The renal collecting duct carcinoma (CDC) (Bellini duct carcinoma), case report - A. Barakauskienė, L. Neverauskienė, T. Petraitis, J. Strimaitienė
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The renal collecting duct carcinoma (CDC) (Bellini duct carcinoma), case report A. Barakauskienė, L. Neverauskienė, T. Petraitis, J. Strimaitienė
The renal collecting duct carcinoma (CDC)
exhibits special clinicopathological
features, high degree of malignancy and poor
prognosis
Synonyms like Bellini duct carcinoma,
medullary renal carcinoma, distal renal
tubular carcinoma and distal nephron
carcinoma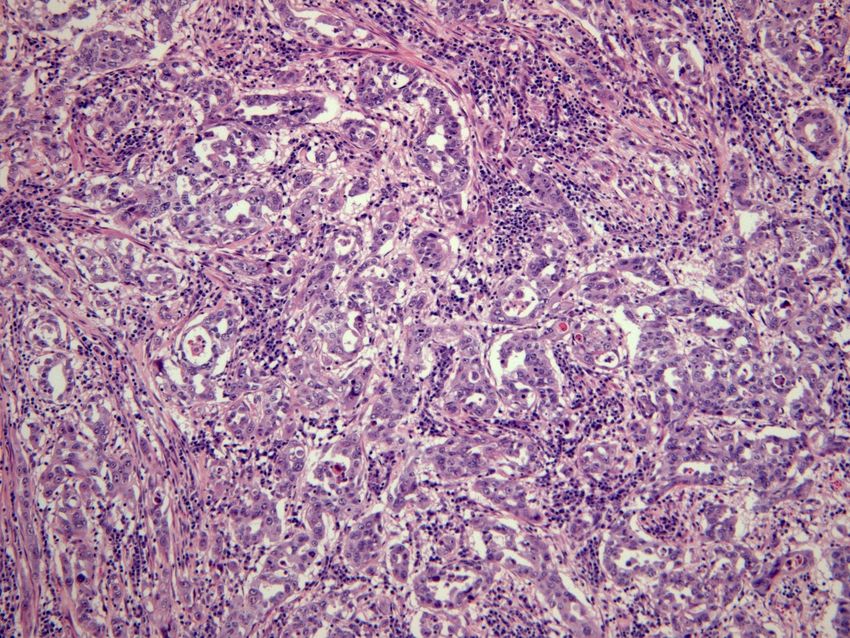
The diagnosis depends on the
histopathological examination
Early detection and early surgical treatment
are still the main methods to improve the
prognosis of patients with CDC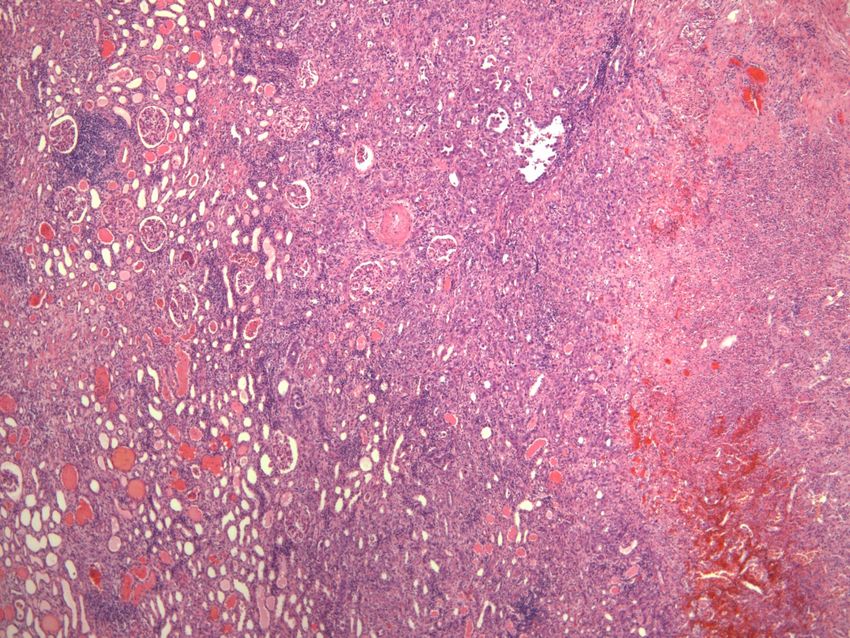
CDC is located in the renal medulla and
originates from the epithelial cells of Bellini
collecting ducts
Currently, WHO names it as Bellini duct
carcinoma, it’s considered to be an independent
histological type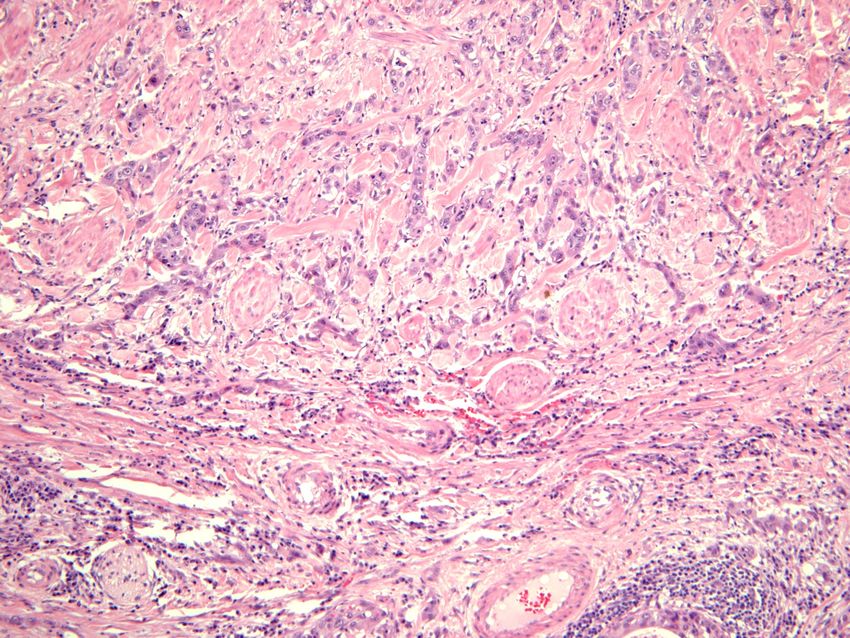
CDC is an unusual variant of renal cell
carcinoma and accounts for about 1-2% of all
renal cell carcinomas
The average onset age is 58 years and male
patients account for 72% of the cases
CDC metastasizes to regional lymph nodes in
approximately 80% of cases, to the lung or
adrenal gland in 25% and to the liver in 20%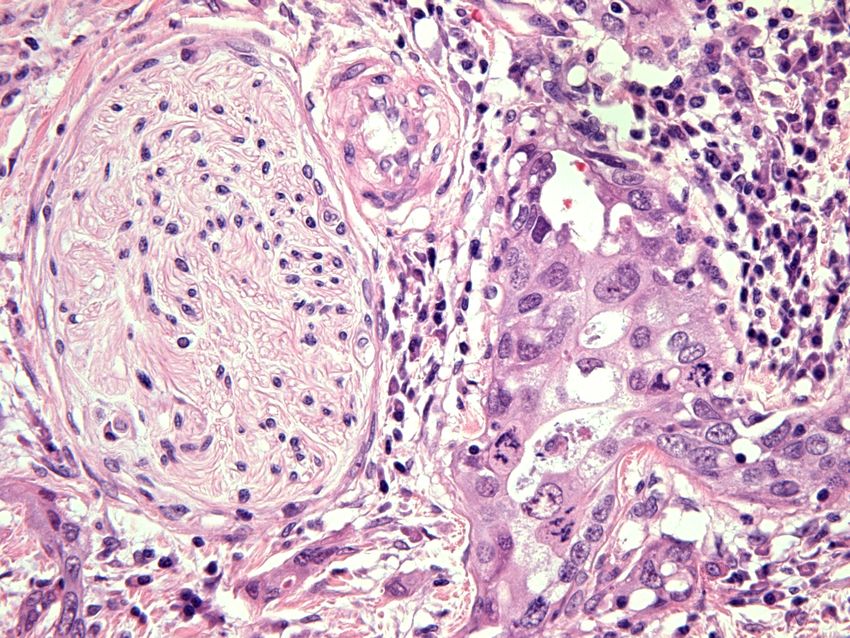
Painless gross hematuria, lumbar abdominal
pain, waist and abdominal mass, fatigue,
fever, and weight loss
Metastasis occurs in most of patients before
treatment, including bone metastasis and
lymph node metastasis
Average survival time has been reported to be
22 months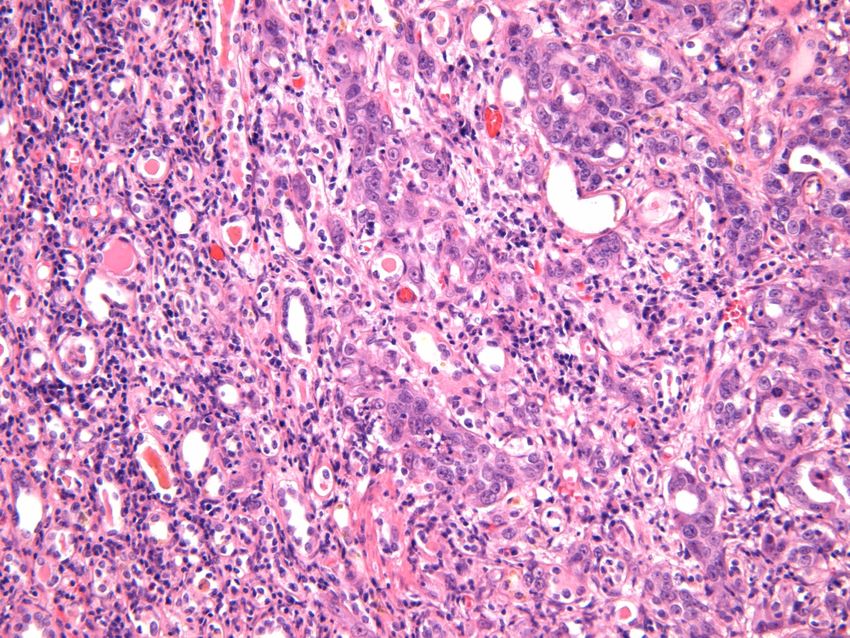
Imaging examinations are the main methods for CDC diagnosis The tumors are hypo-vascular with ill-defined border Pose invasions to the renal cortex and renal sinus
CT is able to detect the invasions of tumors into pelvis and renal cortex Calcification and hemorrhage can also be seen in some cases Mild to moderate uneven delayed enhancement can be detected in dynamic contrast-enhanced scan MRI gives iso-intensity or hyper-intensity
CDC doesn’t have specific imaging features
that distinguish it from other types of renal cell
carcinoma such as renal medullary carcinoma,
sarcomatoid renal cell carcinoma and renal
pelvis carcinoma
Its diagnosis requires pathological examination
- the gold standard for diagnosis of CDC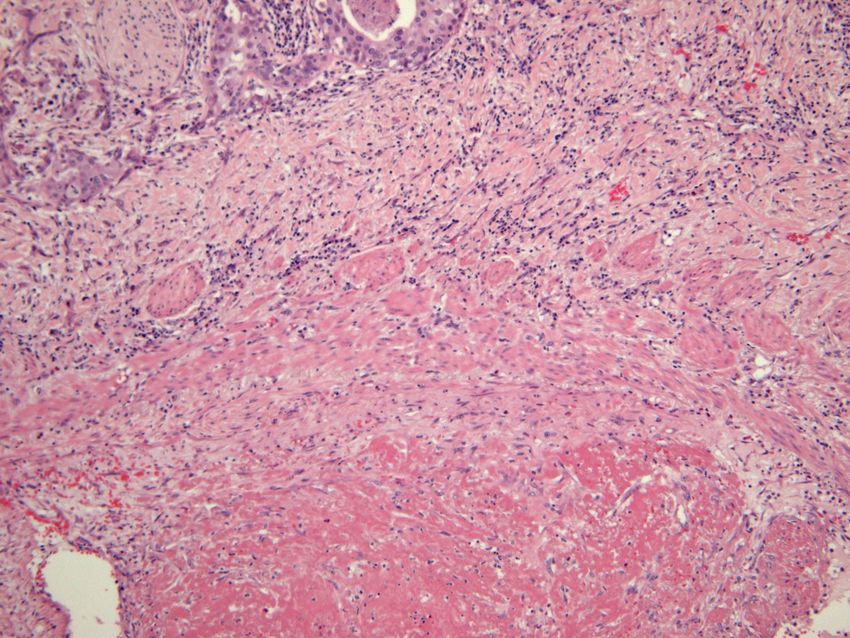
Our case report of CDC
(woman 76 years old)
• 2011 Painless microhematuria
• 2012.04 Abdomen pain, CT: renal upper part tumor 6,5 cm, no
mts
• Performed nephrectomia et lymphonodectomia per
lumbotomiam infiltrate into renal cortex: Ca renis pT3aG3
N0M0 anemia (C64)
• 2012.07 Progresing to liver 4,5 cm mts and lower v. cava 2 cm
l/m, mutiple pulmonary mts 5 mm 3x1cm recidivating tumour in
the same location, aortocavalis l/m 1x1 cm l/m.
• 2012.08 Biological Chemotherapy Sunitinibi: 37,5-12,5 mg 4/2
weeks. After 2 weeks: diarrhea, weakness.
• 2012.04 – 2012.12 (8 month) Ca renis pT3aG3 N0M0 anemia
(C64)Our case report of CDC
• Pathology • Pathology
macroscopic data microscopic data
• Renal upper part tumor • Presents with
tubulopapillary
7x6x2 cm: yellow with
architecture
multiple necrosis zones,
• tumor cells form hobnail
infiltrates portal part,
pattern along the
subcapsular fat glandular tube
• infiltrate into renal cortex,
agressive perineural
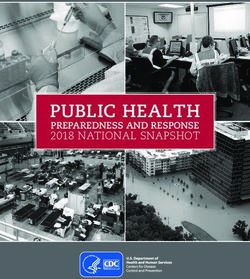
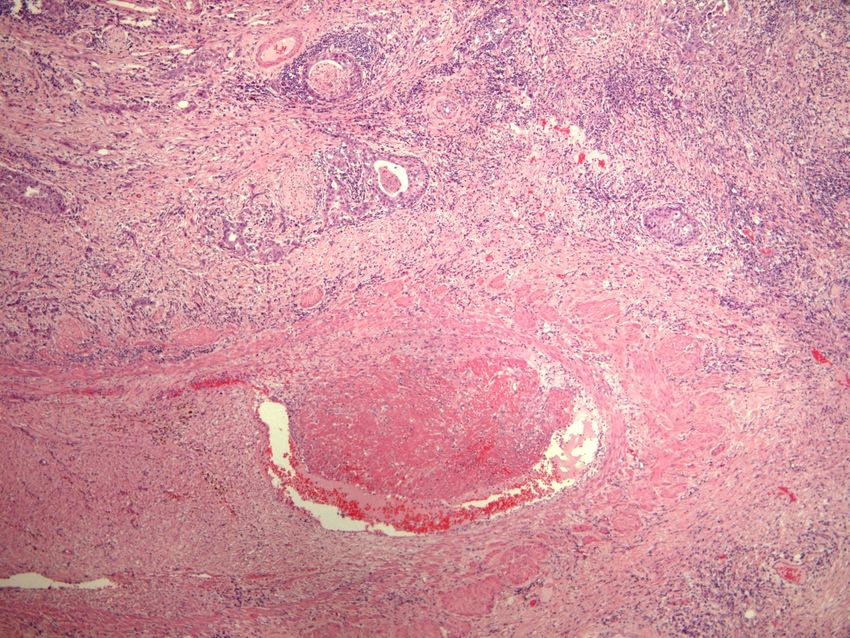
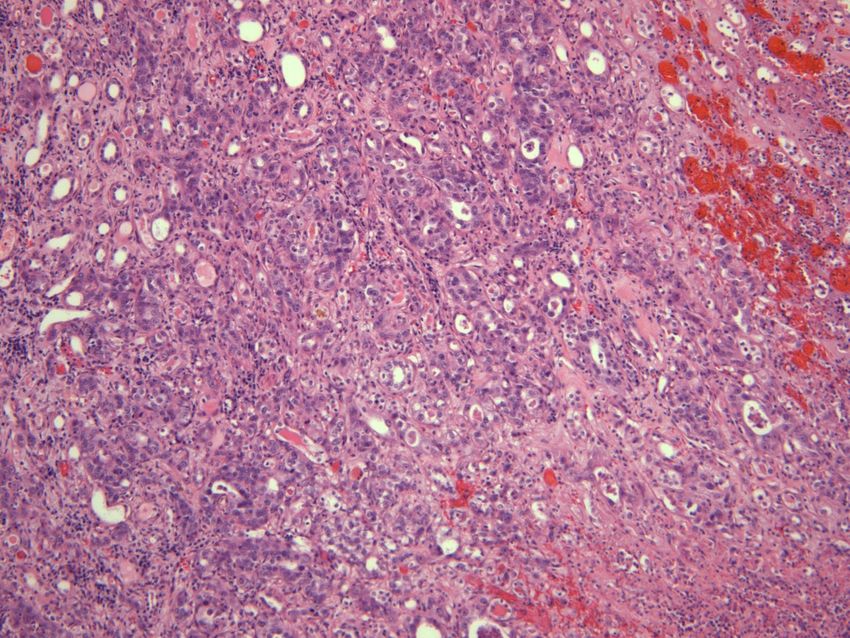
infiltrationTumor cells form tubulopapillary hobnail pattern along the glandular tube
Tumor cells form tubulopapillary hobnail pattern along the glandular tube
CDC morphology • Tubulopapillary architecture with the hobnail-shaped cells protruding into the glandular lumen, and accompanied by interstitial fibrosis and dysplasia of epithelial cells in collecting ducts adjacent to the tumors
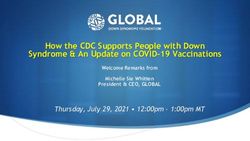
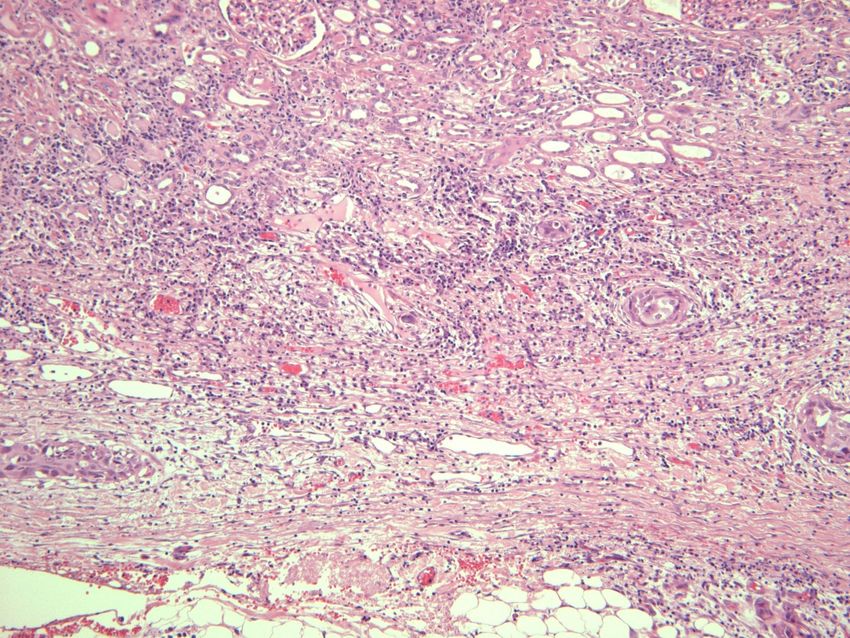
Dysplasia of epithelial cells in collecting ducts adjacent to the tumors
Dysplasia of
epithelial cells
in collecting
ducts
Normal
tubul
Neoplastic
tubular pattern• Poorly differentiated tumor cells show nest-shaped, • rope-like, sarcomatoid • or adenoid cystic morphology, with or without interstitial connective tissue reaction
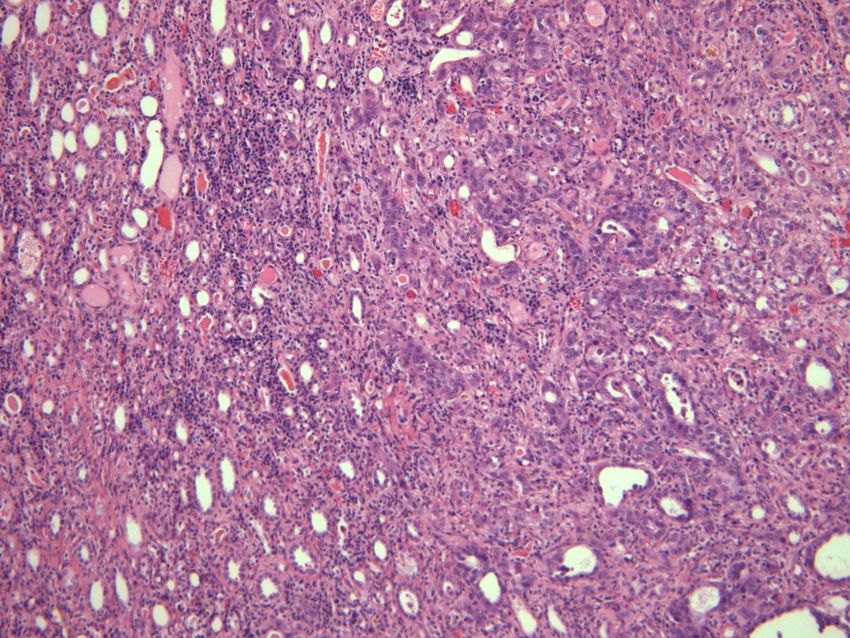
Interstitial fibrosis
Agressive perineural
infiltration
Agressive perineural
infiltrationAgressive perineural
infiltration
Intravascular
trombusInfiltrate into renal cortex, subcapsular fat
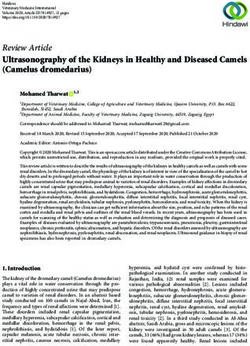
Immunofenotype • Cancer cell have positive expressions of CK (AE1/AE3), CK7, CK19, EMA, vimentin, CK34BE12, PNA and ulex europeus agglutinin (UEA), and negative expression of CD10 and CK20 • Combination of CK34BE12 and PNA is able to detect 90% of CDC • Our case: PANCK CK (AE1/AE3) (+++) 90%, CK7 (+++) 90%, EMA 80%(+++), vimentin (+) 10%, CD10 (+) 30%, CK20 (-), TTF1 (-)
PANCK / CK7 +++ 100%
EMA +++ 100%
CD10 + 30%
VIM ++ 10% EMA +++ 100%
Treatment • Recently, there are a few reports on the effectiveness of targeted therapy with Sunitinib (multiple tyrosine kinase inhibitor) and sorafenib in treatment of CDC • However, there’s a study indicating no response of targeted therapy • Postoperative interferon immunotherapy is recommended
Survival time The postoperative survival time for the cases of stage IV 5 to 6 months for the patients of stage III 9 to 12 months for the case of stage II 18 months
Conclusions • CDC is an unusual variant of renal cell carcinoma and accounts for about 1-2% of all RCC. • CDC doesn’t have specific imaging features. • Pathological examination is the gold standard for diagnosis of CDC. • Radical nephrectomy is the major method to treat CDC. • Treatments and corresponding outcomes are valuable information for guiding future clinical practice, therefore, the efficacy of targeted therapy on CDC remains to be demonstrated.
You can also read