Socioeconomic Status and the Increased Prevalence of Autism in California
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
American Sociological Review
76(2) 320–346
Socioeconomic Status and the Ó American Sociological
Association 2011
Increased Prevalence of DOI: 10.1177/0003122411399389
http://asr.sagepub.com
Autism in California
Marissa D. Kinga and Peter S. Bearmanb
Abstract
The prevalence of autism has increased precipitously—roughly 10-fold in the past 40
years—yet no one knows exactly what caused this dramatic rise. Using a large and represen-
tative dataset that spans the California birth cohorts from 1992 through 2000, we examine
individual and community resources associated with the likelihood of an autism diagnosis
over time. This allows us to identify key social factors that have contributed to increased
autism prevalence. While individual-level factors, such as birth weight and parental educa-
tion, have had a fairly constant effect on likelihood of diagnosis over time, we find that com-
munity-level resources drive increased prevalence. This study suggests that neighborhoods
dynamically interact with the people living in them in different ways at different times to
shape health outcomes. By treating neighborhoods as dynamic, we can better understand
the changing socioeconomic gradient of autism and the increase in prevalence.
Keywords
neighborhoods, health gradient, autism, socioeconomic status, inequality
Autism is a disorder characterized by impair- changes in diagnostic criteria and an influx
ments in communication, social interaction, of resources dedicated to autism diagnosis
and repetitive behaviors. Over the past 40 may be critical to understanding why preva-
years, the measured prevalence of autism lence rates have risen. Increased awareness
has multiplied roughly 10-fold. While and social influence have been implicated
progress has been made in understanding in the rise of autism and a variety of compa-
some of the factors associated with increased rable disorders, where social processes
risk and rising prevalence, no one knows mimic the effects of contagion (Christakis
with certainty what causes autism or what and Fowler 2007; Liu, King, and Bearman
caused autism prevalence to rise so precipi- 2010; Pescosolido and Levy 2002). Studies
tously. There is, however, a growing aware-
ness among scholars that focusing solely on a
Yale University
individual risk factors such as exposure toxi- b
Columbia University
cants, prenatal complications, or parental
education is insufficient to explain why Corresponding Author:
Peter Bearman, Paul F. Lazarsfeld Center for the
autism prevalence rates have increased so Social Sciences, CB3355, Columbia University,
stunningly. Social and institutional processes New York, NY 10027
likely play an important role. For example, E-mail: psb17@columbia.eduKing and Bearman 321
have examined the contribution of changes in rates. In doing so, we present a more
diagnostic criteria and diagnostic substitution dynamic framework for understanding the
to rising autism prevalence rates, but the way in which individual and neighborhood
importance of institutional factors, resources characteristics interact over time to shape
for diagnosis, and greater awareness have not health outcomes. The majority of studies
been systematically assessed. The sociological that examine how neighborhoods and institu-
literature on health and inequality, however, tions shape inequalities in health are static
provides substantial motivation for exploring (Diez Roux and Mair 2010; Freese and Lut-
how individual- and community-level effects fey forthcoming; Sharkey 2008). Here, we
operate to shape the likelihood of an autism demonstrate that communities and institu-
diagnosis. tions do not passively exert the same influ-
This article examines why autism preva- ence over time; rather, neighborhoods have
lence has increased in the aggregate by different effects on different individuals and
exploring why autism prevalence has histori- different effects at different moments in the
cally been uneven across different communi- autism epidemic. Paying closer attention to
ties. Three processes could explain these temporality when trying to understand health
phenomena, both the unevenness and the inequalities can provide important insight
increase. First, the risk associated with a spe- into factors that may mitigate or exacerbate
cific factor could increase over time. If this the relationship between socioeconomic sta-
were the case, the size of the population at tus and health outcomes. By showing that
risk would remain constant but an increase the socioeconomic gradient for autism
in risk would drive the increase in prevalence. changed in the course of a decade, this
Second, risk factors could contribute to work suggests that socioeconomic health gra-
increased prevalence by becoming more prev- dients can and do change.
alent in the population. Third, the characteris-
tics of places could drive the rate of autism
diagnoses. Put another way, otherwise similar Socioeconomic Status,
children living in different areas could be at Fundamental Cause, and Health
significantly different risk for autism, not Gradients
because of their own characteristics, but
because of the characteristics of the communi- It is a sociological truism that social status
ties in which they reside. If sociologically affects one’s life chances, including one’s
salient community characteristics matter for health. The more resources people have, the
autism diagnosis, we should observe a strong less likely they are to experience disease or
temporal patterning of risk at the community early mortality. This generates the negative
level, such that increases and decreases in socioeconomic (SES) health gradients that
risk associated with community characteristics have been identified for a broad array of
map onto changing prevalence rates. In this conditions ranging from infant mortality to
article, we use a large geographically and tem- heart disease (Pamuk et al. 1998). The per-
porally sensitive multilevel data structure to sistence of health gradients across time
understand dynamics underlying the increased and in different contexts has given rise to
prevalence of autism by examining changes in the idea that SES status itself is a fundamen-
patterns of risk over nine birth cohorts. tal cause of health (Link et al. 1998; Link
This study makes two contributions to the and Phelan 1995). Within this framework,
empirical literature on autism by providing gradients are thought to be robust because
the first multilevel analysis of risk factors they operate through a multitude of
for autism and by identifying critical social micro-mechanisms (Link and Phelan 2002;
factors that map onto changes in prevalence Lutfey and Freese 2005), such that if access322 American Sociological Review 76(2)
to one health resource becomes saturated or Neighborhood context, independent of the
blocked, numerous other pathways are individuals composing the neighborhood, is
available through which the SES health gra- associated with all-cause mortality and
dient can be expressed. Health gradients are a host of negative health outcomes (Kawachi
believed to arise and persist because actors and Berkman 2003).2 Neighborhoods can
with more resources can devote more of influence health, independent of the individ-
those resources to their health. When tech- uals who compose them, through the physical
nological and medical advances create environment, the social environment, and by
opportunities for better health, educated structuring access to medical care and serv-
and wealthy individuals are disproportion- ices (Adler and Newman 2002; Roberts
ately able to exploit those opportunities. 1997). The physical environment can affect
Therefore, much of fundamental cause the- health directly and indirectly. Directly, it
ory relies on purposive agents’ use of can expose residents to toxicants. Indirectly,
resources (Freese and Lutfey forthcoming). it can structure opportunities to engage in
Progress in understanding how health dis- healthy behaviors, for instance by providing
parities can change has been stymied by an access to parks and playgrounds (for a review,
incomplete conceptualization of the mecha- see Kaczynski and Henderson 2008). Studies
nisms by which social and environmental exploring how the social environment may
contexts shape health outcomes and how affect health outcomes have examined fac-
these can change over time. With regard to tors such as a lack of social cohesion or dis-
the fundamental cause literature, the bulk of organization, which tend to increase stress
attention has been devoted to theorizing and isolation, thereby adversely impacting
about how and why health gradients should inhabitants’ health and well-being (Sampson,
endure. Relatively little attention has been Morenoff, and Gannon-Rowley 2002). Aside
given to empirically assessing whether, and from stress-mediated mechanisms, networks
under what conditions, health gradients can can influence health outcomes by shaping
change. However, the advent and diffusion how individuals identify and treat (or do
of new technologies has transformed socio- not treat) health problems (Pescosolido
economic gradients for cholesterol (Chang 1992). By structuring opportunities for social
and Lauderdale 2009) and cancer screening interaction through architecture or the quality
(Link et al. 1998). Autism is a particularly of their institutions, neighborhoods can affect
important case in this regard because there health outcomes through network-based
has not been a technological innovation in mechanisms. Finally, neighborhoods provide
the autism realm akin to cholesterol lowering differential access to health-related services,
statins or cancer identifying mammograms.1 such as sanitation, hospitals, and primary-
Autism diagnoses have always been based care providers (Matteson, Burr, and Marshall
solely on presentation. Because technological 1998).
change has had no impact, if we identify To date, research examining the role of
changes in the autism gradient, broader neighborhoods and social context in shaping
social processes are likely implicated. health outcomes has been largely static and
devoid of adequate mechanisms. Yet, neigh-
borhoods and institutions can interact with,
Socioeconomic Status, exacerbate, and mitigate the relationship
Neighborhoods, and Health between individual SES and health over
Gradients time (Auchincloss and Diez Roux 2009;
Freese and Lutfey forthcoming). Inert con-
It is well established that where people live ceptualizations of the role of neighborhoods
has an important effect on their health. are not confined to studies of healthKing and Bearman 323
outcomes, but pose a problem for under- us to link changing patterns of identification
standing stratification processes more and treatment to rising prevalence rates. We
generally (Sharkey 2008). While a few lon- discover that over the course of a decade,
gitudinal studies examine how individual a positive SES gradient for autism appears
health outcomes are shaped by neighbor- and then begins to reverse, a transformation
hoods over the life course (Carson et al. driven by changing patterns of identification
2007; Pollitt et al. 2008), little research ana- and treatment. Before we take these
lyzes how neighborhoods themselves may steps, however, we first consider what we
have different effects over time. This study know—and do not know—about the causes
contributes to efforts to address this short- of rising autism prevalence.
coming in the literature by allowing the
effects of neighborhoods to vary across
cohorts. By dynamically conceptualizing AN INTRODUCTION TO THE
how neighborhoods shape health outcomes
and tracking them over time and space, we
DETERMINANTS OF AUTISM
gain insight into the changing socioeco- Despite a growing body of research, the eti-
nomic gradient for autism and rising autism ology of autism remains unknown and highly
prevalence rates. uncertain. At the biological level, studies
examining parental, prenatal, perinatal, and
obstetric risk factors have identified a host
Roadblocks and a Roadmap of conditions associated with an increased
risk of autism. Prenatal and perinatal factors
It follows that combining insights from per- associated with an increased risk of autism
spectives emphasizing the role of individual include parental age (King et al. 2009), low
resources in inducing health inequalities birth weight (Eaton et al. 2001), low Apgar
with a dynamic conceptualization of the score (Eaton et al. 2001), fetal distress
way that neighborhoods influence health out- (Glasson et al. 2004), multiple births (Croen,
comes increases our ability to understand Grether, and Selvin 2002), small for gesta-
how gradients arise, persist, and change. tional age (Hultman and Sparen 2004; Lars-
We examine how the socioeconomic gradient son et al. 2005), and birth order (Durkin
for autism changes over time. We then turn et al. 2008). However, there is considerable
to the mechanisms that might account for inconsistency across studies, casting doubt
the gradient. Rather than focusing on tech- on which of these factors are truly associated
nology, we examine differences in the with increased autism risk (for a review, see
expression of SES across the autism spec- Kolevzon, Gross, and Reichenberg 2007).
trum.3 If ascertainment accounts for the Autism surely has a genetic component,
autism gradient, a positive SES gradient although how important it is remains unclear.
should be strongest for less severe cases. On one hand, the largest twin study to date
This follows from the idea that less severe estimates a concordance rate of 47.5 (95 per-
cases are harder to identify and diagnose, cent CI: 41.6–53.4), so there is indirect evi-
because the symptoms on which a diagnosis dence of substantial heritability (Liu, Zeruba-
is based are less prominent. Because a dispro- vel, and Bearman 2010). On the other hand,
portionate share of the increased caseload in molecular genetic research has not yet identi-
California arises from the high-functioning fied genetic causes for the vast majority (85
tail of the distribution (Liu, King, and to 98 percent) of all autism cases (Abrahams
Bearman 2010), a stronger SES effect for and Geschwin 2008).
less severe cases, which have disproportion- Environmental toxicants have also been
ately contributed to the increase, would allow highlighted as a potential cause. Currently,324 American Sociological Review 76(2)
five chemicals are known to cause neuro- persons diagnosed with autism in California,
developmental disorders, including autism. King and Bearman estimate that diagnostic
Additionally, another 200 chemicals are accretion and substitution may account for
known to have neuro-toxic effects in adults close to one-quarter of the increase in the
(Grandjean and Landrigan 2006). Thus, there California caseload. Hence, there is some
is strong reason to believe that chemical evidence that changes in diagnostic standards
exposure might be implicated in the autism and diagnostic substitution are driving some
epidemic. However, empirical studies inves- component of the observed increase in
tigating the role of environmental toxicants autism prevalence.
have been limited, and the two ecological Scholars have also investigated parental
studies that do exist (Palmer et al. 2005; social characteristics, such as socioeconomic
Windham et al. 2006) cannot causally disen- status, education, and occupation for possible
tangle aggregated and individual exposures correlations with autism. This literature is
or directly assess exposure.4 largely inconclusive (Croen, Grether, and
Turning to potential social sources of the Selvin 2002; Larsson et al. 2005; Palmer
epidemic, autism is difficult to diagnose et al. 2005). Early studies identified consis-
because there are no known biological tent associations between parental education
markers and the symptoms are hard to or socioeconomic status and autism (Finegan
assess, especially among persons with cog- and Quarrington 1979), while more current
nitive impairments. Diagnoses are based studies tend to find little to no association
solely on clinical presentation and parental between parental education, income, or
interviews. This fact has led some scholars wealth and autism (Larsson et al. 2005).
to suggest that diagnostic substitution plays However, a recent study by Durkin and col-
a significant role in the increasing preva- leagues (2010) using area-based measures
lence of autism (Shattuck 2006; Wing and of socioeconomic status found that preva-
Potter 2002). Evidence in support of the lence of autism increased with SES in
diagnostic substitution hypothesis arises a dose-response manner.
from a few recent studies that show Resources may matter because obtaining
increased autism rates accompanied by con- an autism diagnosis can be extremely
current declines in the prevalence of mental difficult. In obtaining a diagnosis and
retardation and other developmental disabil- services for their children, parents often
ities (Bishop et al. 2008; Coo et al. 2008; confront a dizzying institutional maze and
Shattuck 2006). spend considerable resources navigating
Independent of diagnostic substitution, through it. Some communities do not
some scholars argue that changes in diagnos- have qualified diagnosticians. Accordingly,
tic practices lie behind the increased preva- community resources—including screening
lence of autism. Of course, these scholars resources, service availability, educational
note that changing diagnostic practices and spending levels, the number of school-based
procedures accompany and are implicated health centers, and the number of pediatri-
in a process of diagnostic substitution. Since cians in a community—have been tied to
Kanner first described autism in 1943, diag- autism (Barbaresi et al. 2005; Mandell and
nostic standards, practices, and procedures Palmer 2005; Palmer et al. 2005). As with
have changed considerably (Fombonne studies of potential environmental toxicity,
2001). Research shows that changes in diag- the absence of a multilevel design makes it
nostic criteria prompt changes in diagnostic impossible to disentangle whether commu-
status, specifically from a sole diagnosis of nity resources have an independent effect
MR to a diagnosis of autism-MR (King and or are acting as proxies for aggregated
Bearman 2009). Drawing on a dataset of individual-level effects.King and Bearman 325
The growth in attention and resources data that allow us to simultaneously model
devoted to autism has been almost as individual and social contextual factors over
astounding as the rising prevalence rates. time. This study examines birth and diagnos-
Autism was the first specific disorder to tic records for all children born in California
have a Senate hearing focused exclusively between 1992 and 2000. We analyzed
on it (Insel 2007). Between 1997 and 2006, 4,906,926 birth records from this period. Of
funding for autism research by the National these, we could match 18,731 to children
Institutes of Health increased five-fold from with a diagnosis of autism. To identify
$22 million to $108 million (Singh et al. autism cases, we combined birth records
2009). The Centers for Disease Control and obtained from the California Birth Master
Prevention’s funding of autism activities Files and the California Department of
increased from $2.1 million in 2000 to about Developmental Services. The DDS coordi-
$16.7 million in 2005 (Government Account- nates diagnoses, services, and support for
ability Office 2006). And an additional $1 persons with developmental disabilities liv-
billion was committed to autism with the ing in California. The agency provides
signing of the Combating Autism Act in services to patients with autistic disorder
2006. The increase in resources devoted to (ICD-9-CM code 299.0).
autism research and treatment has far out- Our goal is to estimate a series of multi-
paced increasing prevalence rates. Between level models examining the association
1994 and 2004 in California, expenditures between individual- and community-level
by the Department of Developmental Serv- SES measures and the probability of an
ices (DDS), the agency responsible for serv- autism diagnosis across consecutive birth
ing persons with developmental disabilities cohorts. The analysis begins with the birth
in California, increased 160 percent. During cohort of 1992, the first year the DDS began
the same period, the agency’s caseload maintaining electronic records. To ensure
increased by 61 percent (DDS 2007). In Cal- that all children had ample time for case
ifornia, as in the rest of the country, there has ascertainment, the analyses end with the birth
been a dramatic increase in resources avail- cohort of 2000. All children were followed
able to screen for and to treat autism. from the time of birth until June 2006. We
What effect, if any, this influx of resour- allowed differential ascertainment times
ces has had on prevalence rates remains because the age of diagnosis for autism has
unknown. More basic questions about the been consistently falling, from a mean of
importance of parental and community 5.9 years (6 2.9) among the 1992 birth
resources for autism diagnoses remain unan- cohort to 3.8 years (6 .9) for the birth cohort
swered. The literature continues to debate of 2000.5
whether autism has a socioeconomic gradi-
ent. Accordingly, whether infusions of
resources into communities to diagnose and Individual-Level Variables
treat autism have coincided with changes in
the autism gradient and how, if at all, this To obtain demographic, prenatal, and perina-
may relate to prevalence rates present an tal information for persons with and without
important unsolved puzzle. autism, we electronically linked records from
the DDS and Birth Master Files using proba-
bilistic and deterministic matching algo-
rithms developed by Campbell (2004).
DATA AND METHODS Matches were made based on first, middle,
To make progress in answering these ques- and last name; date of birth; race; zip code
tions, we need to work with population-based at birth; and sex. We manually reviewed326 American Sociological Review 76(2)
uncertain matches. On average, 81 percent of in which they were born. California had
DDS files were linked to birth records. The 1,620 zip codes in 1992, this rose to 1,677
linkage rate increased over time from 79 per- numerical zip codes in 2000. We eliminated
cent (1992) to 86 percent (2000).6 zip codes with fewer than 10 births per
We extracted data on parental education year because neighborhood estimates based
and whether a child’s birth was paid for on small numbers of residents may be unreli-
with Medi-Cal (California’s Medicaid pro- able.7 To examine the importance of commu-
gram) from the matched files. These varia- nity resources for autism diagnoses, we con-
bles serve as proxies for socioeconomic sta- structed five community-level variables
tus. Roughly 40 percent of births in using zip codes as the unit of analysis. (See
California are paid for with Medi-Cal, so Table A1 in the Appendix for a more detailed
the program serves a considerable portion list.) From the 1990 and 2000 Censuses, we
of the population. Data on paternal education extracted the median property value of the
was missing for approximately 8 percent of zip code (logged) and the educational attain-
birth records. Maternal education was rarely ment for persons over 25 years. We catego-
missing. To avoid potential biases arising rized educational attainment as the percent
from missing data, we used the maximum of persons in the zip code with a college
education level of either parent as the child’s degree or higher. We used linear interpola-
parental education. To assess whether having tion to obtain data for intermediate years.
missing data on the father has any association Average property value and educational
with risk of autism, we included a dummy attainment correlate at r \ .35; it is thus
variable for missing paternal information. unlikely that problems arise from
From the birth certificates, we also multicollinearity.
obtained the following variables: birth To test for other community factors that
weight, parental age, duration of gestation, might influence the likelihood of an autism
whether the child was admitted to the neona- diagnosis, we aggregated data on the number
tal intensive care unit (NICU), and parity. of autism advocacy organizations, the num-
We calculated parental age similarly to ber of pediatricians, and the number of child
parental education to avoid problems arising psychiatrists operating in a zip code at the
from missing data. We examined birth time of the cohort’s birth. To obtain data on
weight categorically, with birth weight the number of autism advocacy organiza-
greater than or equal to 2,500 grams consid- tions, we searched Guidestar’s tax records
ered normal. Gestational age of fewer than for all organizations that identified ‘‘autism’’
35 weeks was considered pre-term. If a new- as their primary code under the National Tax-
born had a normal birth weight and gesta- onomy of Exempt Entities. Research organi-
tional age but was admitted to the NICU, zations have a different classificatory status.
the baby likely had poor presentation at birth. To identify less formal organizations, which
When these conditions were met, we may not request 501(c)3 status, we conducted
recorded ‘‘low Apgar proxy’’ as 1, otherwise exhaustive Internet searches. For organiza-
zero. We used parity to generate a dummy tions with local chapters, we recorded each
variable for first live birth. chapter as its own entity. For each organiza-
tion, we recorded a founding date, a dissolu-
tion date if applicable, and an address. We
Community-Level Data obtained data on the number of pediatricians
and child psychologists in a zip code from
The birth data files contain the zip code for Medical Marketing Services, who license
residence at birth, which makes it possible data from the American Medical Associa-
to nest individuals within the communities tion. We measured all variables at the timeKing and Bearman 327
of a cohort’s birth to mitigate problems aris- is group mean centered because there is sys-
ing from endogeneity. tematic variation in the mean parental educa-
tional level across zip codes. All level-two,
or community, variables are grand mean cen-
Severity tered. We include two cross-level interac-
tions to understand how the risk associated
To compare how risk is shaped by severity at
with an individual-level variable varies
first diagnosis, we constructed severity meas-
depending on the nature of the characteristics
ures using social and communication scores
of the community in which the individual
that are contained within the DDS’s Client
lives. We examine how the association
Development and Evaluation Report. We
between parental education and autism varies
additively converted nine items into an
depending on the percent of college gradu-
index, with each item equally weighted:
ates in the community, as well as how the
peer interaction, non-peer interaction, friend-
effect of being a Medi-Cal beneficiary on
ship formation and maintenance, participa-
autism varies depending on the median prop-
tion in social activities, unacceptable social
erty value in a community. In summary, the
behaviors, word usage, receptive language,
modeling strategy allows us to examine
and expressive language.8 Cronbach’s alpha
how individual- and community-level risk
for these items exceeds .75. Severe cases
factors for autism vary across time and with
are those above the mean evaluation score,
each other. The multilevel models use an
less severe cases are those below the mean.
unstructured covariance matrix. Because an
The distribution of severity scores is fairly
unstructured covariance matrix does not
symmetrical. Accordingly, the number of
impose any constraints and we have suffi-
severe and less severe cases is roughly equal.
cient statistical power, this is the most con-
The severity score is the score at time of
servative choice. We calculated predicted
entry into the DDS. Because a person enter-
probabilities of diagnosis from the models
ing the DDS at age 3 years will have a lower
in HLM. After reporting findings from anal-
score than someone entering at age 5 years—
yses by birth cohort, with an autism diagnosis
all else being equal, 5-year-olds are more
as the dependent variable, we then focus on
developed than 3-years-olds—we mean-cen-
level of severity.
tered severity scores by birth year and age
at entry.
RESULTS
Multilevel Analysis
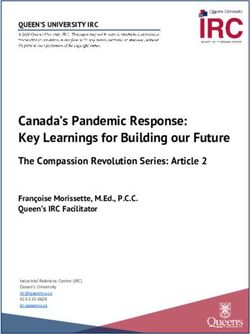
The prevalence of autism among the 1992
To simultaneously consider the association through 2000 California birth cohorts
between individual- and community-level increased considerably, from 29 per 10,000
factors over time, we ran a multilevel model in 1992 to 49 per 10,000 in 2000. Figure 1
for each birth cohort in HLM 6 (Raudenbush, shows this trend: rapid growth and then satu-
Bryk, and Congdon 2004). The dependent ration. Note that the x-axis reports birth
variable in the logistic regression is whether cohorts. Children born in 1992 are largely
a child received an autism diagnosis. diagnosed by 1998, whereas children born
Multilevel models take into account the hier- in 2000 are largely diagnosed by 2005.
archical nature of the social world. Here we Just as there is significant variation in the
consider individuals nested within neighbor- probability of diagnosis over time, we also
hoods, captured by zip code. All of the observe significant variability in the proba-
individual-level variables are grand mean bility of diagnosis between zip codes. The
centered, except parental education, which estimated variance of b0k, t00, is statistically328 American Sociological Review 76(2)
55
50
45
Prevalence Per 10,000
40
35
30
Prevalence by Birth Cohort
25
1992 1993 1994 1995 1996 1997 1998 1999 2000
Figure 1. Autism Prevalence by Birth Cohort
significant at the p \ .01 level in all of the become more prevalent in the population.
unconditional models, except for the model Alternatively, the population at risk could
for the 1995 birth cohort ( p = .09). remain fairly constant but an increase in the
(See Part A in the online supplement for risk of a factor could drive the increase in
a complete table [http://asr.sagepub.com/ prevalence. If this were true, we would
supplemental].) The observed variability in expect to see the risk increase or decrease
prevalence rates is consistent with the identi- in concert with prevalence rates.
fication of statistically significant autism
clusters in California, in which the risk for Individual-Level Factors
autism is four times greater than the risk in
other parts of the state (Mazumdar et al. We first turn to the individual-level factors
2010). The observed variance remains statis- examined in our model. Table 1 summarizes
tically significant in the individual and the results for each of the multilevel models
neighborhood models. Only in the complete by birth cohort.9 Odds ratios and 95 percent
multilevel model is the variance reduced to confidence intervals for each variable appear
statistical insignificance, indicating that our under the year for each birth cohort. As Table
model accounts for the observed variability 1 shows, Medi-Cal, birth order, normal birth
in diagnoses between zip codes. weight, being male, paternal age, and pater-
As we turn to examine the risk factors nal education are consistently associated
associated with autism, recall that a factor with autism risk across all birth cohorts.
could account for the increased prevalence Being a first-born child, a boy, or having
of autism by meeting one of two criteria. older or more educated parents increased
One possibility is that a risk factor may the risk for autism. Increasing parental ageTable 1. Risk Factors for Autism
1992 1993 1994 1995 1996 1997 1998 1999 2000
OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI
Intercept .002 (.001,.002) .002 (.002,.002) .002 (.002,.002) .002 (.002,.002) .003 (.002,.003) .003 (.003,.003) .003 (.003,.003) .003 (.003,.003) .003 (.003,.004)
Individual Level
Medi-Cal .90 (.83,.98) .64 (.57, .72) .66 (.61,.72) .82 (.75, .89) .96 (.89,1.03) .88 (.83,.95) .91 (.84,.98) .85 (.79,.93) .97 (.90,1.03)
First Born 1.13 (1.05,1.23) 1.15 (1.07, 1.24) 1.14 (1.06,1.23) 1.17 (1.09, 1.26) 1.18 (1.10,1.25) 1.13 (1.07,1.20) 1.24 (1.16,1.32) 1.28 (1.21,1.37) 1.25 (1.18,1.32)
Premature 1.01 (.91,1.13) .79 (.87,1.24) 1.07 (.96,1.20) 1.07 (.97, 1.19) .98 (.89,1.08) 1.11 (1.02,1.21) 1.14 (1.04,1.24) 1.09 (.97,1.17) 1.23 (1.13,1.33)
Normal Weight .82 (.70,.96) .70 (.60,.81) 1.03 (.87,1.21) .84 (.73, .98) .73 (.64,.83) .74 (.66,.83) .77 (.68,.86) .80 (.70,.91) .84 (.75,.95)
Male 4.13 (3.80,4.50) 4.03 (3.72,4.37) 4.61 (4.25,5.00) 4.14 (3.82, 4.49) 4.81 (4.48,5.16) 4.53 (4.25,4.84) 4.07 (3.79,4.38) 4.23 (3.96,4.53) 4.25 (3.99,4.54)
Low Apgar 1.13 (.80,1.59) 1.23 (.90,1.69) 1.30 (.98,1.72) 1.28 (.96, 1.72) .92 (.71,1.20) 1.17 (.93,1.48) 1.21 (.96,1.53) .96 (.75,1.24) 1.35 (1.08,1.68)
Max Parental 1.03 (1.03,1.04) 1.04 (1.04,1.05) 1.03 (1.02,1.03) 1.03 (1.03, 1.04) 1.03 (1.03,1.04) 1.04 (1.03,1.04) 1.04 (1.03,1.04) 1.03 (1.03,1.04) 1.04 (1.03,1.04)
Age
Education 1.15 (1.13,1.16) 1.13 (1.11,1.14) 1.11 (1.09,1.13) 1.11 (1.09, 1.12) 1.13 (1.12,1.15) 1.08 (1.07,1.10) 1.10 (1.09,1.12) 1.10 (1.09,1.12) 1.09 (1.08,1.11)
Missing Father .99 (.84,1.16) 1.42 (1.23,1.64) 1.15 (.96,1.40) 1.12 (.96, 1.31) 1.20 (1.06,1.35) 1.25 (1.13,1.38) 1.03 (.92,1.17) .98 (.87,1.12) 1.11 (1.00,1.24)
Neighborhood Level
Logged 1.64 (1.38,1.96) 1.43 (1.24. 1.67) 2.06 (1.82,2.34) 1.85 (1.62, 2.10) 1.51 (1.34,1.71) 1.68 (1.49,1.88) 1.48 (1.33,1.65) 1.48 (1.33,1.65) 1.34 (1.21,1.49)
Property
Percent College .84 (.46,1.53) 1.24 (.74,1.67) .65 (.42,1.01) .56 (.35, .90) .87 (.57,1.34) .70 (.46,1.04) .85 (.59,1.24) .82 (.57,1.19) .99 (.69,1.43)
Graduate
Cross Level
Medi-Cal x .90 (.74,1.10) 1.44 (1.18, 1.74) 1.53 (1.28,1.83) 1.07 (.90, 1.28) 1.29 (1.12,1.49) 1.19 (1.03,1.36) 1.00 (.85,1.17) 1.15 (.99,1.34) 1.52 (1.34,1.71)
Property
Education x .83 (.75,.93) .91 (.82,1.02) .85 (.78,.94) .92 (.83, 1.03) .99 (.90,1.08) .86 (.81,.93) .90 (.82,.99) .89 (.83,.96) .91 (.85,.98)
Percent
College
Random Effects Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD
Intercept .10 .32 .11 .32 .13 .36 .09 .30 .15 .38 .19 .44 .15 .39 .12 .35 .17 .42
Medi-Cal Slope .03 .16 .07 .26 .03 .18 .03 .18 .07 .25 .05 .22 .04 .19 .08 .28 .05 .22
Education .003 .05 .001 .04 .001 .03 .001 .04 .001 .04 .001 .02 .002 .05 .002 .04 .001 .03
Slope
Note: Odds ratios for factors examined for a potential association with autism risk appear in the column labeled OR. An odds ratio over one indicates an increased risk
for autism. An odds ratio of less than one suggests that the variable is associated with a decreased risk for autism. The 95 percent confidence intervals appear in
parentheses. Factors that are statistically significant at the p .05 level appear in bold. The year heading for each column indicates the birth cohort that the results
pertain to. The estimated variance of b0k , t00 is statistically significant in the unconditional model for all years at p \ .001 except 1995.
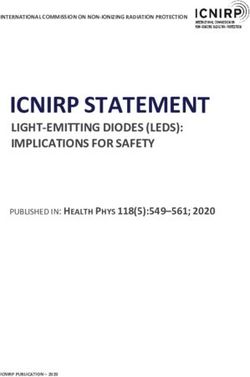
329330 American Sociological Review 76(2) may increase risk of autism as a result of the is group mean centered; therefore, odds ratios increasing likelihood of de novo mutations represent the effect of parental education rela- that occur with age (Liu, Zerubavel, and tive to the average level of parental education Bearman 2010). Alternatively, parental age within a child’s neighborhood. Having more could be an indirect proxy for elements of education relative to one’s neighbors is associ- socioeconomic status not captured by educa- ated with an increased risk of autism diagnosis. tion and property values, as parents of higher Only the effects of Medi-Cal reveal mean- SES tend to delay childbirth (Baldwin and ingful periodicity. Among the birth cohorts of Nord 1984). Conversely, being on Medi- 1993 until 1995, Medi-Cal receipt reduced the Cal, our measure of income status, is associ- odds of an autism diagnosis by roughly 20 to ated with a decreased risk of an autism diag- 40 percent. Accordingly, autism had a positive nosis. Being male is associated with a four- socioeconomic gradient. Individuals with fold greater risk of autism diagnosis. The greater resources were more likely to receive gender gap in autism prevalence (mirrored an autism diagnosis. Early in the epidemic, in ADHD) remains unexplained (Baron- individuals relying on Medi-Cal for health Cohen, Knickmeyer, and Belmonte 2005).10 care likely did not have the resources neces- Birth weight in excess of 2,500 grams reduced sary to acquire an autism diagnosis. Note the likelihood of an autism diagnosis in the that the strength of the positive SES gradient majority of cohorts, suggesting that low birth waned among later cohorts as diagnoses weight increases risk for autism. Premature became increasingly prevalent and knowledge birth, in which the gestational age was fewer about the disorder diffused widely. By the than 35 weeks, is associated with increased 2000 birth cohort, the odds ratio for Medi- risk of autism in three out of nine years, reach- Cal was .97 (.90, 1.03), suggesting that the ing statistical significance only in later years. positive socioeconomic gradient was disap- This could be due to the increased survival pearing. With the exception of Medi-Cal, the rate among premature births. The consistent individual-level variables in our model do birth-order effect indicates that first-born chil- not exhibit periodicity in risk consistent with dren are at greater risk for autism. Possible changing prevalence rates. mechanisms to account for this finding Similarly, there is little variation in the involve the concentration of fat-soluble chem- prevalence of any of the risk factors in the icals in maternal milk and tissue, slower population. While average parental age and development of immune systems due to fewer the proportion of births that were premature exposures to infections, and the statistical or had poor presentation all increased, these effect of parents who stop having children increases are not large enough to make after having a child with autism (Durkin even a minimal contribution to increases in et al. 2008). autism prevalence. (See Table A1 in the Turning to the temporal variability and peri- Appendix for a summary of demographic odicity of individual risk factors, we observe changes across cohorts.) Accordingly, it is that the majority of individual-level factors unlikely that the increasing prevalence of have a consistent effect size. As Figure 2 dem- an individual-level risk factor in the popula- onstrates, the odds ratios for parental age are tion accounts for the observed increase in largely invariant across birth cohorts, ranging autism prevalence. from 1.03 (95 percent CI: 1.03, 1.04) to 1.04 (95 percent CI: 1.03, 1.05). Parental education Neighborhood Wealth and Autism is similarly stable, varying from a high of 1.15 (95 percent CI: 1.13, 1.16) to a low of The effect of community wealth on the 1.08 (1.07, 1.10). Recall that parental education chance of acquiring an autism diagnosis is
King and Bearman 331
1.3 1.5
A C
First Born
1.25 Parental Age
1.4
1.2
Odds Ratio
1.3
Odds Ratio
1.15
1.2
1.1
1.1
1.05
1 1
1992 1993 1994 1995 1996 1997 1998 1999 2000 1992 1993 1994 1995 1996 1997 1998 1999 2000
1.3 1.1
B D
Education Medi-Cal
1.25 1
1.2 0.9
Odds Ratio
Odds Ratio
1.15 0.8
1.1 0.7
1.05 0.6
1 0.5
1992 1993 1994 1995 1996 1997 1998 1999 2000 1992 1993 1994 1995 1996 1997 1998 1999 2000
Figure 2. Graphic Representation of the Odds Ratios and Confidence Intervals Obtained for
Select Individual-Level Variables
Note: The multilevel models used to obtain the point estimates for each birth cohort adjust for all of the
individual- and community-level covariates and their interactions listed in Table 1.
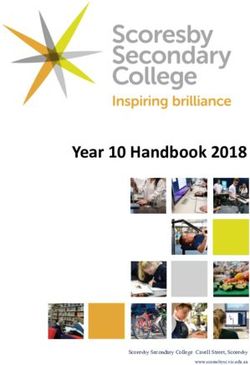
of central interest. Figure 3 plots the odds the predicted probability of an autism diag-
ratios for logged median property values nosis for children who do and do not receive
over time and demonstrates that the effect Medi-Cal in communities with very high
of community wealth varies with changes (top 90 percent) and very low (bottom 90
in prevalence rates. The grey line tracks percent) median property values. The y-
the percent change in prevalence over the axis can be thought of as a prevalence
previous period (or the rate of increasing rate. Figure 4a reports the probability of an
prevalence). The effect size of community autism diagnosis for children whose birth
property values appears in black. The corre- was paid for by Medi-Cal and who reside
lation between the odds ratio for property in a neighborhood in the bottom decile of
value and changes in prevalence across the the neighborhood property distribution
cohorts is .71. These results indicate that (dashed line) compared with the ‘‘same’’
the economic composition of a community child residing in a neighborhood in the top
matters most when prevalence rates are ris- decile (solid line) of the property value dis-
ing. As diagnoses became more common tribution. A child born on Medi-Cal and
and the rate of increase slowed, the impor- residing in the wealthier neighborhood
tance of community wealth declined. was, on average, close to 250 percent more
Turning to how prevalence rates vary by likely than his counterpart living in a poorer
levels of individual and community eco- neighborhood to be diagnosed with autism.
nomic resources, we now consider cross- This can be seen by comparing the differ-
level interactions. Figures 4a and 4b plot ence in prevalence rates between the solid332 American Sociological Review 76(2)
2.2 16
14
2
12
Percent Change in Prevalence
1.8
10
Odds Ratio
1.6 8
6
1.4
4
1.2
2
1 0
1992-1993 1993-1994 1994-1995 1995-1996 1996-1997 1997-1998 1998-1999 1999-2000
Property Value Change in Prevalence
Figure 3. Comparison of Odds Ratios for Property Values and Changes in Prevalence Rates
Note: The black line tracks the changing effect size of logged property values at the zip code level across
successive birth cohorts. The grey line tracks changes in prevalence rate.
and dotted lines in Figure 4a. Moreover, the of obtaining an autism diagnosis. However,
importance of neighborhood context the diagnostic rate among this group was
increased over time, as seen by diverging stagnant after 1994. Diagnoses among
prevalence rates in wealthier and poorer wealthier individuals in wealthier neighbor-
neighborhoods. hoods appear to have hit a ceiling around 40
By contrast, for a child whose birth was per 10,000. By contrast, prevalence rates
not paid for by Medi-Cal (see Figure 4b), among children whose birth was paid for
moving from the bottom decile (dashed by Medi-Cal living in these same neighbor-
line) to the top decile (solid line) of the hoods experienced consistent increases from
property value distribution increased the 20 per 10,000 in 1992 to 46 per 10,000.
probability of diagnosis by 190 percent, on Similarly, the probability of diagnosis for
average, over the same period. Although children living in the poorest neighborhoods
community resources matter, they matter increased steadily across cohorts, although
less than if the child received Medi-Cal. at a slower rate. In summary, neighborhood
Finally, the predicted probabilities reveal resources matter tremendously for autism
an important temporal pattern that yields prevalence rates. However, they matter
insight into changes in the socioeconomic much more for children born to parents
gradient for autism. Recall that autism ini- with fewer economic resources. The trends
tially had a strong positive socioeconomic presented here add further support to the
gradient. Children born to wealthier and notion that the socioeconomic gradient for
more educated parents living in wealthy autism has begun to reverse. In wealthy
neighborhoods had the highest probability communities, the socioeconomic gradientKing and Bearman 333
0.005
0.004
Probability of Autism Diagnosis
0.003
0.002
0.001
0.000
1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
10th Percentile Property Value 90th Percentile Property Value
Figure 4a. Community Effect of Property Value on Medi-Cal Recipients
Note: Figure shows the probability of diagnosis for children receiving Medi-Cal residing in communities
at the bottom decile (dashed line) compared with the top decile (solid line) of property value.
0.005
0.004
Probability of Autism Diagnosis
0.003
0.002
0.001
0.000
1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
10th Percentile Property Value 90th Percentile Property Value
Figure 4b. Community Effect of Property Value on Non–Medi-Cal Recipients
Note: Figure shows the probability of diagnosis for children not receiving Medi-Cal residing in commu-
nities at the bottom decile (dashed line) compared with the top decile (solid) of property value.334 American Sociological Review 76(2)
for autism has flattened; a different picture likelihood of diagnosis. Supplementary
arises from poorer communities. analyses, which included breast cancer
advocacy organizations, suggest that this
Neighborhood Educational relationship is likely due to ecological fac-
Attainment tors, rather than the presence of autism
organizations themselves. Furthermore,
Educational attainment in a neighborhood inclusion of all the supplementary variables
had a small effect on the likelihood of an has very little effect on other measures of
autism diagnosis. In contrast to the results socioeconomic status included in the model.
for economic resources, educational resour- This suggests that whatever socioeconomic
ces primarily operate at the individual level, status is capturing, it is not the availability
as reported in Figures 5a and 5b. Comparing of health care providers or advocacy
Figure 5a, which shows the probability of organizations.
diagnosis for a child whose parents are at
the 25th percentile of education relative to Severity
their neighbors, with Figure 5b, which plots
the probability of diagnosis for a child While we gained little by trying to measure
whose parents are in the top 75th percentile health care resources in a community, insight
of education, we see that diagnoses are con- into possible mechanisms that could account
sistently more likely for children born to rel- for the changing autism gradient does arise
atively more educated parents. However, the by looking at whether there are differences
overall effect of education at the parental or in socioeconomic status by severity. More
community level appears to be relatively severe cases are easier to identify, because
weak. the symptoms upon which a diagnosis are
made are less ambiguous. It follows that if
Health Care Resources differential ascertainment and diagnostic
capacity underlie the SES gradient, we
Of course, property values are likely acting should be able to observe this by comparing
as proxies for more meaningful mechanisms. SES gradients for more and less severe cases.
One way to address more proximate mecha- When autism cases are split by severity,
nisms is to try to identify variables that prop- a striking pattern is revealed. Less severe
erty value may capture. We consider three cases are disproportionately found in wealth-
variables—the number of pediatricians, child ier and more educated neighborhoods. Figure
psychiatrists, and autism advocacy organi- 6 shows the ratio of less severe to more
zations in each community—to try to under- severe cases with respect to neighborhood
stand whether access to health care or expo- wealth and education. Recall that we split
sure to organizations committed to severity at the mean, so there are relatively
increasing awareness about autism might equal numbers of more and less severe cases
afford a more detailed understanding of var- in the population. If severity were indepen-
iability in autism prevalence rates across dent of neighborhood context, we would
time and communities. None of these varia- expect the ratio to be roughly one to one.
bles are substantively important for the like- This is not the case. The most diagnostically
lihood of an autism diagnosis. As Table 2 ambiguous cases, those that are the hardest to
shows, while the number of pediatricians identify and diagnose because the symptoms
and child psychologists are statistically that provide a basis for diagnosis are less pro-
significant in many years, their effect nounced, are disproportionately found in
size is small. Autism organizations are occa- educated and wealthy neighborhoods. Thus,
sionally negatively associated with the the observed SES gradient for autism is atKing and Bearman 335
0.005
25th% Parental Education
75th% Parental Education
Probability of Autism Diagnosis
0.004
0.003
0.002
0.001
0.000
1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
Less Educated Area More Educated Area
Figure 5a. Community Effect of Education on Children Born to Parents with Less Education
Note: Figure shows the probability of diagnosis for children whose parents are at the 25th percentile of
education residing in areas with a lower percentage of college graduates (dashed line) compared with
a higher percentage of college graduates (solid line).
least partially driven by identification and reversing and becoming negative. Parental
ascertainment. education, shown in Panel B, is positively
Odds ratios obtained from multilevel associated with the likelihood of both
models examining the probability of a more a more severe and a less severe diagnosis.
or less severe diagnosis add further support Odds ratios are higher, however, for less
to the assertion that differential ascertain- severe cases, relative to more severe cases,
ment may be driving the socioeconomic gra- consistent with our observations for income.
dients, and hence increased prevalence. Fig- Turning to community-level factors, we
ure 7 presents these results graphically. find a positive, although generally insignifi-
(See Part B of the online supplement for cant, effect of community educational attain-
complete tabular results.) ment for less severe cases. Neighborhood
Odds ratios for more severe cases are property value matters for case identification
shown in black, those for less severe cases for more and less severe cases. This is con-
are shown in grey. As Panel A shows, the sistent with the overall importance of prop-
effect of Medi-Cal is always stronger for erty value identified with all autism cases.
less severe cases; that is, the grey line Of note, however, is the declining signifi-
(odds ratio for less severe cases) always cance of property value for more severe cases
appears below the black line (odds ratio after the 1994 cohort. This pattern is almost
for more severe cases). By 1997, odds ratios identical to the one observed when we con-
for Medi-Cal for more severe cases gener- sider all autism cases together. In summary,
ally exceed one, suggesting that the socio- if less severe cases are more difficult to
economic gradient for severe cases may be identify, then differential ascertainment336 American Sociological Review 76(2)
0.005
25th% Parental Education
75th% Parental Education
0.004
Probability of Autism Diagnosis
0.003
0.002
0.001
0.000
1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
Less Educated Area More Educated Area
Figure 5b. Community Effect of Education on Children Born to Parents with More Education
Note: Figure shows the probability of diagnosis for children whose parents are at the 75th percentile of
education residing in areas with a lower percentage of college graduates (dashed line) compared with
a higher percentage of college graduates (solid line).
capacity at the community level may be one will be more important than a community’s
mechanism through which SES effects oper- general education level. This appears to be
ate. The stronger effects of socioeconomic the case with autism, because access to
status on less severe cases provide support a highly trained specialist—not just any
for this idea.11 Recall that the majority of specialist—is often critical to getting a
the increased caseload in California arose diagnosis. Similarly, because granular
disproportionately from an increased num- information is more easily transmitted
ber of less severe cases. Patterns of ascer- through embedded social relations (Uzzi
tainment and identification underlie not 1996), the diffusion of information about
only the autism gradient but also the autism through communities likely occurs
increased prevalence of autism in around foci of repeated parental interac-
California. tions, rather than through more traditional
Results for neighborhood education and institutions, as shown by Liu, King, and
community resources provide some clues Bearman (2010).
about the type of information that may be
required for identification and ascertain- CONCLUSIONS
ment. These results suggest that specialized,
granular knowledge is likely required for Limitations and Robustness Checks
diagnosis. When specialized knowledge is
costly to obtain or difficult to access, the This study has several limitations. First, we
financial resources available in a community interpolated the property value data used inTable 2. Risk Factors for Autism Including Health Care Resources
1992 1993 1994 1995 1996 1997 1998 1999 2000
OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI OR 95% CI
Intercept .002 (.002, .002) .002 (.002, .002) .002 (.002, .002) .002 (.002, .002) .002 (.002, .003) .003 (.003, .003) .003 (.003, .003) .003 (.003, .003) .003 (.003, .004)
Individual Level
Medi-Cal .89 (.82, .97) .72 (.66, .80) .66 (.59, .74) .81 (.74, .88) .95 (.88, 1.02) .85 (.80, .92) .89 (.83, .97) .85 (.78, .93) .96 (.90, 1.02)
First Born 1.13 (1.05, 1.23) 1.15 (1.07, 1.24) 1.14 (1.05, 1.25) 1.17 (1.09, 1.26) 1.18 (1.10, 1.26) 1.13 (1.06, 1.20) 1.23 (1.17, 1.32) 1.28 (1.21, 1.37) 1.24 (1.18, 1.32)
Premature 1.01 (.91, 1.13) .97 (.86, 1.10) 1.07 (.94, 1.23) 1.07 (.96, 1.20) .98 (.88, 1.08) 1.11 (1.01, 1.21) 1.14 (1.05, 1.24) 1.07 (.97, 1.17) 1.22 (1.13, 1.32)
Normal .82 (.70, .96) .70 (.60, .82) 1.03 (.85, 1.25) .84 (.73, .98) .73 (.64, .83) .74 (.66, .83) .77 (.69, .86) .80 (.70, .90) .84 (.75, .95)
Weight
Male 4.13 (3.80, 4.50) 4.04 (3.73, 4.39) 4.61 (4.15, 5.12) 4.14 (3.82, 4.49) 4.82 (4.48, 5.17) 4.57 (4.27, 4.90) 4.07 (9.80, 4.37) 4.23 (3.95, 4.52) 4.23 (3.97, 4.51)
Low Apgar 1.13 (.80, 1.59) 1.23 (.89, 1.70) 1.30 (.92, 1.85) 1.28 (.96, 1.72) .92 (.77, 1.20) 1.16 (.92, 1.49) 1.21 (.96, 1.52) .96 (.75, 1.24) 1.35 (1.09, 1.67)
Max Parental 1.03 (1.03, 1.04) 1.04 (1.04, 1.05) 1.03 (1.02, 1.04) 1.03 (1.03, 1.04) 1.03 (1.03, 1.04) 1.04 (1.03, 1.04) 1.04 (1.03, 1.04) 1.03 (1.03, 1.04) 1.04 (1.03, 1.04)
Age
Education 1.14 (1.13, 1.16) 1.13 (1.11, 1.15) 1.11 (1.09, 1.13) 1.11 (1.09, 1.13) 1.13 (1.12, 1.15) 1.09 (1.08, 1.11) 1.09 (1.08, 1.11) 1.10 (1.09, 1.12) 1.08 (1.07, 1.09)
Missing .99 (.84, 1.16) 1.43 (1.24, 1.65) 1.15 (.91, 1.46) 1.12 (.96, 1.31) 1.19 (1.06, 1.35) 1.24 (1.12, 1.39) 1.04 (.93, 1.16) .98 (.87, 1.12) 1.11 (1.01, 1.23)
Father
Neighborhood Level
Logged 1.64 (1.37, 1.95) 1.59 (1.41, 1.80) 2.05 (1.73, 2.43) 1.84 (1.62, 2.09) 1.52 (1.34, 1.72) 1.68 (1.48, 1.90) 1.46 (1.32, 1.63) 1.47 (1.32, 1.64) 1.33 (1.20, 1.47)
Property
Percent .84 (.46, 1.53) .90 (.57, 1.41) .61 (.34, 1.11) .48 (.29, .76) .75 (.49, 1.18) .57 (.37, .87) .85 (.58, 1.25) .74 (.50, 1.08) .85 (.59, 1.23)
College
Graduate
Number of .97 (.94, 1.01) 1.00 (.97, 1.02) .99 (.96, 1.03) 1.02 (1.004, 1.04) 1.03 (1.01, 1.05) 1.05 (1.02, 1.07) 1.02 (.98, 1.05) 1.02 (.99, 1.04) 1.01 (.98, 1.04)
Child
Psychiatrists
Number of 1.005 (1.003, 1.009) 1.001 (.86, 1.10) 1.01 (1.00, 1.01) 1.004 (1.001, 1.009) 1.003 (1.00, 1.01) 1.003 (1.00, 1.01) 1.001 (.998, 1.004) 1.002 (1.00, 1.01) 1.004 (1.002, 1.008)
Pediatricians
Autism Orgs .85 (.64, 1.12) .78 (.64, .96) .82 (.64, 1.05) .73 (.57, .94) .74 (.49, 1.18) .91 (.78, 1.09) 1.00 (.87, 1.15) .96 (.86, 1.08) 1.04 (.92, 1.17)
Cross Level
Medi-Cal x .89 (.73, 1.09) 1.34 (1.12, 1.62) 1.51 (1.21, 1.90) 1.07 (.90, 1.28) 1.30 (1.13, 1.51) 1.21 (1.04, 1.41) .82 (.70, .97) 1.15 (.99, 1.04) 1.49 (1.32, 1.68)
Property
Education x .83 (.74, .93) .91 (.82, 1.02) .85 (.75, .97) .92 (.83, 1.03) .99 (.90, 1.09) .87 (.80, .93) .87 (.81, .96) .89 (.83, .96) .90 (.85, .96)
Percent
College
Random Effects Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD Variance SD
Intercept Full .10 .32 .10 .32 .13 .36 .09 .30 .14 .37 .18 .42 .16 .41 .12 .35 .18 .42
Model
Medi-Cal .02 .16 .06 .24 .03 .18 .04 .19 .06 .24 .04 .21 .05 .24 .08 .28 .08 .28
Slope
Education .003 .05 .001 .03 .001 .03 .001 .04 .001 .04 .001 .03 .002 .05 .002 .04 .001 .03
Slope
Note: Odds ratios for factors examined for a potential association with autism risk appear in the column labeled OR. An odds ratio over one indicates an increased risk for
337
autism. An odds ratio of less than one suggests that the variable is associated with a decreased risk for autism. The 95 percent confidence intervals appear in parentheses.
Factors that are statistically significant at the p \ .05 level appear in bold. The year heading for each column indicates the birth cohort that the results pertain to. The
estimated variance of b0k , t00 is statistically significant in the unconditional model for all years at p .001 except 1995.You can also read