The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Bronchopneumonia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
6/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
THE BRIEF CASE
July 2021 Volume 59 Issue 7 e02472-20
https://doi.org/10.1128/JCM.02472-20
The Brief Case: Capnocytophaga sputigena Bacteremia in a
94-Year-Old Male with Type 2 Diabetes Mellitus,
Pancytopenia, and Bronchopneumonia
Benjamin M. Liu a, Christopher P. Carlisle b, Mark A. Fisher a,c, and Salika M. Shakir a,c
a Department of Pathology, University of Utah School of Medicine, Salt Lake City, Utah, USA
b Department of General Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah, USA
c ARUP Laboratories, Salt Lake City, Utah, USA
KEYWORDS Capnocytophaga sputigena, bacteremia, pancytopenia, bronchopneumonia
Published 18 June 2021
Citation Liu BM, Carlisle CP, Fisher MA, Shakir SM. 2021. The Brief Case: Capnocytophaga sputigena bacteremia
in a 94-year-old male with type 2 diabetes mellitus, pancytopenia, and bronchopneumonia. J Clin Microbiol
59:e02472-20. https://doi.org/10.1128/JCM.02472-20.
Editor Burnham Carey-Ann D., Washington University School of Medicine
Copyright © 2021 American Society for Microbiology. All Rights Reserved.
CASE
A
94-year-old male presented to the emergency department with 3 days of fever and total
body weakness. The patient’s past medical history was significant for coronary artery
disease, type 2 diabetes mellitus, gastroesophageal reflux disease, Parkinsonism, hypertension,
and chronic kidney disease. Physical examination revealed fever (38.7°C), mild elevation in blood
pressure (138/62 mm Hg) and a normal room air oxygen saturation of 96%. Lung sounds were
distant, and no rales, wheezing, or rhonchi were appreciated. The patient presented with
tachycardia (heart rate, 112 beats per minute [bpm]) without murmur, rub, or gallop. The patient’s
abdomen was soft and nontender, and no peripheral edema was observed. Neurologic
examination showed diffuse, generalized motor weakness and fine resting hand tremor but was
otherwise normal. Recent laboratory tests showed pancytopenia (white blood cells, 1.16 ×
103/mm3; platelets, 8 × 103/mm3) and low hemoglobin (8.5 g/dl). Creatinine was 1.78 mg/dl with a
known baseline of 1.7 mg/dl. Chest X-ray (CXR) revealed peribronchial cuffing. The patient denied
cough, diarrhea, mouth pain, nausea, or vomiting. No recent pet exposures or animal bites were
reported. No mucositis, gingival disease, or mouth tenderness was noted in patient history.
However, given the patient’s advanced age, tooth loss, and poor dental care, the existence of
damage to the oral mucosa could not be ruled out. The patient’s social history was significant for
residing at an assisted living facility where a coronavirus disease 2019 (COVID-19) outbreak had
been present. The patient was initially suspected of having COVID-19, but initial and follow-up
COVID-19 molecular testing were both negative. Two sets of blood cultures were obtained, and
intravenous fluids were administered. Due to the peribronchial cuffing noted on CXR, ceftriaxone
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 1/76/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
and azithromycin were initiated to treat for possible early bronchopneumonia. Within 24 h of
admission, the patient developed acute hypotension and subsequently died of circulatory collapse.
Two sets of anaerobic blood culture bottles (Bactec; Becton, Dickinson, Sparks, MD) collected
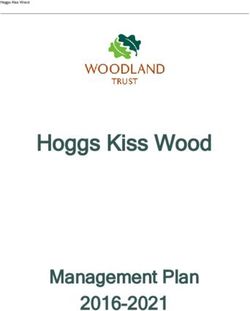
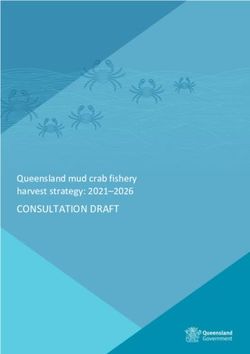
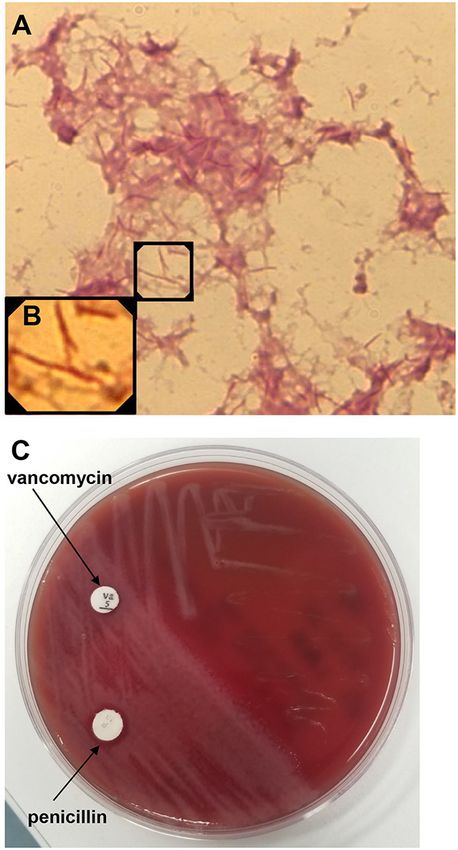
at the time of admission signaled positive on day 4 of incubation. Thin, spindle-shaped, Gram-
negative bacilli were observed on Gram stain (Fig. 1A and B). After 24 h, very small, gray,
nonhemolytic colonies with spreading edges grew on a Columbia blood agar plate incubated at
35°C with 5% CO2 (Fig. 1C). They reached 2 to 4 mm in diameter after 2 to 4 days and were
convex or flat and slightly yellow. The colonies were resistant to vancomycin (5 μg; Hardy
Diagnostics, Santa Maria, CA) and penicillin (10 IU; Becton, Dickinson, Sparks, MD) disks (Fig.
1C), and there was no growth on MacConkey plates. The isolate was identified as
Capnocytophaga sputigena by matrix-assisted laser desorption ionization–time of flight mass
spectrometry (MALDI-TOF MS) (Bruker Daltonik GmbH, Bremen, Germany) using Biotyper
software with the 8468 spectrum database. The MALDI score of the isolate was 2.46, which was
well above the threshold for a high-confidence species-level identification (≥2.0), and all database
matches were for C. sputigena. Additional biochemical testing confirmed that the isolate was
negative for catalase, oxidase, or indole production but positive for esculin hydrolysis, consistent
with the biochemical characteristics of C. sputigena. Antimicrobial susceptibility testing (AST) was
performed by adding 50 μl of a standard bacterial suspension (0.5 McFarland) to 11 ml brain heart
infusion broth supplemented with 5% lysed horse blood due to the fastidious nature of the
organism. The organism suspension was used to inoculate custom broth microdilution AST panels
(Sensititre; Thermo Fisher), followed by incubation at 35°C in 6.6% CO2 for 24 h. MIC values were
determined for penicillin (≥4 μg/ml), ceftriaxone (≥4 μg/ml), meropenem (≤0.06 μg/ml), ciprofloxacin
(≤0.12 μg/ml), levofloxacin (≤0.06 μg/ml), and azithromycin (0.12 μg/ml).
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 2/76/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
FIG 1 Phenotypic features of Capnocytophaga sputigena. (A) Gram stain of positive, anaerobic blood culture
demonstrating thin, spindle-shaped, Gram-negative bacilli. (B) Inset of image panel A highlighting the morphology of
the Gram-negative bacilli. (C) Gray, nonhemolytic colonies on a Columbia blood agar plate after 24 h of incubation
at 35°C with 5% CO2. Note the spreading edges with gliding motility and the resistance results to the indicated
vancomycin (5 μg) and penicillin (10 IU) disks.
DISCUSSION
Belonging to the Flavobacteriaceae family, members of the genus Capnocytophaga are fastidious,
facultatively anaerobic, indole-negative, fusiform Gram-negative bacilli, consisting of eight species,
i.e., Capnocytophaga canimorsus, Capnocytophaga cynodegmi, Capnocytophaga gingivalis,
Capnocytophaga granulosa, Capnocytophaga haemolytica, Capnocytophaga leadbetteri,
Capnocytophaga ochracea, Capnocytophaga sputigena, and the unnamed genospecies AHN8471
(1). As suggested by its name (the Greek “kapnos” meaning “smoke”), Capnocytophaga is
capnophilic (carbon dioxide loving) and displays enhanced growth in high concentrations of
carbon dioxide. Capnocytophaga species fail to grow on enteric media and are infrequently
isolated from clinical samples. They are nonmotile, but their colonies on blood agar can
demonstrate spreading edges with gliding motility (Fig. 1C).
Most bacteria in the genus Capnocytophaga are normal but not prominent members of the oral
or nasopharyngeal microbiota of animals or humans and may cause opportunistic infections in
humans. Catalase and oxidase can be used to divide Capnocytophaga spp. into zoonotic and
human groups. The oxidase- and catalase-positive species C. canimorsus and C. cynodegmi are
considered part of oral flora of healthy dogs and cats (2). Human clinical cases of C. canimorsus
or C. cynodegmi infection are often associated with dog or cat bites or contact (e.g., licking of
wounds). Conversely, the oxidase- and catalase-negative species, such as C. ochracea, C.
gingivalis, C. sputigena, C. haemolytica, and C. granulosa, inhabit the oral cavities of humans.
Among them, C. ochracea, C. gingivalis, and C. sputigena are considered periodontal pathogens,
although they were also isolated from adults without periodontitis (1, 3, 4). Furthermore, the
oxidase- and catalase-negative species can also cause extraoral infections in immunocompetent
and immunocompromised patients, including septicemia, empyema, endocarditis, endometritis,
osteomyelitis, soft tissue infections, peritonitis, ophthalmic lesions, and noma (1, 5).
C. sputigena bacteremia has been reported among immunocompromised patients with
hematological malignancy during the neutropenic period, for instance, chronic lymphocytic
leukemia, relapsed lymphoma/leukemia after hematopoietic stem cell transplantation (HSCT), or
Hodgkin’s lymphoma after bone marrow transplantation (6–10). Most of these infections were
found to be accompanied with oral mucositis and ulceration during chemotherapy, which may
increase the risk of spreading the organisms from oral cavity to the bloodstream (9). In contrast to
C. ochracea, the most frequently isolated species causing bloodstream infections in auto-HSCT
patients (9), C. sputigena has been isolated from sputum or pleural fluid in rare cases of
community-acquired pneumonia and empyema and from other body sites in patients with mild or
unnoted mucositis (5, 6, 9, 11). Lo et al. recently reported C. sputigena pneumonia and
bacteremia in an 84-year-old patient with type 2 diabetes mellitus (12). Interestingly, though C.
sputigena is not present in the female genital tract, it appears to be a potential risk factor for
second-trimester abortion, chorioamnionitis, and neonatal infections (13–15). Organisms
introduced into the vaginal area during pregnancy may result in preterm labor as well as
septicemia and respiratory failure in newborn children (13, 14).
Identification of Capnocytophaga species using conventional phenotypic methods is
challenging and may present some difficulties in disease diagnosis. In positive blood culture
samples, the organisms may be difficult to discern from the background due to weak staining (Fig.
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 3/76/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
1A and B). Colonies of Capnocytophaga spp. on blood agar are very small after 24 h of incubation
at 37°C (Fig. 1C) and would need an additional 1 to 3 days to grow to a larger diameter for
recognition. Other fastidious Gram-negative bacteria that colonize the human or animal oral cavity,
such as the HACEK group (a group of Gram-negative bacilli consisting of Haemophilus spp.,
Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and
Kingella spp.), may cause similar endogenous infections as Capnocytophaga species (1). As
shown in Table 1, animal contact or exposure history, Gram stain appearance (typical morphology
of medium-to-long fusiform cells), colony characteristics, and biochemical testing, to some extent,
may be helpful to distinguish some Capnocytophaga spp. (e.g., C. canimorsus) from the HACEK
group. Catalase and oxidase are useful to distinguish zoonotic C. canimorsus and C. cynodegmi
from other catalase- and oxidase-negative human oral Capnocytophaga spp. However, within the
oxidase-negative group, similar biochemical reactions of some species may make their phenotypic
differentiation inconclusive. Of note, esculin hydrolysis is a useful biochemical test to confirm C.
sputigena, which is positive. Molecular methods, like 16S rRNA gene PCR and sequencing, are
considered useful diagnostic tools for the identification and differentiation of Capnocytophaga
species. Commercial MALDI-TOF MS systems can reliably identify C. sputigena, and the Vitek 2
ID-NH card may also be used for genus-level identification (1).
There are no AST guidelines or interpretive breakpoints for Capnocytophaga spp. from the
Clinical and Laboratory Standards Institute (CLSI) or European Committee on Antimicrobial
Susceptibility Testing (EUCAST), making it challenging to perform or interpret AST results for C.
sputigena. Despite this, breakpoints established for other organisms, such as anaerobes or
HACEK organisms, have been used in previous studies (6, 16), resulting in Capnocytophaga spp.
being considered susceptible to clindamycin, linezolid, tetracyclines, carbapenems, and beta-
lactam combination agents but resistant to polymyxins. MICs are variable for aminoglycosides,
cephalosporins, macrolides, and fluoroquinolones, suggesting that AST should be performed if
considering these agents (17). Multidrug-resistant C. sputigena strains have been isolated from
patients with bacteremia or lung abscess; a bloodstream isolate with high MICs to β-lactams (e.g.,
penicillins and first-, second-, and third-generation cephalosporins), ciprofloxacin, and
trimethoprim was described (8), and an isolate from a lung abscess following bronchoscopy was
considered resistant using EUCAST HACEK breakpoints to all tested drugs except imipenem,
including penicillins, first-, third-, and fourth-generation cephalosporins, levofloxacin, azithromycin,
clindamycin, and minocycline (18). Clinical treatment failure was observed on initial therapy with
garenoxacin, ampicillin-sulbactam, clindamycin, and cefepime, and improvement was seen only
after switching to carbapenem therapy (18). Of note, β-lactam antibiotic MICs vary among
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 4/76/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
Capnocytophaga spp. Up to ∼80% of Capnocytophaga species isolates may carry β-lactamases,
including the extended-spectrum β-lactamases (ESBL) CfxA and CSP-1 in C. sputigena (19, 20).
Such isolates are generally considered resistant to amoxicillin and most cephalosporins (19, 20).
In a study on 48 Capnocytophaga isolates from periodontitis patients (21), C. sputigena was the
predominant species (64%) producing β-lactamases, followed by C. ochracea isolates (11%).
Interestingly, blaCSP-1 was identified only in a subgroup of these C. sputigena isolates (21).
Another ESBL, TEM-17, has been described in C. ochracea, and whole-genome sequencing
revealed a novel class D beta-lactamase (blaOXA-347, related to blaOXA-48) with broad-substrate
specificity, including amoxicillin-clavulanate and imipenem, from animal-associated
Capnocytophaga species (22, 23). Macrolide and clindamycin resistance due to erm(C) and
erm(F) genes has been described (21), and gyrA mutations are associated with fluoroquinolone
resistance (7, 16, 20, 22).
In summary, we present a case on C. sputigena bacteremia in a patient with diabetes and
pancytopenia. Our case illustrates the importance of accurate identification for this
underappreciated but important Gram-negative organism. Notably, microbiologists and clinicians
should recognize that C. sputigena strains can exhibit high MICs to β-lactam antibiotics and
fluoroquinolones, necessitating antimicrobial susceptibility testing.
SELF-ASSESSMENT QUESTIONS
1. Which body site is the habitat of Capnocytophaga sputigena in mammals?
a. Oral cavity of dogs
b. Oral cavity of humans
c. Female genital tract of dogs
d. Female genital tract of humans
2. Which of the following biochemical testing results can differentiate Capnocytophaga sputigena
from C. canimorsus?
a. Catalase positive and oxidase positive
b. Catalase negative and oxidase negative
c. Catalase positive and oxidase negative
d. Catalase negative and oxidase positive
3. Which of the following resistance mechanisms may be found in multidrug-resistant
Capnocytophaga sputigena?
a. CSP-1
b. VanC
c. KPC
d. NDM
For answers to the self-assessment questions and take-home points, see
https://doi.org/10.1128/JCM.02473-20 in this issue.
REFERENCES
1. Zbinden R. 2015. Aggregatibacter, Capnocytophaga, Eikenella, Kingella, Pasteurella, and other
fastidious or rarely encountered Gram-negative rods: bacterology, p 652–666. In Jorgensen JH, Pfaller
MA, Carroll KC, Funke G, Landry ML, Richter SS, Warnock DW (ed), Manual of clinical microbiology,
11th ed, vol 1. ASM Press, Washington, DC. Crossref.
2. van Dam AP, van Weert A, Harmanus C, Hovius KE, Claas EC, Reubsaet FA. 2009. Molecular
characterization of Capnocytophaga canimorsus and other canine Capnocytophaga spp. and
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 5/76/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
assessment by PCR of their frequencies in dogs. J Clin Microbiol 47:3218–3225. 10.1128/JCM.01246-
09. PubMed.
3. Stevens RH, Sela MN, McArthur WP, Nowotny A, Hammond BF. 1980. Biological and chemical
characterization of endotoxin from Capnocytophaga sputigena. Infect Immun 27:246–254.
10.1128/IAI.27.1.246-254.1980. PubMed.
4. Frandsen EV, Poulsen K, Könönen E, Kilian M. 2008. Diversity of Capnocytophaga species in children
and description of Capnocytophaga leadbetteri sp. nov. and Capnocytophaga genospecies AHN8471. Int
J Syst Evol Microbiol 58:324–336. 10.1099/ijs.0.65373-0. PubMed.
5. Li A, Tambyah P, Chan D, Leong KK. 2013. Capnocytophaga sputigena empyema. J Clin Microbiol
51:2772–2774. 10.1128/JCM.00884-13. PubMed.
6. Kim JA, Hong SK, Kim EC. 2014. Capnocytophaga sputigena bacteremia in a patient with chronic
lymphocytic leukemia. Ann Lab Med 34:325–327. 10.3343/alm.2014.34.4.325. PubMed.
7. Isabel R. 2019. Capnocytophaga sputigena bacteremia in a neutropenic host. IDCases 17:e00536.
10.1016/j.idcr.2019.e00536. PubMed.
8. Gomez-Garces JL, Alos JI, Sanchez J, Cogollos R. 1994. Bacteremia by multidrug-resistant
Capnocytophaga sputigena. J Clin Microbiol 32:1067–1069. 10.1128/JCM.32.4.1067-1069.1994.
PubMed.
9. García-Cía JI, Esteban J, Santos-O'Connor F, Román A, Soriano F. 2004. Mixed bacteremia with
Capnocytophaga sputigena and Escherichia coli following bone marrow transplantation: case report and
review. Eur J Clin Microbiol Infect Dis 23:139–141. 10.1007/s10096-003-1063-7. PubMed.
10. Mendes FR, Bruniera FR, Schmidt J, Cury AP, Rizeck C, Higashino H, Oliveira FN, Rossi F, Rocha V,
Costa SF. 2020. Capnocytophaga sputigena bloodstream infection in hematopoietic stem cell
transplantations: two cases report and review of the literature. Rev Inst Med Trop Sao Paulo 62:e48.
10.1590/s1678-9946202062048. PubMed.
11. Gosse L, Amrane S, Mailhe M, Dubourg G, Lagier JC. 2019. Capnocytophaga sputigena: an unusual
cause of community-acquired pneumonia. IDCases 17:e00572. 10.1016/j.idcr.2019.e00572. PubMed.
12. Lo SH, Chang YY, Jao YT, Wang WH, Lu PL, Chen YH. 2018. Capnocytophaga sputigena pneumonia
and bacteremia in a patient with diabetes and gastric cancer. J Microbiol Immunol Infect 51:578–579.
10.1016/j.jmii.2017.11.005. PubMed.
13. Vandemeulebrouck B, Rasigade JP, Sobas C, Vialet A, Roubille M. 2008. Septicaemia with
Capnocytophaga sputigena in a newborn child. Ann Biol Clin (Paris) 66:215–219. (In French.).
10.1684/abc.2008.0212. PubMed.
14. Alanen A, Laurikainen E. 1999. Second-trimester abortion caused by Capnocytophaga sputigena: case
report. Am J Perinatol 16:181–183. 10.1055/s-2007-993854. PubMed.
15. Mekouar H, Voortman G, Bernard P, Hutchings G, Boeras A, Rodriguez-Villalobos H. 2012.
Capnocytophaga species and perinatal infections: case report and review of the literature. Acta Clin Belg
67:42–45. 10.2143/ACB.67.1.2062626. PubMed.
16. Ehrmann E, Jolivet-Gougeon A, Bonnaure-Mallet M, Fosse T. 2017. Role of DNA gyrase and
topoisomerase IV mutations in fluoroquinolone resistance of Capnocytophaga spp. clinical isolates and
laboratory mutants. J Antimicrob Chemother 72:2208–2212. 10.1093/jac/dkx119. PubMed.
17. Jolivet-Gougeon A, Sixou JL, Tamanai-Shacoori Z, Bonnaure-Mallet M. 2007. Antimicrobial treatment of
Capnocytophaga infections. Int J Antimicrob Agents 29:367–373. 10.1016/j.ijantimicag.2006.10.005.
PubMed.
18. Migiyama Y, Anai M, Kashiwabara K, Tomita Y, Saeki S, Nakamura K, Okamoto S, Ichiyasu H, Fujii K,
Kohrogi H. 2018. Lung abscess following bronchoscopy due to multidrug-resistant Capnocytophaga
sputigena adjacent to lung cancer with high PD-L1 expression. J Infect Chemother 24:852–855.
10.1016/j.jiac.2018.03.017. PubMed.
19. Guillon H, Eb F, Mammeri H. 2010. Characterization of CSP-1, a novel extended-spectrum beta-
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 6/76/27/2021 The Brief Case: Capnocytophaga sputigena Bacteremia in a 94-Year-Old Male with Type 2 Diabetes Mellitus, Pancytopenia, and Br…
lactamase produced by a clinical isolate of Capnocytophaga sputigena. Antimicrob Agents Chemother
54:2231–2234. 10.1128/AAC.00791-09. PubMed.
20. Handal T, Giraud-Morin C, Caugant DA, Madinier I, Olsen I, Fosse T. 2005. Chromosome- and plasmid-
encoded beta-lactamases in Capnocytophaga spp. Antimicrob Agents Chemother 49:3940–3943.
10.1128/AAC.49.9.3940-3943.2005. PubMed.
21. Ehrmann E, Handal T, Tamanai-Shacoori Z, Bonnaure-Mallet M, Fosse T. 2014. High prevalence of β-
lactam and macrolide resistance genes in human oral Capnocytophaga species. J Antimicrob
Chemother 69:381–384. 10.1093/jac/dkt350. PubMed.
22. Jolivet-Gougeon A, Tamanai-Shacoori Z, Desbordes L, Burggraeve N, Cormier M, Bonnaure-Mallet M.
2004. Genetic analysis of an ambler class A extended-spectrum beta-lactamase from Capnocytophaga
ochracea. J Clin Microbiol 42:888-90. 10.1128/jcm.42.2.888-890.2004. PubMed.
23. Zangenah S, Andersson AF, Özenci V, Bergman P. 2017. Genomic analysis reveals the presence of a
class D beta-lactamase with broad substrate specificity in animal bite associated Capnocytophaga
species. Eur J Clin Microbiol Infect Dis 36:657–662. 10.1007/s10096-016-2842-2. PubMed.
https://journals.asm.org/doi/epub/10.1128/JCM.02472-20 7/7You can also read