Relations between Immunity and Malignancy - PNAS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Proc. Nat. Acad. Sci. USA
Vol. 69, No. 4, pp. 1026-1032, April 1972
Relations between Immunity and Malignancy
ROBERT A. GOOD
Departments of Pathology, Pediatrics, and Microbiology, University of Minnesota,
Minneapolis, Minn. 55455
ABSTRACT A higher incidence of malignancy as well Leukemia in Bruton-type agammaglobulinemia
as greater susceptibility to infection has been found to be
associated with primary immunodeficiencies. An in- Particularly important to us at the time were studies of
creased incidence of leukemia has been associated with patients who had selective deficiency of immunoglobulin
X-linked infantile agammaglobulinemia-an isolateddefect synthesis and secretion, failure of antibody production,
of humoral immunities. An increased frequency of a wide
variety of malignancies have been found to accompany absence of plasma cells from bone marrow and lymphoid
several different forms of primary immunodeficiency. tissues, and deficiency of germinal centers and cell populations
Secondary immunodeficiencies produced by immuno- in the far cortical areas of lymph nodes (6-9) (Fig. 1). Recent
suppressant therapy to facilitate renal transplantation work by Cooper and associates (10) and Grey et al. (11) show
have also been found to have far too much cancer to be that such patients lack B cells as well as plasma cells. We had
explained by chance association. Many experimental
associations between immunity and malignancy have found that these patients often cannot form antibody even
also been encountered, indicating that these two adaptive in response to repeated and most intense antigenic stimula-
processes have an essential relationship that must be tion.
elucidated. Their cellular immunologic vigor was quite good and
An area in rapid development, and hence one of considerable probably intact (12, 13). Such patients have been found to
controversy is that which was opened by a postulate ex- develop delayed allergic responses normally, to show and
pressed by Lewis Thomas in 1958 (1). It was Thomas' concept develop contact allergy with vigor, and to have lymphocytes
that transplantation immunity as defined in the extraor- that respond to kidney-bean extract (phytohemagglutinin)
dinary analysis of Medawar (2) must play a major role in in vitro and to allogeneic (of different genetic constitution)
the body economy. Thomas could not visualize this new form lymphocytes in mixed leukocyte culture quite normally (14).
of immunity as having its high specificity and destructive We have studied the capacity for allograft rejection in
potential, either as a mechanism placed in the body to con- several of these patients with Bruton-type agammaglobulin-
found aspiring transplantation surgeons or as a basis for emia. Usually they will recognize and reject a skin allograft
diagnosis of persisting bacterial infections, e.g., tuberculosis. quite normally. They often show a significant delay, however,
Rather, he reasoned that the mechanism must have a raison in the rejection of an initial skin graft, but can show a vigorous
d'etre directed toward destruction of cells or tissues, which second set skin-graft rejection (14). Thus, even though such
when arising de novo in the body would be recognized as patients cannot form circulating antibodies, they do not lack
foreign and would be eliminated by a major line of defense. immunity and one can transfer cellular immunity to non-
Thus, Thomas originally stated a hypothesis that has sub- sensitized normal persons by injecting, intradermally, blood
sequently been popularized as the concepts of immuno- lymphocytes of patients with Bruton-type agammaglobulin-
surveillance especially in the writings of Burnet (3). This view emia (15). Through the years, some 50 or so patients with
has been vigorously discussed, and right or wrong, the Bruton-type agammaglobulinemia have been discovered,
postulate has served its purpose. It has generated a great studied, and reported. Of these five have apparently developed
amount of new information concerning the relationship malignancy, and in each instance the malignancy has been
between immunity and malignancy (4). leukemia (Table 1). None, thus far, have developed carcinoma
or solid tissue sarcoma, or even lymphosarcoma. This inci-
My own relationship to this postulate derived from the
fact that I, a former student and colleague of Thomas, was dence of leukemia-about 10%, stands far in excess of that
heavily engaged at the time in studying the nature of the observed in members of the general population of the same
immunologic deficit in patients suffering from primary and age (16,17).
secondary forms of immunodeficiency diseases (5). A corollary Immunodeficiency in patients with Hodgkin's disease
of the postulate was that immunodeficient patients, less
capable than normal of rejecting skin allografts, should not At the same time, we were concerned with the immuno-
only reveal their immunodeficiency in increased susceptibility deficiency in patients with Hodgkin's disease. Schier (18)
to infection, but should have too much cancer when compared had pointed out that such patients often are anergic. We
to immunologically competent persons. At the time Thomas looked at this question and confirmed Schier's findings (19).
expressed this prediction, we were already working intensively We then showed that anergy often progresses with pro-
with several forms of immunodeficiency disease and investi- gression of the disease (20), extends to a frequent deficiency
gating the relations between structure and function in the in vigor of skin allograft rejections (21), and cannot readily
lymphoid apparatus in the perspective of such patients as be corrected by giving leukocytes from normal sensitive
Experiments of Nature. donors (5, 15, 19, 21-23). In some of these experiments, what
Downloaded by guest on October 18, 2021
1026Proc. Nat. Acad. Sci. USA 69 (1972) Relations between Immunity and Malignancy 1027
we considered massive leukocyte infusions from sensitized
donors were tried, and they regularly failed to sensitize the
nonsensitized patient with Hodgkin's disease. By contrast,
patients with Hodgkin's disease produced antibodies well in
response to many antigenic stimulations. They regularly
possessed in their circulation at least normal amounts of all
immunoglobulins, had plenty of plasma cells in their hemato-
poietic tissues, and produced germinal centers in the lymph
nodes, usually after antigenic stimulation. As a counterpoint
experiment of nature to the patients with Bruton-type
agammaglobulinemia (a B-cell immunodeficiency), patients
with Hodgkin's disease exhibited a deficiency of T-cell but
not of B-cell-dependent immune functions. In these same
terms, it was clear that B-cell immune functions are regularly
deficient in multiple myeloma, while T-cell functions are
quite intact (24). In chronic lymphatic leukemia, a disease
apparently based on monoclonal proliferation of B-cells (25),
both T- and B-cell immunities are deficient early in the course
of the disease (26, 27).
Even in these early analyses that were surely crude by
present standards, it was clear that in advanced and ad-
vancing malignancy, deficiency of cellular immunity is a
frequent concomitant. Thus, Southam et al. (28) and Kelly
et al. (20) studied in cancer patients, cellular immunity to
cancer cells, skin allografts, and antigens against which
cellular immunity is widespread in the general population.
They, thus, defined a high frequency of anergy of cellular
immune functions not only in patients with Hodgkin's
disease but in those with advanced malignancies as well.
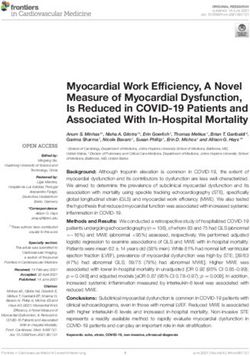
FIG. 1. Lack of germinal centers in the cortical area of a lymph
Ataxia-telangiectasia node from a patient with X-linked infantile agammaglobuli-
Before we studied the immune responses, immunoglobulin nemia.
concentrations and lymphoid tissues of patients with ataxia-
telangiectasia, this disease was considered primarily to be a small, does not show cortical and medullary differentiation,
neurological disorder (29-31). This disease, however, is contains very few lymphocytes, and does not contain Hassall's
featured by an association of progressive cerebellar ataxia, corpuscles (34). The thymus, indeed, has the appearance of
telangiectases of the sclera and skin, especially the skin of an embryonic thymus that is just developing a lymphoid
the eyelids, anticubital, and'popliteal regions. These patients structure. This form of immunodeficiency is important in the
also showed an increased frequency of sinopulmonary in- context of our present analysis because one of the frequent
fection (31, 32). The disease has been considered to be an causes of death in these unfortunate children is malignancy.
autosomally inherited disorder, but Lambrechts and Snoijink Malignancies are frequently reticulum-cell sarcoma, lympho-
(32) have recently presented arguments that it may be based sarcoma, and leukemia, but epithelial malignancies, especially
on an isoimmunization, and J. Finstad and R. A. Good of the gastrointestinal tract and malignancies of other sup-
(unpublished observations) have proposed that if this is porting tissue and mesenchymal tissues have been reported
indeed an isoimmunization, it might be due to isoimmuniza- as well (17, 33). Indeed, the incidence of malignancy in
tion against the human homologue of the isoantigen 0 in the patients of this group has been about 10% of all collected
mouse. The isoantigen is distributed in the central nervous cases. This high incidence is all the more striking, because it
system and in peripheral lymphoid cells of the T-cell class. is occurring at an age in childhood and early life when the
The immunological deficiency in patients with ataxia-telangi- frequency of malignancy is otherwise very low (17).
ectasia includes frequent (60-70% of patients) deficiency or
absence of IgA, frequent absence of IgE, and regular de- Malignancy in the Wiskott-Aldrich syndrome
ficiency of cellular immune vigor (31-35). Concordant with A completely different form of immunodeficiency of man is
the abnormality of cellular immunity in these patients is a represented by the Wiskott-Aldrich syndrome. In this disease
consistent abnormality of the thymus. The thymus is usually the triad of (i) increased tendency to bruise and bleed be-
cause of low platelet count and possibly abnormal platelets
TABLE 1. Leukemias in infantile, X-linked immunodeficiency (ii) increased susceptibility to infection and (iii) an atopic-
like eczema are associated (36, 37). The increased sus-
Acute lymphocytic leukemia ceptibility to infection (38) is associated with a dual system
Malignant lymphoma immunodeficiency of peculiar nature. Patients with Wiskott-
Chronic monomyelogenous leukemia Aldrich syndrome have frequent and progressive deficit of
Thymoma with leukemia cell-mediated immunity, deficiency in the concentration of
Lymphatic leukemia
circulating IgM, and frequently massively elevated con-
Downloaded by guest on October 18, 20211028 Good Proc. Nat. Acad. Sci. USA 69 (1972)
TABLE 2. Malignancies in patients dominant inheritance of a trait that may be expressed in one
with primary immunodeficiency individual as a primary immune deficiency and in other
family members as mesenchymal disease has been encountered
Approximate no. of % (46). Still other cases seem to occur sporadically that would,
Primary disease malignancies collected Cancer of course, be compatible with recessive inheritance. Recent
Bruton-type agam- Five cases, all leukemia 5-10 studies in our laboratory, as well as in several others, e.g.,
maglobulinemia that of Cooper et al. (10, 11, 14, 47, and unpublished observa-
Ataxia-telangiectasia 42 Cases, many forms of cancer 10-15 tions) indicate that these patients possess B cells, but do not
Wiskott-Aldrich 13 Cases, mostly but not exclu- >10 develop secretory B cells or plasma cells normally. Quantita-
syndrome sively lymphoreticular malig- tive studies in our laboratory indicate that very regularly such
nan cies
Common variable More than 30 cases, many forms
patients have fewer than normal responding T cells as well
5-10 (48). As with the patients with ataxia-telangiectasia and
immunodeficiency of cancer
Severe dual system Three cases 1-10 Wiskott-Aldrich syndrome, these patients too are developing
immunodeficiency cancer in an incidence that approaches 10% (17). The
malignancies encountered are often of the lymphoid system
or of the reticular apparatus, but may be epithelial, especially
involving stomach, colon, and intestinal epithelium as well.
centrations of IgA and IgE. These patients fail to respond with The incidence of malignancy encountered in the several
antibody production or with development of cellular im- immunodeficiencies is summarized in Table 2.
munity to polysaccharide antigens, e.g., pneumococcus Chediak-Higashi anomaly
polysaccharide, Vi antigen, blood group antigens, and the Still another human disease in which increased susceptibility
cellular antigens that give rise to heterolysins (39-41). By to infection and malignancy are associated is the so-called
contrast, they make both IgM and IgG antibodies to protein Chediak-Higashi anomaly (49). Patients with this disorder,
antigens very well. Patients with Wiskott-Aldrich syndrome from an early age, are susceptible to recurrent infections
are susceptible to virus, fungus, and bacterial infection, and
especially of the gastrointestinal and respiratory systems.
to both high-grade, encapsulated bacterial pathogens and the If they do not die of infection, they die of malignancy (50).
more frequent low-grade pathogens (38, 39). In this disease
The malignancy is often diagnosed as lymphosarcoma or
also, malignancy occurs far too frequently (17). The most Hodgkin's disease. Although the immunologic basis of their
common form of malignancy is a strange reticulum-cell
susceptibility to infection is not yet clear, they have a granular
malignancy that frequently occurs in the brain as well as in abnormality that involves lymphocytes, polymorphonuclears,
the lymphoid and hematopoietic organs (42). Occassionally, eosinophils, as well as cells of many organs and tissues. It
but certainly too frequently to be explained by chance, other seems certain that this abnormality of single membrane-
malignancies including epithelial malignancies have been bound particles in some way accounts both for the immuno-
encountered in these patients (17). The incidence of malig- deficiency and the increased frequency of malignant disease.
nancy in children with the Wiskott-Aldrich syndrome is
greater than 10%, and thus again represents a fantastic Severe dual-system (cellular and humoral)
excess over that encountered in the general population. immunodeficiency and DiGeorge syndrome
Malignancy in patients with the common
Already several cases of malignant disease have turned up in
variable immunodeficiency patients with severe dual-system immunodeficiency (17),
even though the children with this disorder generally live
Among the most frequent of the immunodeficiency syndromes only a short time. To the knowledge of the writer none have
have been observed in the patients with what has been been encountered in the few patients with the so-called
described in the past as acquired agammaglobulinemia, DiGeorge syndrome. Further studies of these relationships
late-occurring immunodeficiency, sporadic immunodeficiency, are, however, warranted particularly now that these patients
abrotropic immunodeficiency, familial immunodeficiency with are being partially and/or completely corrected by thymus
autoimmune disease, and dysgammaglobulinemia of various and/or marrow transplantation.
types. Whether this is a single disease or multiple entities
yet to be separated remains to be resolved (43, 44). As a Immunologic perturbations during oncogenesis
group, these patients regularly can be shown to have a high with chemical carcinogen
frequency of autoimmune disease, a high frequency of accom- As early as 1952, Malmgren et al. (51) noted that several
panying hematological abnormality, increased frequency of carcinogenic chemicals are also immunosuppressive, whereas
bacterial, virus, and even fungus infection. The immuno- closely related compounds are neither immunosuppressive nor
logical deficiency, likewise, is variable in severity, but regu- carcinogenic. Extensive subsequent studies have since been
larly can be shown to involve both the T and B cells. Although performed that attest to the intimacy of these two influences
valiant efforts have been made to classify and subclassify (52, 53). Surely, the immunosuppressive quality of the
these patients, the variability from time to time in the same chemical carcinogen need not be expressed in vivo in order
patient and between members of the same family has argued to yield a carcinogenic influence, since cells have been trans-
against fine sublcasses at this juncture (43). Particularly, we formed in vitro to putative malignant state where no influence
have found the concept of consistent forms of dysgamma- on the immune response need be considered (54). Further,
globulinemia (45) spurious at best, and we thus, no longer the dosage of chemical carcinogen needed to exercise a
use the term. In some instances an autosomal recessive demonstrable immunosuppressive effect may far exceed the
pattern in families of these patients is clear; in other instances concentration necessary to exercise a carcinogenic influence
Downloaded by guest on October 18, 2021Proc. Nat. Acad. Sci. USA 69 (1972) Relations between Immunity and Malignancy 1029
in vivo (55). Nonetheless, the parallelism of the two cellular regularly to permit cardiac, liver, pancreas, or even marrow
influences cannot represent a chance association. Prehn (56) transplants, and they often cannot control graft-versus-host
particularly has been concerned with these interrelationships reactions. It is to be expected that this approach will be
and has recorded that tumors that are produced by agents improved and even more powerful immunosuppressive
like methylcholanthrene that induce malignancy rapidly therapy will be developed that will extend the transplantation
in vivo are likely to be more powerful immunosuppressants era. One complication of these immunosuppressive regimens
than agents like plastic that induce malignancy more slowly. might be anticipated from the Thomas' postulate (1). Im-
Further, malignancies that develop rapidly under powerful munosuppression, powerful enough to depress organ and cell
chemical carcinogens are likely to have more readily demon- rejection from allogeneic donors, might foster development
strable antigenicity in animals syngeneic to those in which of malignancy. This prediction has apparently been borne out
the tumor developed than are the tumors that develop under because about a 10-fold increase in incidence of malignancy
weaker carcinogenic influence, where longer incubation has been observed in patients given an organ transplant
period is required. under immunosuppressive therapy (17, 62, 63). The malig-
Influence of experimental iinmunosuppression nancies and tumors that have developed have been approxi-
on development of malignancy mately equally divided among tumors of epithelial and
On the other side of the coin, we find evidence that immuno- lymphoreticular origins (63-65). The four tumors of which
we have seen in the Minnesota series have all been epithelial
suppressive regimens in experimental animals foster the in nature. One was an anaplastic carcinoma, one was an
development of malignancies de novo and also may foster the ovarian carcinoma, and two were carcinomas of the cervix
occurrence and establishment of metastases (17, 57). Some
uteri. The frequently indicated association between lympho-
evidence has been presented that immunosuppressive regi- reticular malignancy and antilymphocyte serum (66) is not
mens including thymectomy (58), and even antilymphocyte
serum foster the development of malignancies induced by sufficiently inclusive. Malignancies occur with greater fre-
quency than normal when immunosuppression is accomplished
chemical carcinogens. In this regard, it is important to
consider Allison's (59, 60) more recent analysis that indicates without antilymphocyte serum (64). Further, epithelial as
that with certain immunosuppressive regimens, only the well as lymphoreticular malignancies are observed in patients
malignancy induced by oncogenic virus(es) is influenced by whose immunosuppressive regimen includes antilymphocyte
serum (17, 64). All these relationships are to be predicted from
immunosuppressive agents that are not themselves chemical
carcinogens. the surveillance hypothesis.
Immunosuppression and Transplantation of Cancer in Man. Direct evidence for the relation between
Soon after clinical trials of kidney allotransplantation were immunity and malignancy
introduced some 10 years ago, it became apparent that in For a number of years, evidence has been accumulating that
man, as in experimental animals, allotransplants of malignant reflects in still another perspective the essentiality of an
cells could be achieved in immunosuppressed persons. At immunity-malignancy interface. Wherever they can be
least nine such transplants of malignancy occurred in- effectively studied in experimental animals, malignant tumors
advertently (17, 52, 61). In each instance, the transplanted and malignant cells can be shown to have at their surface
malignancy was epithelial in nature, and in four instances antigens that are foreign to the host (66-68). These antigens
the malignancies became widely disseminated throughout the are called tumor-specific transplantation antigens (TSTA)
body. To achieve complete regression of these widely dis- as a reflection of the methods used for their demonstration.
seminated malignancies, the only treatment required in They differ in chemical-carcinogen and virus-induced malig-
several instances was cessation of the immunosuppressive nancies in that the tumor-specific transplantation antigens
regimen (52, 61). Once this had been done, the widely dis- for virus-induced malignancies tend to reflect the virus induc-
seminated malignancy just like the allogeneic organ transplant, tion and are similar for all the tumors induced by the virus in
was rejected. Thus, under these artificial circumstances, the question. Thus, in experimental animals, whether a polyoma
potential power of the allograft mechanism for eliminating virus-induced malignancy is a mesenchymal or an epithelial
even widely disseminated malignancy was demonstrated. malignancy, sharing of this antigen is to be found. By con-
Immunosuppression and the Development of Malignancy trast, chemical carcinogen-induced malignancies tend to
De Novo in Man. The extension of clinical transplantation have tumor antigens that reflect the particular induction to
has witnessed progressive improvement of skill at immuno- malignancy. Thus, two different malignancies arising within
suppression. This development has been signalled by increasing the same animal by virtue of the influence of methylcholan-
success in organ transplantation. At the present writing threne will possess tumor-specific transplantation antigens
renal transplantation is, indeed, a therapeutic fiat accompli that are different. The same will be true if dibenzanthracene
and renal transplants from well matched sibling donors has been used as the chemical carcinogen. Similarly, human
should not be rejected and can serve as long term therapy malignant tumors are being found in which tumor-specific
for patients with end-stage renal disease. Relatives obviously antigens are present at the surface. In its ultimate con-
not matched at the HL-A histocompatibility determinants sideration, this consistent relationship between immunity
also can donate kidneys with the expectancy that the grafts and malignancy means that cells that should be looked on by
in a high percentage of instances (greater than 80% in some the host as being foreign are not being eliminated from the
series) will provide long term life-saving renal function. body by immunologic means. In experimental systems, as
Even cadaver donors in 60% of instances provide long term for example in mice infected with Maloney sarcoma virus
correction of renal failure for many recipients. Such immuno- (69) and in rabbits infected with Shope papilloma virus (70),
suppressive regimens, however, are not powerful enough one sees progressor and regressor states of the potential
Downloaded by guest on October 18, 20211030 Good Proc. Nat. Acad. Sci. USA 69 (1972)
malignancy. The analysis of the progressor and regressor coveries by Jose, Cooper, and me (reviewed) (85) have re-
adaptations in immunological terms by the Hellstroms (71) vealed that chronic protein or amino-acid deprivation can
and their associates have revealed that in the regressors, have as one consequence profound depression of capacity to
cell-mediated immunity in the form of a killer function of produce humoral immunity and blocking antibody against tu-
lymphocytes is directed toward the tumor cells. Serum of the mor cells in xenogeneic, allogeneic, and syngeneic animals,
animals does not interfere or oppose this action. By contrast, while leaving cellular immunity intact or even enhancing it.
in the progressor status, cellular immunity directed against More profound nutritional deprivation can yield deficiencies
the tumor cells can be demonstrated, but the tumor seems to of both cellular and humoral immunity. It seems possible from
be protected from destruction by blocking antibodies in cursory study of the literature as well as from our own
circulation that inhibit this action. Similarly, in rabbits experimental results that difficulty in developing malignancy
infected with Shope-papilloma virus, a regressor state is in the presence of nutritional deprivation may relate to the
associated with cellular immunity, while in the progressor differential influence of certain forms of nutritional depriva-
state a humoral immunity seems to exist that can interfere tion on the T- and B-cell immunities.
with the destructive action of the cellular immunity on the
tumor cells. Relation between aging, immunity, and malignancy
Much evidence has now accumulated to indicate that in Another interesting relation exists between immunity and
numerous experimental systems and in many different human malignancy that is revealed in aging (86). With aging,
malignancies, cellular immune reactions directed against immunologic vigor, especially the vigor of cellular immunity
malignancy exists concomitantly with blocking antibodies shows remarkable decline in many strains of mice. By con-
that are able to interfere with the killer action of the lympho- trast, capacity to form immunoglobulins and autoantibodies
cytes against the tumor cells (72). These exciting phenomena seems to be retained longer (87). Thus, a lack of immuno-
may well be extensions of the enhancement phenomenon logical balance occurs frequently in aged mice that could
discovered for certain experimental situations long ago (73). favor immunodeviation of the sort that in experimental
I have used the term immunodeviation to describe this animals fosters success of the malignant adaptation (88).
class of reactions. Similar cellular immunodeficiency can also occur with aging
A possible alternate means of circumventing cellular and in man. Much study to extend, quantitate, and evaluate these
humoral tumor immunity that might destroy malignant cells relationships seems warranted in light of the frequent oc-
includes immunological tolerance, but this has not yet been currence of certain forms of malignancy with age in mice and
clearly defined for tumor-host relationships any more than it men, and the greater propensity of aged animals to accept
has for other forms of cellular immunity directed against transplants of malignant cells (3).
foreign cells. Other possible mechanisms by which tumor
cells can avoid effective immune reactions include antigenic The meaning of the interfaces
modulation (74), already known for both human and animal These many interfaces between the malignant adaptation on
tumor cells (70) and inhibition of "the cellular display" of the one hand and immunologic adaptation on the other,
Alexander and others in development of immunity (75). suggest that these two adaptive processes have been inter-
Oncogenic viruses as immunosuppressants acting in some important and possibly essential way for a
Working with the Gross passage A virus, Peterson, Dent, and very long period. There can be no question that Thomas'
I (76, 77) discovered that oncogenic viruses can suppress postulate has been useful. VWhether it is correct is another
cellular as well as certain humoral immune adaptations. In matter. Prehn has beautifully summarized evidence, which
more lateral studies, similar profound influences of various he believes argues against the concept of immunosurveillance
oncogenic viruses on different immune responses have been (54). By contrast, he visualizes the essential relation between
discovered (78). Indeed, it seems a characteristic of many immunity and tumor antigenicity in another way, namely,
oncogenic and nononcogenic viruses that they have capacity that the tumor-specific antigens and the nonself nature of the
to inhibit development and expression of immune reactions, malignant cells may in some way be essential to their ex-
especially cellular immune reactions (79). The temporary and pression of a malignant nature. Whichever view is correct, it
seems that the foreignness of malignant cells will be used to
long-term influences of oncogenic viruses on cellular immune
functions needs much more study, especially at a molecular detect the occurrence of malignancy and perhaps even to
level. Certainly, the capacity of the cells involved in cellular prevent and treat the malignant process. In the latter direc-
immunity to synthesize protein, DNA, and RNA in response tion, the carcinoembryonic antigens first looked at by Gold
to mitogenic stimuli as with phytohemagglutinin (80-82), and Freedman (89), Uriel (90) and others, as well as the
allogeneic cells, or antigen can be profoundly influenced by tumor-specific transplantation antigens, hold promise. Crude
exposure to viruses like rubella virus, rubeola virus, or New- efforts at immunotherapy already are being attempted (91).
castles disease virus. Bone marrow transplantation (92), thymic transplantation
(93, 94), and the use of transfer factor (95) represent the
Relation between nutrition, immunity, and malignancy first steps in correction of the immunodeficiencies that as
Beginning with studies by Moreschi in 1909 (83) and Rous model systems have taught us so much about the development
in 1914 (84) an abundant literature has accumulated indi- and organization of the lymphoid system. Ultimately,
cating that experimental animals that are nutritionally somatic cellular genetic analysis, genetic engineering, and
deprived are less prone to develop various malignancies than cellular engineering applied to these diseases can give us
are well-nourished animals. Protein nutritional deprivation powerful new approaches for correction of these and other
and deprivation of essential amino acids particularly inhibit immunologic deficits that underly development of malig-
development of malignancy in many systems. Recent dis- nancy.
Downloaded by guest on October 18, 2021Proc. Nat. Acad. Sci. USA 69 (1972) Relations between Immunity and Malignancy 1031
The author is an American Legion Memorial Research Profes- Series, eds. Good, R. A. & Bergsma, D. (National Founda-
sor Regents' Professor of Pediatrics, Pathology, and Microbi- tion Press, New York), pp. 370-377.
ology. Aided by grants from the American Cancer Society, The 35. Biggar, W. D., Lapointe, N., Ishizaka, K., Meuwissen, H.,
National Foundation-March of Dimes, and U.S. Public Health Good, R. A. & Frommel, D. (1970) Lancet ii, 1089.
Service (AI-08677), and contract from the Special Cancer Virus 36. Wiskott, A. (1937) Monatsschr. Kinderheilk 68, 212-214.
Program (NIH 71-2261). 37. Aldrich, R. A., Steinberg, A. G. & Campbell, D. C. (1954)
Pediatrics 13, 133-139.
1. Thomas, L. (1961) in Cellular and Humoral Aspects of the 38. St. Geme, J. W., Jr., Prince, J. T., Burke, B. A., Good, R. A.
Hypersensitive States, ed. Lawrence, H. W. (Hoeber-Harper, & Krivit, W. (1965) N. Engl. J. Med. 273, 229-234.
New York), pp. 529-532. 39. Cooper, M. D., Chase, B. P., Lowman, J. T., Krivit, W. &
2. Medewar, P. B. (1961) in Cellular and Humoral Aspects of Good, R. A. (1968) in Immunologic Deficiency Diseases in
the Hypersensitive States, ed. Lawrence, H. S. (Hoeber- Man. Birth Defects Original Article Series, eds. Good, R. A.
Harper, New York), pp. 504- 529. & Bergsma, D. (National Foundation Press, New York), pp.
3. Burnet, F. M. (1970) in Progress in Experimental Tumor 378-387.
Research (Karger, Basel), pp. 1-27. 40. Cooper, M. D., Chase, H. P., Lowman, J. T., Krivit, W. &
4. Smith, R. T. & Landy, M. (eds.) (1970) Immunological Sur- Good, R. A. (1968) Amer. J. Med. 44, 499-513.
veillance (Academic Press, New York). 41. Blaese, R. M., Strober, W., Brown, R. S. & Waldmann,
5. Good, R. A., Kelly, W. D., Rotstein, J. & Varco, R. L. T. A. (1968) Lancet i, 1056-1061.
(1962) in: Progress in Allergy (Karger, Basel and New 42. Ten Bensel, R. W., Stadlan, E. M. & Krivit, W. (1966) J.
York), pp. 187-319. Pediat. 68, 761-767.
6. Good, R. A. (1955) J. Lancet 75, 245-271. 43. Seligmann, M., Fudenberg, H. & Good, R. A. (1968) Amer.
7. Good, R. A. (1954) Revue Hematol. 9, 502-503. J. Med. 45, 817-825.
8. Good, R. A. (1955) J. Lab. Clin. Med. 46, 167-181. 44. Fudenberg, H. H., Good, R. A., Goodman, H. C., Hitzig,
9. Peterson, R. D. A., Cooper, M. D. & Good, R. A. (1965) W., Kunkel, H. G., Roitt, I. M., Rosen, F. S., Rowe, D. S.,
Amer. J. Med. 38, 579-604. Seligmann, M. & Soothill, J. R. (1971) Pediatrics 47, 927-
10. Cooper, M. D., Lawton, A. R. & Bockman, D. E. (1971) 946.
Lancet ii, 791-794. 45. Rosen, F. S., Craig, J. M., Vawter, G. & Janeway, C. A.
11. Grey, H. M., Rabellino, E. & Pirofsky, B. (1971) J. Clin. (1968) in Immunologic Deficiency Diseases in Man, Birth
Invest. 50, 2368-2375. Defects Original Article Series, eds. Good, R. A. & Bergsma,
12. Good, R. A., Zak, S. J., Jensen, D. R. & Papenheimer, A. M., D. (National Foundation Press, New York), pp. 67-70.
Jr. (1957) J. Clin. Invest. 39, 894. 46. Wolf, J. K., Gokcen, M. & Good, R. A. (1963) J. Lab. Clin.
13. Good, R. A. & Zak, S. J. (1956) Pediatrics 18, 109-149. Med. 61, 230-248.
14. Good, R. A. (1971) in Progress in Immunology, ed. Amos, B. 47. Pernis, B. & Kunkel, H. (1971) Discussion of Good, Biggar,
(Academic Press, New York), pp. 699-722. and Park in Progress in Immunology, ed. Amos, B. (Academic
15. Good, R. A., Varco, R. L., Aust, J. B. & Zak, S. J. (1957) Press, New York) p. 723.
Ann. N.Y. Acad. Sd. 64, 882-924. 48. Park, B. H. & Good, R. A. (1972) Proc. Nat. Acad. Sci USA
16. Page, A. R., Hansen, A. E. & Good, R. A. (1963) Blood 21, 69, 371-373.
197-206. 49. Windhorst, D. B., Zelickson, A. S. & Good, R. A. (1966)
17. Gatti, R. A. & Good, R. A. (1971) Cancer 28, 89-98. Science 151, 81-83.
18. Schier, W. W., Roth, A., Ostroff, G. & Schrift, M. H. (1956) 50. Page, A. R., Berendes, H., Warner, J. & Good, R. A. (1962)
Amer. J. Med. 20, 94-99. Blood 20, 330-343.
19. Kelly, W. D., Good, R. A. & Varco, R. L. (1958) Surg. 51. Malmgren, R. A., Bennison, B. E. & McKinley, T. W., Jr.
Gynec. Obstet. 107, 565-570. (1952) Proc. Soc. Exp. Biol. Med. 79, 484-488.
20. Lamb, D., Pilney, F., Kelly, W. D. & Good, R. A. (1962) J. 52. Good, R. A. & Finstad, J. (1969) Nat. Cancer Inst. Monogr.
Immunol. 89, 555-558. 31, 41-58.
21. Kelly, W. D., Lamb, D. I., Varco, R. L. & Good, R. A. 53. Stzernsward, J. (1966) J. Nat. Cancer Inst. 37, 505-512.
(1960) Ann. N.Y. Acad. Sd. 87, 187-202. 54. Prehn, R. T. (1970) in Immune Surveillance, eds. Smith,
22. Good, R. A., Kelly, W. D. & Gabrielsen, A. E. (1962) in R. T. & Landy, M. (Academic Press, New York), pp. 451-
Second International Symposium on Immunopathology, Benno 462.
Schwabe & Co. (Basel, Switzerland), pp. 353-384. 55. Prehn, R. T. (1963) J. Nat. Cancer Inst. 31, 791-805.
23. Warwick, W. J., Archer, 0. K., Kelly, W. D. & Page, A. R. 56. Prehn, R. T. (1964) J. Nat. Cancer Inst. 32, 1-17.
(1961) Fed. Proc. 20, 18-00. 57. Klein, G. (1969) Fed. Proc. 28, 1739-1753.
24. Zinneman, H. H. & Hall, W. H. (1954) Ann. Inter. Med. 41, 58. Defendi, V., Roosa, R. A. & Koprowski, H. (1964) in The
1152-1163. Thymus in Immunobiology. eds. Gabrielsen, A. E. & Good,
25. Seligmann, M. (1971) Presented on section of Immune Dis- R. A. (Hoeber-Harper, New York), pp. 504-520.
orders of Man panel at First Internatiqnal Congress of Im- 59. Allison, A. C. & Law, L. W. (1968) Proc. Soc. Rap. Biol.
munology. In Progress in Immunology (Academic Press, Med. 127, 207-212.
New York). 60. Allison, A. C., Berman, L. H. & Levey, R. N. (1967) Nature
26. Cone, L. & Uhr, J. W. (1964) J. Clin. Invest. 43, 2241-2248. 215, 185-187.
27. Dent, P. B., Peterson, R. D. A. & Good, R. A. (1968) in 61. Wilson, R. E., Hager, E. B., Hampers, C. L., Corson, J. M.,
Immunologic Deficiency Diseases in Man, Birth Defects Merrill, J. P. & Murray, J. E. (1968) N. Engl. J. Med. 278,
Original Articles Series, eds. Good, R. A. & Bergsma, D. 479-483.
(National Foundation Press, New York), pp. 443-458. 62. McKhann, C. F. (1969) Transplantation 8, 209-212.
28. Southam, C. M. (1961) Cancer Res. 21, 1302-1316. 63. Penn, I., Halgrimson, C. G. & Starzl, T. E. (1972) Trans-
29. Louis-Bar (1941) Confin. Neurol. 4, 32-42. plant. Proc., in press.
30. Boder, E. & Sedgwick, R. P. (1963) Little Club Clin. Develop. 64. Starzl, T. E., Penn, I. & Halgrimson, C. G. (1970) N. Engi.
Med. 8, 110-118. J. Med. 283, 934.
31. Boder, E. & Sedgwick, R. P. (1963) in Cerebellum, Posture 65. McPhaul, J. J., Jr. & McIntosh, D. A. (1968) N. Engl. J.
and Cerebral Palsy, ed Walsh, G. (London), pp. 110-118. Med. 272, 105.
32. Lambrechts, A. F. & Snoijink, J. J. (1971) Ataxia telangi- 66. Klein, G. (1966) Is. J. Med. Sci. 2, 135-142.
ectasia. Morbus Lympholyticus Congenitalis (J. E. Bush- 67. Prehn, R. T. & Main, J. M. (1957) J. Nat. Cancer Inst. 18,
mann, Antwerpen, Belgium). 769-778.
33. Peterson, R. D. A., Kelly, W. D. & Good, R. A. (1964) 68. Smith, R. T. (1968) N. Eng. J. Med. 278, 1207-1214, 1268-
Lancet i, 1189-1193. 1275, and 1326-1331.
34. Peterson, R. D. A. & Good, R. A. (1968) in Immunologic 69. Hellstrom, I. & Hellstro1n, K. E. (1969) Int.J. Cancer 4,
Deficiency Diseases in Man, Birth Defects Original Article 587-600.
Downloaded by guest on October 18, 20211032 Good Proc. Nat. Acad. Sci. USA 69 (1972)
70. Hellstrom, I., Evans, C. A. & Hellstrom, K. E. (1969) Int. 82. Olson, G. B., South, M. A. & Good, R. A. (1967) Nature 214,
J. Cancer 4, 601-607. 695-696.
71. Hellstrom, K. E. & Hellstrom, I. (1970) Hosp. Pract. 5, 45- 83. Moreschi, C. (1909) Z. Immunitaetsforsch. 2, 651-685.
61. 84. Rous, P. (1914) J. Exp. Med. 20, 433-451.
72. Hellstrom, I., Hellstrom, K. E., Sjogren, H. 0. & Warner, 85. Jose, D. G., Cooper, W. C. & Good, R. A. (1971) J. Amer.
G. A. (1971) Int. J. Cancer 7, 1-16. Med. Ass. 218, 1428-1429.
73. Kaliss, N. & Fitch, F. W. (1971) in Progress in Immunology, 86. Sigel, M. & Good, R. A. (eds.), in Tolerance, Autoimmunity
ed. Amos, B. (Academic Press, New York), pp. 1545-1547. and Aging (Charles C Thomas, Springfield), in press.
74. Old, L. J., Stockert, E., Boyse, E. A. & Kim, J. H. (1968) 87. Yunis, E. J., Stutman, O., Fernandes, G., Teague, P. 0. &
J. Exp. Med. 127, 523-539. Good, R. A. (1972) in Tolerance, Autoimmunity and Aging,
75. Alexander, P. (1968) Progr. Exp. Tumor Res. 10, 22-71. eds. Sigel, M. & Good, R. A. (Charles C Thomas, Spring-
76. Peterson, R. D. A., Hendrickson, R. & Good, R. A. (1963) field).
Proc. Soc. Exp. Biol. Med. 114, 517-520. 88. Yunis, E. J., Stutman, 0. & Good, R. A. (1971) Ann. N.Y.
77. Dent, P. B., Peterson, R. D. A. & Good, R. A. (1965) Proc. Acad. Sci. 183, 205-220.
Soc. Exp. Biol. Med. 119, 869-871. 89. Gold, P. & Freedman, S. 0. (1965) J. Exp. Med. 122, 467-
481.
78. Friedman, H. & Ceglowski, W. S. (1971) in Progress in Im- 90. Uriel, J., Nechaud, B. de, Birencwajg, M. S., Masseyeff, R.,
munology, ed. Amos, B. (Academic Press, New York), pp. Leblanc, L., Quenum, C., Loisillier, F. & Grabar, P. (1967)
815-829. C.R. Acad. Sci. 265, 75-78.
79. Olson, G. B., Dent, P. B., Rawls, W. E., South, M. A., 91. Mathe, G. (1971) Hosp. Pract. 6, 43-51.
Montgomery, J. R., Melnick, J. L. & Good, R. A. (1968) 92. Good, R. A. (1971) J. Amer. Med. Ass. 214, 1289-1300.
J. Exp. Med. 128, 47-68. 93. Cleveland, W. W., Fogel, B. J., Brown, W. T. & Kay, H. E.
80. Rawls, W. E., Melnick, J. L., Olson, G. B., Dent, P. B. & M. (1968) Lancet ii, 1211-1214.
Good, R. A. (1968) Science 158, 506-507. 94. August, C. S., Rosen, F. S., Filler, F. M., Janeway, C. A.,
81. Montgomery, J. R., South, M. A., Rawls, W. E., Melnick, Markowski, B. & Kay, H. E. M. (1968) Lancet ii, 1210-1211.
J. L., Olson, G. B., Dent, P. B. & Good, R. A. (1967) Science 95. Levin, A. S., Spitler, L. E., Stites, D. P. & Fudenberg, H. H.
157, 1068-1070. (1970) Proc. Nat. Acad. Sci. USA 67, 821-828.
Downloaded by guest on October 18, 2021You can also read