The Skeletal Evaluation and Skeletal Dysplasias - Society for Pediatric Pathology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

4/2/2021
The Skeletal Evaluation and Skeletal Dysplasias
Linda M. Ernst, M.D., M.H.S.
NorthShore University HealthSystem and University of Chicago Pritzker School of Medicine
Perinatal Pathology Course
April 2021
DISCLOSURE
I have no commercial relationships to disclose.
I will not be discussing any unapproved uses of pharmaceuticals or devices
1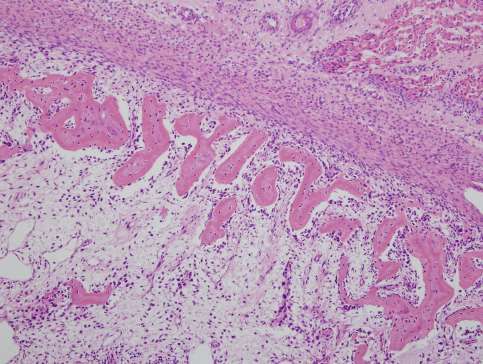
4/2/2021
Objectives
At the conclusion of this lecture, participants will be able to:
• Describe the basic features of skeletal ossification in normal
fetal life.
• Summarize the work-up needed for interpretation of genetic
skeletal dysplasia.
• Compare and contrast the gross, radiologic, and histologic
features of the most common lethal skeletal dysplasias.
• Understand and apply a systematic diagnostic approach to
skeletal dysplasia.
Purpose of radiographs in the perinatal autopsy
• Assessment of fetal maturation
– Ossification centers form in a fairly predictable
pattern over gestation
• Assessment of fetal growth
– Lengths of long bones
• Define skeletal abnormalities
– Skeletal defects as part of a larger syndrome
– Skeletal dysplasia
• Define other soft tissue abnormalities
– Abdominal calcification (meconium peritonitis;
hepatic infections)
– Pneumothorax and other complications
associated with air on xray
2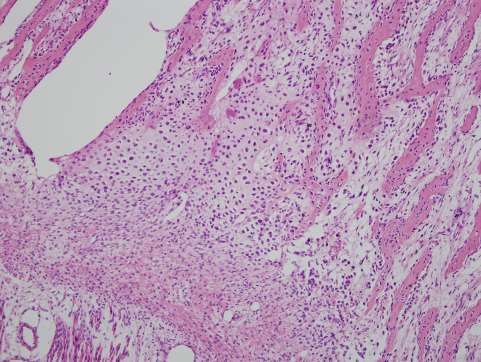
4/2/2021
12% abnormality rate
Did not address its use as a tool for
assessment of fetal maturation
Arthurs OJ, Calder AD, Kiho L, Taylor AM, Sebire NJ. Routine
perinatal and paediatric post-mortem radiography: detection rates
and implications for practice. Pediatr Radiol. 2014 Mar;44(3):252-
7. doi: 10.1007/s00247-013-2804-0. Epub 2013 Nov 8. PMID:
24202433.
From Ernst, Ruchelli, Huff
Color Atlas of Fetal and
Neonatal Histology,
Springer 2011
3
4/2/2021
20 weeks
22 weeks
4
4/2/2021
23 weeks
27 weeks
5
4/2/2021
38 weeks
41 weeks
6
4/2/2021
Skeletal dysplasia
• Bone dysplasias (also known as skeletal dysplasias) are
developmental disorders with their primary phenotypic expression
in the skeletal system
• Characterized by abnormal organization of cells in bone and
cartilaginous tissues.
• Most bone dysplasias are caused by defects in genes that are
expressed in the chondro-osseus tissue.
• The expression of these genes is important in the proper
development and growth of bone and cartilage.
Classification of skeletal dysplasias
• Nosology Classification of Genetic Skeletal Disorders (GSDs)
• A “master list” of skeletal disorders
• Classification based on radiology and genetics
• Identification of a genetic abnormality helps with diagnosis
• Determination of phenotype can guide genetic testing
• 461 disorders placed in 42 groups defined by radiographic, molecular and/or biochemical criteria.
• First publication in 1970 and revised in 1977, 1983, 1992, 1997, 2001, 2006, 2010, 2015, and
2019.
• 2006 215 disorders associated with 140 genes.
• 2010 316 disorders associated with 226 genes.
• 2015 385 disorders associated with 364 genes
• 2019 425 disorders associated with 437 genes
Mortier GR, Cohn DH, Cormier-Daire V, Hall C, Krakow D, Mundlos S, Nishimura G, Robertson S, Sangiorgi L, Savarirayan R, Sillence D, Superti-Furga A, Unger S, Warman ML. Nosology
and classification of genetic skeletal disorders: 2019 revision. Am J Med Genet A. 2019 Dec;179(12):2393-2419. doi: 10.1002/ajmg.a.61366. Epub 2019 Oct 21. PMID: 31633310.
7
4/2/2021
Mortier GR, Cohn DH, Cormier-Daire V, Hall C, Krakow D, Mundlos S, Nishimura G, Robertson S, Sangiorgi L, Savarirayan R, Sillence D, Superti-Furga A, Unger S,
Warman ML. Nosology and classification of genetic skeletal disorders: 2019 revision. Am J Med Genet A. 2019 Dec;179(12):2393-2419. doi: 10.1002/ajmg.a.61366.
Epub 2019 Oct 21. PMID: 31633310.
Classification of Genetic Skeletal Disorders
8
4/2/2021
Inheritance patterns
• Autosomal dominant mutations
– Generally spontaneous mutations with a low recurrence in next
pregnancies.
– In some instances, recurrence can occur due to germ line
mosaicism in the gonad. This feature is well known for
osteogenesis imperfecta and the recurrence risk is
approximately 7 %.
• Autosomal recessive
– Recurrence risk 25%
• Few X-linked disorders
Skeletal dysplasia – A difficult topic
• Fetuses and neonates with bone dysplasias are not commonly
encountered by pathologists.
– The overall frequency among stillbirths and liveborns has
been estimated to be 1 per 4000 to 1 per 6000 births
– Perinatal deaths to be 1 per 110 deaths.
• Approximately, 50 bone dysplasias are lethal and 100 are
recognizable at birth.
– Lethality is usually based on thoracic underdevelopment
and lung hypoplasia.
9
4/2/2021
Uncertainties for pathologists
• Don’t see these cases often.
• Will I recognize the diagnostic features?
– Too many choices to try to picture match.
• How do I deal with fragmented specimens?
• Need a Systematic approach
– Framework to narrow differential diagnosis
Systematic approach
• Clinical findings
• Radiographic findings
Differential dx
• Gross findings
• Histologic findings
Genetic testing
Sometimes a definite diagnosis can not be made even within a group of experts.
104/2/2021
Clinical history
• Family history
• Parental consanguinity
• Prenatal ultrasound features
– Skeletal anomalies
– Other associated anomalies
• Differential diagnosis based on
ultrasound features
• Limitations of ultrasound
– Skull ossification
– Vertebral ossification
– Rib ossification/fractures
– Polydactyly
– Fractures
Gross assessment
• FOR D&E Specimens
• Checklist – Separate out the bony parts from the non-
– Shape of skull/size of fontanelles bony parts
– Lengths of extremities, rhizomelic or
mesomelic shortening. – As best as possible, reconstruct the skeletal
anatomy of the fetus.
– Angulation or curvature of
extremities
• Important to find:
– Curvature of spine – Skull, usually collapsed
– Polydactyly – Extremities,
– Thumbs: hitchhiker thumb » Hands and feet usually present, but not always intact
» Long bones may be fractured by the procedure; find as
– Toes: wide space between first and many fragments as possible
second toe – Vertebral column, as much as possible, usually not
completely intact
– Ribs: size of thorax – Ribs, usually not intact, but usually can be found
– Pelvic bones, if possible
– Scapulae, if possible
114/2/2021
Radiologic assessment
• Usually AP, lateral, and close ups
of hands and feet
• Any additional views directed
toward the differential dx
• Radiography of all the bony parts
for D&E
• Evaluation:
– Radiologist
– Do-it-yourself
Checklist for radiographs
• Skull ossification:
– present and normal
– absent, abnormal
• Vertebral ossification:
– present and normal
– flattened (platyspondyly), irregular (anisospondyly), coronal clefts (on lateral view)
– absent ossification of vertebral bodies
• Ribs:
– normal,
– short, fractures, thinned/thickened
• Long bones (rhizomelic: femur/humerus):
– normal, shortened, bowed, angulated, absent/hypoplastic, fractures, metaphyseal
abnormalities such as bifid, barbell-like enlargement, cupping
• Long bones (mesomelic: radius, ulna, tibia, fibula):
– normal, shortened, tubular, absent/hypoplastic, fractures, metaphyseal abnormalities
such as bifid, barbell-like enlargement, cupping
• Cartilage:
– stippling
124/2/2021
Skull ossification
Absent ossification
Normal
Vertebral ossification
Normal Platyspondyly Absent
134/2/2021
Vertebral ossification
Pear shaped
Normal Coronal clefts
Irregular
Ribs
Normal Multiple fractures Short
144/2/2021
Long bones
Multiple fractures
Bifid metaphysis
Curved / bowed
Long bones
Metaphyseal cupping
Barbell metaphyses
Hunt et al. Am. J. Med. Genet. 75:
326–329, 1998
Rhizomelic shortening
Stippling – often mistaken for fractures
154/2/2021
Histologic assessment
• Sample long bones
– Abnormal bones
– Normal bones for comparison
– Be sure to include ends of bone to
evaluate endochondral ossification
• Sample of ribs, usually processed
longitudinally, include costochondral
junction
• Sample of vertebrae
• Other bones as necessary
Histologic assessment: Checklist
• Fractures:
– present/absent
• Physis:
– normal
– poorly mineralized osteoid
– decreased cartilage at physis
– fibrous bands at periphery of physis
– spindled chondrocytes surrounded by fibrous septa
– enlarged chondrocyte lacunae
– Irregular organization of chondrocytes columns
– calcified cartilage canals
– spherical chondrocytes
– PAS+ chondrocyte inclusions
– perichondral collagen rings
– central fibrosis
– giant cell chondrocytes
– mucoid material in resting cartilage
• Cortex:
– deficient ossification
– thickened bone
• Metaphysis/Diaphysis:
– deficient ossification
164/2/2021
Histology
PAS-D inclusions
Cartilage expansion in
primary spongiosa
Giant cell chondrocytes Cystic changes in cartilage Pericellular collagen
SYSTEMATIC APPROACH
Take all the data you collected from thorough
examination
Employ an algorithm
174/2/2021
Nikkels PG. Diagnostic approach to congenital osteochondrodysplasias at autopsy. Diagnostic Histopathology; 15(9):
413-458.
Severe spondylodysplastic dysplasias Osteogenesis imperfecta IIA
Achondrogenesis 1A (fractures in long bones and ribs)
Schneckenbecken dysplasia
Opsismodysplasia
Skull Abnormal ossification (hypercellular bony trabeculae)
Hypophosphatasia
Fibrochondrogenesis (irregular metaphysis, absent (part of)other
Torrance
Thanatophoric dysplasia
Cervical Absent ossification
bones) (chondroid matrix in trabeculae)
Hypochondrogenesis
type 1 and 2
SADDAN dysplasia vertebrae (absent pubic bone, short long bones)
(vessels with perivascular fibrosis in cartilage)
(short ribs, bowing of femora,
(type 2 straight femur), platyspondylia
short long bones) Thoracic Achondrogenesis II
(short long bones with cupping, short ribs, absent
(irregular growth zone with fibrosis)
Dyssegmental dysplasia
and Absent ossification sacrum)
(vessels with perivascular fibrosis in cartilage)
(short ribs, short, wide and
angulated long bones) lumbar Achondrogenesis IB
irregular (short ribs, very short tubular bones without cupping)
vertebrae (cystic changes in resting cartilage)
Osteogensis imperfecta IIA Ciliopathies with major skeletal involvement
fractures
Ribs short (other congenital anomalies from heart, kidney and or liver)
(short long bones)
Campomelic dysplasia
(small scapulae)
Boomerang dysplasia
and many other skeletal
dysplasias
bowed
Humerus Absent
hypoplastic
(short, bowed limbs)
(absent ossification and giant multinuclear
or femur chondrocytes)
Kyphomelic dysplasia angulated fractures Osteogenesis imperfecta type IIB, C
(multiple fractures in long bones and
some in ribs, normal ossification of
Atelosteogensis II/ Short, tubular Mesomelic skull)
(hypercellular bony trabeculae)
de la Chapelle dysplasia
(cystic changes in resting cartilage) bones Absent/hypoplastic Atelosteogensis I
(distal hypoplasia of femur,
Stippled coronal clefts of vertebrae)
atelosteogenesis III
Chondrodysplasia punctata group cartilage Nikkels PG. 2009 Diagnostic
Histopathology; 15(9): 413-458.
184/2/2021
Weisman PS, Kashireddy PV, Ernst LM. Pathologic diagnosis of achondrogenesis type 2 in a fragmented fetus: case report and evidence-based
differential diagnostic approach in the early midtrimester. Pediatr Dev Pathol. 2014 Jan-Feb;17(1):10-20.
Framework/Pattern recognition
Extremely short femora and humeri +
1. Severe underossification of most or all of the skeleton ---------------------- Lethal hypophosphatasia
2. Strikingly well-ossified overall skeleton---------------------------------------- Blomstrand dysplasia
3. Striking trilobed skull------------------------------------------------------------- TD, type 2 with clover leaf skull
4. Marked anisospondyly of the vertebral bodies -------------------------------- Dyssegmental dysplasia
5. Appearance of fractures in long bones ----------------------------------------- OI, Greenberg dysplasia
6. Missing or poorly ossified bones ----------------------------------------------- Atelosteogenesis type 1/Boomerang
dysplasia, Lethal hypophosphatasia
7. Bifid distal humerus --------------------------------------------------------------- Atelosteogenesis type 2
8. Marked femoral bowing----------------------------------------------------------- TD, type 1
9. Huge barbell-like metaphyses---------------------------------------------------- Fibrochondrogenesis
10. Metaphyseal cupping-------------------------------------------------------------- Achondrogenesis, type 2
11. None of the above------------------------------------------------------------------ Hypochondrogenesis, Torrance dysplasia,
TD, type 2, Schneckenbecken,
Achrondrogenesis 1a, 1b
12. Polydactyly ----------------------------------------------------------------------- Short rib polydactyly syndromes
13. Hitchhiker thumb and/or widely spaced 1st and second toe ------------------ Atelosteogenesis type 2
194/2/2021
Weisman PS, Kashireddy PV, Ernst LM. Pathologic diagnosis of achondrogenesis type 2 in a fragmented fetus: case report and evidence-based
differential diagnostic approach in the early midtrimester. Pediatr Dev Pathol. 2014 Jan-Feb;17(1):10-20.
Weisman PS, Kashireddy
PV, Ernst LM. Pathologic
diagnosis of
achondrogenesis type 2
in a fragmented fetus:
case report and
evidence-based
differential diagnostic
approach in the early
midtrimester. Pediatr Dev
Pathol. 2014 Jan-
Feb;17(1):10-20.
204/2/2021
Case examples
Case 1
18 week fetus
No pertinent family history
Clinical dx of skeletal dysplasia
Ultrasound differential dx:
Thanatophoric dysplasia
Achondroplasia
Gross features:
Collapsed skull
Extremely short extremities
Curvature to extremities
214/2/2021
Gross features:
Extremely short extremities
Curvature to extremities
No polydactyly or thumb abnormalities
Gross features:
Beaded ribs
Fairly normal appearing vertebral column
224/2/2021
Skull:
Collapsed, but no obvious ossification
Long bones:
Short
Bent
Possible factures:
Crumpled
Horizontal markings
Vertebral bodies:
OK
Ribs:
Possible fractures
Pelvic bones:
?
234/2/2021
LONG BONE
244/2/2021
254/2/2021
High likelihood of osteogenesis imperfecta
Nikkels PG. Diagnostic
Histopathology; 15(9): 413-458.
264/2/2021
Diagnosis
• Osteogenesis imperfecta, type 2A.
• Genetic testing suggested.
– Mutation in COL1A1
• COL1A1 (17q) or COL1A2 (7q) mutations
– Disrupt the triple helix assembly of pro-α1 and
pro-α2 chains.
– Leads to reduction in amount of functionally
adequate collagen 1 for bone and other
connective tissue
– Heterogeneous mutations
– 2A Usually de novo mutations, but AR inheritance
has been reported in 10% of OI 2B and 3 cases.
Osteogenesis imperfecta, Type 2A
• Classic features:
– Severe retardation of calvarial bone formation
– Generalized osteoporosis with multiple
fractures/callus formation
– Short ribs with continuous beading
– Thick, short, crumpled shafts of long bones
– Rectangular femora with wavy, acordion-like
appearance
274/2/2021
Appearance of fractures in long bones
• Differential diagnosis:
– Osteogenesis imperfecta, type 2A
» True fractures of long bones AND ribs
– “crumpled” long bones
– “beaded” ribs
» Deficient skull ossification
– Lethal hypophosphatasia
» Severe underossification of most or all of the skeleton
» Usually no fractures
– Greenberg dysplasia
» “Pseudofractures” due to presence of abnormal calcification
» Chondrodysplasia punctata group
– Osteogenesis imperfecta, type 2B
» Long bone fractures
» No/fewer rib fractures
» Skull well ossified
» 10% autosomal recessive
– Osteogenesis imperfecta, type 4
» Better calvarial ossification
» Fewer fractures Lethal hypophosphatasia
Normal OI 2A OI 2B / 3
23 weeks 23 weeks 23 weeks
284/2/2021
Case examples
Case 2
Case #2:
20 week fetus
No pertinent family history
Clinical suspicion of skeletal dysplasia
Gross features:
Collapsed skull
Extremely short
extremities
Curvature to
extremities
294/2/2021
Skull:
Collapsed, but with ossification
Long bones:
Short
Curved femora and humeri
No obvious fractures
Vertebral bodies:
Platyspondyly
Ribs:
Very disrupted
Pelvic bones:
Ilia and ischia present
304/2/2021
Skull:
Collapsed, but with ossification
Long bones:
Short
Curved femora and humeri
No obvious fractures
Vertebral bodies:
Platyspondyly
Ribs:
Very disrupted
Pelvic bones:
Ilia and ischia present
Horizontally oriented
band of fibrosis at
periphery of physis
314/2/2021
Nikkels PG. Diagnostic
Histopathology; 15(9): 413-458.
Thanatophoric dysplasia
• Most common lethal osteochondrodysplasia
• Ultrasound:
– Short limbs and a narrow thorax
– Polyhydramnios is frequently present.
• Classic features:
– Very short extremities,
– A relatively normal trunk length, and a narrow
thorax.
– Craniofacial features:
» Disproportionately large head
» Depressed nasal bridge
» Prominent forehead and protruding eyes.
» Craniosynostosis may be present.
– Brain abnormalities:
» polymicrogyria, neuronal heterotopias,
megalencephaly, hippocampal
malformation, cerebellar hypoplasia.
• Genetics:
– Autosomal dominant, FGFR3 mutation
324/2/2021
Pathologic dx:
Thanatophoric dysplasia,
type 1
Genetics:
FGFR3 mutation
Thanatophoric Dysplasia - Radiography
• Flattening of the vertebral bodies
• Short ribs
• Short and broad long bones with bowing
in type 1 TD.
– straight in type 2 TD.
• Other features:
– Small facial bones
– relatively large calvaria
– cloverleaf skull (type 2 > type 1)
– small deformed scapulae
– short metacarpal and metatarsal bones
– bullet-shaped phalanges
– central defects in the vertebral bodies
– decreased vertical diameter and horizontal
inferior margins of the iliac bones
– short and broad pubic and ischial bones.
334/2/2021
FGFR3 group
Achondroplasia
SADDAN dysplasia
Thanatophoric dysplasia II
Thanatophoric dysplasia I
Cloverleaf skull
344/2/2021
Temporal lobe abnormality
Thanatophoric dysplasia type 2
with cloverleafskull
Thanatophoric dysplasia type 1
TD-differential dx
• Achrondroplasia with similar changes to TD,
but usually less severe than TD.
– Vertebral bodies not as flat
– Long bones not as short and don’t have flared
ends
• Platyspondylic dysplasia, Torrence type
– No cranial changes
– Platyspondyly
– Ragged femoral metaphyses
– COL2 disorder
• Severe achondroplasia with developmental
delay and acanthosis nigricans (SADDAN).
– Bowed femora
– Tibia bowed in opposite direction
– Compatible with life beyond neonatal period
Torrance dysplasia
354/2/2021
Case examples
Case 3
Case #3:
15 week fetus
No pertinent family
history
U/S: lower limb
deformity
Gross features:
Collapsed skull
Extremely short
extremities
364/2/2021
Skull:
Collapsed, but some
ossification noted
Long bones:
Short
Metaphyseal cupping
Vertebral bodies:
Not ossified
Ribs:
Disrupted
No obvious fractures
Pelvic bones:
Disrupted
374/2/2021
384/2/2021
Diagnosis
• Achondrogenesis type 2
(Langer-Saldino) suggested
based on morphology and
histology
• Further testing demonstrated
COL2A1 mutation
Nikkels PG.
Diagnostic
Histopathology;
15(9): 413-458.
394/2/2021
Achondrogenesis type 2
• Key features:
– Markedly shortened extremities (micromelia)
with metaphyseal flaring and cupping.
– Vertebral bodies also show absent or severely
reduced ossification.
– Absent ossification in the sacrum and absent or
delayed ossification of pelvic bones.
– Pysisis severely disorganized and
underdeveloped.
» Prominent blood vessels may be seen in the
resting cartilage with perivascular fibrosis.
19 weeks GA
Achondrogenesis type 2
• Genetics:
– Mutations in type 2 collagen
» essential for hyaline cartilage
formation and endochondral
ossification
– Mutations in COL2A1 disrupt
formation of type 2 collagen and
lead to abnormal intracellular
retention of the defective protein
– Mutations are autosomal dominant
with most occurring as denovo https://www.orthobullets.com/basic-science/9013/collagen
mutations
404/2/2021
Achondrogenesis Type 2 – Diff dx
• Hypochondrogenesis
» long bones are short but not as
short and cupping not present.
» PAS-D+ inclusions
• Spondyloepiphyseal dysplasia
congenita (SEDC).
» PAS-D+ inclusions
• Achondrogenesis 1A
» Ribs are thinner and may be
fractured
• Achondrogenesis 1B
» Long bones lose their longitudinal
orientation.
SEDC
Hypochondrogenesis
Hypochondrogenesis and spondyloepiphyseal dysplasia congenita
Nikkels PJ, Diagnostic Histopathology 15:9
414/2/2021
Conclusion
• Most lethal genetic skeletal
dypslasias have detectable, Clinical findings
Radiographic findings
diagnostic features by the early Gross findings
Differential dx
midtrimester. Histologic findings
• A careful, systematic approach to
the examination of the fragmented
fetus with skeletal dysplasia is
best, and we hope our approach Genetic testing
will benefit pathologists who are
faced with these complex and
challenging specimens.
Extremely short femora and humeri +
1. Severe underossification of most or all of the skeleton Lethal hypophosphatasia
2. Strikingly well-ossified overall skeleton Blomstrand dysplasia
3. Striking trilobed skull TD, type 2 with clover leaf skull
4. Marked anisospondyly of the vertebral bodies Dyssegmental dysplasia
5. Appearance of fractures in long bones OI, Greenberg dysplasia
6. Missing or poorly ossified bones Atelosteogenesis type 1/Boomerang
dysplasia, Lethal hypophosphatasia
7. Bifid distal humerus Atelosteogenesis type 2
8. Marked femoral bowing TD, type 1
9. Huge barbell-like metaphyses Fibrochondrogenesis
10. Metaphyseal cupping Achondrogenesis, type 2
11. None of the above Hypochondrogenesis, Torrance
dysplasia, TD, type 2,
Schneckenbecken, Achrondrogenesis
1a, 1b
12. Polydactyly Short rib polydactyly syndromes
13. Hitchhiker thumb and/or widely spaced 1st and second toe Atelosteogenesis type 2
Nikkels PG. Diagnostic
Histopathology; 15(9): 413-458.
424/2/2021
Final case - Bony abnormalities with Placental Pathology
• 21 weeks 1 day gestational age male fetus
• Mother 31-year-old G2P1101 female was admitted for termination
of the pregnancy due to the recent diagnosis of anhydramnios and
severe intrauterine growth restriction on routine check-up.
• On ultrasound imaging:
– Severe symmetric intrauterine growth restriction.
– Two kidneys were identified but a bladder was not visualized.
Massive
Perivillous Fibrin
Deposition
Renal Tubular
dysgenesis
434/2/2021
Relationship between MPVFD, RTD, and Bone Mineralization
• Radiographs show demineralized
bones with lucency and dense lines
of ossification at the metaphyseal
ends
• Potential for postmortem fractures
• Potential mechanisms:
– Abnormal placental vitD
metabolism
– Secondary hypoparathyroidism
secondary to renal abnormality
Abdulghani S, Moretti F, Nikkels PG, Khung-Savatovsky S, Hurteau-Miller J, Grynspan D.
Growth Restriction, Osteopenia, Placental Massive Perivillous Fibrin Deposition With (or
Without) Intervillous Histiocytes and Renal Tubular Dysgenesis-An Emerging Complex.
Pediatr Dev Pathol. 2018 Jan-Feb;21(1):91-94. doi: 10.1177/1093526617697061. Epub 2017
Mar 15. PMID: 29187034.
444/2/2021
ACKNOWLEDGEMENTS
• Dr Peter Nikkels
• Andrew Poznanski
• Paul Weisman
QUESTIONS
454/2/2021
References
Mortier GR, Cohn DH, Cormier-Daire V, Hall C, Krakow D, Mundlos S, Nishimura G, Robertson S, Sangiorgi L, Savarirayan R, Sillence D,
Superti-Furga A, Unger S, Warman ML. Nosology and classification of genetic skeletal disorders: 2019 revision. Am J Med Genet A. 2019
Dec;179(12):2393-2419. doi: 10.1002/ajmg.a.61366. Epub 2019 Oct 21. PMID: 31633310.
Bonafe L, Cormier-Daire V, Hall C, Lachman R, Mortier G, Mundlos S, Nishimura G, Sangiorgi L, Savarirayan R, Sillence D, Spranger J,
Superti-Furga A, Warman M, Unger S. Nosology and classification of genetic skeletal disorders: 2015 revision. Am J Med Genet A. 2015
Dec;167A(12):2869-92.
Weisman PS, Kashireddy PV, Ernst LM. Pathologic diagnosis of achondrogenesis type 2 in a fragmented fetus: case report and evidence-
based differential diagnostic approach in the early midtrimester. Pediatr Dev Pathol. 2014 Jan-Feb;17(1):10-20.
Nikkels PG. Diagnostic approach to congenital osteochondrodysplasias at autopsy. Diagnostic Histopathology; 15(9): 413-458.
Warman ML et. al. Nosology and classification of genetic skeletal disorders: 2010 revision. 2011 Am J Med Genet A; 155A (5): 943-968.
Kornak U, Mundlos S. Genetic disorders of the skeleton: a developmental approach. Am J Hum Genet. 2003 Sep;73(3):447-74. Epub 2003
Jul 31.
Olsen ØE, Lie RT, Lachman RS, Maartmann-Moe H, Rosendahl K. Ossification sequence in infants who die during the perinatal period:
population-based references. Radiology. 2002 Oct;225(1):240-4.
Superti-Furga A, Bonafé L, Rimoin DL. Molecular-pathogenetic classification of genetic disorders of the skeleton. Am J Med Genet. 2001
Winter;106(4):282-93.
References
Spranger JW, Brill PW, Poznanski A, Bone Dysplasias: an atlas of genetic disorders of skeletal development, 2 nd ed,
Oxford, New York, 2002.
Spranger, JW. Brill PW, Nishimura G, Superti-Furga A, Unger S. Bone Dysplasias: an atlas of genetic disorders of
skeletal development, 3RD ed, Oxford, New York, 2012.
Lachman RS, Taybi and Lachman’s radiology of syndromes, metabolic disorders and skeletal dysplasias, Mosby,
Philadelphia, 2007.
Gilbert-Barness E, Osteochondrodysplasia-constitutional diseases of bone, in Potter’s pathology of the fetus, infant,
and child, Ed. Gilbert-Barness E, 2nd edition, Philadephia: Mosby, p1836-1897.
Khong TY, Malcomson RDG, Keeling’s fetal and neonatal pathology, Fifth edition, 2017, Springer.
Abdulghani S, Moretti F, Nikkels PG, Khung-Savatovsky S, Hurteau-Miller J, Grynspan D. Growth Restriction,
Osteopenia, Placental Massive Perivillous Fibrin Deposition With (or Without) Intervillous Histiocytes and Renal
Tubular Dysgenesis-An Emerging Complex. Pediatr Dev Pathol. 2018 Jan-Feb;21(1):91-94. doi:
10.1177/1093526617697061. Epub 2017 Mar 15. PMID: 29187034.
46You can also read