The Brain on Fire: A Case Study on Anti-NMDA Receptor Encephalitis - Exeley
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Australasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
The Brain on Fire: A Case Study on Anti-NMDA Receptor
Encephalitis
Grissel B Crasto 1.
1
Toronto Western Hospital, Ontario
Abstract
Anti-NMDA receptor encephalitis is a rare disease that occurs when antibodies produced by the
body’s own immune system attack the N-methyl-d-aspartate (NMDA) receptors in the brain
(Dalmau, 2016). For a relatively rare condition, one academic hospital in an urban centre noted four
cases of anti-NMDA receptor encephalitis in one single year. Patients develop a multistage condi-
tion that progresses from psychosis, memory deficits, seizures, respiratory difficulties, abnormal
catatonic movements and language disintegration into a state of unresponsiveness (Dalmau, Lan-
caster, Hernandez, Rosenfeld and Gordon, 2011).
This case study will focus on the pathologies and medical journeys of three female patients diag-
nosed with anti-N-NMDA receptor encephalitis at this hospital. This paper will discuss the presen-
tations of each of the cases and the individualized nursing care plans developed to address the
needs of this patient population. More specifically, it will highlight the importance of ensuring patient
and staff safety in the development of these care plans. The need for implementing ongoing evalua-
tions of these nursing care plans to address the developing needs of patients as they proceed
through the diverse and complex phases of the condition will also be discussed.
Key Words
Anti-NMDA receptor encephalitis, autoimmune encephalitis, encephalitis, N-methyl-d-aspartate re-
ceptors
Introduction plasticity affecting learning and memory (Day,
High, Cot, & Tang-Wai, 2011).
Literature Review
Due to the pathology, patients may develop
In 2005, Dr. Josep Dalmau described a con- psychiatric symptoms, seizures, memory defi-
dition in four young women with ovarian tera- cits and abnormal movements (Ding, et al.,
tomas and precipitating antibodies generated 2015). Focal neurological signs of the condi-
against antigens highly expressed in the hip- tion include decreased level of conscious-
pocampus called N-methyl-d-aspartate ness, weakness in limbs, seizures, altered
(NMDA) receptors (Dalmau et al., 2011). behavioural patterns, memory loss and confu-
NMDA receptors are concentrated in the hip- sion (Dalmau et al., 2007). Patients present
pocampus and play a vital role in synaptic with psychiatric symptoms such as changes
adaptation processes that affect learning, in personality, irritability or behavioural
memory, personality, movement and auto- changes such as violence, agitation and par-
nomic regulation (Newcomer, Farber & anoid thoughts. These symptoms are often
Olney, 2000). Antibodies are formed in re- misdiagnosed as their clinical presentation is
sponse to antigens presented by a teratoma consistent with psychosis and schizophrenia
often found in the reproductive organs such (Dalmau et al., 2007). The disruption of
as the ovaries or gonads and in some cases NMDA receptor activity also leads to disturb-
the antibodies formed are in response to neo- ances in respiratory drive that cause
plastic related antigens (Dalmau, 2016). hypoventilation (requiring ventilatory support)
These antibodies cross the blood brain barri- and impedes the body’s autonomic functions
er (BBB) and bind with NMDA receptors dis-
rupting their synaptic functionalities and caus- Questions or comments about this article should be
directed to Grissel Crasto
ing neurobehavioural pathology (Ding, Jian, Email address: crastogrissel@gmail.com
Stary, Yi and Xiaoaxing, 2015). The down
regulation of NMDA receptor activity in the DOI: 10.21307/ajon-2017-014
hippocampus results in changes in synaptic Copyright © 2019ANNA
Australasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
that cause bradyarrhythmias (Dalmau et al., adults of all ages (Dalmau et al., 2011). Ap-
2016). Moreover, patients are then admitted proximately 60 percent of diagnosed cases
to psychiatric facilities instead of acute care are associated with tumours, but there are
facilities, which prolongs timely diagnosis and many documented cases with no detectable
intervention (Dalmau et al., 2007). Alterna- tumour. It tends to occur in both males and
tively, when patients are admitted to acute females, however 80 percent of the diag-
care facilities, the condition is often also mis- nosed cases as yet have been women
taken for viral infections (Day et al., 2011). (Dalmau, 2016). The condition has recently
gained more attention in popular media. Su-
Studies have linked early intervention and sanah Cahalan, a journalist who worked for
treatment with complete recovery. However, the New York Post shared a powerful narra-
delay in treatment could result in death tive of her personal experiences with the con-
caused by neuronal degeneration, respiratory dition in the book, ‘The Brain on Fire’. For a
and/or cardiac failure (Dalmau, 2016). The relatively rare condition, one academic hospi-
risk of relapse has been noted in 20 to 25 tal in an urban centre treated four cases in a
percent of patients without teratomas, but this single year.
risk increases in patients if the teratomas
have not been resected and treated appropri- Clinical Presentation
ately (Ding et al., 2015). This further makes
the case for anti-NMDAR encephalitis to be A notable clinical manifestation of anti-NMDA
considered as a differential diagnosis when receptor encephalitis involves a triad of spe-
patients present with autonomic dysregula- cific features that present as epilepsy, dyski-
tion, seizures and psychiatric features (Day nesia and psychiatric symptoms (Omura et
et al., 2011). al., 2015). A list of general clinical features
such as focal neurological signs, psychiatric
Objective signs and autonomic instability noted in vari-
ous documented cases to date are listed in
The purpose of this case study is to raise the Table 1.
awareness about this condition. It aims to
encourage nurses, and other clinicians to Diagnostics
consider it as a differential diagnosis in pa-
tients presenting with signs of fever, psychiat- An analysis of serum and cerebrospinal fluid
ric symptoms, seizures, memory deficits, ab- (CSF) via lumbar puncture (LP) is conducted
normal movements and autonomic dysfunc- to detect the presence of specific NMDA anti-
tion. bodies (Dalmau, 2016). In addition, brain im-
aging via computer tomography (CT) is used
Epidemiology to detect changes in the brain and magnetic
resonance imaging (MRI) is used to detect
The first anti-NMDAR encephalitis case was any underlying teratomas, particularly in the
reported in 2005, but it was only character- ovaries, gonads and mediastinal regions
ized as a condition by Dr. Josef Dalmau in (Dalmau, 2016). Sometimes the tumours are
2007 (Ding et al., 2015). The exact incidence undetectable and in these cases, a positron
of the condition is still not known (Kelly & emission tomography (PET) scan may also
Sexton, 2016). Anti-NMDAR encephalitis has be done (Kelly & Sexton, 2016). Further-
been known as the most common cause of more, an electroencephalogram (EEG) may
autoimmune encephalitis after acute demye- reveal abnormal and/or focal slowing with
linating encephalomyelitis (Dalmau, 2016). epileptiform discharges (Kelly & Sexton,
This condition has been noted in children and 2016).
Table 1. Clinical features noted in patients with Anti-NMDAR receptor encephalitis
Focal neurological signs Weakness in limbs, seizures, altered behaviour, memory loss,
confusion
Psychiatric signs Auditory, visual and olfactory hallucinations; irritability, agitation,
aggression and violent behaviour; catatonia
Autonomic instability Fever, tachycardia/bradycardia, hypotension/hypertension,
hypoventilationAustralasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
Treatments lone, dexamethasone and prednisolone to
reduce inflammation in the brain. Concurrent
In patients with primary tumours, the first treatment with H2 receptor antagonists such
course of treatment involves tumour resec- as ranitidine or pantoprazole are given to pre-
tion (Halbert, 2016). As these tumours have vent steroid induced mucosal damage
predominantly been noted in the ovaries of (Omura et al., 2015). In addition, immuno-
female patients, a laparascopic oophorecto- therapies like intravenous immunoglobulin
my can be performed (Dalmau et al., 2007). (IVIg) are administered to decrease inflam-
Patients are treated with first-line immuno- mation of the meninges and inhibit the bind-
therapy treatment. This includes corticoster- ing of anti-NMDA antibodies. Also, plasma
oid therapy agents such as methylpredniso- exchange may be used for treatment by
Table 2. Clinical presentations, treatments and outcome of cases seen at our hospital
Case Symptoms Treatment Adjunct therapies Complications Outcomes
F, 25, Aphasia, posturing Bilateral ECT, Intubation, Complex care
A (rigid), myoclonus Oopherectomy Methylprednisolone, ventilator rehab,
jerks, tonic-clonic IVIG, Rituximab, associated discharged
seizures, Tetrabenzene, pneumonia, home
opsoclonus, Quetiapine, bacteremia, status
decreased level of Haloperidol, epilepticus, febrile
consciousness, Olanzapine, neutropenia
respiratory Ketamine and
difficulties, loss of Cyclophosphamide
tone, agitation,
aggression
F, 22, Confusion, Bilateral AEDs, Acyclovir, Manic symptoms, Repatriation,
B hallucinations, global Oopherectomy IVIG, psychosis cognitive
aphasia, agnosia, plasmapheresis, (Psychiatry rehab,
prosopagnosia, methylprednisolone consulted for discharged
memory deficits, unresolved mania) home
posturing, myoclonus
and seizures
Behavioural issues
like cursing, spitting,
yelling, agitation and
aggression
F, 30, Brocca’s aphasia Right Methylprednisolone, UTI, allergic Cognitive
C progressed to global Oopherectomy IVIG reaction to rehab,
aphasia, parasthesia RRR methylprednisolon discharged
in arms, generalized e (Psychiatry home
seizures, consulted for
hallucinations, unresolved
sensitivity to light and catatonia)
noise, agnosia,
prosopagnosia,
falling spells and
wanderingAustralasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
removing anti-NMDA antibodies from the hospital and discharged home. She was
blood (Dalmau et al., 2007). Second-line im- found unresponsive at home and re-admitted
munotherapies such as rituximab or cyclo- the following day. She also presented with
phosphamide, or both are used for patient posturing, rigidity and severe myclonus. Belle
showing little or no response to first-line im- was treated with anti-epileptic drugs and Acy-
munotherapies (Dalmau, 2016). clovir for suspected viral encephalitis. Her
MRI was normal, but her cerebrospinal fluid
Case Studies (CSF) tested positive for Anti-NMDA receptor
Our first patient in 2016, whom we will antibodies at the community hospital. Upon
refer to as Anna, was a 25-year-old, universi- confirmation of the diagnosis, she was trans-
ty student who presented to a community ferred to the ICU at our centre.
hospital with agitation, aggression, myoclo- Belle’s symptoms were similar to
nus jerks, generalized tonic clonic seizures, Anna’s symptoms. They both had hallucina-
opsoclonus and tremors. Due to her psychiat- tions, agnosia and prosopaganosia as men-
ric symptoms, she was initially misdiagnosed tioned in Table 2. Furthermore, Belle present-
and treated with antipsychotic medications. ed with severe psychosis. She was cursing,
She also received six sessions of electrocon- spitting, yelling, was often whispering, agitat-
vulsive therapy. However, after noting a fe- ed and aggressive. Belle was treated with
ver, rigidity and decreased level of con- IVIG, plasmapheresis and steroid therapy,
sciousness, a lumbar puncture was per- but continued to have seizures. She was
formed. Anna tested positive for anti-NMDA treated with multiple anti-epileptic medica-
receptor encephalitis. Although her MRI tions. Her MRI showed no evidence of a tera-
showed no signs of a teratoma, she was still toma. Despite this, the physicians chose a
treated with methylprednisolone and IVIg. bilateral oophorectomy as she was deterio-
After no improvements were noted, she was rating quickly. Her symptoms improved dras-
transferred to our Intensive Care Unit (ICU). tically after surgery. The pathology of her
She spent the next nine months in the ICU ovaries later revealed a microscopic terato-
where she received plasma exchange and ma. She was started on hormone therapy for
rituximab. She was further treated with tetra- surgically induced menopause and trans-
benzine, quetiapine, haloperidol, olanzapine ferred to our inpatient unit. Despite improve-
and ketamine to suppress the myoclonus ments in her symptoms, her manic symptoms
jerks, yet no improvement was noted. Upon a had not yet improved. A plan was needed to
repeat MRI, a tiny right cystic teratoma was address Belle’s manic symptoms, behaviour-
noted on her ovary. Due to the severity of her al issues, her safety and the safety of staff
symptoms and to prevent relapse, Anna re- caring for her during the agitated periods.
ceived a bilateral oophorectomy and was
subsequently treated for surgical meno- Our last patient (whom we will call Cathe-
pause. rine), was a 30- year old female whose symp-
toms began with facial twitching and pares-
Anna went on to develop several com- thesia in her right arm. She reported having
plications in the ICU including bacteremia, some word finding difficulty for a week. Later
ventilator associated pneumonia, status epi- in the week, she had a tonic-clonic seizure
lepticus and febrile neutropenia. Due to her and fell down at a baseball game. Post-
slow recovery and following further consulta- seizure, Catherine was brought to our emer-
tion with Dr. Josef Dalmau, she was started gency department for her progressive apha-
on a monthly treatment of cyclophosphamide. sia and a new onset of focal seizures. Her
After nine months, she was finally transferred brain MRI and CT were unremarkable. An
to the inpatient unit where she presented with EEG showed diffused slowing, but no abnor-
the symptoms outlined in Table 2. Her opso- malities. However, Catherine continued to
clonus myoclonus and seizures were uncon- present with global aphasia, visual hallucina-
trollable and putting her at high risk for falls. tion, agnosia, falling spells and a sensitivity to
We will refer to the next patient as Belle. She light and noise (Table 2). Unlike Anna and
was a 22-year old female, who initially devel- Belle, she did not exhibit agitation nor ag-
oped changes in her personality and started gression.
neglecting her personal hygiene following a A pelvic MRI revealed a 5cm ovarian terato-
vacation in Cuba. Belle was initially misdiag- ma and an LP further confirmed the presence
nosed with a psychiatric illness, started on of anti-NMDAR antibodies in her CSF. She
anti-psychotic medications in a community was started on IVIG treatments and herAustralasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
teratoma was resected within eight days of improvement. Brain injury can ensue as early
her admission. She was also started on IV as the five minutes into sustained seizure
steroid therapy, but developed a reaction to activity (Ramazan, et al., 2017). As a result, it
it. As a result, the steroids were discontinued. is imperative to prepare for the administration
of medications like IV lorazepam, phenytoin,
Nursing Implications midazolam and diazepam to manage status
Acute Confusion Management epilepticus effectively (Matata et al, 2015).
Each of these patients presented with unique Non-convulsive status epilepticus (NCSE) in
and unpredictable symptoms making their patients with an altered mental status have
medical management incredibly complex. also been noted in this population (Day et al.,
Matata et al. (2015) suggests it is important 2011). Hassan (2016) describes NCSE as a
for nurses to ensure a thorough Mini-mental prolonged seizure without perceptible motor
status exam and Glasgow Coma Scale signs but with an altered mental status and
(GCS) assessment is performed to establish continuous epileptiform EEG changes. NCSE
a patient’s baseline on admission. Thereafter, should be monitored closely for changes and
a Confusion Assessment Method (CAM) and communicate updates to the team as they
GCS must be performed regularly every shift may need continuous EEG monitoring and
in coordination with the physician’s order. might need to be treated with anti-epileptic
These tests enable nurses to detect minute medications.
changes in the patient’s physiological and Memory Loss
psychological status, and enhance communi-
cation to the team for psychiatric manage- Long term cognitive effects such as memory
ment. Matata et al. (2015) suggest that pa- loss, disinhibition and impulsiveness, impair-
tients with this condition often develop para- ments in executive function such as inatten-
noia. Thus, patients may benefit from nurses tion, poor organization and planning difficul-
clustering their interventions to minimize ties have been noted in this population
stress and decrease stimulation (Matata et (Bach, 2014). As a result, patients may re-
al., 2015). In addition, Matata et al. (2015) quire total assistance with activities of daily
also suggest that the concerns of family or living (ADL). Occupational therapy and Physi-
relatives at the bedside be taken seriously as otherapy may be required to help manage
they could be an indicator of the patient de- and to develop a plan care around the pa-
veloping subtle psychiatric features. Nurses tient’s general physical deconditioning
can play a crucial role in advocating for refer- (Tham, 2012).
rals to psychology, neuropsychology and
mental health services within the interdiscipli- All three of the previously discussed cases
nary team. developed agnosia (inability to process sen-
sation and recognize objects), prosopagnosia
Seizure Management (inability to recognize faces), receptive apha-
sia (inability to comprehend language) and
According to Dalmau et al., (2007), seizures expressive aphasia (inability to speak) in
are a characteristic symptom of the condition. some capacity (Dalmau et al., 2007). In addi-
Focal seizures, generalized seizures, status tion, the patients also exhibited dysphagia
epilepticus and non-convulsive status epilep- and communication deficits, requiring a
ticus have all been noted in patients with Anti Speech Language Pathologist (SLP) consult.
-NMDAR encephalitis (Dalmau, 2016). Nurs-
es should monitor the patients closely for Patient Safety, Staff Safety and Transition-
changes in behaviour and confusion as they al Care
could be signs of seizures. It is also important
to prepare the bedside with safety equipment All our patients’ families were quite involved
such as airway management equipment and in their care and tried to stay at the bedside
intravenous (IV) access to allow for quick and as much as possible. However, when the
effective seizure management in order to pre- families were unable to do so, a plan was
vent brain injury. developed for every single patient to ensure
that their unique medical and psychosocial
Guven, Aydin & Kaykis (2017) define status needs were being met, especially in regards
epilepticus as a critical condition in which a to patient safety. The nurse to patient ratios
seizure lasts for more than five minutes or on the inpatient unit is one to five versus one
when two or more seizures occur without any on one in the ICU. Their transitional needsAustralasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
became more apparent during their transition routine, providing non-slip slippers, placing
from ICU to the inpatient unit. Families may the bed to the wall and de-cluttering the bed-
have difficulty adjusting to the fact that the side space were quite useful in preventing
care provided on the inpatient unit is no long- falls in these patients.
er on a one-on-one basis.
Some patients with this condition may be-
Families will require additional emotional sup- come quite violent and aggressive during the
port. Organizing family meetings can be help- psychosis stage. It is recommended that a
ful in communicating ongoing updates and behavioural safety alert and plan be imple-
establishing the goals of care. Nurses play a mented to ensure the safety of the patient,
crucial role in initiating the discharge planning family members and all staff in the interdisci-
process from the point of admission and ad- plinary team. All possible options must be
vocating for patients to receive all the appro- explored before the use of physical restraints
priate referrals and services prior to dis- such as soft mitts, restraint jackets and wrist
charge. Nursing representation at family restraints. It is recommended that chemical
meetings is also critical to help ensure fami- and physical restraints be used with caution
lies understand the plan and goals of care. to prevent patients from harming themselves,
their families and staff. In addition to medical
Due to the possibility of tonic-clonic seizures, and safety concerns, another downside to the
posturing and myoclonus jerks, patients with use of restraints is the distress it may cause
anti-NMDAR are at high risk of falls. Strate- to both patients and their family members.
gies such as bed alarms, placing falls mats Nurses should provide ongoing emotional
on the floor, ensuring the patient’s belongings support to distressed family members as a
were within reach, establishing a toileting
Save the Date!
2019 ANNA National Conference
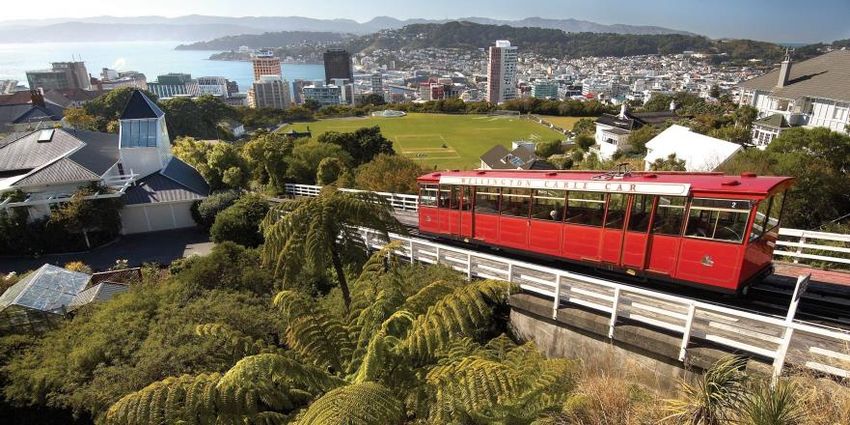
17-18 October 2019
Wellington New Zealand
The 2019 ANNA National Conference will be an action-packed two days of
professional development and networking at the Intercontinental Hotel in
Wellington, New Zealand!
Block out Thursday 17 and Friday 18 October, 2019 in your calendar now
and stay tuned for more information about what is shaping up to be a fantas-
tic National Conference
We look forward to seeing you thereAustralasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
part of the discussion about the goals of care Discussion
for such patients. Other alternatives may be
explored and agreed upon in discussion with Prior to 2005, undiagnosed and untreated
family members at family meetings. For ex- patients with this condition often developed
ample, constant observers or “sitters” were complications such as infections, cognitive
organized for patients whose family members and motor dysfunction, life long impairments
were distressed by the use of restraints for and even death (Dalmau et al., 2007). In a
our patients. multi-institutional observation study Titulaer
et al. (2013) reported that out of 577 patients,
Although medicine is more informed about 495 became bedridden and 440 were admit-
the condition today than ever before, patients ted to the ICU at some point, 394 went on to
and families may struggle to cope with the reach good outcomes and 30 patients ended
rarity of the condition, the lack of information up dying. The patients in this case study pre-
about the condition and the devastating ef- sented with both neurological and psychiatric
fects of a oophorectomy or hysterectomy, features similar to those noted in literature.
early menopause and possible life altering However, thanks to the advances made by
changes. The families of all three patients Dr. Josef Dalmau, in comparison to cases
were provided ongoing emotional support prior to 2005, the patients in this case study
and offered spiritual care services or referred faired relatively well with two going back to
to hospital chaplains. They were also referred work and one returning home to live with her
to support groups such as the Anti-NMDA family. The value of early diagnosis and treat-
Receptor Encephalitis Foundation and social ment is colossal to the successful recovery of
services when appropriate. patients suffering from anti-NMDAR enceph-
alitis.
Patient Outcomes
In summary, the triad noted often in this pa-
Anna was transferred to a Complex Care Re- tient population is seizures, psychosis and
habilitation facility and moved back home dyskinesia (Dalmau, 2016). Based on their
with her family. Although, Anna did not return observational study, Titulaer et al. (2013)
completely back to her baseline, she is suggest that early diagnosis and timely inter-
healthy again and doing very well. Her family vention is predictive of improved outcomes in
says that her cognition has improved, and this patient population. Nurses, physicians
that she is talking and walking again. Her and allied health professionals especially in
family also mentioned she is attending day community health, emergency and neurology
programs three times a week and spending a departments, family medicine and psychiatric
lot of time engaged in activities with family facilities play an integral role in recognizing
and friends. symptoms earlier on and facilitating or deliv-
A Psychiatry consult was arranged for Belle ering timely medical intervention to these pa-
and she was started on anti-psychotic medi- tients. Nurses in particular play a crucial role
cations to manage her agitation and violent in supporting patients and their families
behaviour. Upon successful medical and psy- through this rare and distressing neurological
chological management, Belle was repatriat- condition. Nursing implications include regu-
ed to a community hospital in her hometown larly communicating ongoing neurological
for further monitoring. She received cognitive developments to the team, acute confusion
rehab for two months and she is still receiv- management, seizure management, respira-
ing treatment on an outpatient basis. She is tory and cardiac monitoring, making appropri-
currently working through a program offered ate referrals, patient advocacy, providing
by the March of Dimes of Canada. The com- emotional support, coordinating additional
munity based rehabilitation program helps support services, educating patients and fam-
people with disabilities transition back into ilies, ensuring patient and staff safety and
the work force. As per family, she has almost discharge planning.
returned back to her baseline and hopes to Acknowledgements
attend college next year.
The patients and their families,
Following her improvement, Catherine was Arlene Vasconcelos, Adassa Wilson,
discharged to a cognitive rehabilitation centre Aline Ha, Charmaine Arulvarathan, Nadia
close to her family home. She has almost Walfall, George Crasto and Valerian Gladys
completely recovered, has returned to work Crasto
at her previous position. She continues to be
followed by Neuropsychiatry at our hospital.Australasian Journal of Neuroscience Volume 29 ● Number 1 ● May 2019
References Guven, R., Aydin, M. N. and Kaykisiz, E. K.,
(2017). An emergency medicine perspective
Bach, L. J., (2014). Long Term Rehabilitation for non-convulsive status epilepticus. Eura-
Management and outcome of anti-NMDA sian Journal of Emergency Medicine. 16: 83-
receptor encephalitis: Case Reports. Neu- 89.
rorehabilitation 35: 863-875.
Halbert, R. K., (2016). Anti-N-methyl-D-
Dalmau, J., (2016). NMDA receptor enceph- aspartate receptor encpehalitis. Journal of
alitis and other antibody-mediated disorders Neuroscience Nursing, 48(5): 270-273.
of the synapse-The 2016 Cotzias Lecture. Hasan, A., Q., (2016). Non Convulsive Status
American Academy of Neurology, 87:2471- Epilepticus in Emergency Department: A di-
2482. agnostic Challenge. Journal of Medical Sci-
Dalmau, J., Lancaster, E., Matinez- ence and Clinical Research, 4(8): 12305-
Hernandez, E., Rosenfeld, M., Balice- 12308.
Gordon, R., (2011). Clinical Experience and Kelly, L. J., & Sexton, V. L., (2016). Anti
Laboratory Investigations in patients with Anti NMDA encephalitis. The Neurodiagnostic
- NMDA receptor encephalitis. The Lancet – Journal, 56:101-108.
Neurology 10 (1): 63-74.
Matata, C et al., (2015). Managing patients
Dalmau, J., Tuzun, E., Wu, H., Masjuan, J., with encephalitis. Nursing Standard,30(11):
Rossi, J. E., Voloschin, A., Lynch, D. R., 50-58.
(2007). Paraneoplastic Anti-N-methyl-D-
aspartate receptor encephalitis associated Newcomer, J. W., Farber, N. B. & Olney, J.
with ovarian teratoma. Annals of Neurology, W., (2000). NMDA receptor function,
61:25-36. memory, and brain aging. Dialogues in Clini-
cal Neurosciences, 2(3): 219–232.
Day, G. S., High, S. M., Cot, B. & Tang-Wai,
D., (2011). Anti-NMDA receptor Encephalitis: Omura, T., Sonoda, S., Nagata, K., Okita, T.,
Case report and literature review of an under- Hoshiai, A., Sano, H., Shoichi, O., (2015).
recognized condition. Journal of General In- Acute Medicine & Surgery, 2: 56-59.
ternal Medicine, 26 (7): 811-816.
Titulaer, M. J., McCracken, L., Gabilondo, I.,
Day, G. S., Laiq, S., Tang-Wai, D. F. & Mun- Armangue, T., Glaser, C., Lizuka, T., …
hoz, D., (2014). Abnormal neurons in terato- Dalmau, J., (2013). Treatment and prgnostic
mas in NMDAR encephalitis. JAMA Neurolo- factors for long-term outcome in patients with
gy, 71 (6):717-724. anti-N-Methyl-D-Aspartate (NMDA) receptor
encephalitis: a cohort study. The Lancet –
Ding, H., Jian, Z, Stary, C. M., Yi, W and Neurology 12 (2): 157-165.
Xiaoaxing, X., (2015). Molecualr Pathogene-
sis of Anti-NMDAR encephalitis. BioMed Re- Tham SL, Kong KH (2012) A case of anti-
search International, 1: 1-6. NMDAR (N-methyl-D- aspartate receptor)
encephalitis: a rehabilitation perspective.
NeuroRehabilitation. 30 (2) 109-112.You can also read