Time- and dose-dependent correlations between patient-controlled epidural analgesia and intrapartum maternal fever
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Zhao et al. BMC Anesthesiology (2021) 21:31
https://doi.org/10.1186/s12871-021-01249-1
RESEARCH ARTICLE Open Access
Time- and dose-dependent correlations
between patient-controlled epidural
analgesia and intrapartum maternal fever
Bai-song Zhao1†, Bing Li2†, Qing-ning Wang1, Jun-xiang Jia2* and Xing-rong Song1*
Abstract
Background: To investigate the relationship between intrapartum maternal fever and the duration and dosage of
patient-controlled epidural analgesia (PCEA).
Methods: This observational study included 159 pregnant women who voluntarily accepted PCEA. During labor,
patients with body temperature ≥ 38 °C were classified into the Fever group, (n = 42), and those with body
temperature < 38 °C were classified into the No-fever group (n = 117). The outcome measures included the duration
of PCEA, number of PCEA, and total PCEA amount. Body temperature and parturient variables, including
interpartum fever status and the duration of any fever were monitored.
Results: The total PCEA duration and total PCEA amount in the Fever group were significantly higher than the
corresponding values in the No-fever group (both, p < 0.05). The duration of fever was weakly correlated with the
duration of PCEA (R2 = 0.08) and the total PCEA amount (R2 = 0.05) (both, p < 0.05). The total and effective PCEA
were higher in the Fever group than in the No-fever group (both, p < 0.05). The total PCEA duration and total PCEA
amount were positively correlated with the incidence of fever (both, p < 0.05). The diagnostic cutoff value for fever
was 383 min, with a sensitivity of 78.6% and specificity of 57.3%. The mean temperature-time curves showed that
parturients who developed fever had a steeper rise in temperature.
Conclusions: This study showed that there were weak time- and dose-dependent correlations between PCEA and
maternal fever during delivery. A total PCEA duration exceeding 6.3 h was associated with an increase in the
duration of maternal intrapartum fever.
Keywords: Patient-controlled epidural analgesia, Maternal fever, Epidural duration, Anesthetic dosage
* Correspondence: ybmzjjx@126.com; songxingrong510623@163.com
†
Bai-song Zhao and Bing Li contributed equally to this work.
2
Department of Anesthesiology, Women and Children’s Hospital, School of
Medicine, Xiamen University, Xiamen 361000, Fujian, China
1
Department of Anesthesiology, Guangzhou Women and Children’s Medical
Center, Guangzhou Medical University, No. 9 Jinsui Road, Tianhe District,
Guangzhou 510623, Guangdong, China
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.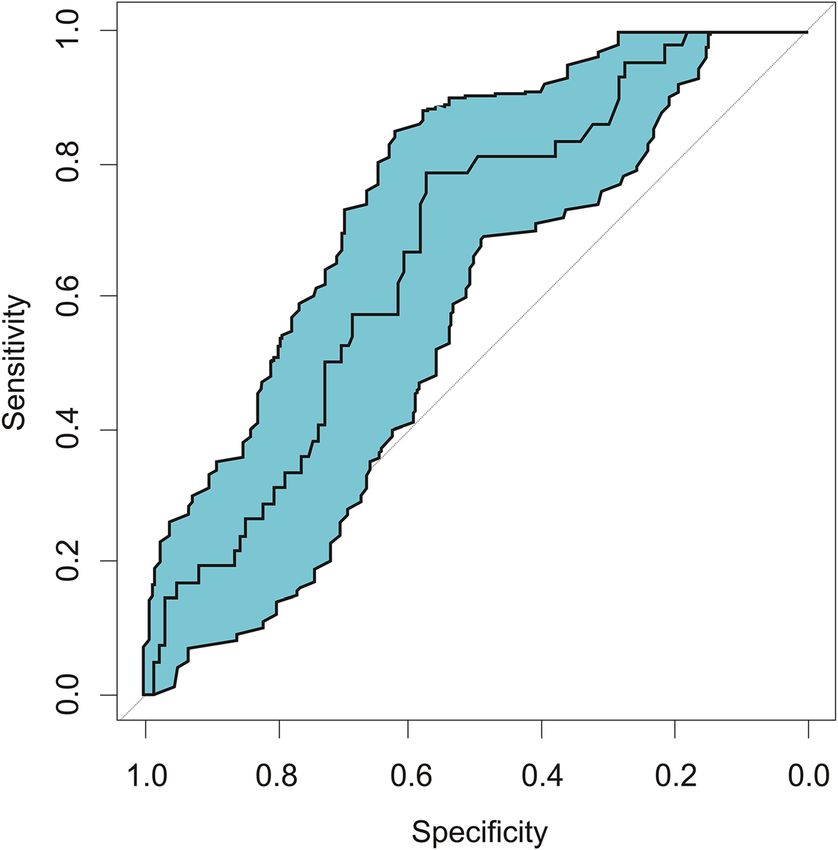
Zhao et al. BMC Anesthesiology (2021) 21:31 Page 2 of 8 Background analgesic data during labor. We focused on the effect of Intrapartum maternal fever refers to an oral analgesia duration on fever, with the goal of generating a temperature ≥ 38 °C during childbirth [1, 2]. Various mean temperature-time curve to guide the clinical man- prospective and retrospective studies as well as random- agement of ERMF. ized controlled trials have shown that non-infectious fever during childbirth is associated with patient- Methods controlled epidural analgesia (PCEA); about 20% of Research population parturients that receive PCEA develop epidural-related This study was approved by the Ethics Committee of maternal fever (ERMF) [1–3]. Our previous study con- Guangzhou Women and Children’s Medical Center firmed this through accurate and continuous monitoring (Protocol Number: 201939000). Pregnant women who of core temperature, which revealed a maternal fever planned to give birth during the daytime working hours rate of 26.4% in women who used PCEA. at our institution between September 30, 2019 and The specific mechanism of ERMF is not clear. It has December 31, 2019 were recruited for this study. Writ- been suggested that local anesthetics trigger non- ten informed consent was obtained from all participants infectious inflammation via immune regulation and cell before the start of the trial. injury. A single-center observational cohort study The inclusion criteria were as follows: 1) parturient posited that ERMF occurred due to impaired release of with full-term singleton pregnancy (> 37 weeks); 2) anti-pyrogenic interleukin-1 receptor antagonist (IL- scheduled vaginal in-hospital delivery; 3) vertex presen- 1Ra). The researchers investigated the effects of tation; 4) no risk of mother-to-child transmission of an bupivacaine on apoptosis, caspase-1 activity, intracellular infectious disease; 5) no suspected fetal coagulopathy; 6) IL-1Ra, and the plasma IL-1Ra/IL-1β ratio in mono- willingness to use PCEA and ability to provide informed nuclear leucocytes from laboring women. The study consent; and 7) pre-epidural temperature > 37 °C. The found that bupivacaine decreased the activity of caspase- following exclusion criteria were applied: 1) need for 1 in the peripheral blood mononuclear cells of laboring vascular access in both upper extremities; 2) absent women, which subsequently inhibited the release of upper extremities; 3) history of myocardial infarction, intracellular IL-1Ra by circulating leukocytes and re- heart failure, maternal hepatitis, or HIV infection; 4) his- vealed that immunomodulation by bupivacaine during tory of serious skin allergies, allergy to silicone or plastic; labor promoted ERMF [4]. In two different studies, 5) preeclampsia; 6) taking paracetamol within 6 h before Wang et al. found that although the average analgesic the study; 7) presentation other than vertex (i.e., breech duration in the early PCEA group was significantly lon- or transverse); 8) gestational age < 37 weeks; or 9) sus- ger than that in the late PCEA group, the average body pected fetal coagulopathy. temperature and fever rate were almost the same [5, 6]. On admission to the delivery room, all eligible par- They speculated that the relationship between PCEA turients were informed about the study by the re- and ERMF could be attributed to the “triggering effect” searchers and consent was obtained for study of local anesthetics via non-infectious inflammation. participation. The individuals collecting the body Consequently, they concluded that this effect was not as- temperature data were blinded to the duration and sociated with the duration of PCEA or the dosage of dosage of PCEA. local anesthetics, although further research is needed to confirm the speculation. However, the relationship of Body temperature measurement and treatment of fever epidural analgesia and maternal fever was not a relevant The axillary temperature was recorded (10 measurements comparison. Investigations are limited in scope due to per second) throughout labor using a smartphone/iPad- the existing body temperature monitoring methods. In connected wireless thermometer (iThermonitor; Rui Ren most current investigations, maternal temperature is Medical, China). The iThermonitor was secured to the measured at predefined time points according to cervical (shaved) axilla using a hypoallergenic adhesive patch. The dilatation [7] or at regular intervals during labor [6, 8]. women were instructed to adduct the ipsilateral arm for Therefore, it is impossible to generate a precise and con- up to 5 min after the iThermonitor had been secured, or tinuous temperature-time curve. Continuous monitoring until the temperature displayed on the paired smart- of maternal core body temperature has not yet revealed phone/iPad was stable. Subsequently, the women were the factors associated with elevated maternal allowed to move their arms freely [9]. Unwarmed intra- temperature during labor. venous (IV) infusions in the contralateral arm were as- This study investigated the associations of PCEA dur- sumed to have had no effect on the measurement of ation, anesthetic dosage, and intrapartum maternal fever axillary temperature with the iThermonitor. using a novel method for the continuous monitoring of Midwives monitored the parturient and followed the maternal core body temperature and the recording of doctors’ prescriptions. The onset of labor was self-
Zhao et al. BMC Anesthesiology (2021) 21:31 Page 3 of 8
reported by the mothers. Fever was defined as an axillary sample size required for the No-fever group was 111 and
temperature ≥ 38 °C. If the parturient developed a fever, that for the Fever group was 37.
the following measures were taken to lower the body 2
temperature: when the axillary temperature rose to 38– ðr þ 1Þ z1 − β þ z1 − α S2
nC ¼
38.5 °C, fluid replacement was also accelerated to replen- r ðΔ − δ Þ2
ish the water lost at this temperature. Acetaminophen ð3 þ 1Þð0:84 þ 1:96Þ2 47277
(Johnson & Johnson Pharmaceuticals, Ltd., China) was ¼ ¼ 37
3ð20 − 136Þ2
administered orally to the women when the axillary
temperature rose above 38.5 °C. Note: r is the ratio between the experimental group
and the control group, Δ is the superiority limit, δ is the
difference between the mean values of the two groups,
Patient-controlled epidural analgesia and S is the combined variance of the two groups.
Epidural analgesia was performed when the contrac- Statistical analysis performed using SPSS software (ver.
tions became regular and cervical dilation was up to 21.0; SPSS Inc., USA) showed that gestational age, BMI,
1 cm. Women receiving PCEA were given IV Ringer’s total PCEA duration, total PCEA dose, total number of
lactate 2 ~ 4 mL/kg/h. Rescue atropine and ephedrine PCEA uses, and effective number of PCEA did not con-
were available at the bedside. An epidural catheter form to normal distributions; therefore, these data were
was introduced at L3–L4 and the epidural analgesia expressed as the median and interquartile range. The
was patient-controlled. After 5 min, a 10 mL bolus of groups were compared using the rank sum test. The cor-
ropivacaine 0.0625% (lot number: H20140763; Astra relations of the duration of fever with the total duration
Zeneca, Sweden) plus 0.3 μg/mL sufentanil (batch of PCEA and the total PCEA dose were analyzed with
number: H20054256; Yichang Renfu Pharmaceutical, the Spearman method, and the effects of different factors
China) was administered. Then, the epidural catheter on intrapartum fever were determined using stepwise lo-
was connected to a pulse analgesia pump with the gistic regression. The association of PCEA time with the
following parameters: loading dose, 10 mL; injection diagnosis of fever was assessed through receiver operat-
rate, 6 mL/h; PCEA (demand) dose, 8 mL; maximum ing characteristic (ROC) curve analysis. p < 0.05 was
dose, 40 mL/h; and lockout interval, 10 min. The anal- considered statistically significant.
gesic level was assessed according to the patient’s
sensitivity to temperature (ice) after 15 min. Add- Results
itional 5 mL boluses of 0.1% ropivacaine were given Study subjects
for breakthrough pain and a visual analogue scale This study included 169 women, among whom 46 devel-
pain score < 3 at any time during labor. oped intrapartum fever (Fever group, > 38 °C) and 123
did not (No-fever group, ≥38 °C) (Fig. 1). Finally, the
Data collection
data for 42 women in the Fever group and 117 women
Maternal demographic and clinical characteristics in the No-fever group were analyzed.
were recorded, including age, height, weight, body There were no significant differences in the maternal
mass index (BMI), gender, and ethnicity. Analgesic demographics (gestational age and BMI) or clinical char-
data, including the duration of PCEA, total and ef- acteristics (primipara/multigravida) between the two
fective number of PCEA doses, and total PCEA dose groups (Table 1). The total PCEA duration in the Fever
were also collected. The body temperature and group (9.70 ± 3.22 h) was significantly higher than that in
changes in the parturients, including intrapartum the No-fever group (8.35 ± 3.98 h) (p = 0.049). The total
fever status and the duration of any fever, were re- PCEA amount in the Fever group (130.50 ± 73.22 mL)
corded. The data for parturients who were converted was also significantly higher than that in the No-fever
to cesarean sections were not analyzed. Maternal group (99.87 ± 48.46 mL) (p = 0.003). However, there was
blood pressure and heart rate were monitored con- no difference in the total PCEA amount/PCEA duration
tinuously during childbirth and the rate and volume between the two groups (13.37 ± 4.62 mL/h vs. 12.84 ±
of fluid administered were measured. 5.78 mL/h, p = 0.591, Table 1).
The mean temperature-time curves for the Fever and
No-fever groups showed that parturients who developed
Statistical analysis fever had a steeper, steady increase in temperature than
Our previous study (in the process of review) showed those who did not develop fever, with a flat curve
that the ratio of fever and no fever in parturients during (Fig. 2).
labor was 1:3. Based on this finding and the following Spearman correlation analysis showed that the dur-
formula with α = 0.05 and a power of 0.9, the minimum ation of fever (1.53 h [1.16]) was positively correlatedZhao et al. BMC Anesthesiology (2021) 21:31 Page 4 of 8
Fig. 1 The flow chart for the study
with the total PCEA duration (9.70 ± 3.22 h, R2 = 0.08) (95% CI: 48.2–66.4%), and odds ratio of 4.913 (95% CI:
and the total PCEA dose (130.50 ± 73.22, R2 = 0.05) 2.157–11.190) (Fig. 3).
(both, p < 0.05), which indicated that the duration of
fever increased slightly with the total PCEA duration Discussion
and dose (Table 2). In this study, continuous real-time body temperature
In the Fever group, the parturients’ demand for anal- monitoring was performed to explore the relationships
gesia was higher, and the total and effective number of between the duration and dosage of patient-controlled
PCEA were higher in the Fever group than in the No- epidural labor analgesia and intrapartum maternal fever.
fever group; the differences between the two groups The wireless temperature sensor used in this study is
were significant (all, p < 0.05) (Table 3). an innovative continuous temperature monitoring device
Stepwise logistic regression analysis was performed that uses a high-precision thermistor probe attached to
with intrapartum fever as the dependent variable. The the axillary root, a model algorithm based on a large
total PCEA duration and amount had positive associa- number of accumulated experimental data, and com-
tions with the incidence of fever (both, p < 0.05). As the puter programs to predict and further, to correct the
total PCEA duration and dose increased, the likelihood body temperature [9]. The parameter values recorded by
of fever increased (Table 4). the sensor were assessed from raw measurement data
ROC curve analysis showed that the area under the using a noise reduction algorithm (filtered and anti-
curve value for diagnosing fever based on the duration interfered). The innovative model algorithm was based
of analgesia was 0.666 (0.577 ~ 0.755) (Fig. 3), which was on a large sample of data collected in the operating
significant (p < 0.05). The diagnostic cutoff value for room environment such as the room temperature and
fever was 383 min, with a sensitivity of 78.6% (95% confi- the human bladder, esophageal, and axillary tempera-
dence interval [CI]: 65.6–91.5%), specificity of 57.3% tures, as well as experimental data from different parts
Table 1 Maternal and neonatal demographic and clinical characteristics
Fever (n = 42) No fever (n = 117) Z/t/x2 P
Gestational age (week) 40.14 (1.50) 39.86 (1.50) −1.182 0.237
BMI (kg/m2) 26.44 (2.90) 25.87 (3.60) −1.592 0.111
Primipara/Multigravida 31/11 73/44 1.780 0.182
Total PCEA duration (h) 9.70 ± 3.22 8.35 ± 3.98 1.983 0.049
Total PCEA amount (mL) 130.50 ± 73.22 99.87 ± 48.46 3.041 0.003
Total PCEA amount /PCEA duration (mL/h) 13.37 ± 4.62 12.84 ± 5.78 0.538 0.591
Data are medians (interquartile range)
BMI body mass indexZhao et al. BMC Anesthesiology (2021) 21:31 Page 5 of 8
Fig. 2 The mean temperature-time curve of parturients in two groups
of the human body. The sensor accurately reflected the was higher than 38 °C. The ROC curve confirmed that
human esophageal temperature. Therefore, the wireless the duration of PCEA predicted maternal fever, with epi-
temperature sensor can be considered a convenient and dural analgesia lasting over 6.3 h significantly increasing
accurate body temperature measurement tool. the risk of fever. Therefore, anesthesiologists and obste-
There was no significant difference in the general data tricians should routinely monitor the body temperature
between the Fever and No-fever groups. Intrapartum of parturients undergoing PCEA, especially when PCEA
maternal fever was time- and dose-dependently corre- lasts over 6.3 h and the analgesia demand is high. Early
lated with PCEA; parturients with a greater demand for measures should be taken to prevent maternal fever,
analgesia were more likely to have a fever. Logistic such as reducing the room temperature, removing cloth-
regression analysis showed that the PCEA duration and ing, applying fluid hydration, and using oxytocin to ac-
total PCEA doses were correlated with the incidence of celerate labor.
fever, with extremely small effect sizes. The mean Other studies found that PCEA was associated with
temperature-time curves showed a steeper increase of maternal fever, which is an important risk factor for
temperature in the Fever group as the duration of anal- adverse neonatal outcomes, including postpartum
gesia increased. In some cases, when the analgesia dur- hemorrhage and labor dystocia, and is also associated
ation was greater than 6 h, the maternal temperature with a higher rate of cesarean section [10]. The effects of
fever on newborns include neurodepressive symptoms,
Table 2 Correlations of duration of fever with total duration such as decreased Apgar scores, a higher likelihood of
and dose of PCEA (n = 159) ventilation and oxygen inhalation, and an increased rate
Total PCEA time Total PCEA amount of cardiopulmonary resuscitation [3]. Previously, we ob-
Duration of fever r 0.279 0.223 served that women receiving epidural analgesia who de-
R2 0.08 0.05
veloped a fever had a prolonged first stage of labor and
increased rates of cesarean section, assisted vaginal deliv-
P < 0.001 0.005
ery, intrapartum and postpartum hemorrhage, andZhao et al. BMC Anesthesiology (2021) 21:31 Page 6 of 8
Table 3 Total and effective number of PCEA uses
Fever (n = 42) No fever (n = 117) Z P
Total number of PCEA uses 3.00 (4.00) 2.00 (3.00) −2.021 0.043
Effective number of PCEA uses 2.00 (2.00) 1.00 (2.00) −2.290 0.022
Data are medians (interquartile range)
PCEA patient-controlled epidural analgesia
turbid amniotic fluid compared with women without proinflammatory cytokines (IL-6 and IL-8) even before
fever, but there were no effects from epidural analgesia receiving epidural analgesia, and the subsequent pro-
on neonate Apgar scores [11]. We believe that it is im- longed use of epidural bupivacaine increased the base-
portant to monitor changes in maternal temperature dy- line cytokine levels gradually [14]. Zhou et al. found that
namically during labor, and to intervene to ensure the the IL-6 and tumor necrosis factor (TNF)-α levels of
safety of mothers and infants. their 0.075% ropivacaine group were significantly lower
Therefore, we continuously monitor the maternal core than those of their 0.1% ropivacaine group [15]. The use
body temperature and plot a temperature-time curve at of 0.075% ropivacaine caused less inflammation. Lower
our institute. More importantly, we use an information anesthetic concentrations contributed to lower rates of
management system during obstetrical delivery to moni- intrapartum fever. However, they did not report the
tor the data from the analgesia pump. This system also anesthesia dosage used in their experiment.
enables us to monitor the duration and dosage of PCEA In the current clinical study, the duration and total
analgesia, and to analyze the correlation between anal- amount of PCEA were both associated with epidural an-
gesia and body temperature. algesia fever during labor. We speculate that with in-
Our study confirmed that there were time- and dose- creasing ropivacaine exposure, the risk of ERMF caused
dependent correlations between PCEA and intrapartum by aseptic inflammation slightly increases. Analysis of
maternal fever. However, the influence was weak and the ROC curve showed that an analgesia time longer
predictable. Women with a PCEA duration exceeding than 6.3 h significantly increased the risk of fever. Yin
6.3 h were more likely to have a fever. PCEA is an inde- et al. reported that the cutoff point for an increased risk
pendent risk factor for intrapartum fever, as confirmed of fever was 6 h after analgesia [12]. However, they mon-
by many studies [1, 3, 7, 12]. However, the mechanism itored body temperature hourly, not continuously, and
by which PCEA causes intrapartum fever is still unclear. thus could not precisely detect the cutoff point.
Wang et al. randomly divided parturients into an early Our study had some limitations. First is the study de-
PCEA group and an IV pethidine with delayed PCEA sign. This is an observational study rather than a ran-
group [5]. The average analgesic time (12.6 h) in the domized trial, and thus a potential bias may exist.
early PCEA group was significantly longer than that in Second, there were no data on the levels of inflammatory
the delayed group (4.8 h), and the average oral tempera- factors during delivery, and the time- and dosage-
tures in the two groups were similar at 37.4 ± 0.4 °C and dependent effects of ropivacaine on body temperature
37.2 ± 0.3 °C, respectively. In another study, Wang et al. were obtained from clinical observations. In addition,
randomly divided parturients into immediate and de- the sample size was relatively small. In future research,
layed PCEA groups (average delay, 129 min) after spinal we will increase the sample size and determine the levels
analgesia, and found no significant difference in the ma- of inflammatory factors.
ternal fever rate between the groups [6]. Therefore, some
researchers speculate that the “trigger-effect” of local an- Conclusions
esthetics leads to intrapartum fever via non-infectious This study was conducted with continuous real-time
inflammation [13]. monitoring of maternal core body temperature and the
Others believe that the exposure time and dosage of recording of analgesic data during labor, and investi-
local anesthetics may also promote maternal fever. Riley gated the associations of PCEA duration and drug dos-
et al. found that women with ERMF had higher levels of age with intrapartum maternal fever. The duration of
Table 4 Logistic regression analysis of factors associated with intrapartum fever (n = 159)
Risk factors Regression coefficient Standard error Wald P OR 95% CI
Total PCEA duration (h) 0.002 0.001 6.181 0.013 1.002 1.000 ~ 1.004
Total PCEA amount (ml) 0.008 0.003 5.569 0.018 1.008 1.001 ~ 1.015Zhao et al. BMC Anesthesiology (2021) 21:31 Page 7 of 8
Fig. 3 Receiver operating characteristic (ROC) curve for diagnosing fever based on analgesic time. Area under the curve = 0.666, Standard error =
0.045, 95% CI = 0.577–0.755, P = 0.001
PCEA and total PCEA dose in parturients with fever Availability of data and materials
during delivery were significantly higher than the corre- The datasets generated and analyzed during the present study are available
from the corresponding author on reasonable request.
sponding values in those without fever. There were weak
time- and dose-dependent correlations between PCEA
Ethics approval and consent to participate
and maternal fever during delivery. Analgesic drugs can This study was approved by the Ethics Committee of Guangzhou Women
cause ERMF and an analgesic time over 6.3 h increases and Children’s Medical Center (protocol no. 201939000) and written
the risk of maternal intrapartum fever to some extent. informed consent was obtained from all subjects.
Consent for publication
Abbreviations Not applicable.
BMI: Body mass index; ERMF: Epidural-related maternal fever; PCEA: Patient-
controlled epidural analgesia; ROC: Receiver operating characteristic;
SD: Standard deviation; TNF: Tumor necrosis factor Competing interests
The authors declare that they have no conflict of interest.
Acknowledgments Received: 26 March 2020 Accepted: 20 January 2021
Not applicable.
Authors’ contributions References
ZBS conceived and designed the research; LB analyzed and interpreted the 1. Sultan P, David AL, Fernando R, Ackland GL. Inflammation and epidural-
data and wrote the initial paper; WQN collected data and conducted the related maternal fever: proposed mechanisms. Anesth Analg. 2016;122(5):
research; JJX had primary responsibility for the final content; SXR had 1546–53.
primary responsibility for the final content. All authors read and approved 2. Higgins RD, Saade G, Polin RA, Grobman WA, Buhimschi IA, Watterberg K,
the final manuscript. et al. Evaluation and management of women and newborns with a
maternal diagnosis of chorioamnionitis: summary of a workshop. Obstet
Gynecol. 2016;127(3):426–36.
Funding 3. Sharpe EE, Arendt KW. Epidural labor analgesia and maternal fever. Clin
This project was supported by the Natural Science Foundation of China Obstet Gynecol. 2017;60(2):365–74.
(grant no. 81701109). The authors declare that they have no financial 4. Del Arroyo AG, Sanchez J, Patel S, Phillips S, Reyes A, Cubillos C, et al. Role
relationship with the organization that sponsored the research, and the of leucocyte caspase-1 activity in epidural-related maternal fever: a single-
funding body was not involved in the study design, data collection, analysis centre, observational, mechanistic cohort study. Br J Anaesth. 2019;122(1):
and writing of the manuscript. 92–102.Zhao et al. BMC Anesthesiology (2021) 21:31 Page 8 of 8
5. Wang F, Shen X, Guo X, Peng Y, Gu X. Epidural analgesia in the latent phase
of labor and the risk of cesarean delivery: a five-year randomized controlled
trial. Anesthesiology. 2009;111(4):871–80.
6. Wang LZ, Chang XY, Hu XX, Tang BL, Xia F. The effect on maternal
temperature of delaying initiation of the epidural component of combined
spinal-epidural analgesia for labor: a pilot study. Int J Obstet Anesth. 2011;
20(4):312–7.
7. Lavesson T, Kallen K, Olofsson P. Fetal and maternal temperatures during
labor and delivery: a prospective descriptive study. J Matern Fetal Neonatal
Med. 2018;31(12):1533–41.
8. Towers CV, Yates A, Zite N, Smith C, Chernicky L, Howard B. Incidence of
fever in labor and risk of neonatal sepsis. Am J Obstet Gynecol. 2017;216(6):
596.e1–5.
9. Pei L, Huang Y, Mao G, Sessler DI. Axillary temperature, as recorded by the
iThermonitor WT701, well represents core temperature in adults having
noncardiac surgery. Anesth Analg. 2018;126(3):833–8.
10. Dior UP, Kogan L, Eventov-Friedman S, Gil M, Bahar R, Ergaz Z, et al. Very
high intrapartum fever in term pregnancies and adverse obstetric and
neonatal outcomes. Neonatology. 2016;109(1):62–8.
11. Qian X, Wang Q, Ou X, Li P, Zhao B, Liu H. Effects of ropivacaine in patient-
controlled epidural analgesia on uterine electromyographic activities during
labor. Biomed Res Int. 2018;2018:7162865.
12. Yin H, Hu R. A cohort study of the impact of epidural analgesia on maternal
and neonatal outcomes. J Obstet Gynaecol Res. 2019;45(8):1435–41.
13. Arendt KW, Segal BS. The association between epidural labor analgesia and
maternal fever. Clin Perinatol. 2013;40(3):385–98.
14. Riley LE, Celi AC, Onderdonk AB, Roberts DJ, Johnson LC, Tsen LC, et al.
Association of epidural-related fever and noninfectious inflammation in
term labor. Obstet Gynecol. 2011;117(3):588–95.
15. Zhou X, Li J, Deng S, Xu Z, Liu Z. Ropivacaine at different concentrations on
intrapartum fever, IL-6 and TNF-alpha in parturient with epidural labor
analgesia. Exp Ther Med. 2019;17(3):1631–6.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in
published maps and institutional affiliations.You can also read