available recommended anticoagulant therapy. GPs indicated high levels
to GPs, however only 10-15% report regularly of acceptance of self-screening and reported little impact on
palpating their patients’ pulse. Time is the their workflow. Patient observations and interviews with reception
greatest barrier to AF screening by GPs and is staff indicated that assistance was often required for patients to
being increasingly challenged by more complex complete self-screening.
patients and shorter consultation times. CONCLUSION
THE INNOVATION Internationally, this is the first intervention to successfully integrate
A purpose-built AF self-screening station was a fully-automated AF self-screening station that transfers screening
developed and included a Kardia ECG device results into the electronic medical record. By effectively overcoming
and iPad. Customised software integrated the time barriers to opportunistic screening for GPs, this AF self-
station with practice software and seamlessly screening solution increases the detection and diagnosis of AF.
identified eligible patients booked for a face- With some adjustments to improve patient usability it could be
to-face GP appointment and sent an automated implemented at scale to reduce AF-related strokes.
text message prompt to patients to undertake
screening before seeing the GP. The station
guided patients through the screening process
and exported their single-lead ECG with
automated analysis into their electronic medical
record. Treating GPs viewed the screening
outcome and ECG prior to the patient entering
the consultation room and then discussed the
screening outcome during the consultation.
Figure 1 outlines the self-screening flow.
DESIGN AND SETTING
The intervention was trialed in 6 Australian
general practices: 2 rural, 2 Greater Sydney, and 2
Metropolitan Sydney, for ~3 months per practice,
between August 2020-August 2021. Process
evaluation of staff acceptability and patient
usability was undertaken by semi-structured
interviews with 20 practice staff and observation
of 22 patients undertaking self-screening.
www.AFpioneers.org 5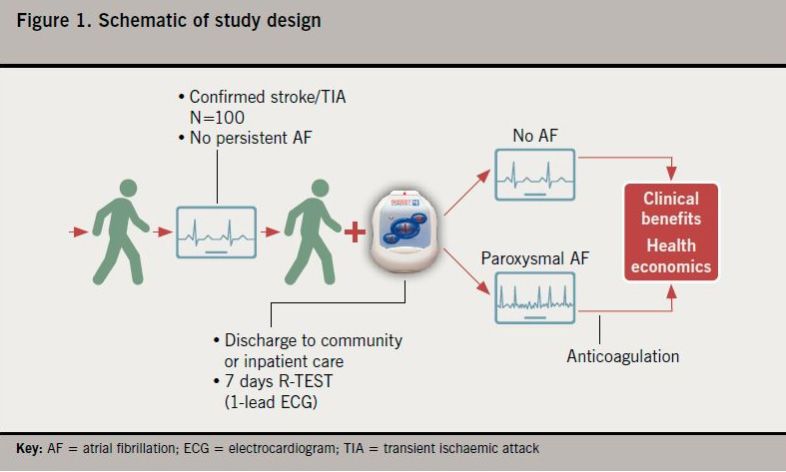
THE DEVELOPMENT OF A NOVEL MDT PATHWAY FOR DIRECT ACCESS ILR
TECHNOLOGY TO DETECT AF IN PATIENTS POST EMBOLIC STROKE AT UHNM
MR VINCENT WALKER, DR SAVINI GUNATILAKE, MR JOSEPH MAYER,
DR INDIRA NATARJAN, DR A PATWALA, MISS F PARSONAGE
University Hospital of North Midlands
ABOUT THE CASE STUDY
Opportunistic screening using conventional cardiac monitoring to detect AF post stroke
has very low diagnostic value but at significant fiscal cost to the NHS. An MDT pathway has
been developed at UHNM to bypass conventional cardiac monitoring in favour for direct
ILR monitoring to allow access to quicker and more valuable diagnostic data. Prompt detection of AF and initiating
anticoagulation is critically important in reducing secondary AF related stroke, death, disability, hospitalisation and its
associated spiralling social care costs.
INTRODUCTION Patients with known AF, those (EY51Z, National schedule of NHS
Embolic stroke related to Atrial already prescribed anticoagulation costs for 2019 to 2020). An MDT
Fibrillation (AF) are often devastating or where anticoagulation would be pathway has been developed at
(~70% mortality or disability) contraindicated were excluded. Data UHNM to bypass conventional
and largely preventable with was analysed by cardiac physiologists cardiac monitoring in favour of
anticoagulation. CRYSTAL-AF with advanced training in cardiac direct ILR monitoring to allow
demonstrated prolonged cardiac rhythm management. In line with access to quicker and more
rhythm monitoring using an the local post stroke protocol; valuable diagnostic data. Prompt
implantable loop recorder (ILR) can AF>6minutes would reach the detection of AF and initiating
uncover a substantial proportion of threshold for anticoagulation. anticoagulation is critically
patients with AF that would otherwise important in reducing secondary
RESULTS AF related stroke, death, disability,
not be detected by conventional
short-term monitoring. NICE (2020) A total of 826 days of continuous hospitalisation and its associated
guidelines suggest a Medtronic monitoring was performed using spiralling social care costs.
Reveal LINQ™ device as an option to 24hr (37%), 48hr (15%) and 72hr
detect AF with negative, conventional (36%) ambulatory monitors and
non-invasive monitoring. A clear MDT wearable BARDY monitors up to
pathway was established at UHNM 14 days (12%). AF was detected in
for this cohort of patients to have 1 patient with a diagnostic yield
direct access to ILR implantation, of 0.25%. The waiting list for these
bypassing potentially substantial monitors was up to 11 weeks. In the
waiting times for conventional ILR arm, AF was detected in 15% of
monitoring. the 52 patients with an average time
to detection of 54.5 days during an
METHOD average continuous monitoring of
A retrospective service evaluation 229 days. All patients went on to
exploring the standard of care receive anticoagulation. The waiting
utilisation of cardiac 24hr to 14 day list for ILR insertion was no more
ambulatory and wearable monitors than 5 weeks.
was conducted in 400 patients over
CONCLUSION
6 months. 52 patients underwent
Medtronic Reveal LINQ™ insertion Opportunistic screening using
over a 17 month period. Inclusion conventional monitoring to detect AF
criteria included non-lacunar, acute post stroke has very low diagnostic
ischaemic stroke detected by MRI value but at significant fiscal cost to
or CT without identifiable cause. the NHS of circa £30K per annum
6 www.AFpioneers.org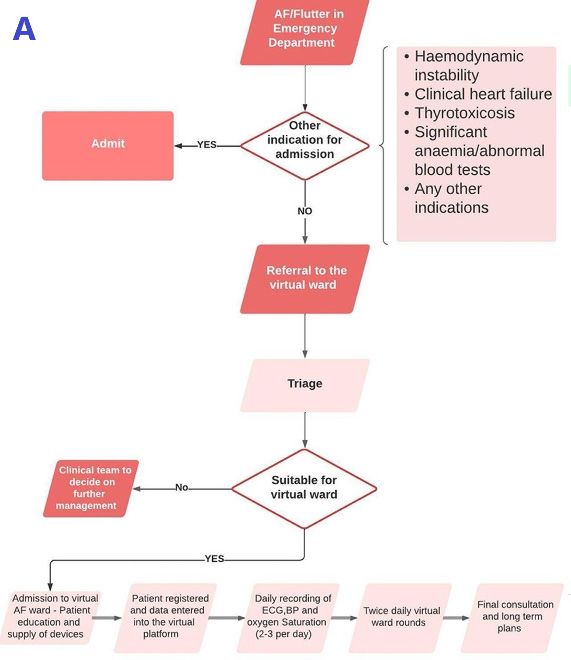
PHYSIOLOGIST-LED IMPLANTABLE LOOP RECORDER INSERTION TO DETECT ATRIAL
FIBRILLATION IN CRYPTOGENIC STROKE PATIENTS
MRS VICTORIA GURNEY, MRS REBECCA RANKIN
University Hospitals Plymouth NHS Trust, Plymouth, Devon
ABOUT THE CASE STUDY
A review of how advancing diagnostic technology can enhance the detection of
atrial fibrillation in cryptogenic stroke patients.
CASE STUDY CONTENT
An Implantable Loop Recorder (ILR) is a form of continuous monitoring over the course of up to four years. A
small device is implanted underneath the skin in the left pectoral region (usually) to monitor ECG on a continuous
loop, storing information according to pre-programmed settings for tachycardia, bradycardia, pauses and atrial
fibrillation (AF). This information is then accessed either via in clinic visits and device interrogation or, more
commonly, through the use of a home monitor which sends information to a secure online server, accessible by the
clinic remotely. Our initial implant for cryptogenic stroke was in March 2021. This referral came via inter-Consultant
referral; Neurologist to Cardiologist and then to us; Cardiac Physiologists. We felt this needed streamlining to allow
more timely monitoring of patients with cryptogenic stroke (CS) for which AF was suspected but not yet identified.
After multidisciplinary consultation with all relevant parties, we decided on the following criteria and guidelines:
• Recent stroke or Transient Ischaemic Attack (TIA) supported by consistency between symptoms and
findings on MRI or CT (not lacunar). TIA only if symptoms were speech problems, limb weakness or
hemianopsia, and there is a visible lesion on MRI/CT
• 12 lead ECG documenting sinus rhythm
• Prolonged non-invasive ECG monitoring with normal result as a minimum requirement
• Doppler USS carotids documenting absence of atheroma
• Intra-cardiac embolic cause excluded by transthoracic echocardiogram
• Absence of contra-indication to full anticoagulation. It was not considered appropriate to implant an ILR
in patients who already had an indication for chronic anticoagulation or previously documented AF.
With the introduction of this direct referral pathway, numbers increased and to date we have implanted 28 patients.
Even within this relatively short space of time (10 months) we have detected AF in 25% (7) of these patients.
Following detection of AF, a standardised letter with evidence of AF on ECG is sent to the patient’s GP to begin
anticoagulation. Prior to this, following detection of cryptogenic stroke, these patients will have been established on
antiplatelet medication. Patients will then be removed from follow-up and offered a device explant. Of our cohort of
28 patients, 1 will be receiving a pacemaker implant following detection of a 7 second sinus pause as an incidental
finding. We agreed to refer to our Cardiac Devices MDT in the event of finding clinically significant arrhythmias
outside of AF.
www.AFpioneers.org 7
IMPROVING STROKE PREVENTION IN DEVICE-DETECTED ATRIAL FIBRILLATION THROUGH
A MULTIDISCIPLINARY PATHWAY BETWEEN CARDIAC RHYTHM MANAGEMENT TEAM
AND STROKE PREVENTION IN ATRIAL FIBRILLATION (SOS-AF) SERVICE
MR NICK MILLS, VIKI CARPENTER, PAULINE HOUGH, DR ELIZABETH WARBURTON,
DR ISURU INDURUWA, DR KAYVAN KHADJOOI
Cambridge University Hospital NHS Foundation Trust
ABOUT THE CASE STUDY
Improving stroke prevention
in device-detected atrial
fibrillation.
INTRODUCTION
The SOS-AF service, run by
2 stroke prevention nurses
and 3 stroke physicians at
Cambridge University Hospitals
(CUH), screens for AF in
patients admitted to CUH;
reviews, manages and advises
secondary and primary care
on anticoagulation decisions.
Since its inception in 2017,
the service has grown to
include outpatient clinics as
well as close liaisons with indicated. If so, the patient and GP are pro- letters recommending GP to
other diagnostic services. actively contacted and informed (first-input). start anticoagulation were sent
Historically, if AF was detected Within a remote consultation, patients are (52: started on anticoagulation);
on a pacing device (PPM) or fully educated on AF, assisted to make an 29: advised anticoagulation not
implantable loop recorder informed decision on anticoagulation and indicated or contraindicated; 18:
(ILR) by the Cardiac Rhythm provided with a direct contact number. already on anticoagulation, dose
Management (CRM) team, a Individualised electronic letters are sent to correction advised in 4.
generic letter would be sent GPs on the same day covering anticoagulant
to the GP, however, the rates CONCLUSION
choice, dose, rate control, minimum review
of anticoagulation and time to frequency including when to repeat bloods This innovative pathway has led
prescription were very poor. and the importance of blood pressure to considerable improvement
OUTLINE OF THE management. in patient safety and patient
CARE PATHWAY satisfaction (informal feedback)
RESULTS
through rapid referral triage and
We have designed a In the first year (31/5/21 to 30/5/22), the timely contact with patients and
multidisciplinary pathway to SOS-AF service received 100 referrals (PPM GPs delivering education, advice
initiate collaboration between 90; ILR 10) from the CRM team (median; age and a practical management
CRM and SOS-AF services 80 (72-86), CHA2DS2-VASc 4 (3-5); females plan. This has led to a 98%
using CUH electronic patient 31%). The referrals were all triaged within 24 anticoagulation rate in patients
system. If AF is detected on hours (median days 1 (1-1)) and the median with device-detected AF who are
PPM or ILR, an electronic time between referral to first-input with eligible for anticoagulation, while
referral is made to SOS-AF patients was 3 days (1-12.5). 99% of referrals decreasing the workload and
service. The SOS-AF triages the had a final documented plan for stroke saving time for the primary care at
case and holistically considers prevention within a few days of referral: 53 no additional cost to the trust.
whether anticoagulation is
8 www.AFpioneers.org
ATRIAL FIBRILLATION VIRTUAL WARD - A GLIMPSE INTO THE FUTURE OF AF CARE
DR AHMED KOTB, MRS SUE ARMSTRONG, PROFESSOR G. ANDRÉ NG
University of Leicester - University Hospitals of Leicester NHS Trust
machine and pulse oximeter, with
instruction to record daily ECGs, blood
pressure, oxygen saturations and fill an
online AF symptom questionnaire via a
smart phone or electronic tablet. These
are lent to patients if needed, to avoid
digital exclusion. Data are uploaded to a digital platform (Dignio
Prevent by Dignio Ltd) which facilitates clinical review. Care pathway
and/or treatment virtual ward rounds occur at least twice daily with
clinical readings reviewed by the clinical team. Communication is
conducted through in-app messaging or video consultation. Clinical
support is available 7 days/week, 09:00-17:00. After hours, patients
are instructed to call the hospital switchboard and speak to the
on-call cardiology registrar if urgent advice is needed. Medication
adjustment is arranged through the hospital pharmacy. Remote
management continues until the patient is clinically stable for at least
24 hours and discharged from the virtual ward with a long-term plan.
RESULTS
There were 50 admissions to the virtual ward between January
and August 2022. In 24 patients, hospital admissions were avoided
ABOUT THE CASE STUDY with direct enrolment into virtual ward from the outpatient setting.
A further 25 re-admissions were appropriately prevented due
We aimed to develop an innovative and practice- to timely remote clinical interventions, saving a total of 98 - 245
changing pathway of care for patients with atrial hospital bed-days. The oldest
fibrillation through remote management. We patient enrolled was 87 years old
implemented a virtual AF ward which can act and two patients were registered
as an alternative to hospital-based care while blind. There were 3 patients who
maintaining similar safety and efficacy standards. required hospital readmission.
The NHS friends and family
INTRODUCTION
test participation rate was 90%
Atrial Fibrillation (AF) hospitalisations impose (n=45) and yielded 100% positive
significant burden on healthcare. A virtual responses.
ambulatory AF ward providing multidisciplinary
CONCLUSION
care with remote hospital-level monitoring could
reshape the future model of AF management. This is a first real-world experience
of a virtual ward for hospital
OUTLINES OF THE SERVICE
patients with fast AF who can be
An AF virtual ward was implemented at Glenfield safely managed remotely using a
Hospital, a UK tertiary centre as a proof-of- digital platform. It demonstrates
concept model of care. Patients presenting with a new work model with clear
a primary diagnosis of AF or atrial flutter who appetite among patients and
are haemodynamically stable with HR
IMPROVING CLINICAL OUTCOMES AND REDUCING HEALTH INEQUALITIES IN REMOTE
AND RURAL COMMUNITIES USING A TECHNOLOGY-ENABLED SOLUTION FOR
PAROXYSMAL ATRIAL FIBRILLATION MONITORING
DR DAVID MUGGERIDGE, MRS KARA CALLUM, MRS LYNSEY MACPHERSON,
MR NICK HOWARD, MRS CLAUDIA GRAUNE, PROF IAN L MEGSON,
DR ADAM GIANGRECO, MRS SUSAN GALLACHER, MRS LINDA CAMPBELL,
DR GETHIN WILLIAMS, DR ASHISH MACADEN, PROF STEPHEN J LESLIE
University of the Highlands and Islands, Edinburgh Napier
ABOUT THE CASE STUDY for a device either as an inpatient or
This was a joint working project between NHS Highland, outpatient. In the 100 patients who
the University of the Highlands and Islands, and Daiichi were referred for an R-TEST device, PAF was detected
Sankyo. It was led by Prof Steve Leslie (NHSH) with in 8.4% who had had a stroke and 5.9% with a TIA.
support from Dr Adam Giangreco (UHI) and Ms Karen Similarly, 9.3% of inpatients and 6.5% of outpatients were
Thomas (Daiichi Sankyo) who coordinated provision of identified with PAF. All patients with PAF were provided
funding for the purchase of R-TEST monitors. Dr David appropriate anticoagulation therapy. The incidence of
Muggeridge (Napier University) performed most of the
PAF in this evaluation (5.9-8.4%) was used to derive
data analysis.
a health economic model based on the 71% of NHS
CASE STUDY CONTENT Highland patients presenting with stroke or TIA and not
known to be in AF, an estimated secondary stroke risk of
Atrial Fibrillation (AF) is a major cause of recurrent 15 to 30% in patients with undiagnosed and untreated
stroke and transient ischaemic attack (TIA) in the UK. PAF, and a 66% reduction in secondary stroke risk in
As many patients can have asymptomatic paroxysmal AF patients following anticoagulation. Based on these
AF (PAF), prolonged arrhythmia monitoring is advised figures 4-11 patients with undiagnosed and untreated
in selected patients following a stroke or TIA. Each AF were predicted to be at high risk of secondary
year NHS Highland, Scotland’s largest health board stroke within one year of their initial stroke or TIA.
and representing a predominantly remote and rural Implementing R-TEST monitoring and anticoagulation
population, sees >600 patients with stroke or TIA, 68% of is predicted to prevent 3-7 of these secondary strokes.
whom have no AF detected at diagnosis. This evaluation The intervention is, therefore, projected to deliver a
assessed the clinical and health economic benefits of reduction of 78-182 inpatient bed days and annual gross
AF monitoring using R-TEST ECG devices. Patients were savings of £31,200 to £72,800. Accounting for additional
identified by a member of the stroke team and referred intervention costs, the annual net savings
to NHS Highland is estimated at up to
£35,235.75, or £5,033 per secondary stroke
prevented. This evaluation demonstrates
that establishing post-stroke AF
monitoring is feasible within existing NHS
resources. In addition to improving patient
care and reducing remote and rural health
inequalities, economic analysis suggests a
net financial benefit to the health board.
As a result, prolonged AF monitoring has
been established within NHS Highland for
all stroke and TIA patients in sinus rhythm
at the time of presentation. Full project
details are published in the British Journal
of Cardiology (Muggeridge D et al Br J
Cardiol 2022;29:46).
10 www.AFpioneers.orgPROTECT AND PERFECT - PREVENTING ATRIAL FIBRILLATION RELATED STROKES ACROSS A PRIMARY CARE NETWORK IN A DEPRIVED BOROUGH MR ANTONY GRAYSON AND MRS CAROL HUGHES Inspira Health OBJECTIVE Ensuring patients with atrial fibrillation (AF) are appropriately anticoagulated across West Knowsley Primary Care Network (PCN), a deprived borough in North-West England, with the primary goal of reducing AF-related strokes. OUTLINE OF SERVICE All GP practices in the PCN participated. The following approach was taken: Phase 1 - System interrogation to identify patients with AF from the clinical system; Phase 2 - Completion of 3 clinical audits; comprehensive patient case note review for AF patients not on anticoagulants; review of all DOAC patients, ensuring drug optimisation and in date bloods; independent assessment of warfarin patient safety; patients who were eligible for, but not on, anticoagulation. Phase 3 - Systematic patient invitation A further 11 (8%) patients taking VKA medications were for telephone consultations; Phase 4 - deemed sup-optimal with regards to INR control with TTR Specialist-led telephone clinics hosted
ESTABLISHING HIGHLY SPECIALISED MULTIDISCIPLINARY MANAGEMENT OF PATIENTS
UNDERGOING THIRD OR SUBSEQUENT ABLATIONS FOR AF OR
ATRIAL TACHYCARDIAS TRANSFORMS OUTCOMES
DR SHOHREH HONARBAKHSH, DR ANTHONY CHOW,
PROFESSOR ROSS J HUNTER
The Barts Heart Centre, St Bartholomew’s Hospital, Barts Health NHS Trust
ABOUT THE CASE STUDY An additional procedure was
recommended in 72 out of the 76
The aim of this study was to evaluate the impact a patients (94.7%). Comparing these patients to the 84 patients
specialist MDT approach had on third and subsequent that underwent ≥2 redo procedures over a 1 year period
AF/AT ablations at a single tertiary centre. The study pre-implementation of the meeting there was no significant
showed that the use of a specialist MDT greatly improved difference in baseline characteristics particularly with regards
outcomes for third and subsequent procedures through to LA size, number of previous procedures, LV function and
ensuring better patient selection, optimisation of co- BMI (Figure 1). Comparing procedural outcomes pre- and
morbidities, well thought out ablation strategies and post-implementation of the MDT there was a significant
operator selection. improvement in rates of freedom from AF/AT during a similar
INTRODUCTION follow-up period (47/72, 65.3%, 12.1±2.2 months, post
meeting vs. 30/84, 35.7%, 12.9±2.0 months, pre meeting;
Guidelines suggest selection for ablation is via a pPHARMACIST-LED INTERVENTION FOR ATRIAL FIBRILLATION IN
LONG-TERM CARE: THE PIVOTALL STUDY
MISS LEONA A RITCHIE1,2,6, DR PETER E PENSON1,2,3, DR ASANGAEDEM
AKPAN4,5, PROF GREGORY Y H LIP1,2,6, PROF DEIRDRE A LANE1,2,6
1. Liverpool Centre for Cardiovascular Science, University of Liverpool, Liverpool, L7 8TX, United Kingdom
2. Department of Cardiovascular and Metabolic Medicine, Institute of Life Course and Medical Sciences,
University of Liverpool, Liverpool, L7 8TX, United Kingdom
3. School of Pharmacy and Biomolecular Sciences, Liverpool John Moores University, Liverpool, L3 3AF,
United Kingdom
4. Musculoskeletal and Ageing Science, Institute of Life Course and Medical Sciences, University of Liverpool, L7 8TX, United Kingdom
5. Liverpool University Hospitals NHS Foundation Trust, Liverpool, L9 7AL, United Kingdom
6. Liverpool Heart and Chest Hospital, Liverpool, L14 3PE, United Kingdom
ABOUT THE CASE STUDY
A pharmacist-led medicines optimisation for older care
home residents with atrial fibrillation, based on the Atrial
Fibrillation Better Care pathway.
INTRODUCTION
Older care home residents are a vulnerable group
of people with atrial fibrillation (AF) who are under-
represented in research and may be offered sub-optimal
AF care. Few studies have addressed strategies to improve
their management in a holistic or integrated manner.
The Atrial Fibrillation Better Care (ABC: A, Avoid stroke; B,
Better symptom management; C, Cardiovascular and other
comorbidity optimisation) pathway is the gold-standard
AF management approach recommended in the 2020
European Society of Cardiology AF guidelines, but it is not
known how easy it is to use in older care home residents.
BRIEF OUTLINE OF SERVICE, CARE PATHWAY resident with a documented history of type 2 diabetes
but no record of blood glucose levels or evidence of
AND/OR TREATMENT prescription or oral antidiabetic medicines; (3) review
Researchers at the Liverpool Centre for Cardiovascular prescription of diltiazem and atenolol due to the
Science conducted a pilot and feasibility study of a potential for worsening of heart failure in a resident
pharmacist-led medicines optimisation based on the ABC who was complaining of increased breathlessness, and
pathway for older (aged ≥65 years) care home residents then (4) review antihypertensive medications in the
with AF living in Liverpool and Sefton, United Kingdom. same resident who was persistently hypertensive (blood
Where appropriate, the pharmacist made medication pressure >140/85mmHg). There were 17 other non-ABC
recommendations to residents’ general practitioners (GPs). pathway specific medicines recommendations made
Treatment suggestions for complex residents were agreed as part of the pharmacist review, and 15 (88%) were to
amongst a wider multi-disciplinary research team, including repeat blood tests for routine medication monitoring.
a pharmacist, health psychologist, consultant geriatrician CONCLUSION
and cardiologist, in advance of contacting the GP.
The ABC pathway provided a convenient framework
RESULTS for pharmacist-led medicines optimisation.
Twenty-one residents were recruited and 11 (mean age Recommendations made as part of the study
[SD] 85.0 [6.5] years, 63.6% female) received a pharmacist- supported GPs to manage older care home residents
led medicines optimisation. Four ABC pathway specific with AF at time of immense strain during the
medicines recommendations were made for three residents: COVID-19 pandemic. The ABC pathway promoted
(1) switch from warfarin to a non-vitamin K antagonist oral active decision making and individualised assessment
anticoagulant in a resident with time in therapeutic range of the net risk-benefit of pathway implementation inCASE STUDY DEMONSTRATING IMPROVED MONITORING AND PATIENT SAFETY
OUTCOMES FOR PATIENTS PRESCRIBED DOACS IN A BOROUGH IN SOUTH-EAST LONDON
RACHEL HOWATSON, HELEN WILLIAMS, SADHNA MURPHY
Southwark borough, South East London Integrated Care System (SEL ICS)
ABOUT THE CASE STUDY RESULTS
A quality and safety audit for the In 2019/20, 2115 DOAC patients were reviewed
prescribing of and service review at 33 practices and in 2020/21 an additional 221
for patients taking direct acting new DOAC patients were reviewed (see image
anticoagulants (DOACs) in primary care. for interventions made). Aim 1: 795/2115 (38%)
of patients required an up-to-date renal function calculation before
INTRODUCTION DOAC recommendations/actions could be made. Aim 2: 1024/2115
Appropriate monitoring of direct (48%) of patients required an urgent action (eg. a renal function check
oral anticoagulants (DOACs) is key to and/or a DOAC dose change). Of the patients with an accurate CrCl, 21
ensuring safe prescribing and optimal patients required an increased DOAC dose to optimise protection from
outcomes for patients. This project an AF-related stroke or thrombo-embolism and 47 patients required
focused on the quality and safety a reduced DOAC dose in line with Summary of Product Characteristics
of prescribing of DOACs in line with (SmPC) recommendations. Aim 3: 39 patients were referred to a
local guidelines. specialist (eg for a review of anticoagulation for Antiphospholipid
syndrome (APLS), antiplatelet therapy, low haemoglobin/platelets) and
METHOD
36 DOACs, 36 antiplatelets and 5 NSAIDs were stopped. Aim 4: 206/221
Data relating to the safety of DOAC (93%) of DOAC patients in the repeated audit had an annual renal
prescribing was collected at each GP function check and appropriate DOAC dose review compared to 62% in
practice. Patient specific issues were the first audit.
highlighted to the GP practice staff for
CONCLUSION
action. Updated prescribing guidance,
webinars and clinical support were As a result of this work, the quality and safety of prescribing of DOACs
offered to the practices to support across the Southwark borough has improved, with increased prescriber
them in addressing issues identified. confidence. Key themes from the initial audit have been used to inform
updates to local prescribing guidelines. The re-audit indicates that this
PROJECT AIMS
is now embedded as routine clinical practice.
1. To review the monitoring of
DOACs to ensure a bodyweight,
renal function and creatinine
clearance (CrCl) were recorded at
appropriate intervals.
2. To ensure that patients requiring
DOAC dose changes were
highlighted for urgent review by
the GP practice.
3. To review patients with contra-
indications or cautions to DOACs,
co-morbidities and/or concomitant
medicines that affect bleeding risk
to address any safety issues.
4. To ensure GP surgeries have a
process in place for the systematic
review of DOAC patients according
to local SEL guidance.
14 www.AFpioneers.orgTHE 2023 AF ASSOCIATION CENTRES OF EXCELLENCE
The following centres are acknowledged as an Atrial Fibrillation (AF) Centre of Excellence. As evidenced
by the work that has been published in this report, each centre takes an innovative approach to either
detecting, protecting, or correcting AF. Their work can be used to inspire other healthcare professionals to
correct practice by improving care and quality of life for people with atrial fibrillation.
AUSTRALIA
SYDNEY
Automated atrial fibrillation self-screening in general practice waiting rooms that doubled AF diagnosis rates
(AF Self-SMART: Atrial Fibrillation Self-Screening, Management And guideline-Recommended Therapy)
Heart Research Institute (Australia), University of Notre Dame (Australia)
Dr Katrina Giskes, Dr Nicole Lowres, Dr Jessica Orchard, Ms JiaLin Li, Dr Kirsty McKenzie, Assoc Prof Charlotte Hespe, Prof Ben Freedman
www.hri.org.au/our-research/heart-rhythm-stroke-prevention
UNITED KINGDOM
S TO K E O N T R E N T LEICESTER LONDON
The development of a novel MDT Atrial fibrillation virtual ward - a Establishing highly specialised
pathway for direct access ILR glimpse into the future of AF care multidisciplinary management of
technology to detect AF in patients University Hospitals of Leicester patients undergoing third or subsequent
post embolic stroke at UHNM NHS Trust ablations for AF or atrial tachycardias
University Hospital of Dr Ahmed Kotb, Mrs Sue Armstrong, transforms outcomes
North Midlands Professor G. André Ng The Barts Heart Centre, St
Mr Vincent Walker, Dr Savini Gunatilake, www.afvirtualward.co.uk Bartholomew’s Hospital, Barts
Mr Joseph Mayer, Dr Indira Natarjan, Health NHS Trust
Dr A Patwala, Miss F Parsonage INVERNESS Dr Shohreh Honarbakhsh,
www.uhnm.nhs.uk Improving clinical outcomes and Dr Anthony Chow, Professor Ross J Hunter
reducing health inequalities in www.bartshealth.nhs.uk/st-
P LY M O U T H remote and rural communities using bartholomews
Physiologist Led Implantable Loop a technology-enabled solution
Recorder Insertion to Detect Atrial for paroxysmal atrial fibrillation LIVERPOOL
Fibrillation in Cryptogenic Stroke monitoring Pharmacist-led intervention for atrial
Patients University of the Highlands and fibrillation in Long-term care: The
University Hospitals Plymouth Islands, Edinburgh Napier PIVOTALL study
NHS Trust Dr David Muggeridge, Mrs Kara Callum, Liverpool Centre for Cardiovascular
Mrs Victoria Gurney, Mrs Rebecca Rankin Mrs Lynsey Macpherson, Science, University of Liverpool, Liverpool
www.plymouthhospitals.nhs.uk/ Mr Nick Howard, Mrs Claudia Graune, Miss Leona A Ritchie, Dr Peter E Penson,
cardiology Prof Ian L Megson, Dr Adam Giangreco, Dr Asangaedem Akpan, Prof Gregory Y H Lip,
Mrs Susan Gallacher, Mrs Linda Campbell, Prof Deirdre A Lane
CAMBRIDGE Dr Gethin Williams, Dr Ashish Macaden, www.liverpool.ac.uk/health-and-life-
Improving stroke prevention in Prof Stephen J Leslie sciences/lccs/
device-detected atrial fibrillation
through a multidisciplinary K N O W S L E Y, M E R S E Y S I D E SOUTHWARK, LONDON
pathway between Cardiac Rhythm Protect and Perfect - Preventing Case study demonstrating improved
Management Team and Stroke Atrial Fibrillation Related Strokes monitoring and patient safety outcomes
Prevention in Atrial Fibrillation Across a Primary Care Network in a for patients prescribed DOACs in a
(SOS-AF) service Deprived Borough borough in South-East London
Cambridge University Hospital NHS Inspira Health Southwark borough, SEL ICS
Foundation Trust Mr Antony Grayson, Mrs Carol Hughes Rachel Howatson, Helen Williams,
Mr Nick Mills, Viki Carpenter, www.inspirahealth.co.uk/services/ Sadhna Murphy
Pauline Hough, Dr Elizabeth Warburton, primary-care-atrial-fibrillation- www.selondonccg.nhs.uk/what-we-
Dr Isuru Induruwa, Dr Kayvan Khadjooi service do/medicines-optimisation/south-
www.aftoolkit.co.uk/sos-af-the-af- east-london-integrated-medicines-
screening-service-at-addenbrookes- optimisation-committee-sel-imoc/
hospital-video/ cardiovascular-disease-guidance
www.cuh.nhs.uk
www.AFpioneers.org 15PROVIDING INFORMATION, SUPPORT
AND ACCESS TO ESTABLISHED, NEW
OR INNOVATIVE TREATMENTS FOR
ATRIAL FIBRILLATION
AF Pioneers & Centres of Excellence:
www.AFpioneers.org
E: info@afa-international.org
W: www.afa-international.org
Endorsed by
www.heartrhythmalliance.org
©AF AssociationYou can also read

















































