Usefulness of gastroesophageal reflux scintigraphy with technetium-99m in pediatric population.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Usefulness of gastroesophageal reflux scintigraphy with technetium-99m in pediatric population. Authors: Orbea U Luis Alberto1. Basantes María Augusta2. Díaz Robert Antonio3 1. Carlos Andrade Marín Hospital, Postgraduate in Radiology and Image. USFQ Quito, Ecuador. 2. Ministerio de Salud Ecuador, Pontificia Universidad Católica del Ecuador. Quito, Ecuador. 3. Ministerio de Salud Ecuador, Universidad de Guayaquil. Guayaquil, Ecuador. Keywords: Gastroesophageal reflux, gastroesophageal reflux disease, bronchoaspiration, scintigraphy, gastric emptying. Key words: Gastroesophageal reflux, Gastroesophageal reflux disease, bronchoaspiration, scintigraphy, gastric emptying. Ethics Committee: This study was communicated and approved by the nuclear medicine service of the Carlos Andrade Marín Hospital. Main author correspondence email: Dr. Luis Alberto Orbea Ulloa radiologiausfq@gmail.com Receipt date: March 11, 2019 Acceptance date: July 15, 2019. Abstract: Gastroesophageal reflux has a prevalence of up to 18% in infants, being one of the most frequent reasons for consultation and among the most frequent, pulmonary aspiration, is the most important and complex complication of reflux in children. The Retrospective, observational study of 29 scintigraphies of pediatric patients of the Nuclear Medicine service at the Carlos Andrade Marín Specialties Hospital, from august 2018 to march 2019. Results: 14 positive cases were obtained for GER scan. while in the esophagogram / gastroduodenal series, 10 positive cases were found for GER; Agreeing with the scintigraphy in 50%. The scintigraphy showed GER in 48.27% of the patients compared to the esophagogram / gastroduodenal series, which found this condition only in 34.48%. Also, it is estimated that the radiation dose is lower using scintigraphy in relation to the esophagogram. Introduccion According to the Pediatric Gastroesophageal Reflux Clinical Guide 2018, the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) and the European Pediatric Gastroenterology, Hepatology and Nutrition Society (ESPGHAN), Gastroesophageal Reflux (GER) is defined as the passage of gastric contents into the esophagus, with or without regurgitation and vomiting; frequent in the postprandial period, with a prevalence of 18% (1) (5). It is important to differentiate a gastroesophageal reflux from a Gastroesophageal Reflux Disease (GERD), since the first is a physiological condition due to transient immaturity of the lower esophageal sphincter (LES), characterized by regurgitation and vomiting present in up to 95% of infants , without repercussion on the postural development (1),usually disappears at 12 months of age; in contrast to GERD, which includes signs and / or symptoms secondary to GER such as chronic Bronchoaspiration (12%), esophagitis (0.5%) and / or esophageal stenosis (0.1%), leading to an impairment in the development of the infant or child (1) (5) (8). In some pediatric patients, complementary tests is necessary in the presence of warning signs such as: weight loss, lethargy, fever, excessive irritability, pain, as well as persistence of regurgitation and / or vomiting beyond 12 months of age (5). Pneumopathies are very common in pediatric age, many studies have suggested a link between GERD and multiple respiratory symptoms, such as aspiration of gastric contents into the respiratory tree, the presence of gastric contents in the esophagus that causes a vagal reflex and sensitization of the cough center in the brainstem (9) which may constitute the manifestation of aspiration pneumonitis, the main concern of the doctor, so he asks for imaging tests that expose children to high effective doses of radiation, one of the most requested is the esophagogram with an effective dose of 1, 5 mSv, an amount equivalent to 75 chest X-rays, as well as an Esophago-gastro-duodenal study with an effective dose of 3 mSv, an amount equivalent to 150 chest X-rays (2).
The diagnosis of GER is mainly based on clinical suspicion, diagnostic studies are indicated
only in cases of doubtful diagnosis or manifestations outside the digestive system (10).
Esophageal monitoring with a 24-hour pH probe study, radiopharmaceutical scintigraphy,
multichannel intraluminal impedance and ultrasound have gained wide acceptance. However,
the "gold standard" for the diagnosis of GER is the multichannel esophageal intraluminal
impedance test (MII), combined with the 24-hour pH study (pHM), which is restricted for use and
cost (3) (4).
The scintigraphy is a simple and non-invasive technique, with an average duration of one hour,
which can detect not only the reflux event, but also the presence of aspiration, abnormal
esophageal contractions and delayed gastric emptying (4). Therefore, this research aims to
assess the usefulness of scintigraphy in GER in the detection of pulmonary aspiration and
gastric emptying, as well as to analyze the amount of effective radiation to which the patient is
exposed.
Objective
To assess the usefulness of scintigraphy in GER for detection of lung aspiration episodes and
gastric emptying, as well as to analyze the amount of effective radiation to which the patient is
exposed.
Materials and methods
29 studies of gastroesophageal scintigraphy were evaluated retrospectively in the Nuclear
Medicine Service of the Carlos Andrade Marín Hospital (CAMH)(Quito, Ecuador), between
August 2018 to March 2019, patients between 2 months to 14 years of age, 12 female and 17
male, with specific symptoms (regurgitation, nausea and vomiting) for GER. Once the informed
consent of their legal representatives was obtained, patients were prepared according to the
following indications: 4-hour fast; In case of breastfeeding, fasting was not recommended. The
radiopharmaceutical used was Colloidal Sulfate – 99mTc, the dose used from 7.4 to 3.7 MBq
(0.2 to 1.0 mCi), which was combined in 2 bottles with formula for infants and orange juice
(liquid), eggs and bread (semi-solids) for children. High resolution, low energy collimator, pulse
analyzer with 20% window centered on 140 keV photopic was used. Matrix 128x128, zoom x2.
Supine position. Once the radioactive substance is ingested, the serial sampling of the
swallowing in the AP position is performed, in 15-second frames for 1 hour and a static image of
the chest and abdomen 24 hours later to rule out bronchoaspiration, all this according to the
protocols of the Nuclear Medicine service of (CAMH).
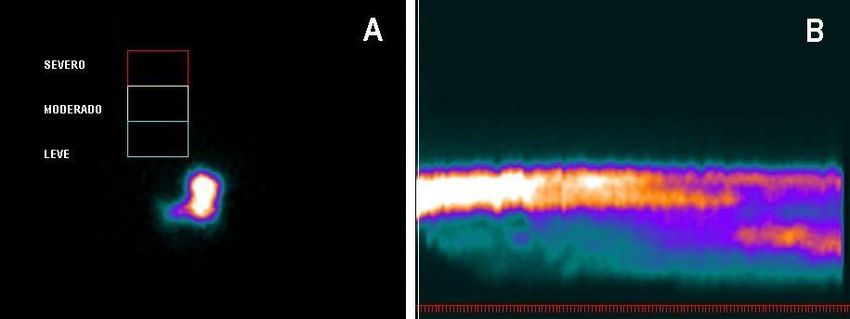
Interpretation / Parameters (Figure 1A)
Normal: Activity is observed exclusively in the abdominal cavity. Next, the radiopharmaceutical
is observed in the intestine due to normal gastric emptying. Up to 4% reflux can be considered
normal in the first minutes of the study.
Abnormal: Attention should be paid to the most distal area of the esophagus. The passage of
gastric content into the esophagus or reflux greater than 5% in the first minutes and control 24
hours later to detect pulmonary aspiration.
Gastric emptying during the first hour:
Parameter: normal percentage of emptying 10 - 63% and retention 90 - 37%.
It is cataloged as: accelerated (> 63%) and prolonged (> 90%).
Table 1. Scan Results
GAMMAGRAPHY GER NO GER TOTAL
Positive 14 0 14
Negative 14 1 15
TOTAL 28 1 29
Sensitivity: 50% Specificity: 100% PPV: 100% VPN: 6.7%
Source: Carlos Andrade Marín, Specialty Hospital.
Results
29 cases were studied, 28 patients had clinical characteristics, and 1 of clinical suspicion for
GER of which 14 cases were positive for GER scan, among which 5 were female and 9 male.
(Table 1) (Figure 2A and 3B).
There were also 12 cases of prolonged gastric emptying (PGE), 5 female and 7
male. Concordance between RGE and VGP was 85%.
In the case of the esophagogram / gastroduodenal series, 10 positive cases for GER were
found; according to the scintigraphy in 50% (Table 2) (Figure 2B and 3A).
Table 2. Scan Results
FLUOROSCOPY GER NO TOTAL
GER
Positive 10 0 10
Negative 18 1 19
TOTAL 28 1 29
Sensitivity: 35.7% Specificity: 100% PPV: 100% NPV:
5.3%
Source: Carlos Andrade Marín Specialty Hospital.
Figure
1A Normal Gastroesophageal scintigraphy, dynamic study, radiopharmaceutical is observed in the
stomach, with no signs of reflux, white letters express valuable degrees of reflux.
1 B. Normal gastro-esophageal scintigraphy assessed throughout the study.
Source: Carlos Andrade Marín, Specialty Hospital.
Figure 2 A. Gastroesophageal scintigraphy, radiopharmaceutical with signs of mild reflux (black
arrow). 2B Esophagogastroduodenal series with signs of reflux (white arrow).
Source: Carlos Andrade Marín Specialty Hospital.
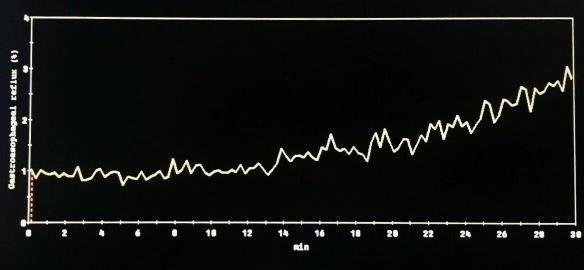
Figure 3 A. Esophagogastroduodenal series with signs of severe reflux (white arrow). Figure 3B Gastroesophageal scintigraphy with color scale inversion, radiopharmaceutical shows signs of reflux (white arrow) Source: Carlos Andrade Marín, Specialty Hospital. Figure 4. Gastroesophageal scintigraphy with color scale inversion, radiopharmaceutical present in the stomach (white arrow), gastric emptying is observed. Source: Carlos Andrade Marín, Specialty Hospital. Figure 5. Activity-time curve evaluation scintigraphy, multiple reflux peaks. Source: Carlos Andrade Marín, Specialty Hospital.
Discussion
Gastroesophageal reflux is one of the most common gastrointestinal problems in children,
which produces a wide variety of symptoms of varying degrees of intensity (1). Occasionally,
GER may cause secondary aspiration and in consequence respiratory complications such as
acute pneumonia, granulomatous pneumonia, lung abscess, bronchiolitis obliterans, pulmonary
fibrosis and chronic bronchitis. (1).
The scintigraphy can demonstrate the aspiration of gastric contents by visualizing the nucleotide
radius in the lungs. It has greater sensitivity than fluoroscopy, but less sharp anatomical
images. According to the various authors, their sensitivity in children is 15 to 59% and their
specificity 83-100% (1). It is a non-invasive method, does not alter the physiology of the
gastroduodenal tract and is well tolerated in most children (12). In order to follow the protocol, it
was used radiopharmaceutical Colloidal Sulfate – 99mTc, with a dose of 7.4 to 3.7 MBq (0.2 to
1.0 mCi), which demonstrates a significantly lower amount of radiation than used in the
esophageal-gastro-duodenal series; the benefit for patients in relation to the equivalent dose is
approximately 0.1 millisievert (mSv) (14) ; that is, the amount of radiation received throughout the
study by the patient is less than that received on a chest x-ray.
In another study that included 76 children between the ages of 1 month to 17 years, in whom
gastroesophageal reflux was confirmed with scintigraphy, it presented greater sensitivity than
with ultrasonography, in addition to this advantage, allows the evaluation of esophageal motility
(12).
and gastric emptying and sometimes allows visualization of pulmonary aspiration
The sensitivity and specificity of the esophageal-gastro-duodenal series is 29% and 15%
respectively (13). In relation to our study, it was found that, among the 29 cases studied,
scintigraphy showed GER in 48.2% compared to the esophageal-gastro-duodenal series that
demonstrated this condition in 34.4%. In accordance with the sensitivity and specificity
mentioned.
It is imperative to highlight that scintigraphy is a method that allows the evaluation of gastric
emptying (Figure 4); Caroccio's works, in which they assessed gastric emptying in infants with
GER, performed in healthy children between 3 and 13 months of age, obtained a final gastric
emptying time for milk formula 78.7 ± 19.3 minutes (8), It is also necessary to stand out that
unlike the esophago-gastro-duodenal series, the scintigraphy has a duration of approximately 1
hour, which makes it possible to assess this parameter.
In our study, a scintigraphy showed a relationship between the presence of GER and PGE with
concordance of 85%. Mori et al. studies’ showed that the symptoms secondary to
gastroesophageal reflux are more severe in patients with prolonged gastric emptying (11).
The limitations of this study are due to the low demand for request of this diagnostic method by
the medical staff, due to this, the sample of this study is small, with no bronchoaspiration being
found in this investigation, although this method has high sensitivity to detect pulmonary
aspiration. (13).Conclusion Pulmonary aspiration is one of the most complex complications in relation to GER, which worries Pediatricians, although this complication was not found in this study, due to the poor medical request for this test, which showed a small sample in this studio ; There is a literature that supports the use of scintigraphy in the detection of bronchoaspiration in 24 hours, GER and assessment of gastric emptying, with significantly lower radiation exposure compared to the esophagogastroduodenal study with fluoroscopy. A study with a larger population group is needed to establish guidelines in the diagnosis of complications of GER in relation to bronchoaspiration. Conflict of Interest: We declare no conflict of interest for this work. Funding source: Private, assumed by the authors and by the Ecuadorian Federation of Radiology and Image.
Bibliography 1. ROA TRINIDAD; “Reflujo Gastroesofágico en 7. Carroccio A, Iacomo G, LiVoti G, Montalto G, Pediatría”; Cátedra de Clínica Pediátrica. UNC Carataio F, Tulone V, Loretto D. Gastric emtying in Servicio de Gastroenterología. Hospital de Niños de la infant with gastroesophageal reflux. Ultrasound Santísima Trinidad de Córdoba. Argentina. evaluation before and after cisapride administration. 2. Andisco D, Blanco S, Buzzi AE. Dosimetría en Scand J Gastroenterol 1992; 27:799-804. radiología. RAR. 1 de abril de 2014;78(2):114-7. 8. Osona Rodríguez De Torres B, Antonio J, Zarza P, 3. Csendes J A, Rencoret P G, Beltrán S M, Smok S Mulet JF. Complicaciones respiratorias en el niño con G, Henríquez D A. Correlación entre síntomas de trastorno de deglución y/o reflujo gastroesofágico. reflujo gastroesofágico y resultados de la pHmetría de 2017;(1):343–56. 24 horas en pacientes con estudio endoscópico 9. Rybak A, Pesce M, Thapar N, Borrelli O. normal o levemente alterado. Revista médica de Chile. Gastroesophageal reflux in children. EMC - Pediatrie. enero de 2004;132(1):19-25. 2017. p. 17. 4. Uslu Kızılkan, N., Bozkurt, M. F., Saltık Temizel, I. 10. Tuncel M, Aksoy T, Bozkurt MF. N., Demir, H., Yüce, A., Caner, B., & Özen, H. (2016). Gastroesophageal re fl ux scintigraphy: interpretation Comparison of multichannel intraluminal impedance- methods and inter-reader agreement. 2011;7(3):245– pH monitoring and reflux scintigraphy in pediatric 9. patients with suspected gastroesophageal reflux. 11. Mori H, Suzuki H, Matsuzaki J, Taniguchi K, World journal of gastroenterology, 22(43), 9595–9603. Shimizu T, Yamane T, et al. Gender Difference of doi:10.3748/wjg.v22.i43.9595 Gastric Emptying in Healthy Volunteers and Patients 5. Rosen, R., Vandenplas, Y., Singendonk, M., with Functional Dyspepsia. Digestion [Internet]. 2017 Cabana, M., DiLorenzo, C., Gottrand, F., … Tabbers, [cited 2019 May 4];95(1):72–8. Available from: M. (2018). Pediatric Gastroesophageal Reflux Clinical http://www.ncbi.nlm.nih.gov/pubmed/28052285 Practice Guidelines: Joint Recommendations of the 12 Elbl B, Birkenfeld B, Walecka A, Szymanowicz J, North American Society for Pediatric Gastroenterology, Listewnik M, Gwardyś A, et al. Upper gastrointestinal Hepatology, and Nutrition and the European Society tract scintigraphy and ultrasonography in diagnosis of for Pediatric Gastroenterology, Hepatology, and gastroesophageal reflux in children. 2011;76(1):63–7. Nutrition. Journal of pediatric gastroenterology and 13. Till H, Thomson M, Foker JE, Holcomb GW, Khan nutrition, 66(3), 516–554. KM. Esophageal and Gastric Disorders in Infancy and doi:10.1097/MPG.00000000000018896. Childhood. Esophageal and Gastric Disorders in 6.Contreras-Contreras K, Villanueva-Pérez RM, Infancy and Childhood. 2017. 1–1526 p. Menez-Díaz DG, Iwasaki-Otake LE, González-Díaz JI, 14. Siegel JA, Wu RK, Knight LC, Zelac RE, Stem HS, Mendoza-Vásquez RG. [Standardization of gastric Malmud LS. Radiation Dose Estimates for Oral Agents emptying scintigraphy with egg white labeled with Usedin Upper. 24(9 99mTc-sulfur colloid]. Rev Med Inst Mex Seguro Soc. diciembre de 2016;54(6):746-51.
You can also read

















































