Polycystic Liver Disease - Marie Hogan, M.D., Ph.D. Associate Professor of Medicine, Nephrology, Mayo Clinic Rochester
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Polycystic Liver Disease
Marie Hogan, M.D., Ph.D.
Associate Professor of Medicine,
Nephrology, Mayo Clinic Rochester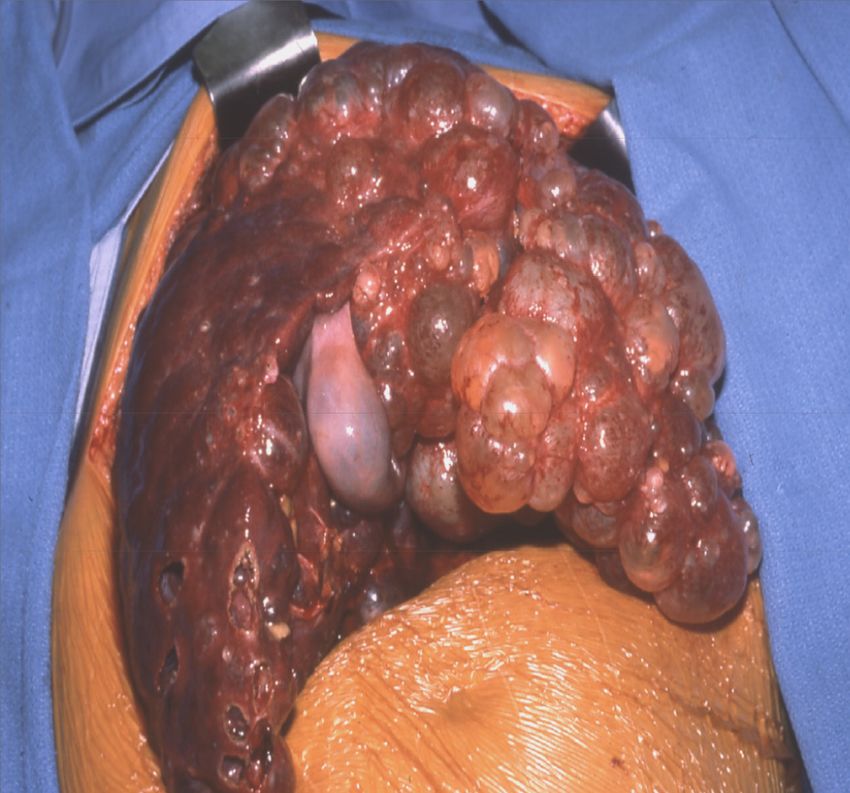
Outline
• Historic
• Natural History
• How do you get liver cysts?
• Symptoms
• Medical Management
• Surgical Management
• New Treatments
pkdcure.org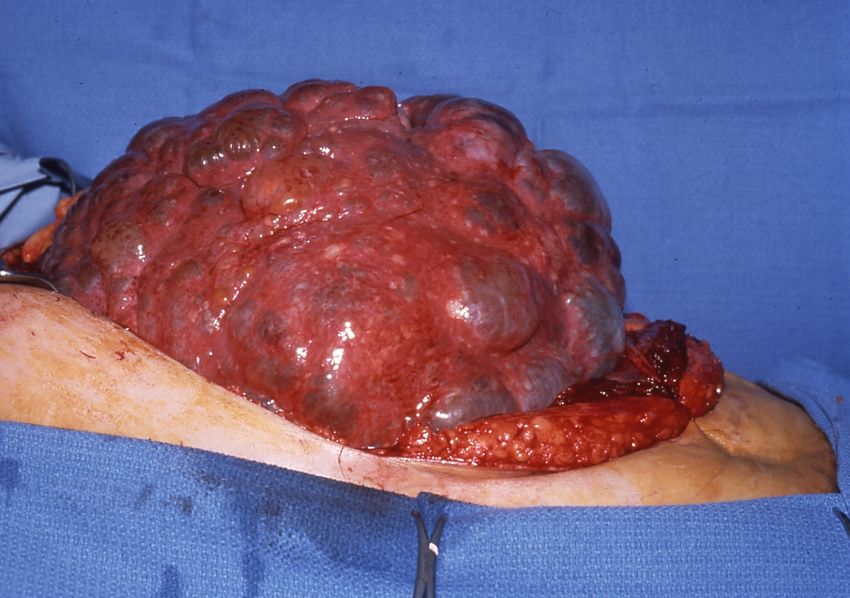
Polycystic Liver Disease
Disease Gene Chromosome Protein Function
ADPKD PKD1 16p13.3 Polycystin1 Membrane
receptor
PKD2 4q21-23 Polycystin2 Calcium
channel
ADPLD PLD1 19 p13.2 GlucosidaseII ER protein
processing
PLD2 6 SEC63 ER protein
processing
pkdcure.org
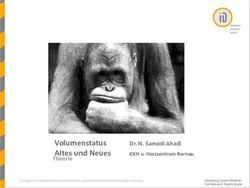
Cystogenesis in ADPLD
Normal PLD
Intralobular ductule
Interlobular duct
Area duct
Segment duct
Right hepatic duct
Common hepatic duct
Common bile duct
CP1047707-3
pkdcure.org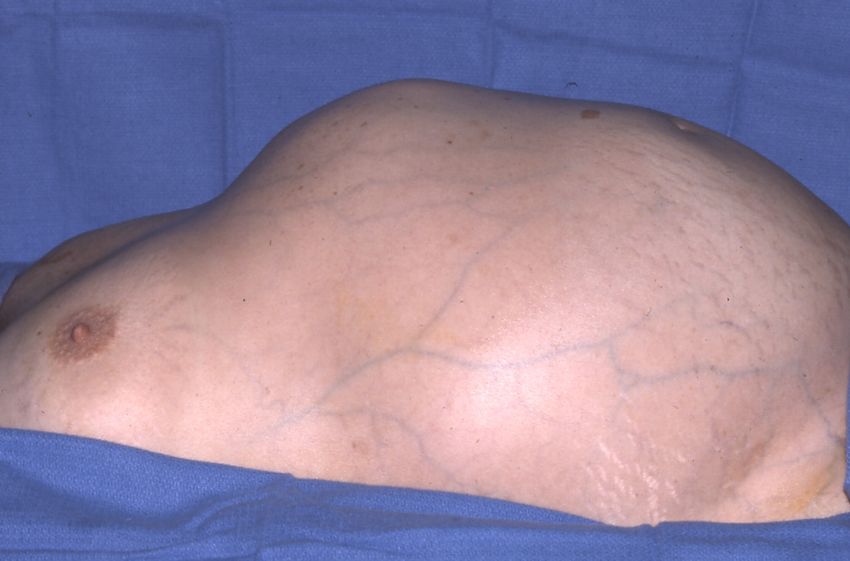
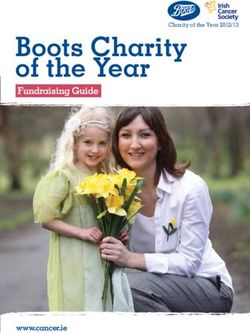
Prevalence of Liver Cysts in
General Population
100
80
60
%
40
20
0
20 40 60 80 >80
Age (yr)
pkdcure.org
PLD in ADPKD Patients
MRI Evaluation of Hepatic Cysts in Early ADPKD: CRISP
Cohort.
• Quantitative MRI scans: 3mm slices
• Prevalence of liver cysts in early ADPKD
• 58% in 15-24yo
• 85% in 25-34yo
• 94% in 35-46yos Bae T et al CJASN 2006;1:64-69.
pkdcure.org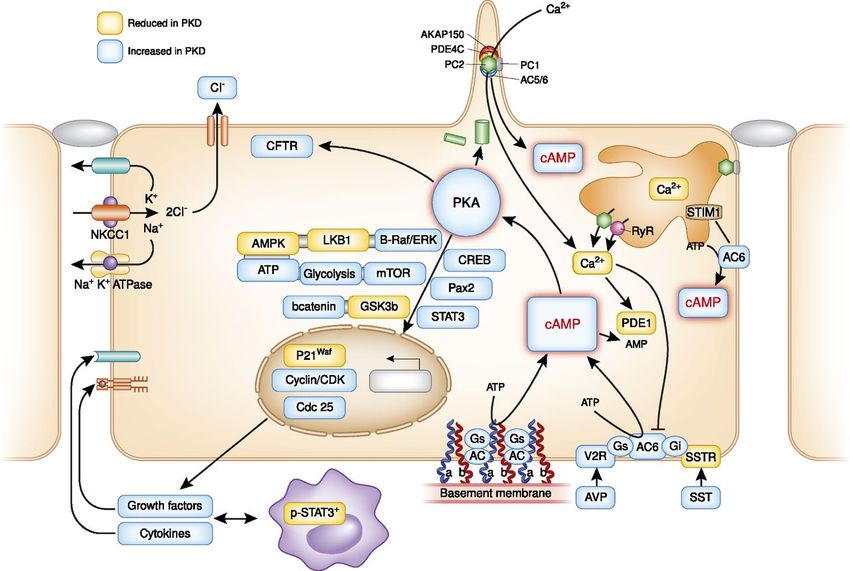
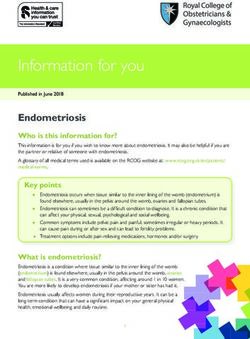
MRI From Four Patients
24yo man liver 46yo man mild
cysts (6.3ml) hepatic cyst (9.3ml)
renal cysts severe renal cysts
(15.4 ml). (1940 ml).
44yo man 30yo woman
hepatic hepatic cysts
cysts(318.7 (2368.8 ml)
ml) but mild and renal
renal cyst cysts (1084.5
burden (37.6 ml).
ml).
Bae, K. T. et al. CJASN 2006;1:64-69
pkdcure.org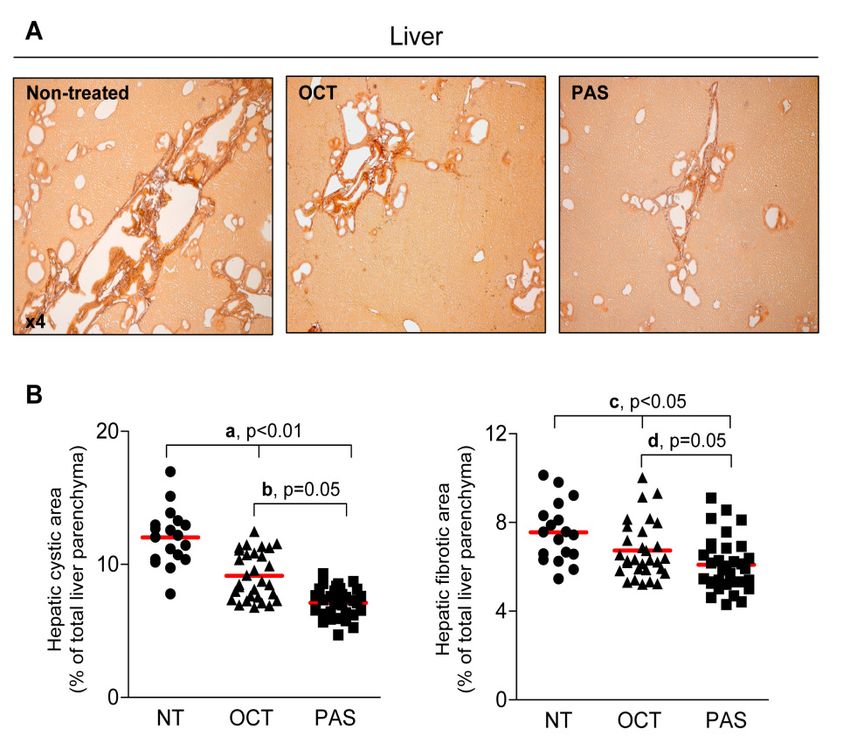
Symptoms of PLD
• Mass Effect (by dominant
cyst/massive PLD)
• Abdominal distension/pain
• Early satiety, heartburn,
emesis
• Malnutrition, loss of
muscle/fat
• Dyspnea, orthopnea
• Change in bowel pattern,
hemorrhoids
• Back pain
• Hernias, uterine prolapse, rib
fractures
• Venous obstruction (hepatic,
IVC, porta)
• Bile duct obstruction
pkdcure.org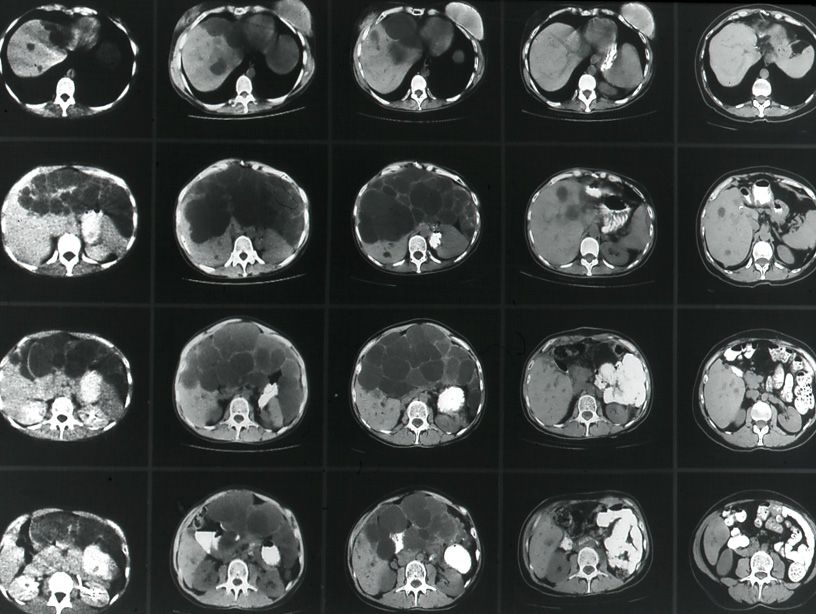
Symptoms of PLD
Complications
– Hemorrhage
– Rupture
– Infection
Rare Associations
– Bile duct dilatation
– Congenital hepatic fibrosis
– Cholangiocarcinoma
pkdcure.org
CRISP & HALT Cohorts:
MR Evaluation of Hepatic Cysts in Early
Disease
• CRISP: C-G GFR >70, quantitative MR scans: 3mm slices
• 58% in 15-24yo
• 85% in 25-34yo
• 94% in 35-46yos
•HALT:
• Women: Men:
• 44% ≤24, 17%
• 68% 25-34 57%
• 84% ≥ 35 79%
Bae T et al (CRISP).CJASN 2006. Chapman A et al (HALT). ASN 2010.
©2011
MFMER |
slide-10Wide Disease Spectrum in PLD:
Hogan et al for HALT
Investigators. Submitted.HALT-A: Wide variability in
Polycystic Liver Disease Severity:
HtLPV also increases,
but then plateaus.
Hogan et al for HALT Investigators. pkdcure.org
Submitted.A. Hepatomegaly (TLV 2677ml) with
larger contribution of LPV
HALT-PKD MRI (2576ml) compared to LCV
(101ml):
images:
B.
Hepatomegaly (11834ml) with larger contribution
of LCV (9806 ml) compared to LPV (2028ml);
C. D.
Splenomegaly (601ml) associated Splenomegaly (542ml) associated wi
with severe PLD (3388ml) with LCV moderate PLD (LV 2082ml,LCV 110ml)
(1044ml);Cyst Infection
• Risk Factors
– Recent abdominal surgery
– Kidney Transplant
– Chronic dialysis
• Symptoms
– Fever + new onset RUQ pain
– Leukocytosis ↑ESR
– ↑ ALP
– Bacteremia
– Cultures of undrained cyst fluid +ve
pkdcure.orgLiver Cyst Infections:
• Risk Factors
• Recent abdominal surgery
• Kidney Transplant
• Chronic dialysis
• Symptoms
• Fever + new onset RUQ pain
• Leukocytosis ↑ESR
• ↑ ALP
• Bacteremia
• Cultures of undrained cyst fluid +ve
pkdcure.orgInfected Kidney & Liver Cysts:
Diagnostic Criteria:
T>38°C x >3 d
Tenderness in kidney/ liver
CRP >5 mg/dl,
Absent intracystic bleeding on CT
•Kidney > Liver
•PET/CT reliably detects cyst infection
•Infected liver cysts require drainage
•US, CT, MRI failed to detect cyst infection in most
cases.
•E.coli commonest (74% all) often B lactam resistant
•Quinolone antibiotics – up to 2 months
Sallée M et al (Necker Hospital). CJASN 2009.
©2011 MFMER | slide-16 Jouret F et al. CJASN 2011. pkdcure.orgNonsurgical Treatment
Options
• Avoid estrogens
• Avoid caffeine
• Caffeine stimulates cAMP
• H2-blocker or H+/K+ ATPase inhibitor
• ↓ secretion rates from unroofed liver cysts, possibly by
inhibiting gastric acidity and secretion of secretin
• Somatostatin analogues
• Long-acting octreotide/ lanreotide
pkdcure.orgSurgical Treatment Options
1. Percutaneous aspiration/sclerosis
2. Fenestration (laparoscopic or open)
3. Hepatic resection/fenestration
4. Liver transplantation
pkdcure.orgpkdcure.org
Alcohol Sclerosis of Liver
Cysts
Success rate:
Primary: 69%
Secondary: 23%
Failure: 8%
Complications:
Major: None
Minor: Transient pain
pkdcure.orgLaparoscopic Fenestration
INTRAOPERATIVE COMPLICATIONS
Hypothermia
Hypercapnia
POSTOPERATIVE COMPLICATIONS
Transient ascites (46%)
SYMPTOMATIC RELIEF
85%
RECURRENCE of SYMPTOMS
73%
Useful for few large cysts
pkdcure.orgMassive PLD
• Focal (preserved liver segments in >80% of patients)
• Parenchymal volume constant
pkdcure.orgMassive PLD Combined
Resection-Fenestration
pkdcure.org-10yrs -3yrs -Pre-op +1 year +3years +10years
Courtesy of Vicente E. Torres.Liver Transplantation for
Massive PLD
pkdcure.orgModel for End-Stage Liver
Disease (MELD)
Numerical system that ranks (from 6 to
40) patients waiting for a liver based
on three lab test results:
– Bilirubin (how effectively the liver excretes
bile)
– INR (prothrombin time, ability to clot
blood)
– Creatinine (kidney function)
pkdcure.orgLiver and Kidney
Transplantation for PLD
•First done 1988
•Malnutrition and failure to thrive
•Baylor/ Dallas Transplant Institute: 14
patients: 1987-2003
•MELD= 15 ± 7.5
•Liver weight 2.6–12.6 kg
•5-year survival for liver transplant considering
all published studies ~ 85%
•Excellent Quality of Life
•Most of the mortality occurring in the first 3
months.
T Ueno. Transplantation. 82 (4) 501-7. 2006
pkdcure.org51yo (59kg) with ADPKD
with 9.1 kg Liver
Wall WJ. NEJM 2007
pkdcure.orgAlternative Treatment
Options
• Hepatic artery embolization
• Endovascular stent
• Transjugular intrahepatic
portosystemic shunt (TIPS)
• La Veen shunt
pkdcure.orgSevere PLD: Hepatic Artery
Embolization
Ubara. AJKD 43: 733, 2004
pkdcure.orgHepatic Artery Embolization:
Pre
Post (2 years)
Ubara. AJKD 43: 733, 2004
pkdcure.orgMolecular Targets
.
Torres V E , and Harris P C JASN 2014;25:18-32Mechanisms of Cyst
Development
Mutations in ADPKD
(PKD1 and PKD2)
Mutations in ADPLD
(PRKCSH and SEC63)
• Defective cell planar polarity
Normal liver • Centrosomal amplification PLD
• Cell cycle dysregulation
• Increased apoptosis
• Increased fluid secretion
• Increased cell proliferation
cAMP elevation pkdcure.orgIn Cholangiocytes, cAMP Facilitates Fluid Secretion & Proliferation
Normal PCK
Basolateral Apical
(blood) (bile)
SSTR2
Somatostatin
Fluid
secretion
[↑cAMP
[↓cAMP] ] SSTR3
Proliferation
Secretin
SSTR5
Cyst growth Masyuk, Gastroenterology, 2007Somatostatin and Its Analogs
SST
SSTR1 SSTR2 SSTR3 SSTR4 SSTR5
T1/2 = 3 min
OCT
SSTR1 SSTR2 SSTR3 SSTR4 SSTR5
T1/2 = 2 h
PAS
SSTR1 SSTR2 SSTR3 SSTR4 SSTR5
T1/2 = 12 h
35Long-Acting Octreotide
Trial Mayo Clinic
Prospective, double blind, placebo controlled (2:1), 42 patients
Octreotide LAR 40 mg IM every 4 weeks
Primary endpoint: % change in liver volume at 12 months (MRI)
Secondary endpoints: % change in kidney and liver/renal cyst
volumes
Patient Characteristics
• Age ≥ 18 years
• PLD associated with ADPKD or isolated ADPLD
• Liver volume >4000 mL or symptomatic due to mass effects
• Not a candidate for or declining surgical intervention
• Serum creatinineStudy Flow Diagram
Hogan, M. C. et al. J Am Soc Nephrol 2010;21:1052-1061
pkdcure.orgLong-Acting Octreotide Trial in
ADPKD:
• Randomized, placebo-controlled, cross-
over study x 6 months
pblind, 1:1 placebo-controlled (6
months) Lanreotide:
Absolute Volume Changes (ml): Liver
n=54
Volume Changes (%)
Liver Kidney
□ Placebo: + 1.6 % □ Placebo: + 3.4 %
■ Lanreotide: - 2.9 % ■ Lanreotide: - 1.5 %
P-valueMAYO OCTREOTIDE TRIAL
Hogan et al. JASN 2010.MAYO OCTREOTIDE TRIAL:
KiDNEY VOLUME
Hogan et al. JASN 2010.Meta-Analysis of 107 PLD Patients
• -5.3% in TLV after 6-12 mo (95% CI: -3.4 to -
7.2%) compared to placebo (p47yrs, treatment
effects of SAs on TLV were significant (-
8.0%, p< 0.001 and -4.2%, p = 0.018), with
largest effect in the younger group
• In the placebo group, young women (≤47
yrs) had the largest growth in TLV (4.9%,
95% CI: 2.7 to 8.1%), whereas mean TLV
did not increase in older women and
men
Gevers et al. Gastroenterology 2013
42.Reduction Of Liver Cyst Burden In Patients Receiving
Continuous OctLAR Therapy.
Patient 1
Decreased 25%
Patient 2 of 10%
Patient 3 13% in TLV.
Hogan M C et al. NDT. 2012;27:3532-9
Ruggenenti, KI, 2005; Van Keimpema. Gastroenterology 2009 Caroli. CJASN. 2010.Therapy with OctLAR over four years
on polycystic liver disease:
• A subgroup of symptomatic PLD patients shows the beneficial
effects in arresting of PLD progression,
• Discontinuation of therapy leads to further organ regrowth.
• WomenPasireotide is more effective than Octreotide in
reducing hepato-renal cystogenesis in rodents PKD &
PLD:
Masyuk T et al Hepatology. 2012
Clinicaltrials.gov NCT1670110
©2011
MFMER |
slide-45Open Label
Lockcyst trial: Extension of Lockcyst
Lanreotide trial: Lanreotide
Mayo: OctLAR
Completed June ALADIN:Italy Nephropathy
2012 3yr f /u
Mayo: OctLAR
Completed
June 2012
RCT
Open label Extension
Completed
ELATE: Octreotide;
Oct+Everolimus
Ruggenenti KI 2005. Chrispijn & Drenth Trials 2011.
Van Keimpena Gastroenterology. Perico Lancet 2013. Hogan JASN 2010. Hogan NDT 2012,Perico et al. Lancet 2013. NCT00309283 N=75
Sirolimus (Rapamycin,
Rapamune®)
• Discovered >30 years ago
• Found in an Easter Island soil sample around 1970.
"Rapamycin" comes from Rapa Nui.
• Anti-cancer activity known since mid-1970s.
• Natural compound made by Streptomyces hygroscopicus,
• Binds FK506 binding protein (FKBP-12) in a molecular
complex that involves the subunit regulatory associated
protein of TOR (RAPTOR), and inhibits mTOR kinase activity.
• Inhibition of mTOR: downregulation of CDK complexes and
p27 (Kip1) accumulation; blocks cell-cycle progression in
late G1/S.
• Inhibits proliferation of endothelial & vascular smooth
muscle cells required for tumor angiogenesis.
pkdcure.orgRetrospective mTOR inhibitor
Studies following Renal
Transplantation:
- 11.9 % + 14.1 %
Qian JASN 22:1769-1771, 2007.
©2011
MFMER |
slide-49mTOR Studies:
Cllinicaltrials.gov pkdcure.orgSummary:
• Liver involvement is common
• Severe PLD is uncommon
– Medical options (not FDA approved)
– Surgical options
– Lifestyle
• Hogan.marie@mayo.edu
pkdcure.orgCaffeine Intake in ADPKD:
• Caffeine Intake is low.
• No correlation with renal volume or GFR
Brazil J Med Biol Research 2012 pkdcure.orgYou can also read