Abduction Contractures within Infants with Developmental Dysplasia of the Hip
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Dissertations and Theses 4-2020 Abduction Contractures within Infants with Developmental Dysplasia of the Hip Nathan Stanton Follow this and additional works at: https://commons.erau.edu/edt Part of the Orthotics and Prosthetics Commons This Thesis - Open Access is brought to you for free and open access by Scholarly Commons. It has been accepted for inclusion in Dissertations and Theses by an authorized administrator of Scholarly Commons. For more information, please contact commons@erau.edu.
ABDUCTION CONTRACTURES WITHIN INFANTS WITH DEVELOPMENTAL DYSPLASIA OF THE HIP by Nathan Stanton A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science of Mechanical Engineering at Embry-Riddle Aeronautical University Embry-Riddle Aeronautical University Daytona Beach, Florida April 2020 i
04/23/2020
Acknowledgements My sincere gratitude goes to Dr. Victor Huayamave for the support and guidance as well as keeping me focused. I would not be where I am at today without your mentorship and belief. My family, as always, has been instrumental in pushing me forward and helped me believe that even the most monumental tasks could be accomplished. I am also very grateful for all of the help and direction I received from my girlfriend, who helped me achieve so many breakthroughs within the study. Finally, I would like to thank my Master’s Family and the BioLab for their support and for dealing with my insanity. ii
Abstract Researcher: Nathan Taylor Stanton Title: Abduction Contractures within Infants with Developmental Dysplasia of the Hip Institution: Embry-Riddle Aeronautical University Degree: Master of Science in Mechanical Engineering Year: 2020 Developmental Dysplasia of the hip is a condition that affects 1 to 3 of every 1000 infants born globally. It is a pathology that involves the instability, subluxation, or dislocation of the femoral head from the acetabulum. Through a rating system by the International Hip Dysplasia Institute or Graf System, hips are rated based on their level of instability or dislocation and the infant is then prescribed a treatment. While Finite element models of dysplastic hips have been developed previously, a study that seeks to understand the contribution of an abduction contracture of the hip has yet to be performed. This assessment and evaluation could impact the way future models are made and could provide guidelines for what muscles are taken into account during modeling. Therefore, through the evaluation and comparison of three models with varying levels of abduction contracture, conclusions can be drawn as to the importance of various muscles and their contribution to developmental dysplasia. These models were developed from a set of CT scans and then used current musculature and skeletal properties in order to properly construct the hip joint. Comparisons between the stresses in each of the models are then made between the hip joints as well as between simulated values and currently available experimental values. The models then show, through engineering stress distributions and concentrations, how detrimental an abduction contracture can be to an infant and that if the condition is prolonged there is a possibility of development of dysplasia or, at minimum, a malformation of the acetabulum. iii
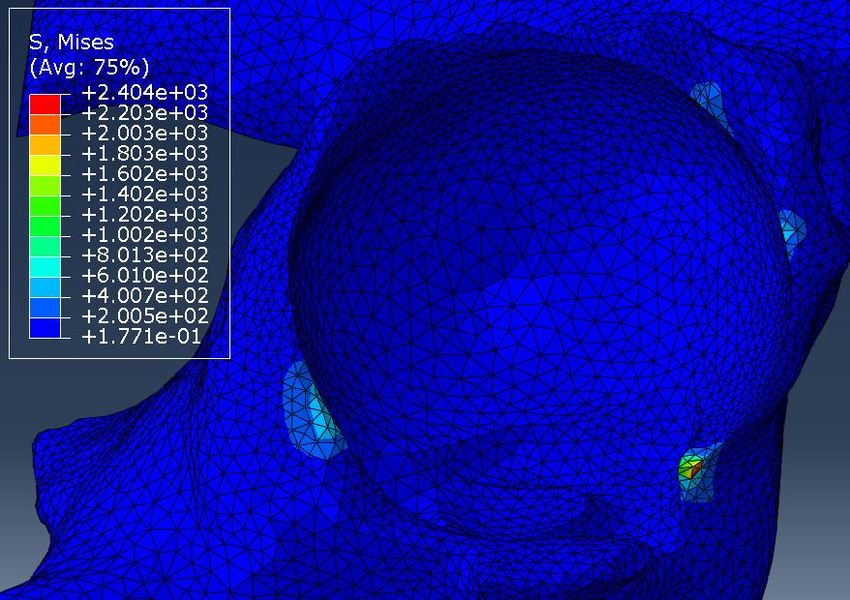
Table of Contents Thesis Review Committee .............................................................................. Error! Bookmark not defined. Acknowledgements ...................................................................................................................................... ii Abstract ....................................................................................................................................................... iii Chapter 1 ...................................................................................................................................................... 1 Introduction:............................................................................................................................................. 1 Treatment and Prevention of Developmental Dysplasia of the Hip .................................................. 4 Abduction Contractures within the Hip............................................................................................... 7 Computational Models and Evaluations ............................................................................................. 7 Chapter 2 .................................................................................................................................................... 10 Literature Review ................................................................................................................................... 10 Diagnosing DDH .................................................................................................................................. 11 Imaging for Diagnosis ......................................................................................................................... 13 DDH Treatments ................................................................................................................................. 16 Abduction Contractures ..................................................................................................................... 19 Gluteus Medius .................................................................................................................................. 20 Gluteus Minimus ................................................................................................................................ 21 Prevention of DDH.............................................................................................................................. 22 Modeling DDH .................................................................................................................................... 25 Chapter 3 .................................................................................................................................................... 30 Methods: ................................................................................................................................................ 30 Padua Specimens and Muscle Choice ................................................................................................ 31 Scans and Segmenting........................................................................................................................ 32 Assembly............................................................................................................................................. 33 Meshing .............................................................................................................................................. 34 Material Properties ............................................................................................................................ 35 Boundary Conditions .......................................................................................................................... 39 New Zero................................................................................................ Error! Bookmark not defined. Finite Element Analysis Loading Conditions and Steps..................................................................... 41 Chapter 4 .................................................................................................................................................... 43 Results..................................................................................................................................................... 43 Specimen 387 Left Hip – Grade A .......................................................................................................... 43 Specimen 387 Right Hip – Grade B ........................................................................................................ 48 iv
Specimen 30 Right Hip – Grade C........................................................................................................... 52 Chapter 5 .................................................................................................................................................... 57 Discussion ............................................................................................................................................... 57 Conclusion .............................................................................................................................................. 63 References: ................................................................................................................................................. 65 v
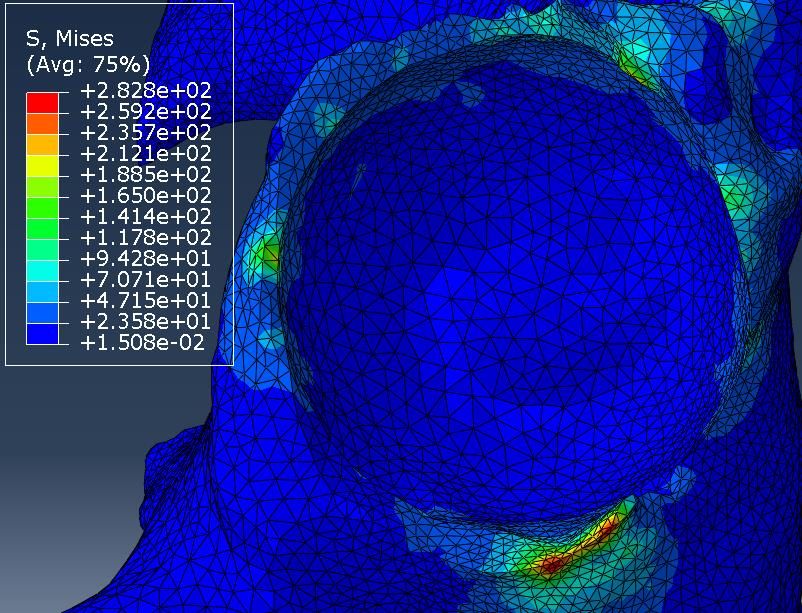
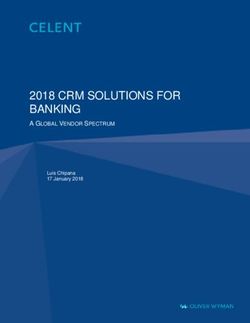
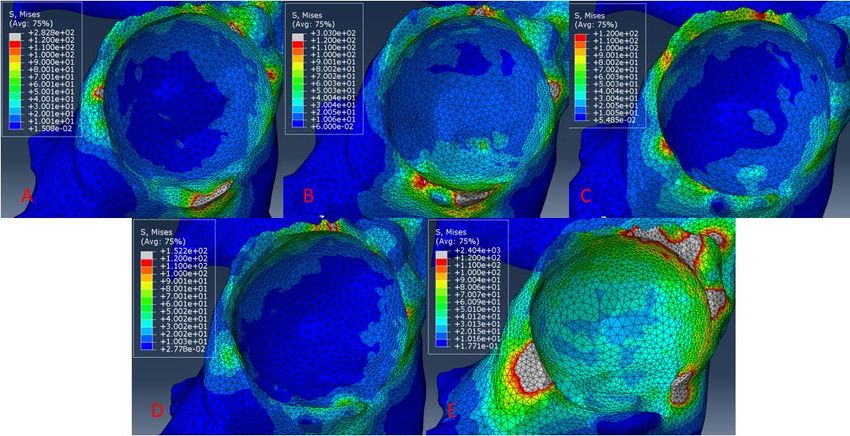
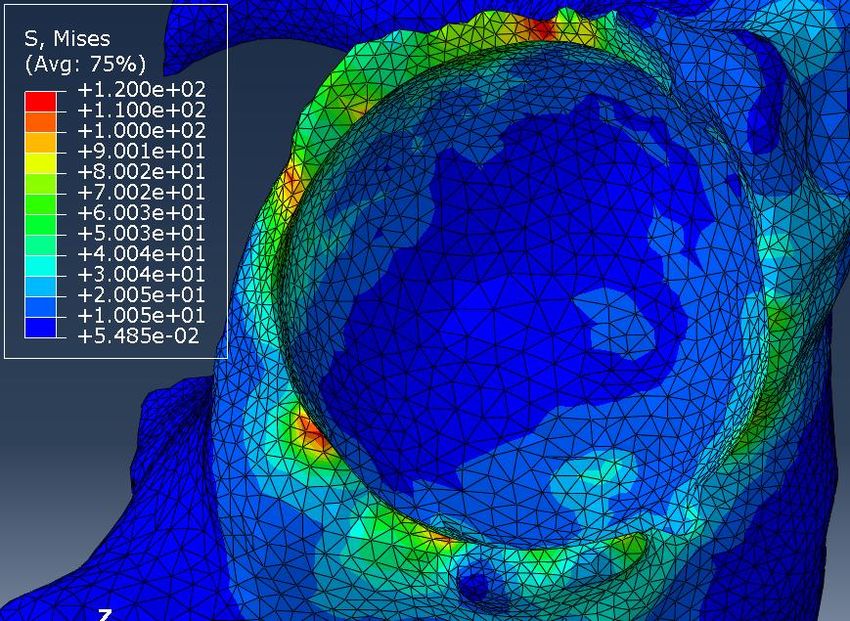
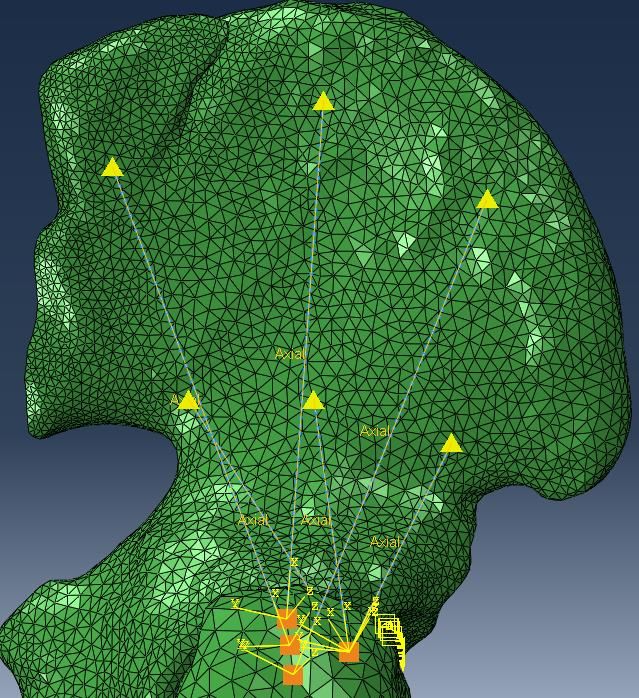
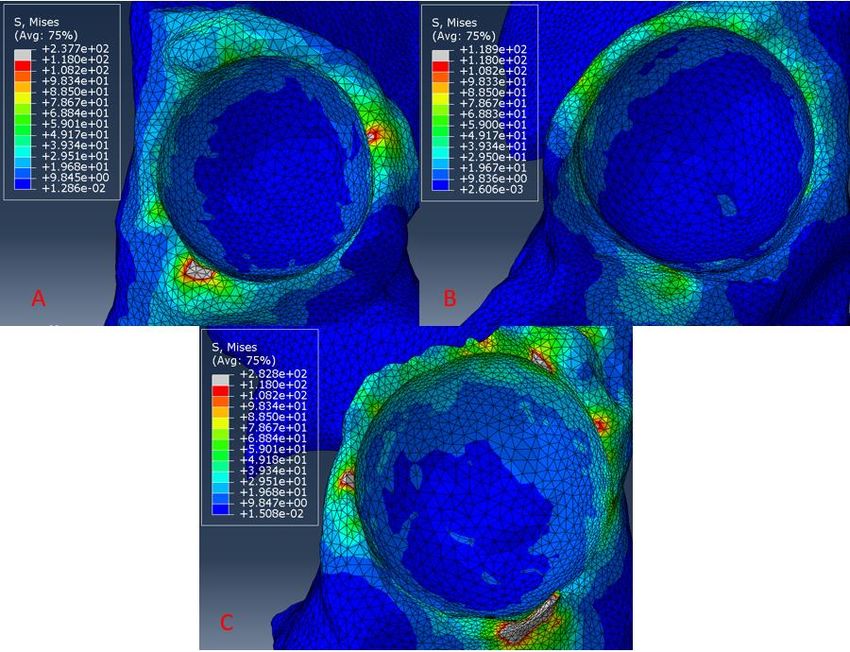
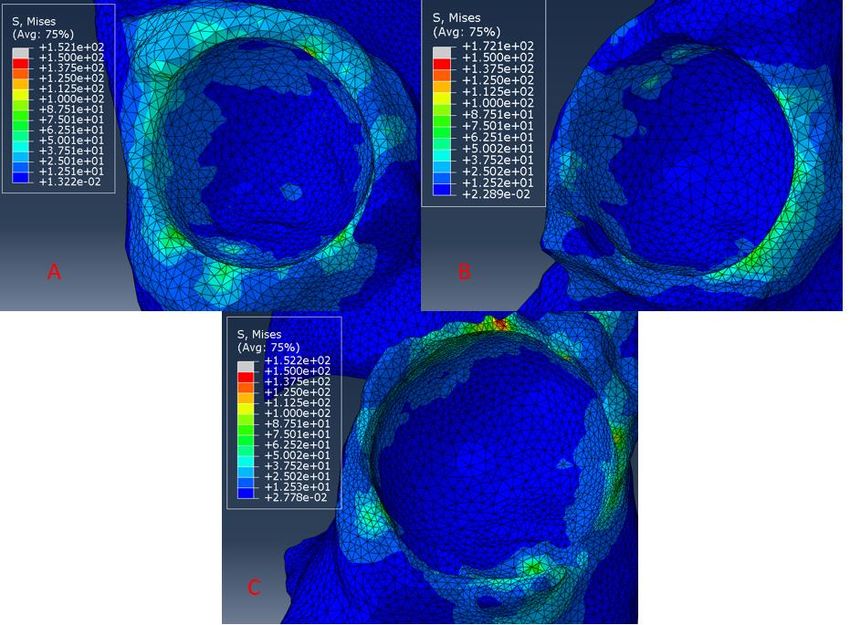
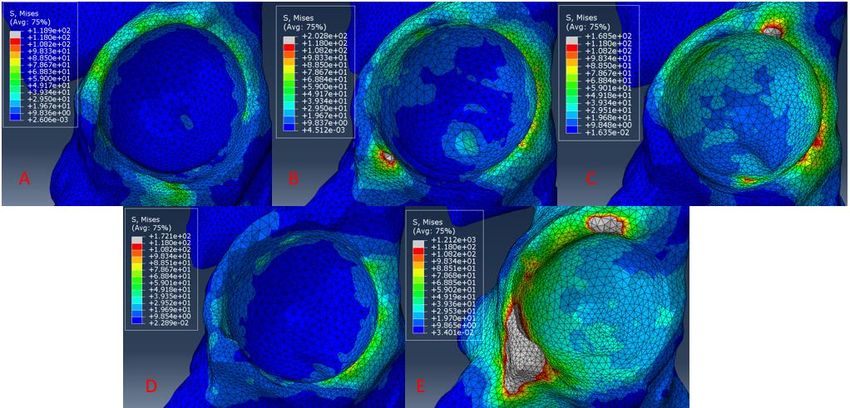
Table of Figures Figure 1: The hip joint as rendered by (Anderson, Ellis, Maas, Peters, & Weiss, 2008) ........................................... 1 Figure 2: Example of Graf Rating System for Hip Dysplasia where Type 1 is normal, Type 2 is mildly dysplastic, Type 3 is subluxated with a shallow acetabulum, and Type 4 where the femoral head is completely dislocated from the acetabulum (French & Dietz, 1999). ............................................................................... 3 Figure 3: Back Carrying example from Malawi (Graham S. et al. 2015). ................................................................. 6 Figure 4: The Ortolani Maneuver (Left) and the Barlow Maneuver (Right) (French & Dietz, 1999). ...................... 12 Figure 5: Ultrasound drawing of a 7 month old infant with the three lines and two angles used in static ultrasound examination (Aronsson et al., 1994). ......................................................................................... 14 Figure 6: Pavlik Harness applied to an infant (Ardila et al., 2013). ....................................................................... 17 Figure 7: Drawing of the Gluteus Medius and Minimus (Gottschalk, Kourosh, & Leveau, 1989) .......................... 21 Figure 8: Gluteus Minimus insertion and origin ................................................................................................... 22 Figure 9: (a) – Nigerian woman carrying her child on her back, (b) – Chinese infant being carried in a sling with the hips observably abducted and flexed, (c) – Northern Canadian Eskimo carrying her infant on her back with the hips in an abducted and flexed position. ....................................................................................... 23 Figure 10: Infant swaddled with the hips extended and adducted on a cradleboard from a Northern Canadian Indian tribe (Salter, 1968). ........................................................................................................................... 24 Figure 11: Specimen 387 Complete Pelvis ............................................................................................................ 32 Figure 12: Specimen 30 Complete Pelvis with Femurs.......................................................................................... 32 Figure 13: Progression of abduction in Specimen 30 ............................................................................................ 33 Figure 14: Meshing Interface for ScanIP ............................................................................................................... 34 Figure 15: Muscle Lines of Action within OpenSim (Delp et al., 2007; Delp et al., 1990) ...................................... 36 Figure 16: Muscle Lines of Action as established within the models and based on OpenSim ............................... 36 Figure 17: Specimen 387 – Right Hip in the anatomical position with musculature and boundary conditions ..... 40 Figure 18: Step Properties for each simulation .................................................................................................... 42 Figure 19: 387L at 15 Degrees of Adduction. Anterior is left of the model. .......................................................... 43 Figure 20: 387L in the anatomical position. Anterior is left of the model. ............................................................ 44 Figure 21: 387L 15 degrees of abduction. Anterior is left of the model. ............................................................... 45 Figure 22: 387L at 30 degrees of abduction. Anterior is left of the model. ........................................................... 46 Figure 23: 387L at 45 degrees of abduction. Anterior is left of the model. ........................................................... 46 Figure 24: Comparison of all 387L stresses. (A) 387L 15 Degrees Adduction, (B) 387L Anatomical Position, (C) 387L 15 Degrees Abduction, (D) 387L 30 Degrees Abduction, (E) 387L 45 Degrees Abduction ............................. 47 Figure 25: 387R with 15 degrees of adduction. Anterior is right of the model. ..................................................... 48 Figure 26: 387R in the Anatomical position. Anterior is right of the model. ......................................................... 49 Figure 27: 387R with 15 Degrees of abduction. Anterior is to the right of the model. .......................................... 49 Figure 28: 387R with 30 Degrees of abduction. Anterior is to the right of the model. .......................................... 50 Figure 29: 387R with 45 degrees of abduction. Anterior is to the right of the model ........................................... 51 Figure 30: Comparison of all 387R stresses. (A) 387R 15 Degrees Adduction, (B) 387R Anatomical Position, (C) 387R 15 Degrees Abduction, (D) 387R 30 Degrees Abduction, (E) 387R 45 Degrees Abduction .................... 52 Figure 31: 30R at 15 degrees of adduction. Anterior is to the right of the model. ................................................ 53 Figure 32: 30R in the anatomical position. Anterior is to the right of the model. ................................................. 53 Figure 33: 30R at 15 degrees of abduction. Anterior is to the right of the model. ................................................ 54 Figure 34: 30R at 30 degrees of abduction. Anterior is to the right of the model. ................................................ 55 Figure 35: 30R at 45 degrees of abduction. Anterior is to the right of the model. ................................................ 55 Figure 36: Comparison of all 30R stresses. (A) 30R 15 Degrees Adduction, (B) 30R Anatomical Position, (C) 30R 15 Degrees Abduction, (D) 30R 30 Degrees Abduction, (E) 30R 45 Degrees Abduction ..................................... 56 Figure 37: Comparison of all 15 Degrees of Adduction stresses: (A) 387L (B) 387R (C) 30R .................................. 58 Figure 38: Comparison of all anatomical position stresses: (A) 387L (B) 387R (C) 30R .......................................... 59 vi
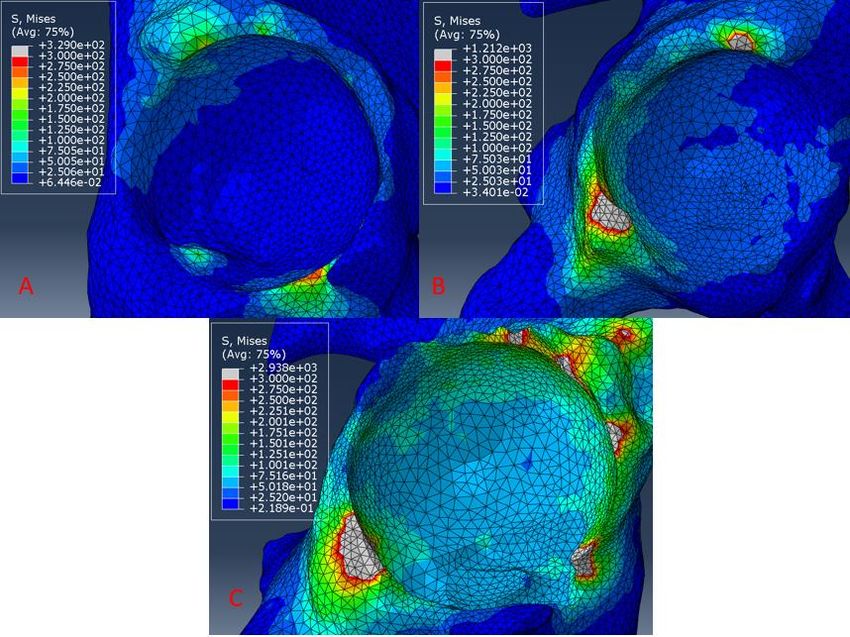
Figure 39: Comparison of all 15 Degrees of Abduction stresses: (A) 387L (B) 387R (C) 30R .................................. 60 Figure 40: Comparison of all 30 Degrees of Abduction stresses: (A) 387L (B) 387R (C) 30R .................................. 61 Figure 41: Comparison of all 45 Degrees of Abduction stresses: (A) 387L (B) 387R (C) 30R .................................. 62 vii
List of Tables Table 1: Scaled Infant PCSA’s based on .036 Ratio (Chang, Rupp, Kikuchi, & Schneider, 2008; Huayamave et al., 2015) ........................................................................................................................................................... 38 Table 2: List of all spring constants used as muscle properties within the models. It is important to note that each of the spring constant values are the same across the specimens due to their reliance on the PCSA .......... 39 viii
Chapter 1 Introduction: Developmental Dysplasia of the hip (DDH) is a pathology that affects 1-3 out of every 1000 children born, depending on geographic location (Ardila et al., 2013; Graham, Manara, Chokotho, & Harrison, 2015; Huayamave et al., 2015; Kotlarsky, Haber, Bialik, & Eidelman, 2015; Zwawi et al., 2017). This pathology is one that “represents a spectrum of disease from transient neonatal hip instability to established dislocation,” (T. C. Clarke C., Judd J., 2016b). Meaning that within the hip joint of the infant there is some instability that can, if left untreated, allow for dislocations of the hip joint as well as long term pathologies such as osteoarthritis. The hip joint itself is composed of the acetabulum and the femoral head as well as surrounding blood vessels and soft tissue. The femoral head is the spherical bony portion of the femur that fits into the acetabulum, also known as the hip socket as seen in Figure 1. Figure 1: The hip joint as rendered by (Anderson, Ellis, Maas, Peters, & Weiss, 2008) The femoral head, as well as the acetabulum, can be malformed or be the reason for the dislocation. The femoral head, without proper movement or in conjunction with other contributing 1
factors, can cause improper morphogenesis of the hip joint and therefore can result in DDH occurring within the infant (Giorgi M., Carriero A., Shefelbine S., Nowlan N., 2015). There are a variety of risk factors associated with DDH. These include being female, the left hip, birthing in the breech position, being a first born, postural deformities, oligohydramnios (a deficiency of amniotic fluid during pregnancy), and a previous family history of hip dysplasia. (Kotlarsky et al., 2015). However, the most important risk factor is being born in the breech position, regardless of a normal birth or cesarean section (Kotlarsky et al., 2015). Being female is also a large contributing factor to the risk of DDH, with 80% of all cases being female (Kotlarsky et al, 2015, Giorgi et al, 2015). This is most likely due to ligamentous laxity as a result of a maternal hormone, relaxin, that circulates through the body during pregnancy (Kotlarsky et al., 2015). However, these are all risk factors that are involved in the prenatal period of the child’s life. It is also possible for the child to develop dysplasia over time due to injury, improper swaddling, improper baby wearing, and a variety of other occurrences during the neonate’s life (Kotlarsky et al, 2015, Graham S., Manara J., Harrison W., 2015). Each case of DDH is rated using a variety of testing methods such as the Barlow and Ortolani Method and often times follow ups for infants with suspected DDH are screened again with Ultrasonographic techniques (Dezateux C., Rosendahl K., 2007). Once these evaluations are performed the hip is then rated according to the Graf or International Hip Dysplasia Institute scale from I-IV. Where 1 is a normal hip and 4 is complete dislocation of the hip (Kotlarsky P., Haber R., Bialik V., Eidelman M., 2015, Huayamave V., Rose C., Serra S., Jones B., Divo E., Moslehy F., Kassab A. Price C., 2015). 2
Figure 2: Example of Graf Rating System for Hip Dysplasia where Type 1 is normal, Type 2 is mildly
dysplastic, Type 3 is subluxated with a shallow acetabulum, and Type 4 where the femoral head is
completely dislocated from the acetabulum (French & Dietz, 1999).
The Graf rating system for dysplastic hips is based on the study done by Graf R. in 1984 where
3500 infants were evaluated via ultrasound due to a suspected instability within the hip. After the
children were evaluated a baseline set of parameters were set up in order to create a consistent
evaluation structure for the hip joint. This resulted in four types of dysplasia (Figure 2) where type one
hips are normal (stable), type two hips are mildly dysplastic (slightly unstable), type three hips are
subluxated with a malformed acetabulum (major instability), and type 4 hips which have a femoral head
that is entirely dislocated from the acetabulum (French & Dietz, 1999; Graf, 1984). These four types
represent the majority of infant hips within Graf’s studies and this rating scale is still used today. There
are however, minor changes to the rating system or other rating systems that by name are different but
are similar in concept to the Graf System. One of the major systems that is similar to the Graf system is
the International Hip Dysplasia Institute which uses a similar 4 type system and rates hips within that
scale ("Developmental Dysplasia of the Hip - International Hip Dysplasia Institute," 2020). This 4-type
rating system is used consistently when seeking to diagnose hip dysplasia in infants and depending on
the type of hip a certain device or procedure is described for treatment. (Huayamave et al., 2015). This
classification and treatment method is extremely important due to the possibility of long-term side
effects of DDH.
3Developmental Dysplasia of the hip is known to cause problems within the adult hip if left untreated. Severe cases often are due to a lack of diagnosis within the childhood of the individual. While these cases are rare, it is possible for a child with DDH to go unnoticed or untreated during the early portions of life. If this occurs there are severe implications for the individual later in life. The most common problems that are seen are a limp, bone deformities, and osteoarthritis (Michaeli D., Murphy S., & Hipp J., 1997). Usually the limp is the first sign of a deformity or problem within the adult or adolescent hip. The individual will compensate for the lack of proper femoral head positioning by favoring one side or the other. However, if the limp is not present severe pain due to early onset osteoarthritis is another likely indicator that there is a problem for the hip joint. Once a problem has been identified by the individual and they seek treatment, it is usually then that the dysplasia is identified and deformities and treatment options discussed (Michaeli, Murphy, & Hipp, 1997). Often times with late identification the femoral head has impounded into the pelvis so much and the head has spent so much time in a specific place outside the acetabulum that a new “socket” has formed (often a Graf IV). After these pathologies have been identified a treatment is enacted to help reduce the hip or change the location of the femoral head within the pelvis. Treatment and Prevention of Developmental Dysplasia of the Hip With the knowledge that cases of hip dysplasia that are left untreated can cause long term side effects in a patient it is important to look at the treatments available to an infant with the pathology. The most common treatment for DDH is a harness that the infant wears in order to attempt to correct DDH during the first few months of life (Singh, 2015; Suzuki, 1994; Wilkinson, Sherlock, & Murray, 2002). The most prevalent of these harnesses is the Pavlik Harness. The Pavlik Harness seeks to eliminate the DDH through the abduction and flexion of the hip (Ardila et al., 2013). The harness uses stirrups and straps that attach around the infant in order to keep the infant’s hips in an abducted and flexed position for an extended period of time so that the acetabulum can properly form. This allows the femoral head 4
to wear into the socket and be properly seated within the acetabulum. Other harnesses such as the Craig Splint, the von Rosen splint, and the Ilfeld abduction orthosis are used to treat DDH but with the high rate of success achieved by the Pavlik harness, around 98%, it is the most common choice for harnesses (Atrey & Katchburian, 2010; Kotlarsky et al., 2015; Ömeroğlu, Köse, & Akceylan, 2016). The harnesses have been known to fail however. In particular, if the classification of the hip is above a Graf III the hip often cannot or will not be reduced through the use of a harness. Therefore, when a harness fails or the infant is too old for the treatment to be effective, surgery is often performed in order to correct the condition. The two types of surgery that are commonly performed are a closed reduction and an open reduction. A closed reduction often is a reduction of the hip without the manipulation of the pelvis or the cutting of any portions of the bone (Zwawi et al., 2017). An open reduction is often an osteotomy, where the pelvis or femur is cut and the acetabulum or femoral head moved to a better position and then reattached using screws and other components. After the surgeries, an infant is often put in a Spica cast in order to keep the hip reduced and allow for the reformation of the acetabulum for proper seating of the femoral head. The cast, unfortunately, does have to be removed and reapplied on a regular basis due to the growth of the child and often requires multiple doses of general anesthesia. In addition to the repeated removal of the cast, it is possible that the child could develop an abduction contracture. This is when the abductor muscles tighten and/or shortened due to the constant abduction the spica cast requires during the healing process. It is then possible that the contraction could contribute to additional incidents of dysplasia. This and the severity of the initial surgery are not ideal and due to the developmental component of the pathology it is important that prevention of DDH be a primary concern. Most importantly, is the recognition that Developmental Dysplasia of the Hip is a developmental disease more often than it is a congenital one. There are risk factors associated with having an ancestry of hip dysplasia as well as some conditions at the time of birth (Dezateux & Rosendahl, 2007; Kotlarsky 5
et al., 2015). However, it is known as a developmental issue due to the fact that there is evidence of hip dysplasia being more related to improper swaddling techniques, improper baby wearing, or leaving a child in a position where the hip has the ability to dislocate or subluxate (Graham et al., 2015). Therefore, it is incredibly important to recognize the environmental factors that play a role in the development of hip dysplasia and through studies such as the one performed by Graham S. et al. 2015 it is seen that the way a child is worn or carried can play a pivotal role in the development of the child’s hip. Figure 3: Back Carrying example from Malawi (Graham S. et al. 2015). This study in addition to others, such as the initiative in Japan to change the swaddling style of children, have granted insight into the development of hip dysplasia as well as brought to light the need 6
for a model to represent a neonate’s hip (Graham et al., 2015; Roper, 1976). With a truly accurate and adaptable model, computational evaluations would become available in order to help determine the viability of treatments and other preventative measures. Abduction Contractures within the Hip An abduction contracture within the hip is when muscles within the hip abductor sub-group experience an increase in the tightening of the muscle fibers or the fibers become shortened within the body due to genetic or environmental factors (Green & Griffin, 1982; Halanski & Noonan, 2008; Proske & Morgan, 2001; Shen, 1975). These contractures are often presented as indentations on the skin, improper gaits, or the inability for the child to properly adduct or abduct the hip. These contractures, if left untreated, can lead to further gait cycle problems as well as other deformities such as a shortening of the leg. The muscles within the abduction group vary depending on publication however, it is commonly accepted that the Gluteus Medius, Gluteus Minimus, and the Tensor Fasciae Latae are the primary abductors (Duda, Brand, Freitag, Lierse, & Schneider, 1996; Flack, Nicholson, & Woodley, 2012; Merchant, 1965; Neumann, 2010). Computational Models and Evaluations Computational methods and models have become an incredibly useful tool within the sciences. With properly developed and accurate models and even with basic models, behaviors of a variety of phenomenon have been modeled and simulated in order to evaluate designs and naturally occurring structures. Computational models have grown in accuracy and have recently become a part of the biomedical field in the study of hips (Bachtar, Chen, & Hisada, 2006). These models, while few exist, have allowed for contact analysis of the hip joint as in the study done by Bachtar et al (2005), energy analysis within the surgical procedure of closed reduction from Zwawi et al (2016), and several other hip joint analyses (Ardila et al., 2013; Bachtar et al., 2006; Chegini, Beck, & Ferguson, 2009; Girish, 2017; 7
Henak et al., 2011). These analyses provide insight into the development, actions, morphology, stresses, strains, and forces that occur within the hip joint. However, while these models provide insights into the phenomenon that occur at the hip joint there are often sacrifices made in the development of the model or within the simulation such as in the study done by Ardila O. et al in 2013. Due to these constraints, some of the inaccuracies within the models, and the limited number of models that exist overall there is room for models to expand the accuracy of hip dysplasia simulations. While a great deal of experimental data exists and there are studies that have defined some best practices within certain parameters. There is not enough justification mathematically or computationally for the clinical findings within baby wearing and treatment for developmental dysplasia of the hip. Therefore, the purpose of this study is to create an accurate representation of an infant’s hip joint with varying levels of an abduction contracture. In particular, models will be developed that can be used to computationally evaluate hip joint reactions, morphology, and growth patterns associated with abduction contractures that can be used in the prevention and treatment of hip dysplasia. These models will include important muscle and skeletal structures that will be able to be manipulated in order to represent an infant with varying levels of an abduction contracture. With these objectives in mind, three hypotheses can be developed: • With a complete skeletal model of the hip joint, the core structures important to the hip joint with hip dysplasia and an abduction contracture are the Gluteus medius and minimus and these muscles allow for the proper distribution of stress within a healthy joint. • With the inclusion of the aforementioned structures, passive stresses that are developed within the healthy hip joint will resemble previous studies. • Abduction contractures contribute to the development or re-development of hip dysplasia and the level of contracture as well as grade of dysplasia contributes to this development. 8
Having limited computational evaluations for developmental dysplasia of the hip in conjunction with the problems, such as osteoarthritis, it is known to cause, it is imperative that models, such as the one proposed, evaluate varying diagnoses. This would not only answer the above questions, but also to allow for more accurate studies to be performed. These studies, when using an accurate model of the hip joint, would allow for the evaluation of new surgical, non-invasive, and preventative measures to be developed. In addition to new methods being developed, current treatment methods and assumptions could be evaluated to create a better treatment plan for patients and an easier regimen for parents. It also would allow for the evaluation of current preventative measures such as baby wearing and swaddling techniques. With each of these possibilities and previous limitations and studies in mind this model has the potential to change the way developmental dysplasia of the hip is analyzed and treated. 9
Chapter 2 Literature Review Developmental Dysplasia of the Hip (DDH) is a prevalent disorder within infants that describes a condition in which a child’s hip is on a spectrum of instability that ranges from minor instability to complete dislocation and irreducibility of the hip (Dezateux & Rosendahl, 2007). DDH replaced the previous terminology of Congenital Dysplasia of the Hip (CDH) after studies found that while there were genetic factors that played a part in the disorder it was possible to develop the condition over time and that the identifying factors for the disorder also changed over time (Aronsson, Goldberg, Kling, & Roy, 1994). With this observation and change in name, came a recommendation that examinations change from the original single exam at birth to a series of examinations that occurred during the growth of the child. This recognition, as well as the change in name, shifted the view of dysplasia from one that could only appear at birth to one that could develop during the early stages in life (Aronsson et al., 1994). Because DDH is a disorder that encompasses such a variety of hip maladies it is important to define what the maladies may include or what may be seen during a screening. “DDH includes hips that are unstable, malformed, subluxated, or dislocated,” (Aronsson et al., 1994; Dezateux & Rosendahl, 2007). At its core, instability of the hip is “the inability to resist an externally applied force without developing a subluxation or dislocation,” according to Aronsson et al., 1994. Meaning that if an external force is applied in any direction to the hip and the hip joint moves close to out of socket or completely out of socket then the hip is dysplastic. Subluxation, is a partial dislocation of the femoral head from the acetabulum. Therefore, if an external force is applied to the hip, the femoral head will shift to a position that is not entirely out of socket, but instead may be sitting on the posterior, lateral edge of the acetabulum or at a different position within the acetabulum. A complete dislocation is when the femoral head moves entirely out of the socket and rests outside of the acetabulum (Aronsson et al., 1994; T. C. Clarke C., Judd J., 2016b; French & Dietz, 1999). 10
Diagnosing DDH DDH, being a disorder that falls on a spectrum, can be diagnosed in a couple of ways. These diagnoses techniques are performed in two ways, physically and through imaging instrumentation. The standard for physical examination was implemented in “many countries after the publication of two landmark studies in 1962,” (French & Dietz, 1999). The two primary physical examination techniques used for diagnosing hip dysplasia are the Ortolani and Barlow maneuvers (French & Dietz, 1999). These maneuvers both require the infant to be calm and in no way fussy. This is primarily due to the fact that if the neonate is moving erratically the muscle activation within the legs may inhibit the movement of an unstable hip (French & Dietz, 1999). If the hip is being moved erratically or the infant is flexing the muscles surrounding the hip the results of the tests will be distorted and normally the results will not be used in a diagnosis. However, if the child is relaxed it is possible to perform the tests and arrive at a possible diagnosis. Both tests, through the movement of the hip, seek to feel for instability or a dislocation within the hip. Before the neonate has the tests performed on the hips identification of possible dislocation or instability is possible through observation (Aronsson et al., 1994). The examiner is attempting to identify any asymmetry between the two lower limbs. This asymmetry could appear in the form of asymmetric thigh folds, an appearance of having a shorter leg, a prominent greater trochanter, or limited abduction or adduction of the hip (Aronsson et al., 1994). Once one of these observations has been made, the Ortolani or Barlow test is done. According to French and Dietz, “for the examinations the infant’s hips are flexed to 90 degrees; the thumbs of the examiner are placed on the medial proximal thigh, and the long fingers are placed over the greater trochanter,” (1999). This however, is where the two tests begin to differ. 11
Figure 4: The Ortolani Maneuver (Left) and the Barlow Maneuver (Right) (French & Dietz, 1999). For the Ortolani maneuver, with the thumb placed on the medial proximal thigh, and the long fingers placed on the fingers over the greater trochanter, the physician seeks to feel or even hear a “clunk” as the femoral head moves over the acetabulum (Dezateux & Rosendahl, 2007; French & Dietz, 1999). If this clunk or any instability is felt there is a possibility of diagnosis. In addition to the dislocation, if the femoral head is already dislocated the movement can also be used to test the ability of the femoral head to reduce back into the socket (Aronsson et al., 1994). If the femoral head is able to reduce back into the socket then the hip is considered reducible. The Barlow test still attempts to dislocate the hip as seen in figure 4. However, the test attempts to dislocate the hip through the adducting the hip and gently applying pressure towards the posterior of the infant via the knee (Aronsson et al., 1994). If the hip slips over the posterior of the acetabulum there is normally an audible “clunk” indicating the dislocation of the femoral head. This test is usually performed in tandem with the Ortolani test in order to increase the likelihood of dysplasia detection. 12
Unfortunately, these tests usually only can be performed during the first 10 to 12 weeks of life due to the reduction of ligament and capsular laxity (Aronsson et al., 1994). However, if both hips are dislocated or have severe instability it can be more difficult to detect the inconsistencies within the leg length or the irregular thigh folds, thereby making the tests circumstantial in effectiveness. In addition to the lack of external observational signs it is possible that due to the severity of the dislocation that the hips will in no way reduce or maneuver in a way that makes the “clunking” sound and therefore may cause the severe dysplasia to go undetected. As the child ages there may be other physical signs as well, in particular, when the child approaches walking age there can be a significant limp or oddities within their gate that can indicate DDH (Aronsson et al., 1994; Dezateux & Rosendahl, 2007; Kotlarsky et al., 2015). Imaging for Diagnosis In addition to the physical clinical examinations it is also possible for hip dysplasia to be detected through imaging examinations (Clarke C., Taylor C., & J., 2016; Dezateux & Rosendahl, 2007; Kotlarsky et al., 2015). There are a few imaging examinations that are commonly used in addition to the physical examinations. It is common for imaging techniques to be used after instability or dislocation is detected within the hip from a physical examination these examinations include sonograms, radiographs, and magnetic resonance imaging (MRI). However, there are some countries where imaging is required upon the birth of the child. There have been issues with overdiagnoses due to the use of imaging examinations and the requirement of imaging to detect DDH is still debated. The most common form of electronic imaging used for diagnoses is an ultrasound. This is primarily due to the ability to diagnose the infant relatively quickly and that the ultrasound does not introduce high levels of radiation to the infant. Meaning that even when the infant is within its first week or even day of life an ultrasound can be used in order to properly diagnose the infant with DDH. 13
The ultrasound is also the means by which the Graf system of categorizing hips was developed. Through the screening of over 3000 infants the classification system was developed and is still in use today. This procedure is done with the infant in the static decubitus position with the hip at 35 degrees of flexion and 10 degrees of internal rotation (Aronsson et al., 1994). Three lines are then drawn on the image and a series of angles are measured between the three lines. (Figure 4) Figure 5: Ultrasound drawing of a 7-month old infant with the three lines and two angles used in static ultrasound examination (Aronsson et al., 1994). These angles are then used to determine the level of dysplasia within the hip. In particular, if the alpha angle is measured to be greater than 55 degrees the angle is thought to be normal and for the beta angle if it is measured to be less than 72 degrees it is thought to be normal (Aronsson et al., 1994). However, there are problems with the static method. The largest problem being that the alpha and beta angles are not easy to reproduce when attempting to take images of the infant repeatedly and if the image is not precise or the placement of the infant is not correct than the hip may appear to be more dysplastic than it really is (Aronsson et al., 1994). In addition to the static method of examination there is also the dynamic method described by Aronsson et al, 1994. This method seeks to observe the Barlow 14
and Ortolani maneuvers. Just like the physical examination posterior stress is applied to the knee and subluxation or dislocation is noted. In addition to any motion felt by the examiner the imaging will also show the movement and allow for a better diagnosis. After the Ortolani and Barlow tests are performed with the ultrasound additional images are taken in the transverse plane in order to visualize “the position of the femoral head with respect to the triradiate cartilage of the acetabulum.” (Aronsson et al., 1994). After both forms of dynamic screening a diagnosis is then given to the infant. However, the use of the ultrasound has resulted in a high false positive rate as well as a high treatment rate (Aronsson et al., 1994; Dezateux & Rosendahl, 2007). Ultrasounds are not the only form of imaging used on infants during early life in the diagnosis of DDH. Radiographs are another common imaging technique used with infants in order to determine dysplasia or the type of dysplasia the infant may have. Unfortunately, the radiograph is difficult to interpret during the neonatal period due to the cartilaginous nature of the femoral head and the pelvis (Aronsson et al., 1994; Kotlarsky et al., 2015). Therefore, the radiograph is usually unreliable until ossification has occurred within the femoral head. This ossification normally occurs around 6 months of age and it is then more reliable. In addition to the radiograph, Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) have been used to examine infant hips. However, while there is limited exposure to radiation with the CT scans there is still radiation involved and for that reason the MRI is preferred to the CT. Unfortunately, the MRI is not always consistent with respect to protocols used in the process of obtaining the images and may sometimes require sedation of the infant (Kotlarsky et al., 2015). Therefore, with the drawbacks of most imaging processes it is common to see the ultrasound used in addition to the clinical examinations. After diagnosis, a treatment plan is then issued to the infant in order to correct the dysplasia. 15
DDH Treatments There are a wide variety of treatments for DDH but overall, there are two groups for the treatment, surgery and harnesses/external treatment devices (Kotlarsky et al., 2015). After diagnosis and based on the severity of the DDH a treatment is prescribed in order to correct the instability or dislocation within the hip. This treatment normally comes in two forms. First, a harness is prescribed to the patient in order to attempt reduction of the hip and correction of the hip dysplasia over time. This is normally an effective form of treatment and the standard in most societies is the Pavlik harness (Ardila et al., 2013; Aronsson et al., 1994; Atrey & Katchburian, 2010; Dezateux & Rosendahl, 2007; Kotlarsky et al., 2015). The Pavlik Harness and the other harnesses are often prescribed within the first few weeks of the neonate’s life and seek to correct the current type of Hip Dysplasia as well as prevent further development of hip dysplasia within the neonate. If the harness is ineffective or doesn’t correct the dysplasia fast enough a surgical approach may be taken. The surgical approach is often done in more severe cases or in cases where the hip does not reduce or improve with previous treatment (Kotlarsky et al., 2015). There are two surgeries that are normally performed and they are known as open and closed reduction surgeries. These surgeries seek to force the femoral head back into the acetabulum and in severe cases change the angle and location of the acetabulum or the anteversion of the hip (Zwawi et al., 2017). However, due to the need to use general anesthesia on the infant during the surgery and for the removal and replacement of the casts every few weeks after the surgery, the operations are seen as a last resort in treatment. There are a variety of harnesses used throughout the world including the Pavlik Harness, Craig Splint, the von Rosen splint, and the Ilfeld abduction orthosis (Sankar, Nduaguba, & Flynn, 2015; Wilkinson et al., 2002). Each of the harnesses seek to reduce and confine the hip in slightly different ways. These devices, at their core, seek to reduce the hip if it is in anyway dislocated, hold the hip in an orientation that is conducive to proper growth, and allow for enough movement to prevent avascular 16
necrosis (Suzuki, 1994; Wilkinson et al., 2002). These devices accomplish this by moving the hips to an abducted and flexed position. In this position the hip is the most likely to reduce and is conducive to proper femoral head and acetabulum development (Suzuki, 1994). However, there are fundamental differences in how these harnesses accomplish this position. For this reason, certain harnesses or splints are preferred over others and certain harnesses/splints are more effective than others. Currently the Pavlik harness is the most popular form of treatment due to its high success rate although it is possible that other harnesses could be more effective (Kotlarsky et al., 2015). Figure 6: Pavlik Harness applied to an infant (Ardila et al., 2013). As previously the Pavlik harness is the most common form of treatment for neonates after a diagnosis of DDH. This harness has been proven to be effective in up to 99% of all Graf III or lower cases and has been used extensively throughout the world (Atrey & Katchburian, 2010; Kotlarsky et al., 2015; Ömeroğlu et al., 2016). The system works by placing the feet of the infant in stirrups and using the anterior and posterior stirrup straps to abduct (posterior) and flex (anterior) the hips in a position 17
determined by the attending physician for the treatment of the child. These straps are held in place using a touch fastener or buckles that are attached at the halter to the shoulder straps (Ardila et al., 2013). Often times a mark is placed on the straps in order to ensure that the harness is put in the same place after each removal. The system is preferred due to its pliability and high success rate. The pliability is important due to the need of the infant to be able to move its’ hips during the treatment because without movement there is an increased likelihood of avascular necrosis. The system also can adapt to the shape of the child and is easy to adjust as needed by the attending physician. However, there are instances where this treatment is ineffective and therefore more drastic action must be taken in order to prevent further development of hip dysplasia. After the failure of harness or splint treatment, the next step is surgery (T. C. Clarke C., Judd J., 2016a; Dezateux & Rosendahl, 2007). The surgeries are either open or closed reduction and both seek to force the femoral head back into the acetabulum. This is usually done through an osteotomy or a femoral head correction. An osteotomy is where the acetabulum is identified as malformed, underdeveloped, or is simply angled wrong within the pelvis to allow for the proper seating of the femoral head. Therefore, during an open reduction the pelvis is cut and the acetabulum is rotated in order to properly align it with the femoral head (Clarke C. et al., 2016). The femoral head is then placed back within the socket and the pelvis is put back together using screws and other devices to ensure there are no further problems with the hip joint during growth or adulthood. There is also a possibility that the femoral head is malformed within the hip joint. This can be due to developmental problems during the prenatal state or developmental problems that occur once the child is born. If the femoral head is deformed and is the cause of the dysplasia, surgical action is taken to correct the deformity and allow for proper growth. After the hip has been reduced via surgical means it is then important to ensure that the hip remains properly positioned to allow for morphological changes to occur. This then requires the hip joint 18
to be fixed or restrained in some manner to allow for proper healing. Often times this restraint is in the form of the spica cast. Treatment with a spica cast takes the infant and places a cast around the lower limbs with the hips both abducted and flexed. With the hips flexed and abducted healing process can then begin. Over the course of a few months the child’s hip heals and develops the proper morphological interference between the femoral head and the acetabulum. During this time the femoral head takes its spherical shape and the acetabulum matches that shape as the socket. However, there are some risks involved. This includes skin deterioration or irritation, repeated exposure to anesthesia, and muscle contractures such as an abduction contracture (Halanski & Noonan, 2008; Kotlarsky et al., 2015; Reed, Carroll, Baccari, & Shermont, 2011; Sankar et al., 2015). Abduction Contractures An abduction contracture is an uncontrolled stiffening or contraction of the hip abductor muscles. This condition is known to be both congenital as well as developmental. Thereby meaning that an infant can be born with the condition or, as discussed earlier, it can be developed through injuries or treatments such as the spica cast. Due to the harsh level of abduction needed for the treatment of hip dysplasia during the casting process the hips can be left in a position that can cause a contracture. There are a few muscles most commonly associated with an abduction contracture including the following: Gluteus Maximus, Gluteus Medius, Gluteus Minimus, Tensor Fasciae Latae, and the Piriformis. These muscles, when uncontrollably stiffened or tightened, are known as an abduction contracture and often present themselves as an abnormal indentation in the skin, abnormal sitting conditions, gait cycle problems, or the inability to perform certain lower body movements such as squatting (Green & Griffin, 1982; Shen, 1975). These abnormalities have long standing negative effects and are therefore often met with surgery or physical therapy to help reduce the stiffness within the muscles. While a few clinical studies have been performed in order to understand the role abduction contractures may play in the development of DDH there is no definitive answer to whether or not an abduction contracture can 19
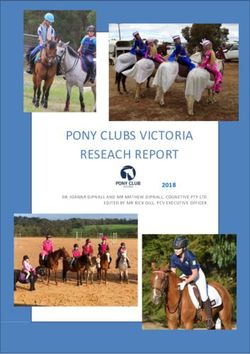
cause hip dysplasia. There however, is an established connection between abduction contractures and contralateral DDH. It is important to note that while no finite element models have been developed for abduction contractures there have been some clinical studies. Within those studies performed by Green et al. (1982), Somerville et al., and Shen (1975) it was observed that the contractures were linked to contralateral dysplasia of the hip with an increased level of force or stress on the acetabulum of the hip joint with the contracture. It has also been observed that when there is also an abnormal indentation of the skin there is also likely a skeletal skew (Green & Griffin, 1982; Shen, 1975; Somerville & Macnicol). Gluteus Medius The Gluteus Medius is considered the primary abductor of the hip and an important stabilizer of the pelvis (Retchford, Crossley, Grimaldi, Kemp, & Cowan, 2013). This muscle originates at the top of the iliac crest and inserts at the femoral head as seen in Figure 7. The Gluteus Medius is, like many other muscles including the Gluteus Minimus, a sheet of muscle. In addition to being a sheet of muscle it is also innervated by the gluteal nerve. This sheet of muscle is broken up into three sections known as the posterior, middle, and anterior parts as seen in Figure 7. 20
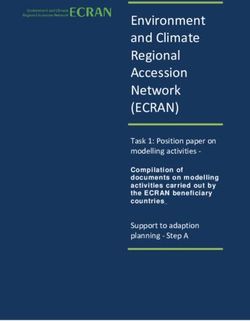
Figure 7: Drawing of the Gluteus Medius and Minimus (Gottschalk, Kourosh, & Leveau, 1989) The break-up of the muscle into three separate sections is also important to note due to the phasic activation the muscle experiences during various activities such as walking or standing. (Gottschalk et al., 1989; Retchford et al., 2013) Gluteus Minimus The Gluteus Minimus, is similar to the Medius in several ways. Primarily the gluteus minimus is known as a hip abductor but it also is known for playing a major role within the stabilization of the hip. This stabilization comes into play primarily during walking or standing and is known to help keep the femoral head properly seated within the acetabulum (Flack et al., 2012; Gottschalk et al., 1989). Similarly, the medius also is a sheet of muscle but, due to its consistent muscle fiber orientation is not always broken into three distinct sections. The Gluteus minimus lies underneath the medius and originates from the anterior inferior iliac spine to the posterior inferior iliac spine as seen in Figure 8. Its insertion point is at the inner aspect of the anterosuperior margin of the greater trochanter (Flack et al., 2012; Gottschalk et al., 1989; Robertson et al., 2008). 21
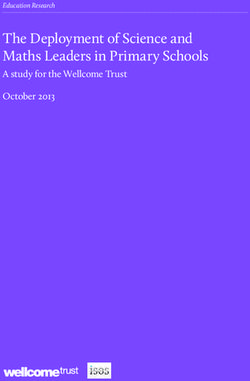
Figure 8: Gluteus Minimus insertion and origin Prevention of DDH It is always better to prevent DDH rather than having to diagnose and treat an infant for the condition. Unfortunately, DDH cannot always be avoided due to some of the genetic factors and predispositions certain infants may have due to the nature of their birth. It is possible however, to prevent certain cases of hip dysplasia and in particular allow for the proper development of the hip. Therefore, it is important to not only look at the state at which an infant is born but also at the way a hip is swaddled and positioned during the development of the infant in the early stages of life. Some of these preventative measures include babywearing and proper swaddling techniques. Preventative measures in baby wearing primarily rely on the abduction and flexion of the hips of the infant. This preventative measure has been observed naturally in places like Africa, China, and Northern Canada where the children are commonly worn on the mother during the first few months of life (Figure 9). 22
Figure 9: (a) – Nigerian woman carrying her child on her back, (b) – Chinese infant being carried in a sling with the hips observably abducted and flexed, (c) – Northern Canadian Eskimo carrying her infant on her back with the hips in an abducted and flexed position. (Girish, 2017; Graham et al., 2015) This position has been used by these groups for extended periods of time and due to the similarity of the carrying method to that of the treatment of the Pavlik harness it is likely that baby wearing in these positions can help reduce the number of incidents of DDH in infants. In addition to the groups mentioned in Figure 9 there are other groups such as the Bantu as well as the native population of Malawi that have shown a small incidence of DDH (Graham et al., 2015; Roper, 1976; Salter, 1968). While genetic factors may still play a large part in the low incidence of dysplasia, it is likely that the environment and positioning of the hip still play a large role in the development of the hip overall. This has been validated by the treatments used to prevent DDH as the hip is placed in a manner that is abducted and flexed in a similar fashion to the way infants are carried in Africa, China, and Northern Canada. 23
In addition to the way the infants are carried by the mothers there are other environmental factors that can play a role in the development of hip dysplasia. In particular, improper swaddling techniques have been attributed to the malformation of infant hip jointss in specific groups of people. These improper swaddling techniques normally include the extension and adduction of the hips so that the infant is laying in a flat and extended position as seen in Figure 10. Figure 10: Infant swaddled with the hips extended and adducted on a cradleboard from a Northern Canadian Indian tribe (Salter, 1968). The infant above is swaddled in a manner where the legs are tightly held in the adducted and extended position and is believed to contribute to a higher incidence of developmental hip dysplasia (Salter, 1968). With this type of swaddling identified, other groups with similar swaddling styles were identified as well with similarities existing between some Northern Italian, Northern Scandinavian, and Japanese swaddling techniques (Graham et al., 2015; Salter, 1968). After these techniques were identified as possible causes for dysplasia, a program in Japan was implemented to change the 24
You can also read