Understanding Cancer in the Liver - A guide for people affected by primary liver cancer or secondary cancer in the liver
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Understanding
Cancer in the Liver
A guide for people affected by primary liver
cancer or secondary cancer in the liver
Cancer
information
www.cancercouncil.com.auUnderstanding Cancer in the Liver A guide for people affected by primary liver cancer or secondary cancer in the liver First published October 2007. This edition July 2014. © Cancer Council Australia 2014. ISBN 978 1 925136 32 6. Understanding Cancer in the Liver is reviewed approximately every two years. Check the publication date above to ensure this copy is up to date. Acknowledgements This edition has been developed by Cancer Council NSW on behalf of all other state and territory Cancer Councils as part of a National Publications Working Group initiative. We thank the reviewers of this booklet: A/Prof Vincent Lam, Sydney Medical School Hepatobiliary, Pancreatic and Transplant Surgeon, Westmead Hospital, NSW; Prof Peter Angus, Medical Director, Director of Gastroenterology and Hepatology and Professorial Fellow, Austin Hospital and University of Melbourne, VIC; Jenny Berryman, Consumer; Ann Bullen, Cancer Care Coordinator, Royal Brisbane and Women’s Hospital, QLD; Prof Jonathan Fawcett, Director, Queensland Liver Transplant Service, Professor of Surgery, University of Queensland, QLD; Dr Dan Madigan, Interventional Radiologist, Royal Adelaide Hospital, SA; Dr Monica Robotin, Medical Director, Cancer Council NSW; and Dr Simon So, Interventional Radiologist, Westmead Hospital, NSW. Some of the information from previous editions of this booklet was sourced from Macmillan Cancer Care, UK. Editor: Laura Wuellner. Designer: Eleonora Pelosi. Printer: SOS Print + Media Group. Note to reader Always consult your doctor about matters that affect your health. This booklet is intended as a general introduction to the topic and should not be seen as a substitute for medical, legal or financial advice. You should obtain appropriate independent professional advice relevant to your specific situation and you may wish to discuss issues raised in this book with them. All care is taken to ensure that the information in this booklet is accurate at the time of publication. Please note that information on cancer, including the diagnosis, treatment and prevention of cancer, is constantly being updated and revised by medical professionals and the research community. Cancer Council Australia and its members exclude all liability for any injury, loss or damage incurred by use of or reliance on the information provided in this booklet. Cancer Council NSW Cancer Council is the leading cancer charity in NSW. It plays a unique and important role in the fight against cancer through undertaking high-quality research, advocating on cancer issues, providing information and services to the public and people with cancer, and raising funds for cancer programs. This booklet is funded through the generosity of the people of NSW. To make a donation to help defeat cancer, visit Cancer Council’s website at www.cancercouncil.com.au or phone 1300 780 113. Cancer Council NSW 153 Dowling Street, Woolloomooloo NSW 2011 Cancer Council Helpline 13 11 20 Telephone 02 9334 1900 Facsimile 02 9334 1741 Email feedback@nswcc.org.au Website www.cancercouncil.com.au ABN 51 116 463 846
Introduction This booklet has been prepared to help you understand more about cancer that affects the liver. Many people feel shocked and upset when told they have primary liver cancer or secondary cancer in the liver. We hope this booklet will help you, your family and friends understand how cancer in the liver is diagnosed and treated. We also include information about support services. We cannot give advice about the best treatment for you. You need to discuss this with your doctors. However, we hope this information will answer some of your questions and help you think about other questions to ask your treatment team. This booklet does not need to be read from cover to cover – just read the parts that are useful to you. Some medical terms that may be unfamiliar are explained in the glossary. You may also like to pass this booklet to your family and friends for their information. If you’re reading this book for someone who doesn’t understand English, let them know that Cancer Council Helpline 13 11 20 can arrange telephone support in different languages. They can also call the Translating and Interpreting Service (TIS) direct on 13 14 50.
Contents What is cancer?................................................................. 4 The liver.............................................................................. 6 Key questions.................................................................. 8 What is primary liver cancer?.............................................................. 8 What are the risk factors?................................................................... 8 Can primary liver cancer spread?....................................................10 What is secondary cancer in the liver?.............................................11 What are the symptoms?................................................................12 How common is cancer in the liver?................................................13 Diagnosis....................................................................... 14 Blood tests.......................................................................................... 14 Scans (imaging tests).......................................................................... 15 Biopsy...........................................................................................18 Further tests........................................................................................ 20 Staging cancer in the liver................................................................... 21 Prognosis............................................................................................ 22 Which health professionals will I see?................................................. 23 Key points........................................................................................... 25 Making treatment decisions........................................... 26 Talking with doctors............................................................................ 26 A second opinion................................................................................ 27 Taking part in a clinical trial................................................................. 27 Treatment......................................................................... 28 Surgery................................................................................................ 28
Tumour ablation................................................................................... 34 Chemotherapy..................................................................................... 36 Biological therapy................................................................................ 38 Radioembolisation (selective internal radiation therapy)..................... 39 Endoscopic stent placement............................................................... 40 Palliative treatment.............................................................................. 41 Key points........................................................................................... 42 Looking after yourself..................................................... 43 Relationships with others.................................................................. 44 Life after treatment.............................................................................. 45 Seeking support.............................................................. 47 Practical and financial help............................................................... 47 Talk to someone who’s been there...................................................... 47 Caring for someone with cancer................................... 49 Useful websites...........................................................50 Question checklist........................................................... 51 Glossary........................................................................... 52 How you can help............................................................ 56
What is cancer?
Cancer is a disease of the cells, which are the body’s basic building
blocks. The body constantly makes new cells to help us grow,
replace worn-out tissue and heal injuries. Normally, cells multiply
and die in an orderly way.
Sometimes cells don’t grow, divide and die in the usual way. This
may cause blood or lymph fluid in the body to become abnormal, or
form a lump called a tumour. A tumour can be benign or malignant.
Benign tumour – Cells are confined to one area and are not able
to spread to other parts of the body. This is not cancer.
Malignant tumour – This is made up of cancerous cells, which
have the ability to spread by travelling through the bloodstream or
lymphatic system (lymph fluid).
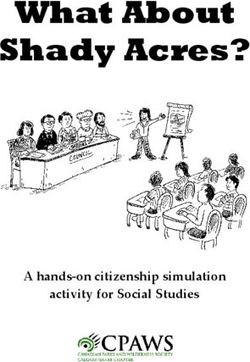
How cancer starts
Normal cells Abnormal Angiogenesis
cells
Boundary
Lymph vessel
Blood vessel
Normal cells Abnormal cells Abnormal cells Malignant or
multiply invasive cancer
4 Cancer CouncilThe cancer that first develops in a tissue or organ is called the
primary cancer. A malignant tumour is usually named after the
organ or type of cell affected.
A malignant tumour that has not spread to other parts of the
body is called localised cancer. A tumour may invade deeper
into surrounding tissue and can grow its own blood vessels
(angiogenesis).
If cancerous cells grow and form another tumour at a new site,
it is called a secondary cancer or metastasis. A metastasis keeps
the name of the original cancer. For example, liver cancer that
has spread to the bones is still called liver cancer, even though the
person may be experiencing symptoms in the bones, while breast
cancer that has spread to the liver is still called breast cancer.
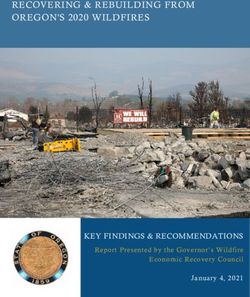
How cancer spreads
Primary cancer
Local invasion
Angiogenesis –
tumours grow their
own blood vessels
Lymph vessel
Metastasis –
cells invade other
parts of the body via
blood vessels and
lymph vessels
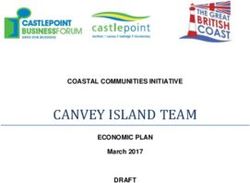
What is cancer? 5The liver
The liver is the largest organ inside the body. It is on the right
side of the tummy area (abdomen), next to the stomach. It
is found under the ribs, just beneath the right lung and the
diaphragm. The diaphragm is a sheet of muscle that separates
the chest from the abdomen.
The liver is made up of two sections: the right and left lobes.
Blood flows into the liver from the hepatic artery and the portal
vein. Blood from the hepatic artery carries oxygen, while blood
from the portal vein carries nutrients and waste products (toxins).
The liver performs several important functions including:
• producing bile to help dissolve fat so it can be easily digested
• converting sugar and fat into energy
• storing nutrients
• making proteins and chemicals the body needs
• helping the blood to clot
• breaking down substances, such as alcohol and drugs,
and getting rid of waste products.
Unlike other internal organs, the liver can usually repair itself.
It can function even if only a small part of it is working. After
surgery or injury, a healthy liver can grow back to normal size
in 6–8 weeks.
Bile is made in the liver and is stored in the gall bladder. When
needed, bile is released into the bowel to help break down fats.
6 Cancer CouncilThe liver
Lung
Hepatic vein Diaphragm
Liver (left)
Liver (right)
Stomach
Gall bladder
Hepatic artery
Pancreas
Common
bile duct
Portal vein
The liver 7Key questions
Q: What is primary liver cancer?
A: This is when a malignant tumour starts in the liver. There are
different types of primary liver cancer:
• Hepatocellular carcinoma (HCC) – starts in the
hepatocytes, the main cell type in the liver. HCC, also called
hepatoma, is the most common type of primary liver cancer.
• Cholangiocarcinoma – starts in the cells lining the
bile ducts, which connect the liver to the bowel and the
gall bladder. It is also called bile duct cancer.
• Angiosarcoma – a rare type of liver cancer starting in the
blood vessels. It usually occurs in people over 70.
Q: What are the risk factors?
A: The majority of liver cancer cases are related to long-term
(chronic) infection caused by the hepatitis B or C viruses.
Other causes of liver cancer aren’t always known, but some
factors that increase the risk include:
• liver scarring (cirrhosis) due to: hepatitis B or C,
alcohol, fatty liver disease or genetic disorders, such as
haemochromatosis or alpha 1-antitrypsin deficiency
• type 2 diabetes
• high alcohol consumption
• eating a high-fat diet and/or being overweight or obese
• smoking tobacco
• exposure to certain chemicals or substances (such as
aflatoxins, vinyl chloride and arsenic).
8 Cancer CouncilThe link between hepatitis and liver cancer
About eight in ten of HCC cases worldwide are attributable
to chronic hepatitis infection. In Australia, hepatitis C and
hepatitis B infections are the biggest known risk factors for
primary liver cancer.
It’s estimated that more than a third of the world’s population
has been infected with the hepatitis B virus. People can spread
either type of hepatitis without knowing they’re infected.
Hepatitis is spread by contact with infected blood, semen,
or other body fluids. Spread can occur through sex with an
infected partner or sharing personal items, such as razors or
toothbrushes, with an infected person.
The most common way that hepatitis B is spread is during
birth, from mother to baby. Although the infection usually goes
away (is cleared) in adults, if hepatitis is acquired in infancy or
early childhood, it can lead to chronic hepatitis infection.
Chronic infection with hepatitis B affects the liver cells
(hepatocytes). This stimulates the body’s immune system
to attack the virus. The immune response causes liver
inflammation, which can lead to ongoing damage and can
cause liver cancer.
People with chronic hepatitis infection often develop cirrhosis,
which increases the risk of liver cancer.
Key questions 9To reduce the spread of hepatitis B and the incidence of
primary liver cancer, all at-risk people should be vaccinated
against the virus. These include:
• migrants from South-East Asia, Africa and the Pacific Islands
• sexually active partners of infected individuals
• people in the same household as someone with hepatitis B
• recipients of blood products
• infants and children (as part of Australia’s national
immunisation program).
Vaccination is not effective if you are already infected with
the virus. In this case, you need regular monitoring to ensure
you don’t develop health problems, including liver cancer.
If you are concerned about hepatitis, contact your doctor for
more information.
Q: Can primary liver cancer spread?
A: If primary liver cancer isn’t found in its early stages, or if
treatment is unsuccessful, it can spread. It typically spreads
to other parts of the liver first, then the lungs, lymph nodes
and bones.
The two most common ways that liver cancer spreads are
through the bloodstream or the lymphatic system. The
lymphatic system is part of the body’s defence system against
infection and disease. It includes a network of thin lymph
vessels, which carry a clear fluid called lymph to and from
tissues, before emptying it into the bloodstream.
10 Cancer CouncilQ: What is secondary cancer
in the liver?
A: Secondary cancer in the liver is cancer that started in another
part of the body but has spread (metastasised) to the liver.
Most cancers can spread to the liver. Cancers that start in
the digestive system (including cancers of the oesophagus,
stomach, pancreas and large bowel) are most likely to
spread to the liver. This is because blood cells flow from the
digestive organs through the liver, and cancerous blood cells
can get stuck (lodge) in the liver.
Melanoma and cancers of the breast, ovary, kidney and lung
can also metastasise to the liver.
Secondary cancer in the liver is sometimes found at the same
time that the primary cancer is diagnosed. However, it can
also be diagnosed soon after the primary cancer, or it may be
diagnosed months or years after someone has been treated
for primary cancer.
It could also be diagnosed before the primary cancer is
found. If other tests don’t show what the primary cancer is,
this is called cancer of unknown primary (CUP).
If you have secondary cancer in the liver, it may be useful to
read information about the primary cancer, or about CUP
if the primary cancer is unknown. Call 13 11 20 or go to your
local Cancer Council website to access relevant publications.
Key questions 11Naming secondary cancers
A secondary cancer is named cancer with liver secondaries,
after the primary site where colorectal metastasis,
it began. metastatic bowel cancer or
advanced bowel cancer.
For example, bowel cancer that
has spread to the liver is still In this booklet, we use the term
called bowel cancer. To indicate ‘secondary cancer in the liver’
that the cancer has spread, to refer to any cancer type that
doctors may call it bowel has spread to the liver.
Q: What are the symptoms?
A: Primary liver cancer doesn’t tend to cause symptoms in
the early stages, but they may appear as the cancer grows
or becomes advanced. Secondary liver cancers may cause
similar symptoms.
Symptoms can include:
• weakness and tiredness (fatigue)
• pain in the upper right side of the abdomen
• severe abdominal pain
• appetite loss and feeling sick (nausea)
• weight loss
• yellowing of the skin and eyes (jaundice)
• pale bowel motions
• swelling of the abdomen (ascites)
• fever.
12 Cancer CouncilQ: How common is cancer
in the liver?
A: Primary liver cancer is one of the less common cancers in
Australia. About 1400 people are diagnosed with it every
year. It is more than twice as common in men, and the
average age at diagnosis is 66.
The incidence of primary liver cancer is increasing, mainly
because the rate of hepatitis infection is increasing, and more
people are developing serious damage from fatty liver disease.
HCC, the most common type of primary liver cancer, is
common in Asia, Mediterranean countries and Africa due
to the high rates of chronic hepatitis B infection. In Australia,
it is more common in migrants from Vietnam, Hong Kong
and Korea – countries where hepatitis B infection is prevalent.
Secondary cancer in the liver is much more common than
primary liver cancer. It occurs about 20 times more often,
with about 28,000 people in Australia diagnosed every year.
Key questions 13Diagnosis
Primary liver cancer and secondary cancer in the liver are
diagnosed using a number of tests. These include blood tests
and scans. Tissue examination (biopsy) is rarely done.
Blood tests
You will probably have a blood test to check how well the liver is
working (liver function) and how well your blood clots. You may
also have liver function tests before, during and after treatment.
If primary liver cancer is suspected, you will have blood tests to
check for hepatitis B or C and various genetic problems. You may
need a blood test to check the level of certain chemicals known
as tumour markers, which are produced by cancer cells and can
help identify some types of cancer. The tumour markers used to
diagnose primary liver cancer include:
• alpha-fetoprotein (AFP)
• cancer antigen 19-9 (CA19-9)
• carcinoembryonic antigen (CEA) – this is also helpful in
diagnosing secondary cancer that has spread from the large bowel.
Tumour markers do not rise in all people with cancer. Also, some
conditions, such as pregnancy, hepatitis and jaundice, can increase
tumour marker levels without cancer being present. If the markers
are high due to cancer, they should fall if the treatment works.
After blood tests, other tests will need to be done to confirm
your diagnosis of primary liver cancer or secondary cancer in
the liver.
14 Cancer CouncilScans (imaging tests)
You will have at least one of these scans, but you may have more
than one if the doctor needs further information about the cancer.
Ultrasound
An ultrasound is the most common scan used to look for primary
liver cancer. It’s often used to monitor high-risk patients, such as
people with cirrhosis.
The scan uses soundwaves to create a picture of a part of your body.
It can show the size and location of abnormal tissue in your liver.
During the ultrasound, you will lie down and a gel will be spread
over your abdomen to help conduct the soundwaves. A small
paddle-shaped device called a transducer is then moved over the
area. It creates soundwaves that echo when they meet something
dense, like an organ or tumour.
The soundwaves are sent to a computer and turned into a picture.
This process takes about 15 minutes and is painless.
If a solid lump is found, the scan will help show whether it is
cancer. Non-cancerous (benign) tumours in the liver can also be
found during an ultrasound.
You will be asked to not eat or drink for about four hours before
the ultrasound.
Diagnosis 15CT scan
The CT (computerised tomography) scan is a type of x-ray that
takes three-dimensional pictures of several organs at the same
time. It helps doctors make a diagnosis and see if the cancer has
spread. It can also help doctors plan surgery.
The test usually takes 10–30 minutes. You will need to drink
a liquid dye (contrast) or have an injection of contrast into a
vein beforehand to make the pictures clearer. The injection may
be uncomfortable and the dye may briefly make you feel hot
and sweaty. Some people can’t have this scan because of poorly
functioning kidneys or an allergy to the contrast (see below).
In this case, a different scan will be arranged.
You will lie on a table while the CT scanner, which is large and
round like a doughnut, takes the pictures. The scan itself is painless.
Some people are allergic to the contrast used in a CT or MRI scan.
If you have any known allergies, let your doctor know in advance.
You should also tell your health care team if you have a pacemaker
or other metallic device in your body. These may interfere with the
MRI scan.
MRI scan
An MRI (magnetic resonance imaging) scan uses both a magnetic
field and radio waves to take detailed cross-sectional pictures of
the body.
16 Cancer CouncilThese show the extent of the tumour and whether it is affecting
the main blood vessels around the liver. The pictures are taken
while you lie on a table that slides into a metal cylinder – a large
magnet – that is open at both ends. You may be given an injection
of contrast into your veins to make the pictures clearer.
An MRI is painless but some people find that lying in the cylinder is
too confined (claustrophobic) and noisy. If you feel uncomfortable,
let your doctor or nurse know. They can give you medication to
ease this feeling or earplugs to reduce the noise level. You can also
usually take someone into the room with you for company.
I had various scans when I was diagnosed with primary
liver cancer. At first, I found the MRI was frightening, going
into the cylinder head first and having to hold my breath.
But now when I have this scan during check-ups, I count to
myself. This helps me feel more in control. Robyn
PET-CT scan
A positron emission tomography (PET) scan combined with a
CT scan (see page 16) is a type of imaging test available at some
major metropolitan hospitals. It produces a three-dimensional
colour image that may show where cancers are in the body.
PET scans are most commonly used for secondary liver cancers,
such as bowel cancer or melanoma that have spread to the liver.
They are not often used to detect primary liver cancers.
Diagnosis 17For the PET scan, you will be injected in the arm with a glucose
solution containing a small amount of radioactive material. It
takes 30–90 minutes for the solution to go through your body.
During this time you will be asked to sit quietly.
Your whole body will then be scanned for high levels of
radioactive glucose. Cancer cells show up brighter on the scan
pictures because they are more active and take up more of the
glucose solution than normal cells.
During PET scans, you will be exposed to radioactive material, but
doses are low and generally not harmful. The nuclear medicine staff
who perform the scan will discuss this with you.
Biopsy
A biopsy involves removing a small amount of tissue to examine
under a microscope. This can sometimes show if the cancer in
your liver is a primary or secondary cancer. A biopsy is usually
done for:
• people without liver cirrhosis
• people who have cirrhosis but have other inconclusive or
abnormal test results
• before surgery or other treatment, if there is uncertainty about
the diagnosis.
A biopsy may not be needed if you are able to have a transplant
(see page 35).
18 Cancer CouncilBefore a biopsy, you may have a test to check how well your blood
clots. This is because the liver contains many blood vessels.
Biopsy is done either by fine needle aspiration or laparoscopy:
Fine needle aspiration
You will have a local anaesthetic to numb the area, then a thin
needle is passed through the skin into the tumour. An ultrasound or
CT scan will be done at the same time to help the doctor guide the
needle. Cells are drawn into the needle and removed.
Afterwards, you will stay in hospital for a few hours. If there is a
high risk of bleeding, you may need to stay overnight.
Sometimes the results of this biopsy are not clear and it will need
to be repeated.
Laparoscopy
This operation is also called keyhole surgery. It allows the
doctor to look at the liver and surrounding organs using a thin
tube containing a light and a camera (a laparoscope). It is often
done if your doctor thinks the cancer may be in other areas of
the body.
A laparoscopy is done under general anaesthetic. A small cut is
made in your lower abdomen for the laparoscope to be inserted.
During the procedure, carbon dioxide gas is used to increase
the size of your abdomen to make space for the surgeon to see.
Diagnosis 19The surgeon can take tissue samples, then after the laparoscope
is removed, the small cut is closed with a couple of stitches.
The most common risks of laparoscopy are wound infection
and bruising. There is a slight risk of bleeding, but this is rare.
The carbon dioxide can also cause shoulder pain and wind for
a few days.
Usually you will need to stay in hospital overnight for monitoring.
Some people need to stay in hospital for a few days.
Further tests
If you have not been diagnosed with cancer and the tests
described on pages 14–19 show you have secondary cancer in the
liver, you may need further tests to find out where the primary
cancer started.
Some people have:
• an examination of the bowel (colonoscopy), the stomach
(endoscopy) and, for women, the breasts (mammogram)
• blood tests to look for different tumour markers
• a urine test to check the kidneys or bladder
• other imaging tests, such as a PET-CT scan, to see different parts
of the body.
In other cases, it will be clear where the primary cancer began, as
you may have been diagnosed and treated for cancer in the past.
This is common for people who have bowel cancer.
20 Cancer CouncilICG test
An indocyanine green During an ICG test, green dye
(ICG) test may be done for is injected into the blood. Over
people who have primary liver the next 15 minutes, readings
cancer and cirrhosis. The test are taken using a probe placed
helps surgeons assess how well on the finger. The probe
the liver is functioning and measures how quickly the
determine if surgery is a liver clears the dye from the
treatment option. bloodstream.
ICG may be done before If the dye is cleared quickly,
surgically removing part of the this shows that the liver is
liver. This is because healthy working well. However, if it is
people can withstand an slow, it may be too dangerous
operation (the liver may regrow to remove parts of the liver. In
during recovery), but a person this case, the medical team
with cirrhosis has liver damage will discuss other available
that can impair liver regrowth. treatment options.
Staging cancer in the liver
The tests described in this chapter will show whether you have:
• primary liver cancer
• primary liver cancer that has spread
• secondary cancer that has spread to the liver from elsewhere.
Working out whether the cancer has spread from the primary
cancer site – and if so, how far – is called staging. This helps your
doctor recommend the best treatment for you.
Diagnosis 21Ask your doctor to explain more about the stage of the cancer and
how it relates to your diagnosis and treatment.
The different stages of cancer are based on how far away from the
original tumour site the cancer is found. Different types of cancer
have different staging systems. Secondary cancers in the liver are
staged using the system relating to the primary cancer.
In primary liver cancer, generally stage 1 and stage 2 tumours are
confined to the liver. Usually stage 3 and stage 4 describes cancer
that has spread away from liver.
Prognosis
Prognosis means the expected outcome of a disease. You may wish
to discuss your prognosis with your doctor, but it is not possible
for any doctor to predict the exact course of your disease. Factors
used to assess your prognosis include:
• test results
• the type of cancer, where it is in the body, and the rate of growth
• the treatment available
• how well you respond to treatment
• your age, fitness and medical history.
Doctors often use numbers (statistics) when considering someone’s
prognosis. Statistics reflect the typical outcome of disease in large
numbers of patients. While statistics give doctors a general idea
about a disease, they won’t necessarily reflect your situation.
22 Cancer CouncilLiver transplantation or surgical resection (removal of the
diseased section of the liver) may be an option to treat some
people with primary liver cancer. These procedures may offer
the chance of a cure.
Other treatments for primary liver cancer and secondary cancer in
the liver may enable you to live for much longer than if you were
to have no treatment.
Which health professionals will I see?
Your general practitioner (GP) will arrange the first tests to
assess your symptoms. If these tests do not rule out cancer, you
will probably be referred to a gastroenterologist who will organise
further tests for you and advise you about treatment options.
You may need to see other specialists, such as a surgeon or
a medical oncologist, who can discuss the different types of
treatment with you.
A range of health professionals who specialise in different
aspects of your treatment will care for you. This is called a
multidisciplinary (MDT) team, and includes doctors, nurses and
allied health professionals, such as a physiotherapist and dietitian.
Some people in non-metropolitan areas will have to travel to
appointments with specialists. Your GP can be kept informed of
all your test results and treatment. They can answer questions you
have in-between appointments with specialists.
Diagnosis 23Health professional Role
a doctor who specialises in surgery of the
hepatobiliary surgeon
liver and its surrounding organs
a specialist in diseases of the digestive
gastroenterologist
system, including the liver
a gastroenterologist who specialises in
hepatologist
diseases of the liver
prescribes and coordinates the course of
medical oncologist
chemotherapy
help to diagnose cancer by interpreting
radiologist and nuclear results of diagnostic tests, and delivers some
medicine specialists treatments, including those with chemical
compounds
cancer care provide care, information and support
coordinators and throughout your treatment, and administer
nurses drugs, including chemotherapy
social worker, provide information and support with
physiotherapist, practical matters, such as mobility, and link
occupational therapist you to community support services
determines if you are getting enough
dietitian nutrients, and recommends an eating plan for
you to follow during treatment and recovery
assists you with symptom management and
palliative care team
emotional support for you and your family
24 Cancer CouncilKey points
• There are a number of tests a colonoscopy or endoscopy
used to diagnose primary to find out where the primary
liver cancer or secondary cancer started.
cancer in the liver.
• All of these tests will help
• Blood tests show how the your doctor work out the best
liver is working and whether treatment options for you and
there are tumour markers in whether it may be possible to
the blood that might indicate try and cure the cancer.
cancer in the liver.
• Your doctor may tell you what
• Imaging tests include a stage the cancer is at. This
range of scans that allow describes how far the cancer
doctors to see your organs has spread in your body.
and determine whether there
are any abnormal tissue or • You may wonder about the
tumours. Sometimes non- likely outcome of the disease
cancerous (benign) lumps (the prognosis). There are
are found. many factors in considering
your prognosis, such as test
• A biopsy is when tissue is results, the type of cancer you
removed for examination have and your medical history.
under a microscope. This is
not done very often. If it is • You will see many health
done, it is done using a fine professionals when you have
needle or during surgery. tests and treatment. These
include specialists, cancer
• If you have secondary care coordinators, nurses, and
cancer in the liver, you may other health professionals,
also need tests such as such as social workers.
Diagnosis 25Making treatment
decisions
Sometimes it is difficult to decide on the type of treatment to have.
You may feel that everything is happening too fast. Check with
your doctor how soon your treatment should start, and take as
much time as you can before making a decision.
Understanding the disease, the available treatments and possible
side effects can help you weigh up the pros and cons of different
treatments and make a well-informed decision that’s based on
your personal values. You may also want to discuss the options
with your doctor, friends and family.
You have the right to accept or refuse any treatment offered. Some
people with more advanced cancer choose treatment even if it
only offers a small benefit for a short period of time. Others want
to make sure the benefits outweigh the side effects so that they
have the best possible quality of life.
Talking with doctors
When your doctor first tells you that you have cancer, you may
not remember the details about what you are told. Taking notes
or recording the discussion may help. Many people like to have
a family member or friend go with them to take part in the
discussion, take notes or simply listen.
If you are confused or want clarification, you can ask questions –
see page 51 for a list of suggested questions. If you have several
questions, you may want to talk to a nurse or ask the office
manager if it is possible to book a longer appointment.
26 Cancer CouncilA second opinion
You may want to get a second opinion from another specialist to
confirm or clarify your doctor’s recommendations or reassure you
that you have explored all of your options. Specialists are used to
people doing this.
Your doctor can refer you to another specialist and send your
initial results to that person. You can get a second opinion even if
you have started treatment or still want to be treated by your first
doctor. You might decide you would prefer to be treated by the
doctor who provided the second opinion.
Taking part in a clinical trial
Your doctor or nurse may suggest you take part in a clinical trial.
Doctors run clinical trials to test new or modified treatments and
ways of diagnosing disease to see if they are better than current
methods. For example, if you join a randomised trial for a new
treatment, you will be chosen at random to receive either the best
existing treatment or the modified new treatment.
Over the years, trials have improved treatments and led to better
outcomes for people diagnosed with cancer.
It may be helpful to talk to your specialist or clinical trials nurse,
or to get a second opinion. If you decide to take part, you can
withdraw at any time. For more information, call the Helpline for
a free copy of Understanding Clinical Trials and Research or visit
www.australiancancertrials.gov.au.
Making treatment decisions 27Treatment
Your treatment will depend on whether you have primary liver
cancer or secondary cancer in the liver; the size and spread of the
cancer; and whether any other disease, such as cirrhosis, affects
your liver. Your doctor will also consider your age and general
health, as well as the options available at your hospital.
• Primary liver cancer – The most common treatments are
tumour ablation using heat (radiofrequency or microwave
ablation) and chemotherapy delivered directly into the cancer,
known as transarterial chemoembolisation (TACE). Surgery is
used for about 5% of people.
• Secondary cancer in the liver – The main treatments are
chemotherapy or a combination of surgery and chemotherapy.
Surgery
During surgery, part of the liver that contains cancer is removed.
Primary liver cancer – Only a small number of people are
suitable for surgery. Your ability to have an operation depends on
the size, number and position of the tumours, how much of the
liver is affected and whether you have cirrhosis. Operating on
patients with cirrhosis is complicated because the liver may not
function well or regrow afterwards.
For some people, it is not possible to remove part of the liver. These
patients may be considered for a transplant. This means the whole
liver is replaced (see page 31).
28 Cancer CouncilSecondary cancer in the liver – Surgery may be possible if
there is enough healthy liver and the cancer hasn’t spread to other
parts of the body where it can’t be removed (such as the bones).
Liver transplantation isn’t an option.
Some people need surgery for both the secondary cancer in the liver
and the primary cancer. These operations may be done separately or
at the same time.
The hardest part of the operation was knowing how
much progress I had to make after the operation. The
nurses wrote some goals for me: pain control, breathing
exercises, tubes out, getting out of bed. Earl
Partial hepatectomy
Surgery to remove part of the liver is called a partial hepatectomy.
The amount of liver removed depends on your circumstances.
In some cases, the surgeons will remove one half of your liver
(hemihepatectomy). In other cases they will only need to cut out
a small section (segmentectomy). The gall bladder is also taken out,
as it is attached to the liver on the border between the right and left
sides. Occasionally, part of the diaphragm muscle may be removed.
The liver can repair itself easily if it is not damaged. The portion
of the liver that remains after resection will start to grow, even if
up to three-quarters of it is removed. The liver will usually be back
to normal size within a few months, although its shape may be
slightly changed.
Treatment 29Surgical approaches
In the majority of liver abdomen and use a camera
operations, a large cut is made to view the organs.
in the upper abdomen. This is
called an open approach. While recovery is faster after
keyhole surgery, you will still
However, it’s becoming be in hospital for at least one
more common for some liver night and you will need pain
operations to be done with medication.
a smaller incision (known
as keyhole or laparoscopic Keyhole surgery is not available
surgery). Your surgeon in all hospitals. Talk to your
will make small cuts in the surgeon for information.
Two-stage surgery (two-stage hepatectomy)
People with tumours in both sides of the liver sometimes need
two operations:
1. A partial hepatectomy is done to remove tumours from one side
of the liver. Sometimes this operation is combined with tumour
ablation (see page 34) or removal of the primary tumour.
The patient is given about two months to recover. During this
time, the liver may regrow. Before a second operation, the size
of the liver will be checked.
2. If enough of the liver has regrown, the tumours in the second
side will be removed during another partial hepatectomy.
30 Cancer CouncilLiver transplantation
Transplantation involves removing the entire liver and replacing it
with a liver from another person (a donor). There is a possibility
that this treatment could cure primary liver cancer, but it is
generally only used in people with small tumours.
Several factors are taken into account before someone is eligible
for a liver transplant. Their overall health must be good, they
cannot smoke or take illegal drugs, and they must have stopped
drinking alcohol.
Donor livers are scarce, and waiting for a suitable liver may take
many months or years. During this time, the cancer may continue
to grow. As a result, most people have other treatment to control
the cancer while they wait for a donor.
If you have a liver transplant, it may take 3–6 months to recover.
You will probably find it takes a while to regain your energy. You
will also be given medications to reduce the chance of infection
and stop the body rejecting the new liver (immunosuppressants).
You will need to take immunosuppressants for the rest of your life.
After you return home, you will need frequent check-ups to
monitor your health and the success of the transplant.
There is no cost for having a liver transplant in Australia, when it is
performed in a public hospital.
Treatment 31After surgery
You will spend 5–10 days in hospital after a partial hepatectomy,
and up to three weeks in hospital following a transplant.
If you have a laparoscopy, the recovery time is shorter – you
should allow about one week to recover before returning to your
usual activities.
Drips and drains – Different tubes will be in place to drain
post-operative fluids, urine and bile. You will also have a drip
(intravenous tube) giving you fluids and nourishment, as you may
not be able to eat or drink for a few days. When you are able to eat,
you will be given clear fluids at first, and then solid foods.
Pain relief – As with many types of surgery, you may
experience pain, as well as breathing difficulties and nausea.
The hospital staff will try to make you comfortable by giving
you pain relief. You may have a tube called an epidural catheter
placed in your back to deliver pain medication, or you may
be given what is known as an intravenous patient-controlled
analgesic (PCA) system.
The PCA system allows you to control the pain by pressing a
button to give yourself a dose of pain relief when you need it.
It is not possible to give yourself an overdose of medication using
a PCA system.
Let your doctor or nurse know if the pain control is not working,
as it may be possible to adjust the medication or dosage.
32 Cancer CouncilFatigue – You will probably feel quite tired and weak after the
operation, but this should improve within a few weeks.
Mobility – A physiotherapist can help with your recovery by
giving you exercises to improve your breathing, strength and
ability to walk (mobility).
Check-ups – After you return home, you will need frequent
check-ups to monitor your health and the success of the surgery.
Your doctor will tell you how often you should have check-ups.
• Start doing light exercise as • If you have an incision, follow
soon as you are able to. Try your health care team’s
walking slowly or standing instructions about cleaning
while doing chores. the area. Contact your doctor
if it becomes red or inflamed.
• Wait six weeks and consult
your doctor before doing • Avoid alcohol for at least
vigorous exercise, such as one month and only drink
running, weight-lifting or alcohol in moderation after
playing sport. this time. If you have cirrhosis,
you must not consume any
• If you are taking strong (opioid) alcohol. Your medical team
pain-killers, follow your
will talk to you about this.
doctor’s advice about driving.
I had an 11 cm long hepatocellular carcinoma, but
I was lucky that the tumour was operable. After surgery, the
physiotherapy exercises helped my recovery. Robyn
Treatment 33Tumour ablation
Tumour ablation is treatment that destroys a tumour. Ablation
works best when there are only one or two small tumours (less than
3 cm in size). It is used most commonly for small primary liver
cancers, and it is rarely used for secondary cancer in the liver.
The most common ablation treatments use radio waves
(radiofrequency) or microwaves to heat and destroy cancer
cells. This can be done with a needle inserted through the skin
(percutaneously) or with a surgical cut.
Less common types of tumour ablation include alcohol injection
and cryotherapy (see opposite).
Percutaneous ablation
During this procedure, a CT or ultrasound scan is used to guide
a fine needle through the skin and into the tumour. Radio
waves or microwaves are passed through the needle and into
the tumour to destroy it. This is done in the x-ray department
or operating theatre while you are under local or general
anaesthetic. It takes 1–3 hours, but you will usually stay in
hospital overnight.
Afterwards you will probably feel quite drowsy. Side effects, which
include pain, nausea or fever, can be managed with medication.
Ablation with surgery
If the tumours are close to the surface of the liver, you may
have an operation to avoid damage to the diaphragm muscle or
34 Cancer Councilnearby organs. A cut is made in the skin to access the liver, and
probes are inserted to do the ablation.
Recovery from ablation with surgery is usually similar to liver
surgery (see pages 32–33).
Alcohol injection
During alcohol injection, pure alcohol is inserted directly into a
tumour to destroy cancer cells. It isn’t available at all hospitals, but is
occasionally used if other forms of ablation aren’t possible.
Treatment is given under local anaesthetic, and an ultrasound
is used to guide the needle into the tumour. You may be given
more than one injection over several sessions.
You may have some pain or a fever after the alcohol injection, but
these side effects can be managed with medication.
Cryotherapy
Cryotherapy (or cryosurgery) is a procedure used to freeze and
kill cancer cells, but it is not widely available.
You will be given a general anaesthetic, then a cut will be made in
your abdomen. A probe is inserted through the cut into the centre
of the tumour. The probe releases liquid nitrogen that freezes and
kills the cancer cells.
Cryotherapy takes about 60 minutes, and recovery is similar to
having surgery (see pages 32–33).
Treatment 35Chemotherapy
Chemotherapy is the use of drugs to kill, shrink or slow the
growth of tumours.
Depending on the type of cancer you have, you will either have
chemotherapy that spreads throughout your body (systemically)
or goes directly into the tumour (TACE).
Systemic chemotherapy
Systemic chemotherapy is generally not used to treat primary liver
cancer unless the cancer has spread to other parts of the body. It
may occasionally be used to shrink a secondary cancer enough
so that it can be operated on later. It can also be used as palliative
treatment to slow down cancer growth and reduce pain.
Chemotherapy may also be given following other treatment, such
as cryotherapy or surgery, to get rid of any remaining cancer cells.
This is called adjuvant chemotherapy. If given systemically, you
may have intravenous chemotherapy (through a drip) or tablets
over weeks or months.
Systemic chemotherapy can cause side effects because the
drugs circulate through the whole body and affect normal,
healthy cells.
Whether or not you have chemotherapy depends on factors such as
your overall health, liver function, and if you have advanced cirrhosis.
36 Cancer CouncilTransarterial chemoembolisation (TACE)
Chemoembolisation, or TACE, is a way of delivering
chemotherapy directly into a primary cancer. By targeting the
tumour directly, stronger drugs can be used without causing
many of the side effects of systemic chemotherapy.
TACE is rarely used for secondary cancers.
You will be given a local anaesthetic before TACE, and possibly some
medication to relax (a sedative). During treatment, chemotherapy
drugs are injected through a thin tube (catheter) that has been
inserted into the hepatic artery. Tiny plastic beads or soft, gelatine
sponges may be placed in the smaller arteries that lead to the
tumour. This blocks the arteries, keeping the chemotherapy in the
tumour and starving the cancer of oxygen and nutrients.
Usually treatment is given only once, or once every few months.
It is done in the hospital x-ray department. After each TACE
treatment, you will need to remain lying down for about four hours.
You may also need to stay in hospital overnight or for a few days.
Side effects of chemotherapy
The side effects of chemotherapy vary, depending on if you have
systemic chemotherapy or TACE.
Side effects of systemic chemotherapy depend on the drugs used.
Temporary side effects may include:
• nausea and loss of appetite
• tiredness
Treatment 37• hair loss and skin changes
• tingling or numbness in fingers and toes
• mouth sores
• an increased risk of developing infections.
After chemoembolisation (TACE), it is common to develop a fever
the next day, but this usually passes quickly. Other side effects,
such as pain, are less common, but can be severe. You will be given
medication to help control your side effects.
There are many ways to manage side effects. For information,
talk to your medical team or read Cancer Council’s booklet about
chemotherapy. Call the Helpline on 13 11 20 for a free copy or visit
your local Cancer Council website.
Biological therapy
Biological therapies (also called biotherapies) are a range of
treatments derived from natural substances in the body, which are
concentrated and purified for use as drugs. The therapies work
against cancer cells by either stopping their growth and the way they
function, or by helping the body’s immune system destroy them.
Biotherapies may be used after or in conjunction with other
treatments for primary liver cancer or secondary cancer in the liver.
Side effects of biological therapies depend on the types used.
Your doctor will discuss any possible side effects with you.
38 Cancer CouncilRadioembolisation
(selective internal radiation therapy)
Radioembolisation (also known as selective internal radiation
therapy or SIRT) is a type of treatment that targets liver tumours
directly with high doses of internal radiation placed in tiny
radioactive beads.
SIRT is used for both primary and secondary cancers in the liver
when the tumours can’t be removed with surgery. It’s often used if
there are many small tumours spread throughout the liver.
Before treatment (work-up day) – If SIRT is an option, you will
have a number of tests, including an angiogram and a simulation
of the treatment. An angiogram shows up the blood vessels in the
liver and helps to map where the radioactive beads need to go.
This test takes about 90 minutes and you will be observed for
3–4 hours afterwards. You may also have CT and lung scans,
which take about an hour. If the results of these tests are good,
treatment will be scheduled for about 1–2 weeks later.
During treatment (delivery day) – You will have another
angiogram. Afterwards, the tiny radioactive beads, which are
known as SIR-Spheres®, are inserted through a catheter that leads
from your groin to your liver.
The procedure takes about 60 minutes and you will be monitored
closely for 3–4 hours before being taken to a general ward where
you will recover overnight.
Treatment 39Side effects of SIRT can include flu-like symptoms, nausea, pain
and fever. These can be treated with medication, and you usually
can go home within 24 hours.
SIRT is not available in all hospitals, and in most states and
territories you will need to fund the treatment yourself if you don’t
have private health insurance. Talk to your doctor about SIRT and
the costs involved.
Endoscopic stent placement
Sometimes cancer in the liver can obstruct the bile ducts,
particularly if it started in the ducts. If this happens, bile builds up
in the liver and can cause symptoms of jaundice, such as yellowish
skin, itchiness, pale stools or dark urine.
Your doctor may recommend that a thin tube (stent) is placed in
your liver to drain the bile and ease your symptoms. The earlier
the stent is inserted, the less severe the symptoms.
Endoscopic stent placement is done as a day procedure. You will
have a local anaesthetic and possibly a sedative to reduce discomfort.
A gastroenterologist or a surgeon inserts a long, flexible tube with
a camera and light on the end (endoscope) through your mouth,
stomach and small bowel into the bile duct. Pictures of the area
show up on a screen so that the doctor can see where to place the
stent. The stent is put in via the endoscope, which is then removed.
40 Cancer CouncilRecovery from endoscopic stent placement is fairly fast. Your
throat may feel slightly sore for a short time and you may be kept
in hospital overnight.
There is a risk of infection of the bile duct and inflammation of
the pancreas after stent placement – your doctor will talk to you
about this.
Palliative treatment
Palliative treatment helps to improve people’s quality of life by
reducing symptoms of cancer without trying to cure the disease.
It is particularly important for people with secondary cancer.
However, it is not just for end-of-life care and it can be used at
different stages of cancer.
Often treatment is concerned with pain relief and stopping the
spread of cancer, but it also involves the management of other
physical and emotional symptoms. Treatment may include
chemotherapy, endoscopic stent placement or medications.
Call the Helpline on 13 11 20 for free resources about palliative
care and advanced cancer.
The chemotherapy has stopped the secondary cancer
from spreading further, but it makes me very tired. Barbara
Treatment 41Key points
• The most common treatments tumour. Ablation techniques
for primary liver cancer include the use of radio
are radiofrequency tumour waves or microwaves to heat
ablation and transarterial the tumour, cryotherapy to
chemoembolisation (TACE). freeze the tumour, and alcohol
injection.
• The most common treatments
for secondary cancer in the • Chemotherapy is medication
liver are chemotherapy or a that kills or slows the
combination of surgery and growth of cancer cells. It
chemotherapy. is given intravenously, as
tablets, or as transarterial
• Surgery is used to remove chemoembolisation (TACE),
tumours that are small, which delivers chemotherapy
accessible and haven’t spread directly into the tumour.
widely throughout the liver.
• Other treatments for cancer
• Some people with primary in the liver include biological
liver cancer are able to have therapies and selective internal
a transplant, but it can take radiation treatment (SIRT).
many months before a donor These are also used when
becomes available. tumours can’t be surgically
removed.
• After surgery, you will need a
number of days in hospital to • Palliative treatment helps
recover. You will be monitored improve quality of life
closely during this time. by reducing symptoms.
Chemotherapy, medications
• Tumour ablation is localised and endoscopic stent
treatment that destroys the placement are options.
42 Cancer CouncilLooking after yourself
Cancer can cause physical and emotional strain. It’s important to
try to look after your wellbeing as much as possible.
Nutrition – Eating healthy food can help you cope with treatment
and side effects. A dietitian can help you manage special dietary
needs or eating problems, and choose the best foods for your
situation. Call Cancer Council Helpline 13 11 20 for a free copy of
the Nutrition and Cancer booklet.
Staying active – Physical activity may help to reduce tiredness,
improve circulation and elevate mood. The amount and type of
exercise you do depends on what you are used to, how you feel,
and your doctor’s advice. Cancer Council’s Exercise for People
Living with Cancer booklet provides more information about the
benefits of exercise, and outlines simple exercises that you may
want to try.
Complementary therapies – These therapies are used with
conventional medical treatments. You may have therapies such
as massage, relaxation and acupuncture to increase your sense of
control, decrease stress and anxiety, and improve your mood. Let
your doctor know about any therapies you are using or thinking
about trying, as some may not be safe or evidence-based.
Alternative therapies are used instead of conventional medical
treatments. These therapies, such as coffee enemas and magnet
therapy, can be harmful. For more information, call 13 11 20 for a
free copy of the Understanding Complementary Therapies booklet
or visit your local Cancer Council website.
Looking after yourself 43You can also read