Volumenstatus Altes und Neues - Theorie Dr. N. Samadi Ahadi KKH u. Herzzentrum Bernau - BBNK
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Volumenstatus Dr. N. Samadi Ahadi Altes und Neues KKH u. Herzzentrum Bernau Theorie
Warum? Transport Schmierlösung Regeln Medium Exkretion

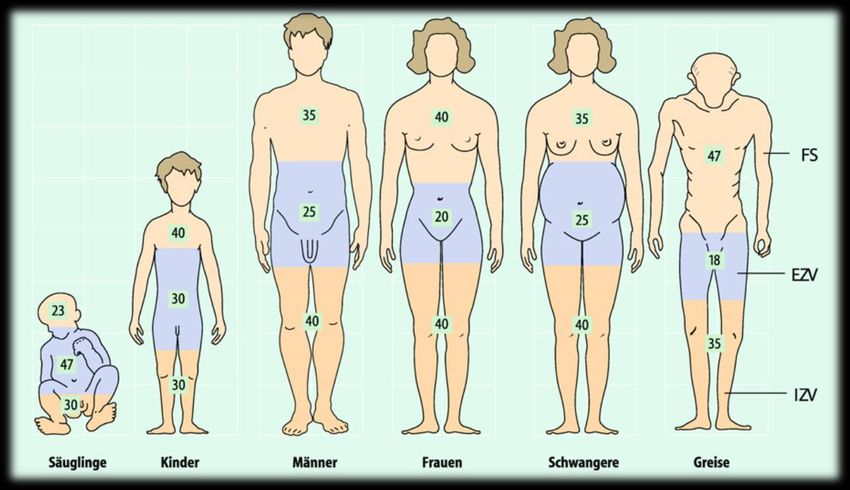
Physiologie
Regulation
Schmidt; (2011) Physiologie des Menschen
Physiologie
15%
85%
http://www.ceufast.com/courses/viewcourse.asp?id=149
Risikofaktoren der Hypovolämie
Geschlecht F>M
Alter>85 Jahre
Mehr als 4 chronische Leiden
Mehr als 4 Medikamente
Bettlägrigkeit
Laxantien-Einnahme
Chronische Infektionen
Lavizzo-Monrey R 1988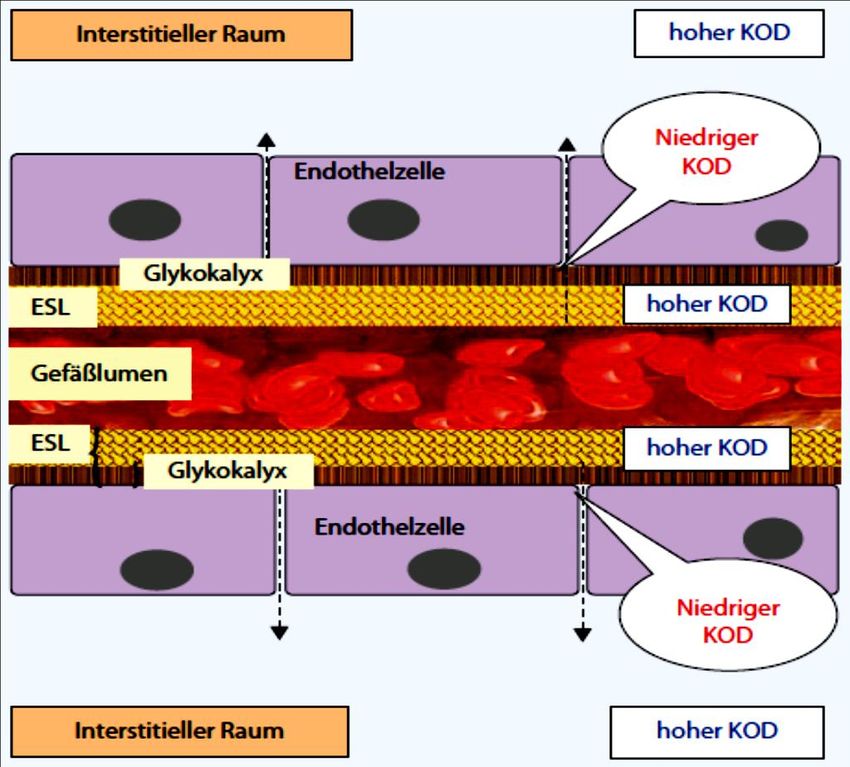
Fluid and Catheter Treatment Trial (FACTT)
Ronald M. Stewart; 2009
Nebenwirkungen der Überwässerung Verschlechterung des Gasaustausches Delir Gastro- und Enteropathie IAP Herzinsuffizienz Wundheilungsstörung Muskelschwäche

Wohin geht die Flüssigkeit?
Adequate Blutvolumen ohne Ödembildung
Komplikationen
Hypervolämie HypovolämieGötter der Medizin Zeus Poseidon
Starling Gleichgewicht
Jv = LpS [(Pc – Pif) – σ (COPc – COPif)]
Aquaporin
niedriger Pi Proteinflux Jv
D. Chappell; 2008Fakt
Die vaskuläre Barriere funktioniert ungeachtet der
Tatsache, dass die interstitielle Proteinkonzentration
der intravasalen nahezu gleicht !
Adamson RH, Lenz JF, Zhang X et al. (2004) Oncotic pressures opposing filtration across non-fenestrated
rat microvessels. J Physiol 557: 889–907
Jacob M, Bruegger D, Rehm M et al. (2007) The endothelial glycocalyx affords compatibility of Starling’s
principle and high cardiac interstitial albumin levels. Cardiovasc Res 73: 575–586
Jacob M, Bruegger D, Rehm M et al. (2006) Contrasting effects of colloid and crystalloid resuscitation
fluids on cardiac vascular permeability. Anesthesiology 104: 1223–1231
Levick JR (2004) Revision of the Starling principle: new views of tissue fluid balance. J Physiol 557: 704
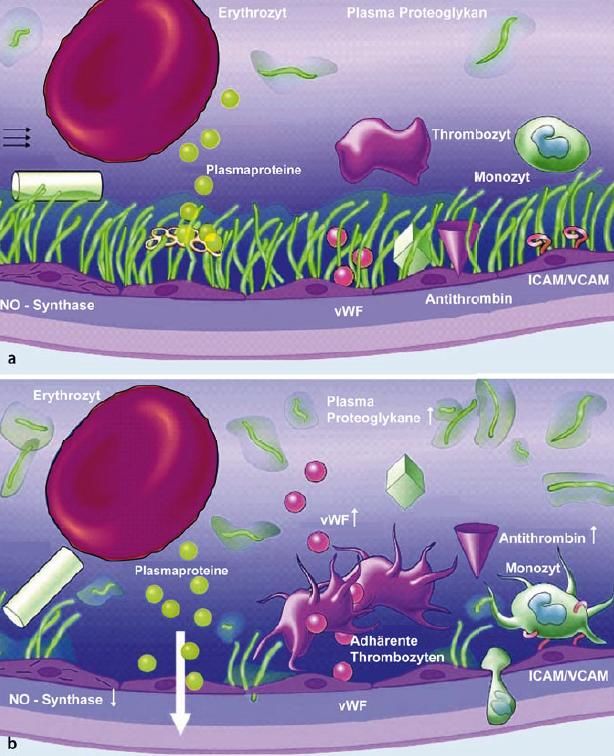
Hu et al(2000); American J Physiology 279, 1724-1736Glykokalyx Chappell D, Jacob M, Hofmann-Kiefer K et al. (2007) Anesthesiology 107: 776–784
Jv = LpS [(Pc – Pif) – σ (COPc – COPg)]
Proteinflux Jv
D. Chappell; 2008ESL & Blutvolumen
Nicht-
zirkulierend
zirkulierend
Rehm M, Haller M, Orth V et al. (2001) Changes in blood volume and hematocrit during acute preoperative volume loading
with 5% albumin or 6% hetastarch solutions in patients before radical hysterectomy. Anesthesiology 95: 849–856
50. Nieuwdorp M, Meuwese MC, Vink H et al. (2005) The endothelial glycocalyx: a potential barrier between health and
vascular disease. Curr Opin Lipidol 16: 507–511
51. Nieuwdorp M, Haeften TW van, Gouverneur MC et al. (2006) Loss of endothelial glycocalyx during acute hyperglycemia
coincides with endothelial dysfunction and coagulation activation in vivo. Diabetes 55: 480–486Physiologie Bruegger D, Jacob M, Rehm M et al. (2005) Am J Physiol Heart Circ Physiol 289: H1993–H1999 Rehm M, Haller M, Orth V et al. (2001) Anesthesiology 95: 849–856
ANP & Volumenregulation
Wen Chen;Cardiovascular Research (2012) 93, 141–151ESL & Blutvolumen
Nicht-
zirkulierend
zirkulierend
Rehm M, Haller M, Orth V et al. (2001) Changes in blood volume and hematocrit during acute preoperative volume loading
with 5% albumin or 6% hetastarch solutions in patients before radical hysterectomy. Anesthesiology 95: 849–856
50. Nieuwdorp M, Meuwese MC, Vink H et al. (2005) The endothelial glycocalyx: a potential barrier between health and
vascular disease. Curr Opin Lipidol 16: 507–511
51. Nieuwdorp M, Haeften TW van, Gouverneur MC et al. (2006) Loss of endothelial glycocalyx during acute hyperglycemia
coincides with endothelial dysfunction and coagulation activation in vivo. Diabetes 55: 480–486Nieuwdorp M, Meuwese MC, Vink H et al. (2005). Curr Opin Lipidol 16: 507–511
Krogh-Zylinder
PO2-Verteilung
Versorgungsbereich einer KapillareZusammenfassung Die Starlingkräfte sind nicht die hauptsächliche Kraft des Volumen-Gleichgewichtes in dem Gewebe. Die neue Sichtweise kann helfen den „low flow lymph paradoxon“ zu lösen. Denn der intraluminale (Interzelluläre) oncotische Druck ist niedriger als der interstitielle . Der Unterschied ist selbst eine Funktion der Filtrationsrate. Die Volumentherapie im klinischen Alltag sollte sich an diesen Tatsachen orientieren. Infusionen sind Medikamente mit der eigenen Wirkungen und Nebenwirkungen.
Praxis Laborwert
ESC Guidelines for the diagnosis and treatment of acute
and chronic heart failure 2012BNP
Torbjørn;Crit Care Med 2008; 36[Suppl.]:S17–S27Ursachen des erhöhten BNP
LVD
Arterielle Hypertonie(Ventrikuläre Hypertrophy)
Myocardial Infarction
Angina
Myocarditis
Primäre pulmonale Hypertonie
Lungenembolie
COPD
Nierenversagen
Sepsis
Myocarditis
Anämie
Leberzirrhose
Alter
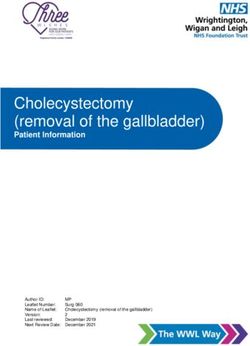
Epaminondas Z.; Heart& Lung® 2008;37:275–285ProBNP Investigation of Dyspnea in the
Emergency Department (PRIDE)
Saif Anwaruddin; Journal of the American College of Cardiology Vol. 47, No. 1, 2006BNP und Niereninsuffizienz
Jae Won Yang, 2008BNP/NT-proBNP in CNI
Schou M et al. Am J Cardiol. 2007;100:1571Y1576NT-ProBNP & Dialyse Clin Nephrol. 2007 Dec;68(6):392-400. Cardiac biomarkers are influenced by dialysis characteristics. Sommerer C, Heckele S, Schwenger V, Katus HA, Giannitsis E, Zeier M. METHODS: Standard chronic hemodialysis lasting 4-5 hs 3 times weekly and using polysulfone dialyzers (high-flux and low-flux) was performed. Blood flow rates varied between 250-350 ml/min. The cTNT levels of 49 chronic hemodialysis patients were measured twice (interval of 6 weeks) before and after a hemodialysis session by a third-generation assay (Elecsys Analyzer, Roche Diagnostics, Mannheim, Germany). NT-proBNP levels were measured with polyclonal antibodies capable of recognizing the N-terminal fragment of BNP. In a follow-up period of 42 months, cardiovascular events and death were assessed. RESULTS: The median concentration of cTNT prior to hemodialysis was 0.024 ng/ml (< 0.001-0.703). All dialysis patients presented high plasma levels of NT-proBNP (median 4,885 pg/ml). Oligoanuric patients had significantly higher cTNT and NT-proBNP levels prior to dialysis compared to patients with normal diuresis (p < 0.0001). cTNT and NT-proBNP levels increased significantly during the hemodialysis sessions in which a low-flux dialyzer was used (p < 0.0001) but remained unchanged when a high-flux dialyzer was utilized. Neither the predialytic nor the interdialytic changes in cTNT and NT-proBNP levels were influenced by blood flow. NT-proBNP levels increased markedly during hemodialysis sessions (p < 0.005) utilizing the low-flux dialyzer. Patients with a non- native fistula had significantly higher predialysis cTNT and NT-proBNP levels (p < 0.05). Patients with cardiovascular events had a significantly higher cTNT and NT-proBNP at the beginning of the study. CONCLUSION: Asymptomatic chronic hemodialysis patients have significantly higher levels of the cardiac biomarkers cTNT and NT-proBNP relative to the general population. The levels are associated with the time of measurement (before and after a hemodialysis session). Dialysis modalities like high-flux dialyzers influence cTNT and NT-proBNP levels and should be taken into account, particularly in patients with acute onset of cardiac ischemia. The elevation of cTNT and NT- proBNP levels after hemodialysis using a low-flux dialyzer are partly due to hemoconcentration. The significant association of cTNT and NT-proBNP with non-native fistulas (catheter or graft) may be due to the chronic inflammation commonly caused by these devices. Both cardiac biomarkers are of prognostic value determining cardiovascular events and death.
BNP & LVH
Autor Patienten Cutoff
Khan et al. 2006 54 with CKD LVH (NT-pro-BNP): 762 pg/ml (sens 63%, spec 67%, PPV 70%,
NPV 57%)
LVH (BNP): 200 pg/ml (sens 60%, spec 71%, PPV
72%, NPV 59%)
deFilippi et al. 207 with LVSD (NT-pro-BNP): 7168 pg/ml (sens 98%, spec
79%)
2005 stages 1 LVH (NT-pro-BNP): 271 pg/ml (sens 76%, spec 60%)
through 5 CKD
David et al, 2007 62 HD LVSD (BNP): ND (sens 94%, spec 21%, PPV 46%,
NPV 83%)
Mark et al 2006 55 HD LVH (BNP): ND (sens 68%, spec 67%, PPV 79%, NPV
53%)
Mallamaci et 212 HD and 34 LVH (BNP): 23.4 pmol/L (sens 62%, spec 88%, PPV
95%, NPV 61%)
al.,2000 PD LVSD (BNP): 38.9 pmol/L (sens 74%, spec 76%, PPV
31%, NPV 95%)Intrakardialer Druck &
Natriuretisches Peptid
Wen Chen;Cardiovascular Research (2012) 93, 141–151NT-ProBNP & Dialyse Erhöht: Kunststoff-shunt Katheter Postdialyse mit Low-Flux-Filter Überwässert Vermindert: Postdialytisch nach High-Flux-Filter Hohe UF
BNP(NT-ProBNP)
Biologische Wirkung
GFR-Steigerung,
Natriurese und Diurese
Vasorelaxation mit Reduzierung der Vor- und Nachlast
Supression von Renin-Angiotensin-Aldosteron
Kardiale Remodeling
Die Interpretation hat nach Bestimmung der NT-ProBNP in klinisch
stabilen Phasen und Einbeziehung historischer Werte zu erfolgen.
• Troughton RW, Lancet 355 : 1126 –1130, 2000
• Jourdain P, The STARS-BNP Multicenter Study. J Am Coll Cardiol 49 : 1733 –1739, 2007ESC Guidelines for the diagnosis and treatment of acute
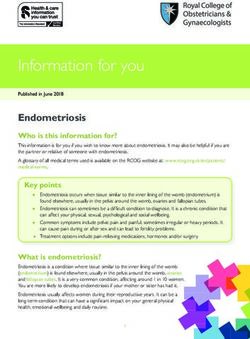
and chronic heart failure 2012Praxis Bildgebung Röntgen
Röntgenthorax • Erweiterte OL-Gefäße • Kardiomegalie • Interstitielles Ödem • Erweiterte pulmonale Gefäße • Pleuraerguß • Alveoläre Ödeme • Prominente VCS • Kerley Linie
Prevalence of Negative Chest Radiography Results
in the Emergency Department Patient With
Decompensated Heart Failure
Sean P. Collins,Praxis Bildgebung Ultraschall
VCI
VCIIndex VCI index = D exp. - D insp/D exp. X 100
Nakao S, Come P, (1987) Am J Cardiol 59:125–132
ZVD und VCI
IVC cm Atemabhängigkeit ZVD
50% 6-10
1,5-2,5 2,5 2,5 20
ACEP ;(2008); Ann. Emergency medicineVCI-Messung Versichern Sie sich vom richtigen Gefäßauswahl Der Meßpunkt ist 2 cm unterhalb der V. Hepatica Denken Sie an die Differentialdiagnosen der dilatierten VCI(Perikardtamponade, MI, TI) Bei intubierten Patienten ist der Atemabhängige Kollaps antizyklisch VCI-Kollaps bei beatmeten Volumensensiblen Patienten beträgt 12-18% Denken Sie an die Lungensonographie
Praxis Lunegensonographie
A-Linie Normalbefund
Ultraschall D. Lichtenstein; Am. J. Respir. Crit. Care Med. November 1, 1997 vol. 156 no. 5 1640-1646
A-Linie
B-LinieLungensonographie
B-Linien-Score
Rechts Links
Mittlere Vordere MCL Parasternal ICR Parasternal MCL Vordere Mttlere
Axillarlinie Axillarlinie Axillarlinie Axillarlinie
II
III
IV
V
Jambrik et al, 2004B-Linien-Score
B-Line -Score
Score Zahl der B-Linien Extravaskuläre
Lungenwasser
0 30 Schwer
Picano E.:J Am Soc Echocardiogr 2006;19:356-363Lungenödem
Lungenöedem
Hämodynamisch vs Hyperpermeabilität
Hämodynamisch Hperpermeabilität
Lungenfeld Oben Unten
B-Linie Anterior Posterior
Symmetrie Bilateral Asymmetrisch
Dynamik Verschwindet nach
Therapie
Konsolidierung keine Sporadisch
Irreguläre Pleuralinie
Lungen- Erhalten Vermindert
verschieblichkeitPneumonie
Lungenembolie
Die zehn Zeichen der Lungensonographie
The bat sign
The A-line
Lung sliding
The quad sign
The sinusoid signDie zehn Zeichen der Lungensonographie The tissue-like sign The shred sign The B-line (& lung rockets) The stratosphere sign The lung point
Das Auge kann nicht sehen
was der Geist nicht kennt!
Leonardo DavinciLichtenstein DA, Mezière. CHEST July 2008 vol. 134 no. 1 117-125
Seashore Stratosphere
PneumothoraxPicano E.:J Am Soc Echocardiogr 2006;19:356-363
Lori B.; Journal of the American College of Cardiology Vol. 50, No. 25, 2007
Wasser: Ein Toxin? Wettbewerb: Frau stirbt nach Wett- Trinken um Nintendo Wii! Der Trink-Wettbewerb eines Rundfunksenders um eine Wii Spielkonsole von Nintendo hat eine junge US-Bürgerin das Leben gekostet. Sie starb an einer Wasservergiftung.
Anämie und Herzinsuffizienz
M. Kosiborod;AmJ Med. 2003Faktoren gegen Ödembildung
Niedrige Compliance der Interstitium im negative Druckbereich
-3 mmHg
Interstitielles Gel
Proteoglycanfilamente im Interstitium
Verhindert als Gitternetz die Volumenzunahme
Erlaubt als Platzhalter das Herausfließen des Wassers bei zu viel
Volumenansammlung
Gesteigerter Lymphabfluß(10-50 fach) bis 7mmHg Ausgleich
„Washdown“-Effekt der Proteine bis 7mmHg Ausgleich
Gesamtausgleichskapazität beträgt 17 mmHg oder das doppelte des
peripheren VenendrucksProBNP Investigation of Dyspnea in the
Emergency Department (PRIDE)
Saif Anwaruddin; Journal of the American College of Cardiology Vol. 47, No. 1, 2006You can also read