Vismodegib and the Hedgehog Pathway: A New Treatment for Basal Cell Carcinoma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Therapeutics/Volume 34, Number 10, 2012
Vismodegib and the Hedgehog Pathway: A New Treatment
for Basal Cell Carcinoma
Frank Cirrone, PharmD,* and Christy S. Harris, PharmD, BCPS, BCOP
Department of Pharmacy Practice, Massachusetts College of Pharmacy and Health Sciences, Boston,
Massachusetts
ABSTRACT carcinoma lesions (P ⬍ 0.001) and at decreasing the sum
Background: Vismodegib is an oral inhibitor of the of the longest diameter of existing lesions (P ⫽ 0.003).
Hedgehog pathway approved by the US Food and Conclusions: For patients with unresectable basal
Drug Administration. It is the first systemic treatment cell carcinoma or where resection would be cosmeti-
for patients with locally advanced or metastatic basal cally disadvantageous, vismodegib is an effective ther-
cell carcinoma that is not amenable to surgery and apy with good response rates. At this time, the data are
radiation. This is the first drug to use the Hedgehog too limited to determine overall survival. The Hedgehog
pathway to inhibit the proliferation of tumors and is pathway is a newly identified area in which mutations or
also implicated in the development of other cancers dysregulation can occur, leading to the development and
such as medulloblastoma. progression of tumors. Studies continue to look at other
Objective: The goal of this review was to summarize cancers with involvement of the Hedgehog pathway.
the development, pharmacology, efficacy, and safety of (Clin Ther. 2012;34:2039–2050) © 2012 Elsevier HS
vismodegib. Journals, Inc. All rights reserved.
Methods: Relevant English-language literature was Key words: basal cell carcinoma, Erivedge, GDC-
identified and then evaluated based on results from 0449, vismodegib.
database searches of MEDLINE and EMBASE from
1975 to June 19, 2012. The terms searched included,
but were not limited to, vismodegib, Erivedge, GDC- INTRODUCTION
0449, basal cell carcinoma, and 2-chloro-N-[4-chloro- On January 30, 2012, vismodegib* became the first
3-(pyridin-2-yl)phenyl]-4-(methylsulfonyl)benzamide. drug approved by the US Food and Drug Administra-
Additional literature was identified by assessing the tion (FDA) for the treatment of locally advanced and
reference lists of previously identified articles and metastatic basal cell carcinoma (BCC).1 This novel
through abstracts presented by the American Society of drug also introduced a new signaling target in the treat-
Clinical Oncology. ment of cancer, the Hedgehog (Hh) pathway. Most of
Results: A total of 70 full text citations were identi- the targeted oral agents approved to date are classified
fied although two national conference proceedings as tyrosine kinase inhibitors, or the “nibs,” based on
were then excluded. An additional 10 published ab- their nomenclature of ending with “-tinib.” Vismo-
stracts were also identified. A Phase II, nonrandom- degib, with the “-degib” suffix, heralds a unique mech-
ized, multicenter, international study demonstrated a anism in which to attack signaling mutations within
30.3% objective response rate in metastatic basal cell car- cells of the body that may lead to abnormal
cinoma and a 42.9% objective response rate in locally proliferation.
advanced basal cell carcinoma. The adverse effect profile
for vismodegib is similar to other identified Hedgehog *Current affiliation: New York–Presbyterian Hospital, Depart-
pathway inhibitors; muscle cramps (71.7%), alopecia ment of Pharmacy, New York, New York.
(63.8%), and dysgeusia (55.1%) were the most common Accepted for publication September 5, 2012.
http://dx.doi.org/10.1016/j.clinthera.2012.08.011
adverse effects seen in trials. A Phase II, randomized, pla- 0149-2918/$ - see front matter
cebo-controlled trial in Gorlin syndrome patients with
© 2012 Elsevier HS Journals, Inc. All rights reserved.
basal cell carcinoma concluded that vismodegib was sig- *Trademark: Erivedge® (Genentech, Inc, San Francisco, Cali-
nificantly better than placebo at reducing new basal cell fornia).
October 2012 2039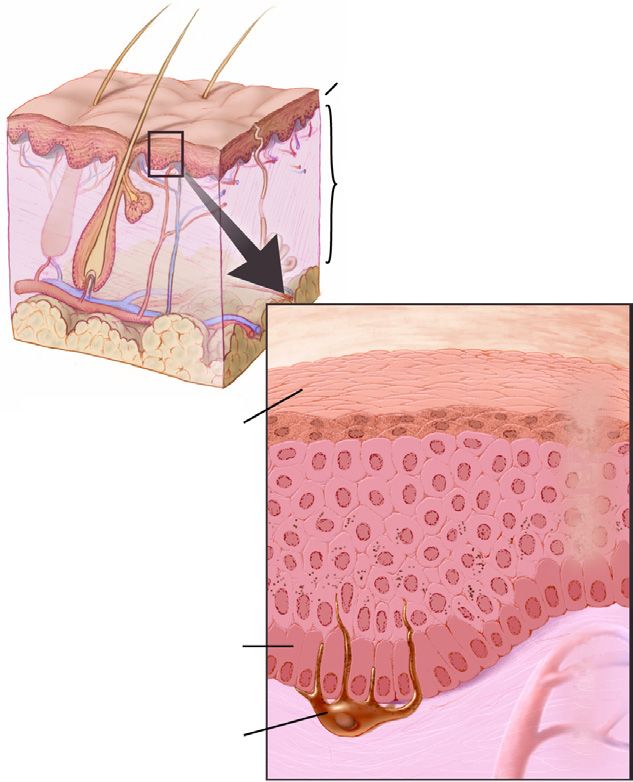
Clinical Therapeutics
riod.8 For women aged ⬍40 years, the diagnosis of
BCC has doubled in the past 30 years.9 The risk of
death is not defined, but expected to be quite low for
Epidermis BCC. However, outcomes can be cosmetically unac-
ceptable or have significant morbidity, as many
(⬎80%) will develop in sun-exposed areas such as the
Dermis
head and neck.10 –12 Metastases occur in only 0.55%
of all cases and may develop years after its original
presentation.11–13
The greatest risk factor for BCC is ultraviolet radi-
ation exposure from the sun, with ultraviolet A and B
rays causing sunburns and DNA damage.3,13 Other
Squamous cells factors that increase the risk of developing BCC in-
Epidermis
clude fair skin, older age, immunosuppression (espe-
cially after organ transplantation), environmental ex-
posure (eg, coal tars, petroleum, arsenic), and specific
genetic conditions such as xeroderma pigmentosum,
albinism, and Gorlin syndrome.10
Basal cells Gorlin syndrome, also known as basal cell nevus
syndrome, is a rare autosomal dominant disorder in
Dermis
which those with the disease are prone to developing
Melanocyte multiple BCCs at an early age, with occurrence of new
lesions being common throughout their lifetime.14 –17
Figure 1. Layers of the Skin. National Cancer In- Biochemically, these patients have a mutation on the
stitute. Don Bliss (Illustrator). http:// Patched 1 (PTCH1) gene of human chromosome
visualsonline.cancer.gov/details.cfm? 9q22.15 This mutation plays an important role in the
imageid⫽4366. regulation of the Hh pathway. In addition to an in-
creased risk for BCCs, these patients have a 5% risk of
developing medulloblastoma, a pediatric malignant tu-
BCC is the most common type of skin cancer and, mor of the cerebellum, and are also at risk for devel-
together with squamous cell carcinoma, are labeled as oping rhabdomyosarcoma.14 –16
nonmelanoma skin cancers.2,3 Skin cancers as a group Current first-line therapy for BCC consists of surgi-
are the most common form of cancer in the United States, cal removal and, potentially, radiation therapy. Most
with ⬎3.5 million cases diagnosed annually.3 Melanoma BCCs are cured by surgery but, in some cases, the can-
is the most lethal, comprising ⬍5% of all skin cancers but cer is unresectable or the surgery is deemed too disfig-
accounting for ⬎75% of skin cancer deaths; nonmela- uring. These are considered locally advanced BCCs
noma skin cancers account for ⬍0.1% of all deaths at- (laBCCs) and may metastasize without treatment.
tributed to cancer.2 Melanoma develops in the melano- Nonsurgical treatment options can include photody-
cytes (skin cells that make pigment), squamous cell namic therapy, topical imiquimod, or 5-fluorouracil.11
carcinoma forms in the squamous cells (flat cells that Until vismodegib, there were no FDA-approved thera-
form the surface of the skin), and BCC forms in the lower pies for these cases, and median survival for metastatic
part of the epidermis (outer layer of the skin)2 (Figure 1), disease varied from as little as 6 months to 3.6 years.12
although there is some evidence to suggest that some Prior systemic treatment recommendations consisted
BCCs may form from hair follicle stem cells.4,5 of platinum-based therapy (cisplatin or carboplatin) or
BCCs account for 80% of nonmelanoma skin can- palliative and supportive care.19
cers.6 The number of these cancers has increased by an The Hh pathway was first elucidated in the fruit fly,
average of 4.2% every year between 1992 and 2006,7 Drosophila melanogaster.16,18 A mutation in the Hh
with treatment of nonmelanoma skin cancers increas- gene led to embryo development that was covered with
ing by an estimated 77% during that same time pe- spiky processes, similar to the spiky appearance of a
2040 Volume 34 Number 10F. Cirrone and C.S. Harris
CI O CI
N N D473H
H CH3 N
S
O 7 1
O 6
Vismodegib 5
Hh ligands
C
SMO
PTCH1
Sufu Gli1, PTCH1, and
PTCH2
Gli3 Gli2 Gli1
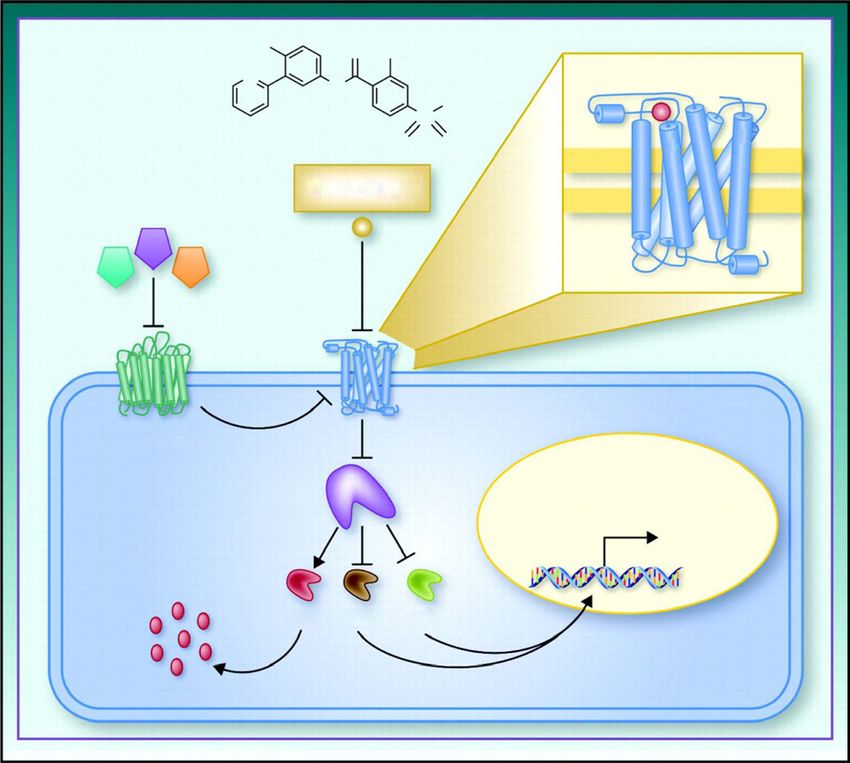
Figure 2. Hedgehog (Hh) signaling, vismodegib action, and acquired resistance. SMO ⫽ Smoothened; PTCH ⫽
patched gene of human chromosome 9q22; Sufu ⫽ suppressor of fused; GLI ⫽ glioma-associated
oncogene. Reprinted with permission from the American Association for Cancer Research: Rudin CM,
Vismodegib, Clinical Cancer Research, 2012;18(12):3218 –3222. DOI:10.1158/1078-0432.CCR-12-
0568.
hedgehog.16 Sonic Hh (SHH), Indian Hh, and Desert that lead to pathway upregulation and abnormal pro-
Hh are 3 ligands that have been identified which stim- liferation. This signaling pathway begins at the pri-
ulate the Hh pathway; SHH was named after a popular mary cilium, which is present on most cells during in-
video game character, and Indian Hh and Desert Hh terphase15,21 (Figure 2). At the base of the primary
were named after species of hedgehogs.15 The Hh path- cilium of a cell is PTCH1, a 12-transmembrane domain
way is important in regulating growth and develop- protein. Normally, the role of PTCH1 is to inhibit ac-
ment in embryogenesis, but it becomes almost dormant tivity of Smoothened (SMO), a 7-transmembrane ser-
during adulthood, with activity limited to some regu- pentine receptor, by blocking it from entering the cil-
lation of tissue homeostasis, continuous renewal and ium.15,17,22,23 When an Hh ligand (SHH, Indian Hh,
repair of adult tissues, and stem cell maintenance.19,20 or Desert Hh) binds to PTCH1, the inhibition of SMO
Inappropriate activation of the Hh signaling pathway is interrupted, and SMO migrates from the intracellu-
is associated with the development of some cancers, lar endosome to the cell membrane of the cilium. SMO
including BCC.17,20 is activated within the cilium and signals downstream
The genetic mutation observed in patients with Gor- activation of the glioma-associated oncogene (GLI) fam-
lin syndrome best characterizes the role of the Hh path- ily of zinc-finger transcription factors, which include
way in BCC pathogenesis. Many of these carcinomas GLI1, GLI2, and GLI3. GLI1 and GLI2 typically function
have genetic alterations in the Hh signaling pathway as activators and GLI3 as a repressor.17,20 The GLI fac-
October 2012 2041Clinical Therapeutics
tors enter the cell nucleus and promote or repress tran- Mechanism of Action
scription of target genes, including PTCH1, GLI1, and Vismodegib is an antagonist of SMO as depicted in
various others. The transcribed target genes go on to reg- Figure 2. It binds and inactivates SMO and inhibits its
ulate cell proliferation via the activation of cyclin D1 and translocation when PTCH1 is stimulated by Hh li-
other cyclin-dependent kinases.17,22 Suppressor of fused gands (ie, SHH, Desert Hh, Indian Hh). Inhibition of
is a negative regulator of the Hh pathway as it binds to the Hh pathway results in decreased downstream pro-
GLI, preventing activation of Hh target genes. Mutations duction of proliferation factors. Decreased prolifera-
can occur in various areas of the Hh pathway and, ulti- tion factors should ultimately lead to suppression of
mately, inactivate PTCH1, causing abnormal prolifera- BCC growth.
tion of cells, potentially leading to several cancers (includ-
ing BCC).15,22 Resistance
In Gorlin syndrome, inhibition of the Hh pathway is Elucidation of resistance mechanisms to vismodegib
impaired due to a mutation of the PTCH1 gene, allow- has been relatively limited. Of note, 1 case report de-
ing dysregulation of the Hh pathway with a resulting scribed a 26-year-old man with treatment-refractory
predisposition of developing BCC. The etiology of metastatic medulloblastoma who developed resistance
BCC in non–Gorlin syndrome patients in almost all after 3 months despite an initial response.16 In this
cases is also linked to upregulated signaling of the Hh patient’s case, it was observed that a D473 resistance
pathway.13,14,24 Therefore, suppression of the Hh mutation had occurred in SMO that prevented vismo-
pathway with an SMO antagonist such as vismodegib degib binding, thus losing efficacy against the tumor.
Dijkgraaf et al22 performed further investigation
would theoretically prevent further basal cell prolifer-
into mechanisms of resistance to vismodegib. First, in a
ation caused by Hh pathway stimulation.
simulation of the mutation that occurred in the previ-
The goal of this review was to summarize the de-
ously mentioned case report,16 substitution of every
velopment, pharmacology, efficacy, and safety of
amino acid for the aspartic acid at position 473 was
vismodegib.
performed, and vismodegib binding was assessed. All
mutant variations were less sensitive to vismodegib
METHODS than wild-type SMO. The study also assessed for other
Relevant English-language literature was identified amino acid residue mutations that may confer resis-
and then evaluated based on results from database tance via alanine-scanning mutagenesis. It was deter-
searches of MEDLINE and EMBASE from 1975 to mined that E518 is an important residue in vismodegib
June 19, 2012. The terms searched included, but were activity on SMO. Its mutation conferred complete re-
not limited to, vismodegib, Erivedge, GDC-0449, basal sistance to vismodegib. Lastly, their study looked at
cell carcinoma, and 2-chloro-N-[4-chloro-3-(pyridin-2- potential compounds to treat Hh pathway resistance.
yl)phenyl]-4-(methylsulfonyl)benzamide. A total of 70 Results showed that Hh pathway–resistant medullo-
full text citations were identified although two national blastoma allografts were sensitive to phosphoinositide-
conference proceedings were then removed. Additional 3-kinase inhibition. Another identified mechanism of
literature was identified by assessing the reference lists of vismodegib resistance is amplification of GLI2 down-
stream of SMO. Other plausible mechanisms exist but
previously identified articles and through abstracts pre-
have yet to be confirmed.
sented by the American Society of Clinical Oncology.
Pharmacokinetics
RESULTS Pharmacokinetic properties of vismodegib were
Chemistry studied in a 2-part, Phase I, open-label trial.19,23,25 In
The chemical formula for vismodegib is part 1, a total of 20 patients were evaluated at 1 of 3
C19H14Cl2N2O3S. Its chemical name is 2-chloro-N-[4- different doses (150, 270, or 540 mg) on day 1, fol-
chloro-3-(pyridin-2-yl)phenyl]-4-(methylsulfonyl)ben- lowed by a washout period of 6 days and then daily
zamide. It is a crystalline-free base with a pKa of 3.8 administration at the same dose beginning on day 8.
and a molecular weight of 421.3 g/mol. The solubility An additional 48 patients were added in part 2 of this
as a free base is far greater at an acidic pH. trial to assess the following: vismodegib’s safety at the
2042 Volume 34 Number 10F. Cirrone and C.S. Harris 150-mg dose (12 patients), patients with BCC at the A group of healthy women of nonchildbearing po- 150- and 270-mg dose (20 patients), and a new 150-mg tential were studied in another Phase I trial to assess formulation evaluation (16 patients). Concentrations single-dose versus 7-day continuous dosing of vismo- of the 3 different doses in part 1 revealed little decline degib.27 AAG levels were monitored to ensure similar- over the 6-day washout period.25 After daily dosing, it ity between the 2 dosing groups. In the single-dose was observed that steady state was achieved earlier cohort, oral vismodegib was administered; 2 hours than would be expected (7–14 days) and did not differ later (the approximate time of maximum plasma con- significantly between the 3 doses.19,25 Less than 1% of centration of the oral form), radiolabeled vismodegib total drug concentration was observed unbound in was administered intravenously. The other cohort re- plasma at steady state.25 The nonlinear kinetics seen in ceived vismodegib orally for 7 days and was then given the daily administration with respect to dose and time the same radiolabeled vismodegib intravenously 2 is explained by vismodegib’s high affinity for binding hours later. Plasma levels were drawn after both dos- with ␣1-acid glycoprotein (AAG). A strong linear cor- age forms in each group and again demonstrated the relation was seen with total steady-state concentra- nonlinear pharmacokinetics of the drug. Clearance tions of the drug and AAG plasma levels.19,25 An and volume of distribution at steady state were in- acute-phase reactant protein, AAG carries lipophilic creased and bioavailability was decreased after con- drugs that are basic or neutrally charged, and AAG tinuous daily dosing due to changes in the unbound levels increase in inflammatory or stress reactions. Up concentration. This finding explains the lack of ex- to a 5-fold elevation in levels has been measured in cessive accumulation of the drug after multiple dos- patients with cancer.24 Vismodegib seems to bind to ing, which would be expected in a drug with the t½ AAG first, and any remaining unbound drug then that was exhibited in the single dose. Compared with binds with human serum albumin. The recommended the single dose, unbound levels of vismodegib in- starting dose for the Phase II trials was determined to creased 2.4-fold with continuous dosing at 7 days. be 150 mg.19,25 The fraction unbound did not return to levels similar The pharmacokinetics of the 33 patients with BCC to the single-dose concentrations until approxi- within the 2-part study was reported by Von Hoff et mately day 35. al.23 Three of the 20 subjects in part 1 had BCC, and each received 1 of the 3 vismodegib doses (150, 270, or 540 mg). The remaining 30 patients enrolled in part 2 Absorption were given either 150 mg (16 patients) or 270 mg (14 Bioavailability after a single 150-mg dose was patients). Median Cmax was found to be 23.0 M. The 31.8% in 1 study.27 The effect of food on absorption median steady-state concentration was 16.1 M, with has been presented in abstract form only.28 Single a median time to steady-state of 14 days (range, 7–22 doses of 150 mg were studied in the setting of a high-fat days). Further evaluation revealed that absorption of meal, low-fat meal, or with fasting overnight. The re- vismodegib was saturable at doses ⬎150 mg and did searchers reported a trend toward a higher Cmax in not result in higher steady-state concentrations of the patients receiving a high-fat meal versus fasting for a drug (median steady-state level of 19.8 M for the single dose, but no statistically significant differences 150-mg dose and 15.9 M for the 270-mg dose). were found between the 3 groups with regard to Another pharmacokinetic study by the same group steady-state Cmax, steady-state Tmax, or steady-state assessed the differences between daily, three times a AUC0 –24. Grade 3 or greater adverse effects were week (TIW), or once weekly dosing of vismodegib at similar between the groups as well. The use of pro- 150 mg.26 The study subjects were stratified according ton pump inhibitors, histamine2-blockers, or antac- to baseline AAG levels and randomized to 1 of the 3 ids may alter the solubility of vismodegib, causing groups. Both total and unbound drug levels were mea- decreased absorption of the drug. At a pH of 1, the sured. Total and unbound levels dropped significantly solubility is 0.99 mg/mL in contrast to 0.0001 in the TIW and once weekly doses compared with the mg/mL at a pH of 7. No formal studies have been daily dosing group. Unbound levels dropped by ⬎50% done to date to evaluate whether agents used to de- in one half of the TIW group and in all patients in the crease the pH of the stomach would affect systemic weekly dosing group. exposure of vismodegib.29 October 2012 2043
Clinical Therapeutics
Table I. Key Phase I trials of vismodegib.
ClinicalTrials.gov
Identifier Cancer Type Key Results
NCT0060772423 Solid tumors (focus: mBCC Established dose of 150 mg orally daily for subsequent trials
and laBCC) Efficacy: 18 of 33 patients with objective response, 11 of 33
with stable disease, 4 of 33 with progressive disease; median
duration of therapy, 9.8 months
NCT0082245832 Refractory medulloblastoma Pediatric study population; 1 grade 3 GGT elevation; BSA
dosing schema for ongoing Phase II trial
(PBTC-032/NCT01239316)
NCT00991718,27 Healthy women of Pharmacokinetic considerations explored; no QTc interval
NCT01173536 nonchildbearing potential prolongation noted at therapeutic doses
mBCC ⫽ metastatic basal cell carcinoma; laBCC ⫽ locally advanced basal cell carcinoma; GGT ⫽ ␥-glutamyl transpeptidase;
BSA ⫽ body surface area.
Metabolism administration. A trial has been designed to study vis-
Vismodegib is minimally metabolized, with ⬎98% modegib in patients with renal or hepatic impairment,
of the drug excreted unchanged. Metabolic pathways but these populations have not been included in the
include oxidation, glucuronidation, and pyridine ring trials produced thus far.
cleavage. The 2 most abundant oxidative metabolites Population pharmacokinetic analyses demonstrated
in feces were produced in vitro by recombinant cyto- that weight (range, 41–140 kg), age (range, 26 – 89
chrome P450 (CYP) 2C9 and CYP3A4/5. However, years), creatinine clearance (range, 30 – 80 mL/min),
drug exposure is not expected to be altered because and sex do not have a clinically meaningful influence
patients were treated concomitantly with CYP3A4 in- on the systemic exposure of vismodegib.29
hibitors and inducers in trials with little change in ex- In the pediatric population, steady-state concentra-
posure.29 Results of in vitro studies suggest that vismo- tions were 10 M after 85 mg/m2 and 15 M after 170
degib is an inhibitor of CYP2C8, CYP2C9, CYP2C19, mg/m2. Clearance was 0.86 mL/min/m2 at steady state,
and the BRCP (breast cancer resistance protein) trans- with an estimated cerebrospinal fluid penetration of
porter. Rosiglitazone, a CYP2C8 substrate, was 1.3% relative to total vismodegib concentration in the
given with vismodegib at steady state with no clini- plasma.32 The concentration of unbound vismodegib
cally significant change in levels, suggesting that measured in the cerebrospinal fluid of patients was
there is no clinically significant inhibition of vismo- similar to the unbound concentration in plasma, sug-
degib with CYP2C8.30 Vismodegib was also found gesting that effective levels of drug do reach the central
in vitro to be a substrate of the p-glycoprotein trans- nervous system.
porter. The manufacturer cautions that systemic ex-
posure and the subsequent adverse effects may be in- THERAPEUTIC EFFICACY/CLINICAL TRIALS
creased when given concomitantly with drugs that inhibit Phase I
p-glycoprotein, such as clarithromycin, erythromycin, or Some key Phase I trials and their essential results are
azithromycin.29 summarized in Table I.23,27,32
Elimination Phase II/III
Vismodegib is eliminated primarily by the hepatic Two Phase II studies investigating vismodegib in
route with 82% recovered in feces and 4.4% recovered BCC have been published, including the pivotal Phase
in urine.31 The estimated t½ of the drug is 12 days after II trial that earned vismodegib its FDA approval.23 No
a single dose and 4 days after continuous once-daily Phase III studies have been initiated or are planned.
2044 Volume 34 Number 10F. Cirrone and C.S. Harris
greater (P ⫽ 0.001) than the hypothesized 10% ORR.
Table II. Phase II trial of vismodegib in locally ad- In the laBCC group (n ⫽ 63), there were 13 complete
vanced (laBCC) and metastatic (mBCC) responses (20.6%) and 14 partial responses (22.2%).
basal cell carcinoma.24 The 42.9% ORR was significantly greater (P ⬍ 0.001)
than the hypothesized 20% ORR. Further breakdown
mBCC laBCC
Outcome (n ⫽ 33) (n ⫽ 63) of responses are listed in Table II. For both mBCC and
laBCC, the median response duration was 7.6 months.
Objective response 10 (30.3%) 27 (42.9%) Overall survival data had not matured by the time the
Partial response 10 (30.3%) 14 (22.2%) study was published. Updated data with an additional
Complete response 0 13 (20.6%) 6 months of follow-up were presented at the 2012
Stable disease 21 (63.6%) 24 (38.1%) American Society of Clinical Oncology annual meet-
Progressive disease 1 (3.0%) 8 (12.7%) ing.33 The presented data supported the previously re-
Unable to be evaluated 1 (3.0%) 4 (6.3%) ported significant clinical effects and adverse effect
profile.
The other Phase II trial, by Tang et al,14 investigated
vismodegib therapy in patients with Gorlin syndrome.
Sekulic et al23 performed the trial that led to vismo-
It was a randomized, double-blind, placebo-controlled
degib being FDA approved. It was an international,
trial involving 3 clinical centers with a primary end
single-arm, multicenter, open-label, 2-cohort trial.
point of reduction in the incidence of new BCCs that
They enrolled 104 patients with either mBCC (n ⫽ 33)
were eligible for surgical resection versus placebo.
or laBCC (n ⫽ 71). Patients with Gorlin syndrome
Forty-one patients were randomized in a 2:1 ratio to
were eligible for enrollment. Patients received 150 mg
receive 150 mg of oral vismodegib or placebo daily for
of oral vismodegib daily until an end point of disease
18 months. At the second interim analysis, the data and
progression or unacceptable toxicity was reached. The
safety monitoring board concluded that there was a
primary indicator of efficacy was objective response
significant difference (P ⬍ 0.0113) between treatment
rate (ORR). This rate included both partial and com-
and placebo groups. The significant results are listed in
plete responses and was defined as a ⱖ30% decrease in
Table III.
disease. Disease progression was defined as a ⱖ20%
increase in lesion size or identification of new BCC
lesions. Safety/Tolerability
From February 2, 2009, to November 26, 2010, a As a class, the Hh inhibitors exhibit adverse effects
total of 96 of 104 patients were evaluated for ORR.24 of muscle spasms/cramps, alopecia, and dysgeusia.12
According to baseline characteristics, the study popu- Unsurprisingly, these adverse effects have played a
lation was 100% white, 61% male, and had a median prominent role in studies assessing vismodegib. Data
age of 62 years. In the mBCC group (n ⫽ 33), there on patients from 4 studies were compiled to evaluate
were 10 confirmed partial responses (30.3%) and no the adverse effect profile and are summarized in Table
complete responses. The 30.3% ORR was significantly IV.29 A total of 138 patients with BCC received vismo-
Table III. Phase II trial results of vismodegib in Gorlin syndrome (also known as basal cell nevus syndrome).14
Vismodegib Placebo
Outcome (n ⫽ 26) (n ⫽ 15) P
New surgically eligible BCCs per year, median 2 25 ⬍0.001
Reduction in size (sum of longest diameters) of existing
surgically eligible BCCs, median ⫺71% ⫺21% 0.003
BCC ⫽ basal cell carcinoma.
October 2012 2045Clinical Therapeutics
had discontinued therapy due to adverse effects. On
Table IV. Adverse effects (n ⫽ 138).29 discontinuation, resolution of dysgeusia and muscle
cramps occurred within 1 month and hair growth
All Grades Grade 3 or 4
within 3 months.
Adverse Effect (%) (%)
Sekulic et al24 reported 7 fatal events occurring dur-
Muscle spasms 71.7 3.6 ing their trial, including hypovolemic shock, myocar-
Alopecia 63.8 – dial infarction, meningeal disease, and ischemic stroke.
Dysgeusia 55.1 – The relationship between vismodegib and these events
Weight loss 44.9 7.2 is unknown. Fifty-seven percent of the patients receiv-
Fatigue 39.9 5.8 ing vismodegib had at least 1 adverse effect. Twenty-
Nausea 30.4 0.7 five percent of patients with laBCC chose to discontinue
Diarrhea 29.0 0.7 therapy on their own accord, although the reason for
Decreased appetite 25.4 – discontinuation was not documented. The authors of this
Constipation 21.0 – trial attributed discontinuation to either long-term, low-
Arthralgia 15.9 0.7 grade adverse effects such as dysgeusia and muscle
Vomiting 13.8 – cramps or patient perception that the maximal benefit
Hyponatremia 4.3 – had already been achieved by vismodegib therapy.
Hypokalemia 1.4 –
Azotemia 2.2 – Dosing/Administration
The FDA-approved dosing of vismodegib is 150 mg
Grading according to National Cancer Institute Common orally daily until disease progression or unacceptable
Terminology Criteria for Adverse Events version 3.0.
toxicity is experienced. A Phase I trial assessed higher
dosing regimens, including 270 mg daily (23 patients)
and 540 mg daily (4 patients).19,25 The increase in dose
degib; severe adverse effects were seen rarely. The most did not reflect an increase in systemic exposure to vis-
common reactions were muscle cramps, alopecia, dys- modegib due to its nonlinear kinetics. Although there
geusia, weight loss, and fatigue. Grade 3 or 4 fatigue was no noted increase in toxicity with higher doses,
was seen in ⬎5% of patients. Although nausea was there was also no added clinical benefit.
seen in ⬃30% of patients, the incidence of grade 3
nausea (ie, unable to adequately take in enough calo- Special Populations
ries or fluid and potential need for parenteral nutrition, Pregnancy and Breastfeeding
tube feedings, or hospitalization)34 was only 0.7%. Vismodegib is listed as a pregnancy category D med-
Notably, 3 of 10 premenopausal women administered ication.29 In rat studies, vismodegib was found to be
vismodegib for BCC developed amenorrhea.29 Only 1 teratogenic at a corresponding 20% of the recom-
patient displayed QTc interval prolongation in a Phase mended daily dose. Teratogenesis in rats included
I study.23 In the pediatric trial reported to date, a Phase craniofacial abnormalities, open perineum, retarda-
I medulloblastoma study investigating vismodegib tions in normal growth, and absence or fusion of digits.
found 1 grade 3 dose-limiting toxicity (increased ␥-glu- When exposed to concentrations equivalent to the rec-
tamyl transpeptidase at a dose of 170 mg/m2); no grade ommended human dose, vismodegib was found to be
4 toxicities were seen.32 embryolethal in rats. Vismodegib’s prescribing informa-
The Phase II trial by Tang et al14 was placebo-con- tion includes a black box warning that embryo-fetal
trolled and therefore clearly illustrates the adverse ef- death and severe birth defects could occur with exposure.
fects of vismodegib versus an inert placebo. In this The development of the first compound to inhibit
study, patients receiving vismodegib were significantly the Hh pathway came from the isolation of cyclo-
more predisposed to experiencing dysgeusia, muscle pamine and jervine from corn lilies. Teratogenic effects
cramps, alopecia, and weight loss compared with pa- (including cyclopia) were noted in sheep feeding on this
tients taking placebo. Also of note from this study were plant.17 Recognizing that the Hh pathway is important
patient medication discontinuation rates. After a mean in embryogenesis, it would suggest that exposure of a
8 months of administration, 7 (27%) of 26 patients fetus to vismodegib could produce significant abnor-
2046 Volume 34 Number 10F. Cirrone and C.S. Harris
malities. The manufacturer encourages women ex- radiation or topical therapy. No analysis is currently
posed to vismodegib during pregnancy, either directly available for treatment in those patients with advanced
or through seminal fluid, to participate in the drug’s cancer that is unresectable. It is difficult to systemati-
pregnancy pharmacovigilance program.29 As this im- cally assess the economics of advanced BCC due to the
plies, men taking vismodegib must also exercise con- lack of histology-specific International Classification
traceptive precautions due to the risk of teratogenesis. of Diseases, Ninth Revision, codes for BCC that were
It is unknown if vismodegib is excreted in breast milk, not created until October 2011. The introduction of
but it is recommended that breastfeeding not occur if a vismodegib is a new area in which to look at economic
woman is receiving the drug based on the same reason- impact because there is nothing to compare it with
ing that it should be avoided during pregnancy.29 beyond symptomatic management. According to the
manufacturer, the wholesale acquisition cost is $7500
Pediatrics per 28 days, and the median duration of treatment for
The safety and efficacy of vismodegib in pediatric most patients in the pivotal Phase II trial was ⬃10
populations have not been well established. In animal months.37
studies, adverse effects at 20% to 40% of the human
exposure range were observed that would be of con-
cern in the pediatric population.29 These adverse ef- DISCUSSION
Vismodegib is an exciting development in the world of
fects included closure of the epiphyseal growth plate
targeted oncologic therapy, introducing a novel mech-
and abnormalities in the development of incisor teeth
anism for fighting cancer. BCC is the most common
(degeneration of odontoblasts, formation of fluid-filled
skin cancer, and there have been few options for those
cysts in dental pulp, ossification of the root canal, and
patients with locally advanced or metastatic disease.
hemorrhage resulting in breakage or tooth loss). Be-
The number of patients within this stage of BCC is
cause inhibition of the Hh pathway may have applica-
small, and there have been only a few studies to give a
tion in the treatment of medulloblastoma, pharmaco-
complete picture of the drug and its adverse effects.
kinetics, efficacy, and toxicities are being assessed in an
Additional information will continue to accrue from
ongoing Phase II study of its use in pediatric patients
postmarketing data as well as from studies incorporat-
aged 3 to 21 years who have medulloblastoma.32
ing vismodegib into chemotherapy and other targeted
Geriatrics therapy regimens. One of the 2 Phase II studies used the
To date, there have been an insufficient number of gold standard design of a randomized, placebo-con-
patients ⱖ65 years of age in studies of vismodegib to trolled trial but was limited only to patients with Gor-
determine whether there are any differences in the lin syndrome. This study was halted at the second in-
pharmacokinetics or safety and efficacy in the geriatric terim analysis based on the data safety and monitoring
population.28 Because the majority of BCCs occur in board’s recommendation regarding statistically signif-
the older population, this group will need to be as- icant improvements in the treatment arm. A placebo-
sessed in the postmarketing phase. controlled study in patients with mBCC and laBCC,
with the exclusion of those with Gorlin syndrome,
Pharmacoeconomics would more accurately portray the safety and efficacy
The estimated cost of nonmelanoma skin cancer in of vismodegib for its FDA-approved indication. How-
patients with Medicare coverage is approximately ever, no Phase III studies are planned because there are
$426 million per year, which ranks as the fifth most no other viable therapies, and it would be considered
costly cancer in this population.35 The overall cost in unethical at this point.
the United States is approximately $650 million annu- More information about vismodegib in different pop-
ally. Most costs are associated with services received ulations is needed. A trial on renal and hepatic dysfunc-
during the physician’s office visit, with the dermatolo- tion with vismodegib is ongoing at the time of this writ-
gist managing up to 82% of the visits in some studies ing, but there are still limited data in the pediatric and
through office-based surgical procedures.36 However, geriatric populations. Studies are currently underway to
economic analyses have only looked at the treatment of look at safety and efficacy in the pediatric medulloblas-
early-stage nonmelanoma skin cancers in which surgi- toma population. Because BCC is prevalent in the older
cal excision is used, sometimes in combination with population, more data on toxicity and pharmacokinetics
October 2012 2047Clinical Therapeutics
will need to be collected. Vismodegib is a promising ther- zole, which acts on SMO as well, although the antag-
apy with a novel mechanism, but its clinical experience to onism is distinctly different from vismodegib and other
date is within a limited patient population. cyclopamine derivatives.21
Resistance patterns of the Hh inhibitors have not yet
been clearly defined but will be closely assessed in pa- CONCLUSIONS
tients undergoing therapy. There are currently no Vismodegib is a novel agent now available in the ever-
proven salvage therapies available for Hh pathway re- growing arena of targeted cancer therapies. Its clinical
sistance. Further investigation into second-line thera- data, despite limited in quantity, have been impressive.
pies for those who fail to improve or whose disease This agent should serve as a key therapy in further
progresses with vismodegib therapy will continue to be investigations into cancers with underlying mutations
researched. Preliminary identification of the role of or enhancements in the Hh pathway. Presently, vismo-
phosphoinositide-3-kinase inhibitors or other path- degib is a step forward for a patient population that
ways as a potential salvage therapy in Hh pathway has had limited options when the disease is unresect-
resistance may potentially provide more options. able or where unacceptable cosmetic outcomes would
The adverse effects profile of vismodegib is some- occur. Additional studies will further elucidate vismo-
thing to watch closely during treatment and is very degib’s role in the treatment of BCC as well as other
relevant when considering therapy in a patient. Al- cancers.
though the majority of toxicities were grade 1 or 2 in
the studies, there is now an understanding that even ACKNOWLEDGMENTS
low-grade toxicities become more of a problem when Both authors contributed equally to the literature
they are associated with an anticancer agent that has to review, data interpretation, and writing of the
be taken every day. As evidenced by Phase II trial re- manuscript.
sults, adherence was compromised by the toxicities
that some of the patients experienced. The discontinu- CONFLICTS OF INTEREST
ation rate by patients from low-grade adverse effects Dr. Harris was responsible for the development of an
such as dysgeusia and muscle cramps was 12% (13 of online publication for a major health-system pharmacy
104 patients)24 and 27.0% (7 of 26 patients)14 in 2 organization as editor and project manager for Lippin-
Phase II studies despite the observed clinical efficacy in cott, Williams and Wilkins. The authors have indicated
treating their disease. To decrease adverse effects, that they have no other conflicts of interest regarding
other means of delivery, including topical application the content of this article.
or intralesion injection of vismodegib have been sug-
gested,13 although another Hh pathway inhibitor
REFERENCES
given topically showed no beneficial results.38
1. US Food and Drug Administration (2012). FDA approves
Although preclinical data suggest that the Hh path- new treatment for most common type of skin cancer [News
way may play a role in development of a number of Release]. www.fda.gov/NewsEvents/Newsroom/Press
cancers, results have been most promising in BCC, Announcements/ucm289545.htm. Accessed August 14,
medulloblastoma, pancreatic adenocarcinoma, and 2012.
hematologic malignancies.21,39 Disappointing results 2. National Cancer Institute. General information about skin
have been seen in some early trials with other solid cancer. www.cancer.gov/cancertopics/pdq/treatment/skin/
tumors such as ovarian and colorectal cancer and even HealthProfessional. Accessed August 14, 2012.
some studies in pancreatic cancer.39 Developing more 3. American Cancer Society. Skin cancer: basal and
useful correlative studies and identifying specific bio- squamous cell. www.cancer.org/Cancer/SkinCancer-
BasalandSquamousCell/DetailedGuide/index. Accessed Au-
markers may aid in the design of future studies to bet-
gust 14, 2012.
ter understand the Hh pathway.39 Research is ongoing
4. Donovan J. Review of the hair follicle origin hypothesis for
to determine the activity of vismodegib in the treat- basal cell carcinoma. Dermatol Surg. 2009;35:1311–1323.
ment of these and many other cancers as well as assess- 5. Grachtchouk M, Pero J, Yang SH, et al. Basal cell carcino-
ing additional semisynthetic Hh pathway inhibitors mas in mice arise from hair follicle stem cells and multiple
that may be more selective or potent. Of interest, an- epithelial progenitor populations. J Clin Invest. 2011;121:
other Hh pathway inhibitor being tested is itracona- 1768 –1781.
2048 Volume 34 Number 10F. Cirrone and C.S. Harris
6. Madan V, Lear JT, Szeimies RM. hibitors. J Clin Oncol. 2010;28: nous and oral pharmacokinetics of
Non-melanoma skin cancer. Lancet. 5321–5326. the Hedgehog pathway inhibitor
2010;375:673– 685. 18. Ganti AK, Kessinger A. Systemic vismodegib in healthy female sub-
7. Rogers HW, Weinstock MA, Harris therapy for disseminated basal cell jects. Br J Clin Pharmacol. 2012 Mar
AR, et al. Incidence estimate of non- carcinoma: an uncommon manifes- 28 [Epub ahead of print].
melanoma skin cancer in the United tation of a common cancer. Cancer 28. Sharma M, Kang SP, Karrison T, et
States, 2006. Arch Dermatol. 2010; Treat Rev. 2011;37:440 – 443. al. Evaluation of food effect on
146:283–287. 19. LoRusso PM, Rudin CM, Reddy JC, et pharmacokinetics (PK) of GDC-
8. Stern RS. Prevalence of a history of al. Phase I trial of hedgehog pathway 0449 (G) in advanced solid tumor
skin cancer in 2007: results of an inhibitor vismodegib (GDC-0449) in patients. Abstract presented at:
incidence-based model. Arch Derma- patients with refractory, locally ad- American Society of Clinical Oncol-
tol. 2010;146:279 –282. vanced or metastatic solid tumors. ogy Annual Conference; June 1–5,
9. Christenson LJ, Borrowman TA, Va- Clin Cancer Res. 2011;17:2502–2511. 2012; Chicago, Ill.
chon CM, et al. Incidence of basal 20. Gupta S, Takebe N, Lorusso P. Tar- 29. Erivedge [package insert]. San Fran-
cell and squamous cell carcinomas geting the Hedgehog pathway in cisco, Calif: Genentech, Inc; 2012.
in a population younger than 40 cancer. Ther Adv Med Oncol. 2010;2: 30. Lorusso P, Piha-Paul SA, Colevas AD,
years. JAMA. 2005;294:681– 690. 237–250. et al. Pharmacokinetic assessment of
10. Amini S, Viera MH, Valins W, Ber- 21. Lin TL, Matsui W. Hedgehog path- drug-drug interaction potential when
man B. Nonsurgical innovations in way as a drug target: smoothened rosiglitazone or combined oral contra-
inhibitors in development. Onco Tar- ceptive is coadministered with vismo-
the treatment of nonmelanoma skin
gets Ther. 2012;5:47–58. degib in patients with locally ad-
cancer. J Clin Aesthet Dermatol. 2010;
22. Dijkgraaf GJ, Alicke B, Weinmann L, vanced or metastatic solid tumors.
3:20 –34.
et al. Small molecule inhibition of Abstract presented at: AACR-NCI-
11. Göppner D, Leverkus M. Basal cell
GDC-0449 refractory smoothened EORTC Molecular Targets and Can-
carcinoma: from the molecular un-
mutants and downstream mecha- cer Therapeutics; November 12–16,
derstanding of the pathogenesis to
nisms of drug resistance. Cancer Res. 2011; San Francisco, Calif.
targeted therapy of progressive dis-
2011;71:435– 444. 31. Graham RA, Lum BL, Morrison G, et
ease. J Skin Cancer. 2011;650258.
23. Von Hoff DD, LoRusso PM, Rudin al. A single dose mass balance study of
12. Walling HW, Fosko SW, Geramine-
CM, et al. Inhibition of the hedge- the Hedgehog pathway inhibitor vis-
jad PA, et al. Aggressive basal cell
hog pathway in advanced basal-cell modegib (GDC-0449) in humans us-
carcinoma: presentation, pathogen-
carcinoma. N Engl J Med. 2009;361: ing accelerator mass spectrometry.
esis, and management. Cancer Metas-
1164 –1172. Drug Metab Dispos. 2011;39:1460 –
tasis Rev. 2004;23:389 – 402.
24. Sekulic A, Migden MR, Oro AE, et al. 1467.
13. Lear JT. Oral hedgehog-pathway in- Efficacy and safety of vismodegib in 32. Gajjar AJ, Stewart CF, Ellison DW, et
hibitors for basal-cell carcinoma. advanced basal-cell carcinoma. al, for the Pediatric Brain Tumor
N Engl J Med. 2012;366:2225–2226. N Engl J Med. 2012;366:2171–2179. Consortium (PBTC 25). A phase I
14. Tang JY, Mackay-Wiggan JM, Aszter- 25. Graham RA, Lum BL, Cheeti S, et al. pharmacokinetic trial of sonic
baum M, et al. Inhibiting the hedge- Pharmacokinetics of hedgehog path- hedgehog (SHH) antagonist GDC-
hog pathway in patients with the way inhibitor vismodegib (GDC- 0449 in pediatric patients with recur-
basal-cell nevus syndrome. N Engl 0449) in patients with locally ad- rent or refractory medulloblastoma.
J Med. 2012;366:2180 –2188. vanced or metastatic solid tumors: J Clin Oncol. 2010;28(18S).
15. Caro I, Low JA. The role of the hedge- the role of alpha-1-acid glycopro- 33. Sekulic A, Migden MR, Oro AE, et al.
hog signaling pathway in the develop- tein binding. Clin Cancer Res. 2011; Efficacy and safety of the hedgehog
ment of basal cell carcinoma and 17:2512–2520. pathway inhibitor vismodegib in pa-
opportunities for treatment. Clin Can- 26. Lorusso PM, Jimeno A, Dy G, et al. tients with advanced basal cell carci-
cer Res. 2010;16:3335–3359. Pharmacokinetic dose-scheduling noma (BCC): ERIVANCE BCC study
16. Rudin CM, Hann CL, Laterra J, et al. study of hedgehog pathway inhibi- update. Abstract presented at:
Treatment of medulloblastoma with tor vismodegib (GDC-0449) in pa- American Society of Clinical Oncol-
hedgehog pathway inhibitor GDC- tients with locally advanced or meta- ogy Annual Conference; June 1–5,
0449. N Engl J Med. 2009;361:1173– static solid tumors. Clin Cancer Res. 2012; Chicago, Ill.
1178. 2011;17:5774 –5782. 34. US Department of Health and Hu-
17. Low JA, de Sauvage FJ. Clinical expe- 27. Graham R, Hop C, Borin M, et al. man Services, National Cancer Insti-
rience with Hedgehog pathway in- Single- and multiple-dose intrave- tute. Common toxicity criteria for
October 2012 2049Clinical Therapeutics
adverse events, version 4.0. http://
evs.nci.nih.gov/ftp1/CTCAE/CTCAE_
4.03_2010-06-14_QuickReference_
8.5x11.pdf. Accessed August 14,
2012.
35. Mudigonda T, Pearce DJ, Yentzer
BA, et al. The economic impact of
non-melanoma skin cancer: a re-
view. J Natl Compr Canc Netw. 2010;8:
888 – 896.
36. Manternach T, Housman TS, Willi-
ford PM, et al. Surgical treatment of
nonmelanoma skin cancer in the
Medicare population. Dermatol Surg.
2003;29:1167–1169; discussion 1169.
37. Pollack A. FDA approves drug for an
advanced skin cancer. New York
Times. January 30, 2012. www.
nytimes.org. Accessed August 14,
2012.
38. Tang T, Tang JY, Li D, et al. Targeting
superficial or nodular basal cell car-
cinoma with topically formulated
small molecule inhibitor of smooth-
ened. Clin Cancer Res. 2011;17:
3378 –3387.
39. McMillan R, Matsui W. Molecular
pathways: the Hedgehog signaling
pathway in cancer. Clin Cancer Res.
2012 June 19. [Epub ahead of
print].
Address correspondence to: Christy S. Harris, PharmD, BCPS, BCOP, De-
partment of Pharmacy Practice, Massachusetts College of Pharmacy and
Health Sciences, 179 Longwood Avenue, Boston, MA 02115-5896. E-mail:
christy.harris@mcphs.edu
2050 Volume 34 Number 10You can also read

















































