TTM and post-arrest care: clinical trials and recent evidence - Benjamin S. Abella, MD, MPhil
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

TTM and post-arrest care:
clinical trials and recent evidence
Benjamin S. Abella, MD, MPhil
Clinical Research Director
Center for Resuscitation Science
Department of Emergency Medicine
University of Pennsylvania
RACI - Anchorage, May 2014
Speaker
Speakerdisclosures
disclosures
Research Funding: NIH – NHLBI
Philips Medical Systems
Doris Duke Foundation
Stryker Medical Corp
Honoraria/consulting: Velomedix
Stryker Medical Corp
Medical Advisory Board: HeartSine
Equity: Resuscor LLC
The post-arrest
Survival problem
in cardiac arrest
arrest in-hospital
arrest data
CPR
% Surviving
52%
ROSC 18%
hospital
discharge
Time
Reperfusion
Reperfusioninjury
injury
Damage observed after restoration
of blood flow to ischemic tissues
% Surviving
Time
Hypothermia mechanisms
Reperfusion injury pathways
ischemia reperfusion
reactive oxygen mitochondrial
species (ROS) inflammatory dysfunction
cascades
hypothermia
vascular dysfunction/hypotension
apoptosis – organ dysfunction
cerebral edema
Modern erafrom
Key RCTs of hypothermia
2001-2002 use
HACA,
2002
Bernard,
2002
Idrissi,
2001
Concept of post-arrest
Temperature TTM
dynamics of TTM
39
Bladder temperature, oC
38
37
36
35
34 Cold (24 hr)
33 Cooling (8-12 hr)
Rewarming (24 hr)
32
0 6 12 18 24 28 32 36 40
Time in hours
Snapshots of the three trials
RCT details
Multicenter? Main site pt rhythm pt location N
HACA YES Austria VF OOH 275
Bernard YES Australia VF OOH 77
Idrissi NO Belgium PEA/asystole OOH 30
Snapshots
More RCT of the three trials, part II
details
Age Female VF ROSC Target Duration Method
(years) sex (#) (min) temp (hours)
(%) (°C)
59 65 254 22
HACA (51-68) (24) (92%) (16-30)
33 24 Cool air
68 25 77 24 Ice
Bernard (57-75) (32) (100%) (17-32)
33 12
packs
74 13 0 33
Idrissi (66-79) (39) - (27-37)
34 Up to 4 Helmet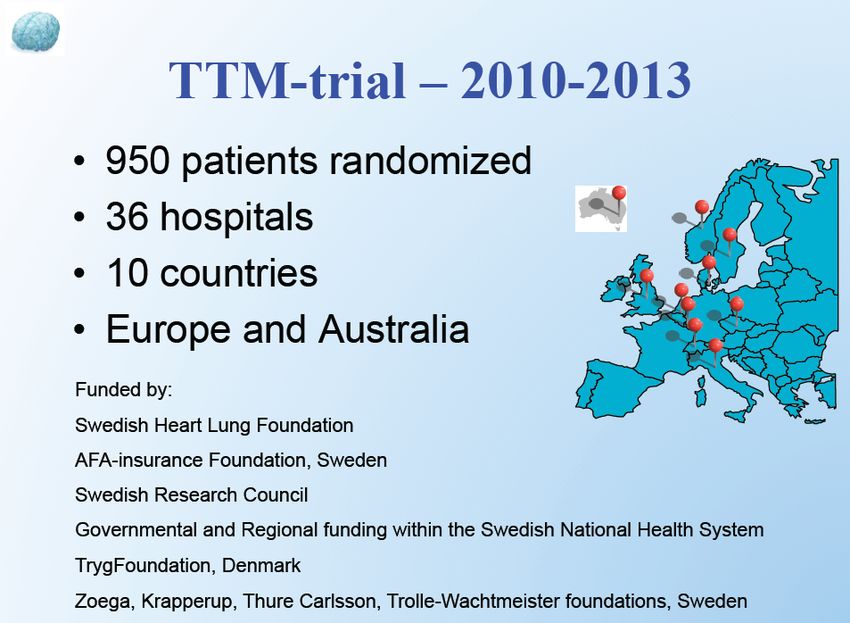
What
HACAcooling looks like
temperature curves
Cold maintenance
Cooling (8-12 hr) Rewarming (24 hr)
HACA, 2002Hypothermia trials: outcomes
RCT outcomes
Hypothermia Normothermia RR P value
(%) (%) (95% CI)
Alive at hospital discharge with
favourable neurological
recovery
72/136 50/137 1.51
HACA (53%) (36%) (1.14-1.89)
0.006
21/43 9/34 1.75
Bernard (49%) (26%) (0.99-2.43)
0.052
4/16 1/17 4.25
Idrissi (25%) (6%) (0.70-53.83)
0.16
Alive at 6 months with
favourable neurological
recovery 71/136 50/137 1.44
HACA (52%) (36%) (1.11-1.76)
0.009Hypothermia
AHA in the guidelines
guidelines
Comatose out-of-hospital VF:
Class IIa recommendation
2010: Changed to Class I
In-hospital arrest, other rhythms:
Class IIb recommendation
2010: Still Class IIbReal worldofusage:
Example Switzerland
real world study
2006
Oddo M et al, 2006
Retrospective study at one hospital in Switzerland
Cooling intervention with historical controls
Survivors of out-of-hospital arrest (n=109)
Cooling initially via ice bags, then cooling mattress
Target temperature 33oC, maintained for 24 hrs
All post-arrest ST elevations received cardiac cathReal world usage:
Outcomes Switzerland
for VF patients
Outcome at discharge for out-of-hospital VF arrest
baseline CPC5 CPC3 CPC2 CPC1
56% 19% 12% 14%
cooling CPC 5 .CPC3 CPC2 CPC1
40% 5% 14% 42%Real world for
Outcome usage: Switzerland
asystole patients
Outcome at discharge for out-of-hospital asystole arrest
baseline CPC5 CPC3
89% 11%
cooling CPC5 CPC1
83% 17%Compilation of recent experiences
TTM for nonshockable rhythms
2009
Hypothermia clinical benefit is robust (consistent across
Numerous studies)Compilation of recent experiences
TTM for nonshockable rhythms
Meta-analysis of hypothermia for non-shockable
Rhythms (non-VF/VT)
Kim Y et al, 2012Research via a hypothermia
Nielsen registry study registry
Nielsen et al, 2009
Bradycardia (13%)
Significant bleed (4%)Cooling
TTM and and
thePCI
cath lab
2011
Less than 40% of patients
had STEMI; yet huge
survival benefits when
OHCA patients cathedPrognostication is a challenge
Post-arrest awakening
Grossestreuer, 2013Comparison between
Comparing TTM devices
devices
No study has shown
significant outcome
or adverse event
differences between
devices
Pittl, 2013The 2013
The TTM TTM
Trial trial (Nielsen
– Nielsen et al et al)
Nov 2013Details
The TTMof the– Setting
Trial TTM trialCharacteristics of each
The TTM Trial – Nielsen group
et alOutcomes in –the
The TTM Trial TTMettrial
Nielsen alTTM subgroup
The TTM analyses
Trial – Nielsen et alKey question
Making sense ofraised by TTM trials
the post-arrest trial
HACA
no cooling 36%
33oC 53%
0 10 20 30 40 50 60
no cooling % 26%
survival
Bernard
How can
this be?
33oC 49%
TTM
36oC 52%
33oC 50%Temperature curve
Marked differences in comparison
control group
Nielsen et al HACA study
~37.6oC
~36.0oC
Bernard et al: ~37.3oC
Large difference in maintenance temperatures2013 TTM trial: key point 2013 TTM trial does not test the same hypothesis as the HACA, Bernard trials 36oC arm in the trial is still active management of temperature
Overview of post-arrest outcomes
Degree of post-arrest injury
severe moderate Mild / none
Poor outcome Good outcome
with any TTM with any TTM
dose of TTM
(33oC v 36oC, e.g.)
affects outcomeRationale for our approach
Given that:
(1)TTM trial was neutral (no differences in benefit or harms)
(2) Cooling to 33oC is based on extensive laboratory evidence
and two RCTs (HACA, 2002; Bernard et al, 2002)
(3) We can t tell who will have significant post-arrest injury
based
on current technology and clinical factors
(4) the chance to modify neurologic injury is in the acute care of
post-arrest patients – and we don t get a second chanceOur consensus approach Therefore: it is reasonable to not change current practice based on the TTM trial, but rather continue to treat comatose post-arrest patients with a TTM goal temperature of 33oC. However, the TTM trial provides evidence that a more flexible approach is possible – for patients intolerant of 33oC (marked bradycardia, increased bleeding, marked QT prolongation, e.g.) or for patients that clinicians feel uncomfortable with treating to 33oC for other clinical factors, it is acceptable to treat with higher TTM temperature goals, up to 36oC.
Other key part of our approach ALL comatose post-arrest patients should at least receive TTM with a maximum temp goal of 36oC – normothermia as defined by lack of any temperature control is not supported by the growing body of literature. In addition to TTM management in the acute phase (12-24 hours of either 33oC or 36oC TTM), all post arrest patients should receive comprehensive best-practice post arrest care, including aggressive avoidance of fever for up to 48-72 hours following rewarming and avoidance of care withdrawal for at least 72 hours post arrest, as supported in the current AHA guidelines and the TTM trial.
More than care
Post-arrest just hypothermia
is multimodal
Requires a critical care bundle :
Therapeutic hypothermia
Careful hemodynamic management
Coronary intervention if STEMI or
high probability of coronary cause
Neurology consultation and assessmentMore than
Practical just hypothermia
training in post-arrest care
Hypothermia and Resuscitation Training
(HART) course at Penn
Philadelphia – next course October, 2014
Intensive two day CME course in hypothermia
methods, protocols, and applications
Designed for critical care, cardiology or emergency medicine
physicians and nurse leaders – i.e., local champions
Offers hypothermia certification
Workshop design – small course size – held quarterlyHands on simulations Expert faculty proctors Honoring survivors and rescuers Interactive learning
More
TTM inthan just hypothermia
the media
Popular
Science
January, 2009
Freezing the Heart
to Save the Life
Good graphics
showing effects of
coolingMore
TTM inthan just hypothermia
the media
2009
CNN television documentary and book
Features a number of arrest survivorsA closing story:
a telephone call from
a strangerA phone call from far away…
Sitting at home with my kids, I get
a telephone call from a stranger
WeDr. Abella?
have This
a soldier
is Colonel
down, John
Dr. Abella,
hePatton from the
had cardiac
United And
arrest…. States
weAir
need
to Force, calling you
cool him….
from Balad Iraq.Post-arrest hypothermia: an
implementation problem
2008
2011
Many hospitals aren t using the therapy;
other hospitals underuse itBack to the scene: my phone call from a stranger
Case presentation • 33 year-old male soldier found unresponsive and pulseless with agonal respirations • First responders noted an anterior chest wall contusion and a freshly discharged halon fire extinguisher.
Soldier suffered VF arrest from commotio cordis
Team wanted to use therapeutic hypothermia but had no experience
Post-arrest hypothermia: an implementation problem We packed patient in ice, lowered core temp to 33 oC Prepared patient for evaculation
Cooling during international
transport to Germany
Critical care transport via C-17 to
tertiary care military facilityArrival in Germany, maintenance
and rewarming
…. Full recovery of patient, now
returned to his unitCase report now published
Carlson et al, 2013Summary points: the big picture
Conclusions
1. Randomized trials strongly support
hypothermia use for OOH VF arrest
2. Benefit doesn t seem dependant on
method of cooling
3. Evidence based medicine supports
basic protocol of 32-34oC for 12-24 hours
4. Adverse effects of cooling are mild;
bradycardia is common, bleeding less soAcknowledgements
Acknowledgements
Center for Resuscitation Science
Lance Becker
West Philadelphia – Penn campus
Marion Leary
Audrey Blewer
Dave Gaieski
Barry Fuchs
Dan Kolansky
Vinay Nadkarni
Raina Merchant
Robert Berg
Gail Delfin
Marisa Cinousis
Kelsey Sheak
David Buckler
Amit AgarwalYou can also read