Weight Loss Surgery Information for patients
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Weight Loss Surgery Information for patients
Notes
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
2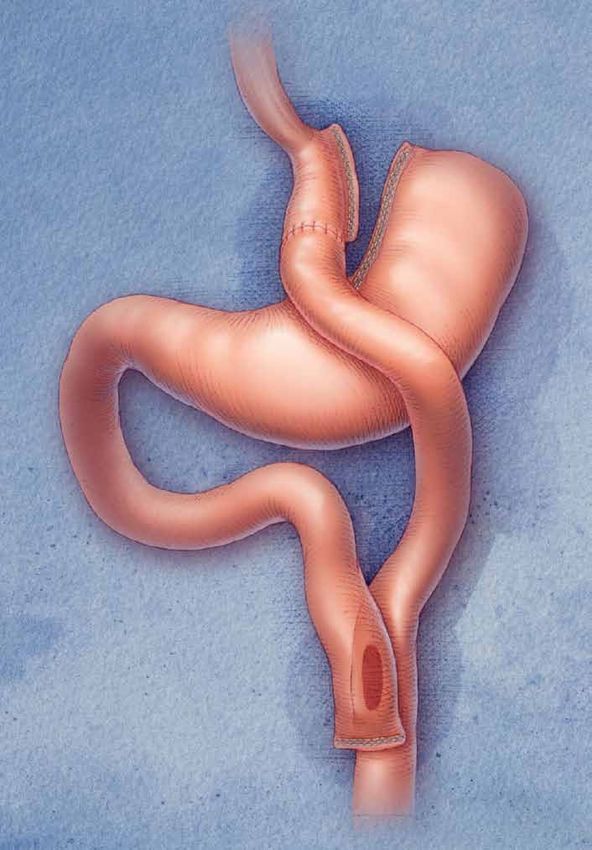
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
What is weight loss surgery?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Why should I consider surgery for weight loss?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Why choose Chelsea and Westminster? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Why treat obesity?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
How can I be referred for weight loss surgery?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
What is a multi-disciplinary team (MDT)?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Weight loss surgery requires commitment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Surgical options. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Laparoscopic Adjustable Gastric Banding (LAGB). . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Laparoscopic Roux-en-Y Gastric Bypass. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Laparoscopic Sleeve Gastrectomy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Biliopancreatic Diversion (BPD) and Duodenal Switch (DS). . . . . . . . . . . . . . . . . . . 11
Intragastric Balloon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Possible complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
What is the right choice? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Preparing for surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
How can I start preparing for surgery?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Do I need to lose weight prior to surgery? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Appointments. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
First appointment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Psychology appointment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
What happens in the assessment?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Other specialist appointments to assess fitness for surgery. . . . . . . . . . . . . . . . . 23
Appointments with the dietitian. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Pre-operative liver shrinkage diet . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Sleep studies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
When will I be put on the waiting list?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Preparation for surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Getting Ready for Weight Loss Surgery workshop. . . . . . . . . . . . . . . . . . . . . . . . . . 25
During and after surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Admission to hospital. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
What happens in hospital after surgery?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Discharge from hospital. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Follow-up after surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
If you are unwell after surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Support . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Hospital patient support group . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
National patient support networks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Further information. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Our contact details . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Membership and Patient Advice & Liaison Service (M-PALS). . . . . . . . . . . . . . . . . 29
3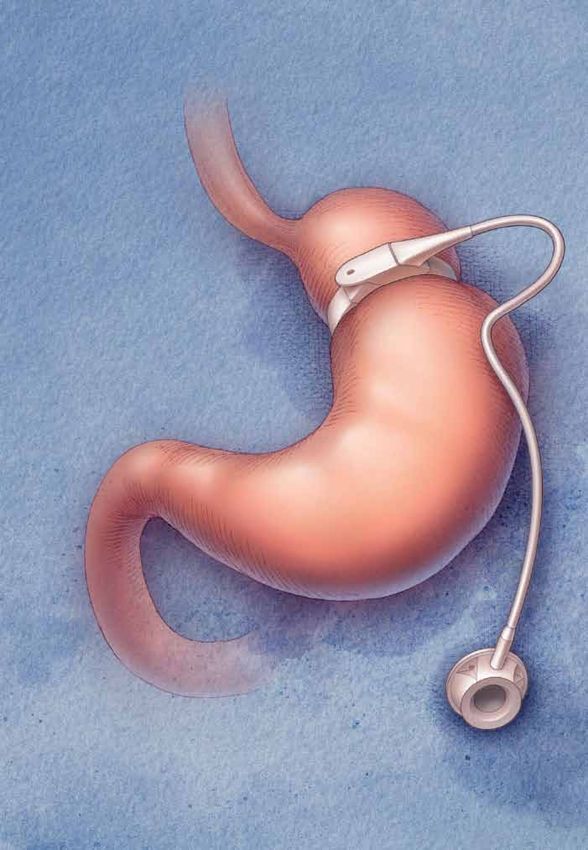
Introduction
This information booklet is designed to Alternatively, you may have never dieted
provide you with an understanding of before but have been referred by your GP
the different surgical weight loss options or another specialist because surgery is
available at Chelsea and Westminster considered the best option for you.
Hospital.
Carrying extra weight can also contribute
We hope that after reading this booklet to many other health problems or affect
and talking with our team, you will have a you physically and emotionally.
better understanding of what is involved in
weight loss surgery including the benefits Why choose Chelsea
and risks.
and Westminster?
Chelsea and Westminster Hospital has
It should also help you decide which option been providing weight loss surgery since
is best for you and your lifestyle goals. the hospital first opened in 1993.
What is weight loss surgery? The procedures we undertake include
gastric banding, gastric bypass, sleeve
Weight loss surgery is also known as gastrectomy, and biliopancreatic diversion
obesity surgery or bariatric surgery. It with duodenal switch. All our operations
refers to operations designed to help are performed laparoscopically (keyhole
reduce your weight. surgery) where possible.
The operations may reduce your hunger, We perform more than 250 procedures
restrict the amount of food you are able a year, and will be performing greater
to eat or reduce the amount of food you numbers each year as more people are
can absorb. referred to our service.
The term does not include procedures We are a ‘preferred provider’ for obesity
that remove fat from the body, such as surgery for patients in London, the South
liposuction or abdominoplasty (tummy East and the East of England.
tuck).
This status means we are a hospital that
specialises in surgery for weight loss
Why should I consider and that our multi-disciplinary team has
surgery for weight loss? expertise in working with people who are
overweight.
Surgery is known to be one of the most
effective methods to aid weight loss and We meet standards that ensure that
maintenance. patients receive the right type of surgery
to suit their needs.
Many of you will have been dieting for
much of your life. You may have lost a It also means that surgery is part of a multi-
large amount of weight in the past but disciplinary service including pre-operative
found it difficult to keep this weight off. and post-operative support.
4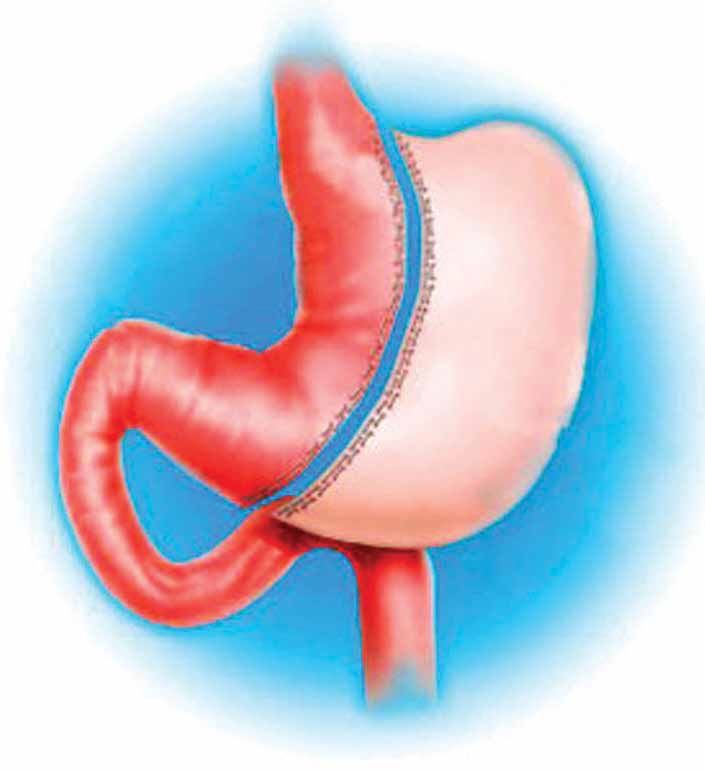
Why treat obesity? How can I be referred for
weight loss surgery?
The main concern about carrying extra
weight is the impact it can have on your Your General Practitioner (GP) can refer you
health. We know that being obese can to our clinic via the NHS Choose and Book
increase the chance of having many other system or by writing to us. To be accepted
diseases such as diabetes and heart for surgery, you must meet the NICE
disease. (National Institute of Clinical Excellence)
guidelines. This means that you must meet
Being obese can also shorten your life the following criteria:
expectancy and approximately 6% of all
• Have a BMI of 40 kg/m2 or more
deaths in the UK are related to obesity.
The heavier you are and the longer you
OR
have been overweight or obese, the
greater the risk. Surgery can be a way • Have a BMI of between 35 kg/m2 and
of managing your weight and preventing 40 kg/m2 with other significant disease
further health problems. (for example, Type 2 diabetes)
Weight loss surgery has been shown AND ALL OF THE FOLLOWING
to prevent or improve conditions and
diseases such as: • Have tried all other appropriate,
available non-surgical measures but
• Type 2 diabetes failed to achieve or maintain adequate,
clinically beneficial weight loss AND
• High blood pressure
• Be willing to see the various specialists
• High cholesterol that we recommend and follow our
• High triglycerides instructions AND
• Heart disease • Be generally fit for anaesthesia and
surgery AND
• Asthma
• Be committed to long-term follow-up
• Sleep apnoea care with us
• Certain cancers such as breast, colon
and endometrial cancer If you have a BMI greater than 50kg/m2,
we can consider surgery as a first line
• Polycystic ovarian syndrome
option (ie without the need to have dieted
• Osteoarthritis and joint problems previously).
• Infertility Obesity surgery is an option if you are
obese, well informed, motivated, and have
• Stress incontinence realistic expectations about what surgery
can achieve for you. You will undergo a
Weight loss surgery can also improve comprehensive, multi-disciplinary assess-
quality of life and increase life expectancy. ment before you can proceed with surgery.
5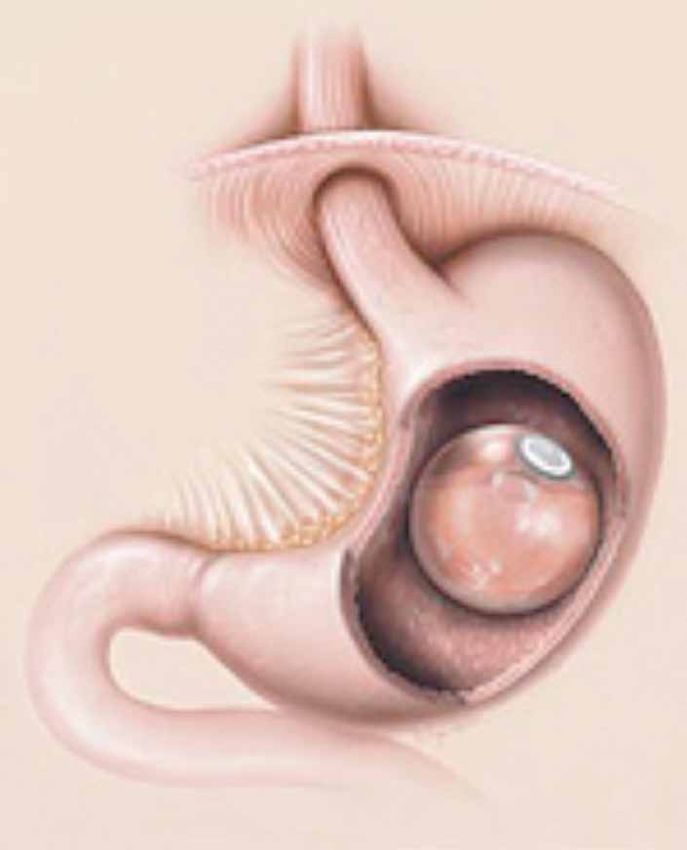
What is a multi-disciplinary Respiratory Physicians
team (MDT)? • Dr Gary Davies
• Dr Suveer Singh
You will see a team of specialists whose
main aim is to ensure you get the best Endocrinologists
treatment and lose weight safely and • Dr Michael Feher
effectively. • Dr Daniel Morganstein
• Dr Kevin Shotliff
These specialists together are known as • Dr Alison Wren
the multi-disciplinary team (MDT).
Weight loss surgery
The members of the team at Chelsea and requires commitment
Westminster Hospital include:
Making the decision to request weight
loss surgery is a serious step and it is
Upper Gastrointestinal (GI)
important that you fully understand what
and Obesity Surgeons
it will involve and what changes you will
• Mr Gianluca Bonanomi have to make.
• Mr Evangelos Efthimiou
• Mr James Smellie From your first visit we will work with you
• Mr Jeremy Thompson to develop a long-term weight loss plan.
We will continue to support you for many
Bariatric Nurse Specialist years after surgery.
• Nuala Davison
Bariatric Specialist Dietitian Surgery is considered a tool for weight
• Kelli Edmiston loss. Weight loss with surgery requires
commitment and motivation. It is not a
Clinical Psychologists quick fix or an easy option.
• Dr Rukshana Ali
• Naomi Biddle (Assistant Psychologist) You will gain the most success from
• Dr Denise Ratcliffe surgery and will avoid complications if you
can commit to the recommended changes
Anaethestists to your diet, exercise and lifestyle, and
• Dr Joanna Allam maintain them for life. This is not always
• Dr Mark Cox easy to do but we will help you to make
• Dr Kevin Haire these changes.
6Surgical options
What do the different under the skin on the left side of your
surgical options involve? abdomen. Fluid can be added to the
band to increase or decrease the sense
1. Laparoscopic Adjustable of satiety. The stomach and intestines
are not cut, stapled or removed when
Gastric Banding (LAGB) placing the band. Therefore digestion and
absorption are not affected.
The band is not filled with fluid at the time
oesophagus
of surgery. Your first band fill will usually be
pouch of band about six weeks after surgery in the X-ray
stomach department. It is likely that you will need
your band tightened more than once to
provide you with the feeling of satiety. A
member of the team will discuss this with
you, based on your food intake, eating
skills and weight loss. Further adjustments
will be perfomed by the nurse specialist or
stomach
dietitian in the band review clinic.
Expected weight loss
You will tend to lose weight steadily over
two years following surgery. On average,
port
people lose about 50–60% of their excess
body weight.
The gastric band is placed around the There is, however, a large variation in
very top of the stomach. There is almost results and weight loss is not guaranteed.
no stomach above the band. The band Adherence to dietary advice and regular
works by providing a feeling of satiety (a exercise is necessary to achieve these
feeling that you are not hungry). When you results.
eat you will get a sense of fullness from a
smaller amount of food and your portion
The dietitian will discuss with you what
sizes will decrease. This feeling of satiety
changes you would need to make to your
will last longer than prior to surgery and
you will not feel hungry between meals. eating patterns to have the best weight
loss results.
The sense of satiety is induced by the
band pressing onto the surface of the Advantages
stomach and stimulating the nerves
leading to the brain. The band is attached • You will feel satisfied sooner, and stay
by some tubing to a port which is placed satisfied for longer
7• The band can be adjusted to increase burn), ulceration, gastritis, bloating,
or decrease satiety via the access port difficulty swallowing, dehydration and
under the skin on your abdomen constipation
• You can lose on average 50–60% of • Nausea and vomiting may occur,
your excess weight particularly in the first few days after
surgery—vomiting is also common if
• The surgery does not involve cutting, you eat too quickly or eat too much
stapling or removing any part of the
stomach and intestines • 10% of people fail to lose the expected
amount of weight with the band
• The stomach and intestines remain
intact so food is digested and absorbed • For successful weight loss, you will have
as normal to follow dietary changes and have self
control
• The surger y can be reversed if
necessary (although you will probably Should you require any other type of
regain the weight) emergency or elective surgery in the future,
the gastric band should not cause any
Disadvantages problem.
• Weight loss may be slow and there is However, the surgeon performing the
large variability in weight loss amongst operation must be informed about your
patients gastric banding prior to surgery.
• Weight loss may not start until many
months after surgery, until the band 2. Laparoscopic Roux-en-Y
is filled to the optimum level for your Gastric Bypass
stomach
• The access port may twist and therefore
be inaccessible for band fills—you may oesophagus
require another operation to correct the
problem pouch of
stomach
• The port or band may leak and deflate, bypassed
which may require another operation to anastomosis portion of
correct the problem stomach
pylorus
• The band may move or slip (2–5%
of cases)—you may need to have all short
the fluid removed from your band intestinal
roux limb
for a period of time, or need another
operation to remove or replace it duodenum
• The band may erode into the stomach
wall and need another operation to
remove or replace it (1% of cases)
• The band or port may become infected
and need to be removed
common
• You may suf fer from worsening channel
gastro-oesophageal reflux (heart
8The gastric bypass is a combined supplements prescribed for you. We will
restrictive and malabsorptive procedure. take regular blood tests to ensure you do
The first step creates a small stomach not develop any nutritional deficiencies.
pouch.
Expectations of weight loss
The surgeon creates this pouch using
metal staples that are similar to stitches. Most people lose weight quite quickly over
The stomach will be cut through so that the first year following bypass surgery. You
the pouch is no longer attached to the rest will generally reach your target weight after
of the stomach. This top section of the 18 months.
stomach (the pouch) will hold your food.
On average, people lose 65–75% of their
The surgeon will count down 75–150cm excess body weight. There is variation in
from the top of your small intestine and the amount of weight that people lose
divide it in two. They will then bring up the following surgery.
lower end of the intestine and bring it up
and attach it to your small stomach (pouch). Adherence to dietary advice and regular
exercise will result in greater weight
Food will now travel from the pouch
loss and better weight maintenance.
straight into the lower part of the small
The dietitian will discuss with you what
intestine. The main part of your stomach
changes you would need to make to your
is left inside your abdomen and continues
eating patterns to have the best weight
to have a blood supply. There is no food
passing through this part of the stomach, loss results.
however it still produces digestive juices.
It is attached further down the small Advantages
intestine to allow these digestive juices
to mix with your food. • The amount of food you can eat is
restricted
The main effect is that the amount of food • You are likely to feel satisfied sooner,
you are able to eat is reduced. Therefore and stay satisfied for longer
you will fill up quickly and stay full for
longer (after only a few mouthfuls of food). • Weight loss starts from the time of
Most people find that they do not get surgery
the same feeling of hunger that they did • You can lose on average 65–75% of
before the surgery. your excess weight
The bypassed portion of stomach and • It is unusual for a patient not to lose
intestine does not affect the absorption of the expected amount of weight
most of the nutrients that you eat. However
• The gastric bypass procedure is
it may reduce the amount of protein,
particularly effective at reducing
vitamins and minerals that you absorb.
medication requirements and improving
To avoid developing a complication blood sugar control for patients
following surgery such as nausea and affected by Type 2 Diabetes Mellitus*
vomiting or a nutrient deficiency it is
*A recent analysis showed resolution of diabetes
essential that you follow the dietary in 81% of patients two years after surgery, and in
advice recommended. You also need to 71% of patients less than two years after surgery
take the daily lifelong vitamin and mineral (Buchwald et al 2007 American Journal of Medicine)
9Disadvantages 3. Laparoscopic Sleeve
Gastrectomy
• Gastric bypass surgery is major surgery
and involves cutting and stapling of the
stomach and intestines
• Obstruction can occur where the new
joins are created at the pouch and
further down the intestine—this may gastric
‘sleeve’
require a procedure (endoscopic or
surgical) to widen the area and allow
excised
food to travel through at the correct rate pylorus
stomach
• You will need to take daily multivitamin
and mineral supplements for life
• You will be at greater risk of suffering
from nutritional deficiencies such as
vitamin B12, iron and calcium
• Your hair may thin although this is
temporary while losing weight at a rapid
rate The sleeve gastrectomy is a restrictive
operation. In this procedure, the surgeon
• You may experience dumping syndrome, creates a narrow tube from the stomach
a condition which occurs if you eat too and removes the remainder. The surgeon
much sugar, fat or alcohol, or large uses metal staples that are similar to
amounts of food—it is not considered stitches and then cuts through the
a health risk, but can be ver y stomach.
unpleasant with symptoms including
About 80% of the original stomach is
nausea, vomiting, diarrhoea, sweating,
removed, leaving about 20% remaining.
faintness, weakness and increased
This new stomach tube, or pouch, is
heart rate (dumping syndrome varies therefore much smaller than the original
from person to person, but tends to stomach. Unlike a gastric bypass where
wear off one year after surgery) food enters a small pouch and then
passes straight into the small bowel, the
• Nausea and vomiting may occur, route that food takes following a sleeve
particularly in the first few days after gastrectomy is the same as it took before
surgery—vomiting is also common if surgery.
you eat too quickly or eat too much
The sleeve gastrectomy can be performed
• You will have better results if you follow as a stand-alone operation.
dietary changes
Sometimes, the procedure will be used as
• Weight regain can occur if you do not the first stage of a two-stage procedure,
adhere to long term dietary, exercise if the surgeon feels it is too technically
and lifestyle changes difficult to proceed straight to a gastric
10bypass. If this is the case, you will have Disadvantages
the sleeve gastrectomy and then after
some weight loss has occurred (9–18 • Sleeve gastrectomy surgery is major
months after the first surgery) the second surgery and involves cutting and
operation can be scheduled. stapling of the stomach
Expectations of weight loss • Your hair may thin—this is temporary
while losing weight at a rapid rate
Most people lose weight quite quickly • Most of your stomach is removed—this
over the first year following a sleeve is a permanent procedure
gastrectomy. Most people lose between
• Nausea and vomiting may occur,
50–60% of their excess body weight.
particularly in the first few days after
There is variation in the amount of weight
surgery—vomiting is also common if
that people lose following surgery.
you eat too quickly, or eat too much
Adherence to dietary advice and regular • You will need to take a tablet daily to
exercise will result in greater weight reduce stomach acidity
loss and better weight maintenance. • You will have better results if you follow
The dietitian will discuss with you what dietary changes and have self control
changes you would need to make to your
eating patterns to have the best weight • Weight regain can occur if you do not
loss results. adhere to long term dietary, exercise
and lifestyle changes
Advantages
4. Biliopancreatic
• Surgery can be offered to patients Diversion (BPD) and
who are at a high risk for progressing
straight to the gastric bypass
Duodenal Switch (DS)
oesophagus
• The amount of food you can eat is
restricted
liver
• You are likely to feel satisfied sooner, pouch
and stay satisfied for longer following
removal of
stomach
• Weight loss starts from the time of anastomosis large
surgery intestine
• You can lose on average 50–60% of
your excess weight bypassed
portion
of small
• Your intestines remain intact so food intestine
is digested and absorbed as normal
common
channel
• The surgery can then be followed by
conversion to the gastric bypass or
duodenal switch resulting in further
weight loss
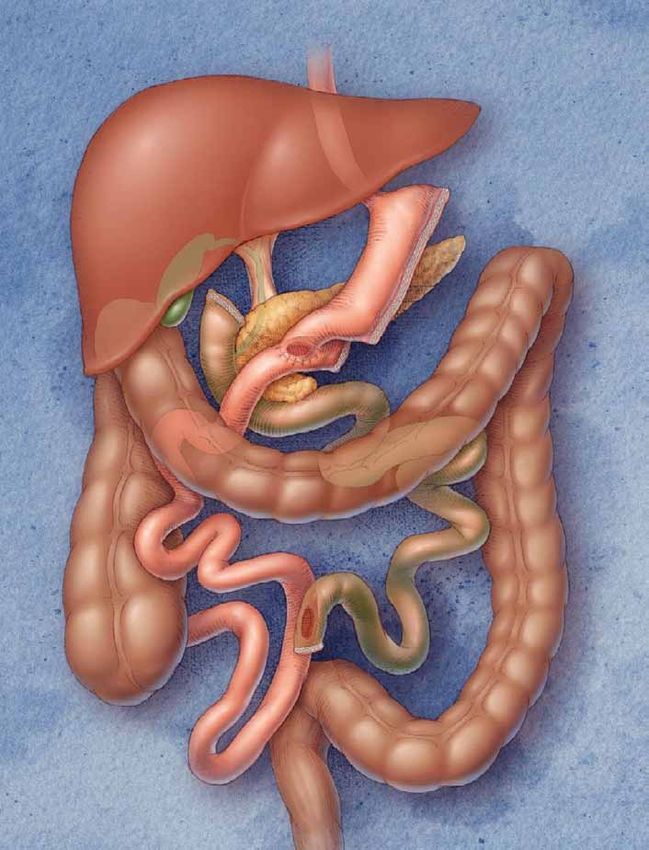
11This is one of the most ef ficient As a result, patients may experience
procedures for weight loss. It is generally frequent loose bowel motions, especially
offered as a two-stage operation in in the first six months. Over time, the
patients with a BMI of more than 60kg/m2. intestine will adapt to better absorb food
and bowel movements will decrease to
The first step creates a pouch. The about 3–5 per day.
surgeon uses metal staples that are
similar to stitches and then cuts through Expectations of weight loss
the stomach. The new stomach pouch is
about a quarter of the size of the original Following this operation people tend to
stomach. The remainder of the stomach lose weight quickly and lose 75–80% of
is removed. their excess body weight after five years.
As with the bypass, the surgeon will then Advantages
divide your small intestine and attach
one end to the pouch. Food will now pass • The amount of food you can eat is not
from your pouch into this section of small restricted
intestine.
• Weight loss starts from the time of
The remainder of your small intestine, that surgery
previously was attached to the bottom of • You can lose on average 75–80% of
your stomach, now joins the other part
your excess weight
of the small intestine close to the large
intestine. This means that your digestive • You may be able to maintain your weight
juices join the intestine to mix with food loss better than with other surgeries
right at the end of the small intestine. This
• Resolution of diabetes in 95% of cases
way, absorption of food is greatly reduced.
after two years
The Duodenal Switch procedure is a
variant of the Biliopancreatic Diversion. Disadvantages
As with the original Biliopancreatic
Diversion, this operation includes dividing • The biliopancreatic diverson and
the stomach but only the outer margin is duodenal switch surgery is major
removed, leaving a sleeve of stomach with surgery and involves cutting and
the pylorus (valve between the stomach stapling of the stomach and intestines
and intestine) and duodenum at its end. • Obstruction can occur where the new
joins are created at the pouch and
The duodenum is divided so that further down the intestine—this may
pancreatic and bile drainage is bypassed. require a procedure (endoscopic or
The near end of the alimentary limb is surgical) to widen the area and allow
then attached to the beginning of the food to travel through at the correct rate
duodenum while the common limb is
created in the same way as described • You will be at greater risk of suffering
before. from nutritional deficiencies than the
bypass, particularly iron, calcium,
Patients can consume larger quantities vitamin A and D and protein—close
than with other surgeries because the monitoring for protein malnutrition,
pouch is bigger and fat and sugars are anaemia, and bone disease is required
not absorbed by the intestine. after these operations
12• You will need to take many multivitamin The intragastric balloon is a soft silicone
and mineral supplements on a daily balloon that is placed inside the stomach
basis for life and filled with saline. By taking up space
within your stomach, the balloon helps
• Your hair may thin although this is you feel full from a smaller amount of food
temporary while losing weight at a rapid which can aid weight loss.
rate
• You may develop gallstones (this Your surgeon may suggest this procedure
happens in 60% of cases) due to rapid for you if they feel you need to lose some
weight loss—it may be necessary to weight prior to further weight loss surgery
undergo a further operation to remove (eg band or bypass), to make surgery safer
your gallbladder, or it may be removed for you. It is not used as the only weight
at the time of surgery loss surgery strategy as after it is removed,
you are likely to regain the weight you have
• Foul smelling flatulence and loose lost. The balloon can also be useful for
stools may be experienced especially helping you to get into good eating habits
if dietary changes have not been made for your next procedure.
to low fat, low sugar choices
What to expect
• You may experience dumping syndrome
which occurs if you eat too much The balloon can be inserted either through
sugar, fat or alcohol, or large amounts a tube down your throat under sedation,
of food—it is not considered a health or under general anaesthetic.
risk, but can be very unpleasant with
symptoms including nausea, vomiting, The balloon is passed down into the
diarrhoea, sweating, faintness, stomach through the mouth, it is inflated
weakness and increased heart rate with saline (sterile water) and some blue
dye. The volume of saline inserted varies
5. Intragastric Balloon from 500–700mls. Once inflated, the
balloon is too large to pass into the bowel
and it will float freely inside the stomach.
oesophagus
The procedure generally takes 20–30
minutes.
After the procedure
After the balloon has been inserted you
will return to the ward and will require
intravenous fluids to keep you hydrated.
Most people stay in hospital for 1–2 nights
after the procedure.
balloon
Nausea and vomiting are very common
after the procedure. You will be given
anti-sickness tablets to help control this.
It is common however, to have these
symptoms for a couple of weeks after
the procedure as your stomach adjusts
to the balloon being in place.
13You can start to take sips of fluids as soon How much weight will I
as you feel able. Your intake of fluids and lose with the balloon?
then food needs to be increased gradually
as tolerated. The amount of weight you lose can vary
depending on how large you are to begin
You will go home with some medication with, and how well you stick to the diet
for sickness and reflux, and a vitamin and and exercise advice.
mineral supplement. The dietitian will see
you before you go home. Possible complications
• Bacterial growth: Should bacterial
How long does the growth occur in the fluid that fills the
balloon stay in place? balloon, release of contaminated fluid
into the intestine when the balloon
Important: The balloon can be used for is punctured for removal may cause
six months but after this time it weakens. infection, fever, cramps and diarrhoea.
It is your responsibility to stay up to date
with your clinic appointments with the • Intestinal obstruction by the balloon:
weight loss surgery team at Chelsea and If the balloon leaks and deflates it may
Westminster Hospital. pass through the intestine and be
passed out of the body.
We will not chase you up if your balloon
has been in for longer than six months. If However, it is possible for a deflated
you need to change an appointment, or balloon to become lodged in the
think you should have an appointment but intestine and cause an obstruction,
particularly in patients who have had
have not received one in the mail, please
previous abdominal surgery.
contact the team.
This is a serious complication possibly
The balloon can be used for six requiring surgical removal of the
months. Longer periods of use are not balloon.
recommended.
Is balloon insertion
Over time the acid content of the stomach suitable for me?
will weaken the balloon material and
cause the balloon to deflate. You may not be suitable for a balloon
insertion if you have had any of the
After six months the balloon is removed following:
by endoscopy under sedation or general
anaesthetic. You will be required to follow • Any inflammatory disease of the
upper gastrointestinal tract including
a special diet for 10 days prior to the
inflammation of the oesophagus
balloon removal. (food pipe), ulceration of the stomach
or duodenum, tumours or other
You may have another balloon inserted for inflammatory conditions
further weight loss, or you may proceed to
further surgery at this point. You will have • Conditions that predispose you to
discussed this with your surgeon before bleeding, such as varices
the balloon is removed. • A large hiatus hernia
14• Strictures of the oesophagus or throat What happens if the balloon
• Any medical condition which increases
deflates spontaneously?
the risks of an endoscopic procedure
If the balloon deflates before a scheduled
• Previous gastric surgery removal you should notice blue dye in
your urine.
• Patients receiving aspirin or other non-
steroidal anti-inflammatory drugs or Contact the team and come to our A&E
those on long term anti-coagulation Department immediately so we can
therapy remove the balloon.
Possible complications
Weight loss surgery may be associated • Marginal ulcers: these can occur at
with complications common to any the junction between the stomach
abdominal gastrointestinal surgery pouch and the intestine in gastric
including: bypass patients.
• General anaesthesia: patients who You will be given medication to prevent
are obese are at greater risk of surgical
this before you go home, which you
anaesthetic complications.
must continue until instructed by
• Pulmonary embolism: this condition your doctor. Smoking after surgery
occurs when a blood clot in the leg significantly increases the risk of ulcer
(deep vein thrombosis) breaks off and formation.
travels to the lungs. Sometimes this can
cause sudden death but most patients • Leaks: leaks from the gastrointestinal
develop sudden shortness of breath. tract can occur where the bowel and
This occurs in about 1% of patients. stomach are connected and sewed.
To help prevent this, you will be put on
blood thinning medication (heparin) and If a complete seal does not form, bowel
given compression stockings while in contents can leak into the abdomen
hospital. You will also be encouraged causing a serious infection. This
to get out of bed and walk as soon occurs in about 0.5–3% of cases of
as possible after surgery. The blood gastric bypass, sleeve gastrectomy
thinning medication will need to be
and biliopancreatric diversion. If a leak
continued for two weeks after you are
is suspected, you may need further
discharged.
surgery.
• Infection: the risk of infection is
generally low. Lung infections are rare • Heart attack: obese patients are at
if you follow post-operative respiratory increased risk of developing a heart
physiotherapy guidelines. Wound and attack due to the higher cardiovascular
urinary infections are rare and can be risk (such as high blood pressure, Type
treated with antibiotics. 2 diabetes, high cholesterol).
15• Bleeding: can occur in 3–5% of cases • Spleen injuries: these are rare but can
and is usually resolved by stopping the occur during surgery. In some cases you
blood thinning medication (heparin) may have to have your spleen removed.
which prevents blood clotting and
pulmonary embolism. Occasionally • Incisional hernia: this occurs more
surgery may be needed to stop the frequently with open surgery techniques
bleeding. and is rare when using laparoscopic
‘keyhole’ techniques. It usually requires
• Gallstones: you may develop gallstones an operation to repair the hernia.
due to rapid weight loss. It may
be necessary to undergo a further • Anastomotic stricture: can occur
operation to remove your gallbladder, in up to 5% of gastric bypass and
although this is quite rare. biliopancreatic diversions. This
usually responds to balloon dilatations
• Bowel obstruction: bowel obstructions (endoscopic procedure).
can be caused by scar tissue in the
abdomen, kinking of the bowel, or the • Death: there is about a 1% risk of death
development of an internal hernia. associated with surgery although this
can change in relation to the surgical
It can occur in up to 5% of cases and procedure and your clinical conditions.
a further operation may be needed to This is usually due to a pulmonary
correct it. embolism or a gastrointestinal leak.
16What is the right choice?
There is no straightforward answer to this After this it slows down and most people
question. It is likely that you will have an reach the expected target after 18 months.
idea of the procedure you would prefer Following the band there is a more steady
when you first attend the clinic. This may weight loss. It may take up to five years.
be based on your own research or from
talking to other people who have had 3. What other health
surgery. problems do I have?
It is our job to provide you with the If you have other health problems that are
information based on our clinical linked to your weight, such as diabetes,
experience to help you decide. It will be a high blood pressure, high cholesterol or
joint decision between you, the surgeon sleep apnoea, losing weight with surgery
and the rest of the team. will help improve them. A bypass has a
higher success rate than bands in curing
Some of the things to consider diabetes so may be a better choice.
when deciding on the right choice of
operation for you are: Certain health problems may place you
at a greater risk when undergoing long
1. How much weight anaesthetics. In this case, the band or
do I need to lose? sleeve gastrectomy may be better choices.
You are likely to lose different amounts of
weight depending on the type of surgery
4. How do my eating patterns
you choose. With a band or sleeve
affect my choice of operation?
gastrectomy you are likely to lose 50–60%
of your excess weight, and with the bypass Your eating patterns are one of the most
65–75% of your excess weight. Your important factors to consider when
dietitian can work out for you what your choosing a surgery as they can affect the
expected amount of weight loss would be amount of weight you are likely to lose,
following each procedure. and how easily you will be able to keep the
weight off. Consider the following:
It is important to remember that surgery
will not necessarily get you back within a) I eat lots of sweets and chocolates:
the healthy weight range (BMI of 20–25 If you tend to eat lots of sweets and
kg/m2), but will get you closer to it. chocolates and find it hard to change
or control this, you may be more suited
2. How quickly do I to the bypass. If you have a band and
need to lose weight? continue to eat these foods you are not
likely to lose weight.
It is worth considering that the different
types of surgery will make you lose weight Most people who have the bypass
over different time periods. With the find that the unpleasant side effects
bypass, the weight loss tends to be rapid that occur after eating sugary foods
with most of the weight lost over the first mean they start to avoid these foods
6–12 months. altogether.
17b) I eat lots of fatty, fried foods and/ you have poor dentition you will need
or I drink alcohol regularly: These to see a dentist prior to getting a date
foods are high in energy and make it for surgery.
hard to lose weight if eaten regularly.
As with the sugary foods, fatty foods g) I comfort eat or binge eat: Surgery
eaten after the bypass can give you does not stop binge eating or emotional
diarrhoea which means you may end up eating or change the triggers for these.
avoiding these foods altogether. You will While binge eating will not necessarily
still be able to eat these foods following prevent you from having surgery, we need
a band, which may therefore slow down to think carefully about whether it would
your weight loss. Consider your ability be better to get some additional help to
to restrict these foods from your diet. address this before having surgery. We
can help you access this support.
c) I eat irregularly and can go long
periods between meals: With all A band may not be suitable if your binge
procedures, you will tend to lose more eating continues after surgery. Trying to
weight if you can stick to a structured, overeat with a band will cause you to be
regular eating pattern. It is particularly sick. Continued overeating and vomiting
important to eat regularly following can lead to damage to the band or your
weight loss surgery because allowing oesophagus and may require further
yourself to become too hungry may surgery or even removal of the band.
result in eating too quickly and not
chewing your food well. This can result Other important considerations include
in pain and vomiting if you overfill your the following:
pouch.
5. I smoke
d) I hardly eat anything at all: If you
already have a small intake, an You will be advised to quit smoking.
operation that only reduces appetite Smoking is associated with higher risk of
(eg gastric band) is unlikely to make anastomotic leaks and ulceration after
much difference to your intake or result surgery. If you need support with this, we
in significant weight loss. You may be can refer you to the Stop Smoking Service
better suited to the bypass. at Chelsea and Westminster Hospital or
you can see your GP or pharmacist.
e) I am vegetarian or lactose intolerant:
This is important to consider if you are
We will not consider you for weight loss
leaning towards the bypass or sleeve
surgery if you are actively smoking.
gastrectomy. Although this does
not stop you from having any of the
procedures, it is important that you 6. I am planning to
are able to get enough protein in your become pregnant soon
diet to meet your requirements. Your
dietitian will discuss with you alternative We recommend that you do not fall
foods to ensure you are eating enough pregnant while you are rapidly losing
protein. weight. During weight loss, your body may
not be getting all the essential nutrients it
f) I don’t have any back teeth: Following needs for you and your baby to be healthy.
weight loss surgery, it is important that After bypass surgery the effectiveness of
you are able to chew your food well. If the oral contraceptive pill reduces.
18You must not become pregnant for 18 10. I am unable to attend
months following surgery. Additional regular appointments
barrier methods of contraception (eg
condoms) are compulsory for 18 months You will need to attend regular hospital
following surgery. appointments after your surgery to ensure
everything is going well and you are losing
If you do fall pregnant, we advise you to weight safely. You will need to see the
let us know as soon as possible so we can dietitian every three months in the first
monitor you more closely. 1–2 years. This is to make sure you have
adequate nutrition. You may also need
It is important to remember that you are regular blood tests. Following the band, you
likely to become more fertile when you may need extra appointments for band fills.
lose weight and so precautions need to
be taken, even if you have been told you If you cannot attend these appoint-
cannot have children. ments you will not be considered for
surgery at Chelsea and Westminster
7. I’m worried about the Hospital.
dangers of having surgery
12. Will my eating patterns
Patients are often worried about the and lifestyle have to
complications of major surgery such as change after surgery?
the bypass.
Yes. Many people believe that surgery
The most common risk following the for weight loss will force you to follow
bypass is a leak from one of the joins in healthy eating patterns but this is not true.
the bowel. This can require a longer stay Surgery can help you lose weight but the
in hospital. amount you lose and how healthy your
diet is depends on your hard work and
determination.
Your surgeon can discuss with you your
individual level of risk for surgery.
Surgery restricts how much you can take
in at a time. This helps you to limit your
8. I’ve had previous food intake and therefore lose weight.
abdominal surgery However, the procedures do not physically
stop you from eating your favourite foods.
Generally you will still be able to undergo You are still ultimately responsible for what
surgery. If you have had many surgeries of food you choose to eat. You will need to
your abdomen, you may need open rather use willpower to stop eating energy dense
than keyhole surgery. Your surgeon will foods such as crisps, chocolate, biscuits
discuss this with you. etc. Even small amounts of these foods
can slow down your weight loss.
9. Is the procedure reversible?
It may be necessary to continue with other
We do not consider any of the procedures methods that you have found successful
reversible as reversing the procedure for weight loss, such as attending regular
would result in weight regain. Reversal Weight Watchers® meetings. Most people
procedures also carry more risk than the find that once they have had surgery and
initial procedure. Reversal is considered are losing weight, it becomes easier to
only if it is medically necessary. stick to a healthy diet and exercise.
19It is quite common to eat to provide pedometer and aim to build to 10,000
comfort or to help cope with stressful steps per day.
or distressing situations. Realistically
we cannot change the fact that you are We recommend caution with alcohol
likely to experience stressful or difficult consumption after bypass surgery. The
things at some point in your life but it is absorption of alcohol is unpredictable
very important to find alternative ways of and one glass of wine may result in
coping with these. you becoming drunk. Alcohol should be
avoided as it is high in calories and may
If you continue comfort eating, you may slow your weight loss.
find you don’t lose the amount of weight
you want even following surgery. Food can Remember, surgery is a tool—no
no longer be your way of coping if you wish matter what you think it is NOT the
to lose weight and it is important to be easy option.
aware that you will need to make many
adjustments. 13. Will I have loose, saggy
skin after I lose weight?
We recommend that people start making
changes to their diet and behaviour before Some people are left with some loose skin,
surgery because surgery alone will not especially around the abdomen, arms and
change your eating habits. thighs. You may feel you need surgery to
remove some of this skin. This surgery is
You need to gradually prepare yourself for not included in your referral for weight
the changes ahead otherwise it can be loss surgery.
daunting to make all the changes following
surgery. We will work with you to set goals You will need to discuss this with your
and make changes prior to surgery. GP who will need to make funding
arrangements. They can then refer you
It is essential that you increase your to our plastic surgery team at Chelsea
activity levels. This will help prevent your and Westminster Hospital. However, you
losing muscle tissue while you lose weight. must wait until you have lost all your
It will also help you to lose more weight, weight and have been weight stable for
and prevent weight regain. We generally six months before we can make a referral
recommend people begin by incorporating to our plastic surgery team. This is usually
daily walks into their lifestyle, or use a around two years after surgery.
20Preparing for surgery
How can I start preparing • Mentally preparing—start to analyse
for surgery? your eating behaviour and any triggers
for comfort-eating or over-eating (eg
In order for surgery to work, there are a particular situations, moods, times etc).
number of ‘rules’ you will need to follow in Start finding alternative ways of coping
order to lose the most amount of weight or other things that you can do at these
and minimise complications. You can start times.
preparing yourself for surgery by starting
to practice the following: Do I need to lose weight
prior to surgery?
• Eating slowly—to avoid overfilling your
small pouch. Overfilling can result in It may be necessary for you to achieve
regurgitation (vomiting). Aim for some weight loss prior to surgery. This
bites the size of your thumbnail, or a makes surgery safer for you. Your dietitian
teaspoon. or surgeon will advise you if they feel you
need to lose some weight prior to surgery.
• Chewing well—to avoid food pieces Weight loss can be achieved using diet,
becoming lodged at the bottom of your activity, medication, or with the help of
pouch. This causes discomfort and can an intra-gastric balloon.
lead to regurgitation. Chewing well also
helps you slow your meals down. Aim to If you do not achieve the weight loss
chew your food at least 20 times before asked of you, your surgeon may not be
you swallow it. able to perform the operation.
• Not drinking fluids with meals—this
It is also important that you use the time
can overfill your pouch and lead to
before the operation to plan ahead. You
regurgitation. It can also dilute your
meals and push them through your will need help at home for the first week
pouch quickly, which means you can or two as you will feel tired as the effects
eat more and not feel full. Aim to stop of the operation take time to wear off.
drinking 10 minutes before you are
going to eat, and then wait 30 minutes We can put you in touch with other people
after eating before you drink again. who have had surgery to talk to them
about their experiences and to ask any
• Eating regularly—this stops you getting questions. There are also patients who are
too hungry and eating too fast. Eating happy to support you after your operation.
regularly also results in more weight
loss than if you ate irregularly, or grazed Appointments
and snacked all day.
Most of these consultations are held in
• Eating small portions—it takes a while the outpatients department on the Lower
for your brain to adjust to the small size Ground Floor of the hospital, unless you
of your pouch. Using a side plate, or have been specifically informed otherwise.
toddler plates and cutlery helps you The hospital has a strict policy regarding
keep your portions under control. missed appointments.
21Please arrive on time for your appointment. These may include:
If you are late for appointments it may not
be possible for us to see you on that day. • Psychologist
• Endocrinologist
If you cannot attend an appointment for • Chest physician
any reason you will need to inform the • Anaesthetists
outpatients department in advance.
Attendance at these appointments is
48 hours notice is required if you are mandatory. You will not be considered
unable to attend. If on two or more for surgery until you have had all of these
occasions, you are late, cancel at short reviews conducted. This is to ensure you
notice or do not attend, you may be receive the best care and that surgery is
discharged. safe for you.
First appointment After these reviews have taken place you
will be booked to see your surgeon. The
During your initial appointment, you will be surgeon will answer any further questions
assessed by our Bariatric Nurse Specialist you have, and if everything is in place, will
and one of our dietitians. They will ask put you on the waiting list for surgery.
you a number of questions about your
medical history, weight loss history, and Before your admission, you will be asked
your eating habits. to attend a pre-operative assessment
clinic.
They will also explain the surgeries in more
detail, outlining the pros and cons of each, Any final checks to assess for fitness for
and answer any of your queries regarding surgery will be done here including blood
surgery. tests, screening for MRSA, and ECGs.
You will be asked to bring along your Psychology appointment
completed questionnaire which will be
discussed by the nurse. All patients will be assessed by the
psychology service—this may be done
Your dietitian will go through in detail the through a telephone appointment.
dietary changes that are necessary prior
to and following surgery. Many people may benefit from some
psychological help and support before or
They can also calculate for you your after surgery. Surgery has a drastic impact
expected weight loss following the on the way you eat, your weight and your
different surgery options. If you need to health and can also have an impact on
lose weight prior to surgery, they will also your self-esteem and body image.
support you with this.
Many people are likely to experience
After this initial appointment, your case psychological difficulties at some point in
will be discussed at our multi-disciplinary their lives and this should not necessarily
team (MDT) meeting and you will be prevent them from having surgery.
allocated a surgeon. You may then be
referred to other members of our team Psychologists are available to provide you
according to your individual situation. with any help and support you may need
22to make the best decision for you at the surgery due to a pre-existing illness. You
current time. may be referred to the following:
It is therefore helpful for you to be as • ECHO, ECG or Stress Study—if you are
open as you can about any concerns you at risk of developing a heart failure, a
have or previous difficulties you have heart attack or other heart disease.
experienced.
• Endoscopy—if you have a history of
What happens in the acid reflux or upper gastrointestinal
assessment? tract disease.
We will ask questions about your • Anaesthetist—every patient’s notes
expectations of surgery, emotional factors will be reviewed by the anaesthetist.
that might affect your eating and think If the anaesthetist feels you are a high
about ways to help you manage difficulties. risk for anaesthetic they will book you
into their specialist assessment clinic.
We will also ask about any other
psychological difficulties that you are • Stop Smoking Service—You will be
currently experiencing or have experienced advised to stop smoking for at least two
in the past. The assessment is a chance weeks prior to your surgery. If you need
to think about whether surgery is the best support with this, we can refer you to
the Stop Smoking Service at Chelsea
option for you and how you will cope with
and Westminster Hospital.
the lifestyle changes.
We can also decide together whether
Appointments with the dietitian
it would be helpful to arrange further
You will meet the dietitian during your
psychology appointments in order to help initial assessment. We may need to see
you address issues (eg emotional eating, you more than once prior to surgery to
low mood, low self-esteem) and make ensure you are well prepared for the
changes. dietary and lifestyle changes needed.
Sometimes we decide that surgery should You will be working closely with the
be postponed for a while so that the dietitians after surgery also, so it is a good
person can get some help to deal with opportunity to get to know them prior to
psychological problems that could prevent surgery.
surgery from working.
Pre-operative liver
This decision would always be discussed shrinkage diet
with you. We can organise referrals to
other support services, for example This needs to be followed strictly for at
specialist services if further help is least two weeks prior to surgery. Many
needed. people needing obesity surgery have a
large fatty liver, which can cause difficulty
Other specialist appointments for keyhole surgery.
to assess fitness for surgery
Therefore it is necessary to follow a diet
Some patients are at a higher risk of that is low in dietary carbohydrate and
developing complications during or after fat. This encourages the body to use up
23glycogen stores (carbohydrate that is If you are advised to have Continuous
stored in the liver), thus helping to shrink Po si tive A ir way Pre s sure (C PAP)
the size of the liver, making surgery safer. treatment, we will need to see that you
are using it effectively for 8–10 weeks,
It is essential that you follow this diet. before allowing you to proceed to booking
If you have not followed it prior to surgery, for surgery.
your operation may be cancelled. If it
has not been followed and the operation This will be related to you via the MDT
proceeds, access to your stomach will Co-ordinator or doctor.
be difficult, your operation may be more
complicated, converted to an open You will need to inform the DVLA of your
procedure, or stopped altogether. diagnosis and treatment—an information
form is available from clinic and on the
Consider the liver shrinkage diet as an DVLA website www.dvla.gov.uk.
opportunity to kickstart your weight loss
and get you into the habit of eating a Once you are given the go ahead for
healthy diet. The more weight you lose surgery you must:
prior to surgery, the lower your risks
related to having surgery. 1. Continue using CPAP before and after
the operation. Don’t stop using it.
Sleep studies
If you are not using it effectively for
You may be investigated for sleep apnoea
the recommended period of time, your
as part of your work up to weight loss
surgery may be cancelled.
surgery. This is for three possible reasons:
2. Bring your machine and mask with you
1. To improve your symptoms
to hospital. Alert our CPAP clinic team
2. To improve your medium and long-term of any equipment problems in advance.
health status—reduce chances of heart
or diabetic problems 3. After surgery, make sure you have a
one-year follow up appointment at the
3. To make the anaesthesia and post- sleep clinic.
operative period safer to you.
Please understand that any delay to your
The process involves: surgery date due to this process is to
improve your safety.
• Being seen in the respiratory/sleep
clinic When will I be put on
the waiting list?
• Having a sleep study—either at home
or one night in hospital (there is a 10% You will be put on the waiting list
chance of a repeat study being needed) once you have completed all of your
assessments listed above and you have
• Being told whether you have sleep made a final decision on which surgery
apnoea—either in clinic or by phone/ you are opting for—and ALL clinicians
letter feel you are fit for surgery.
24Preparation for surgery In our experience, those people who are
well-informed, realistic and make changes
• You need to ensure you prepare for before surgery have better results.
surgery by following the pre-operative
liver shrinkage diet. If you have not The aim of the workshop is to make sure
received this diet from the dietitians, that people are as prepared as possible
please contact them and arrange to beforehand and to provide them with
see them again prior to surgery. essential skills to facilitate this.
• Ensure that you have made What will be covered in the workshop?
arrangements for transport to and
from hospital unless you are eligible There will be two workshop sessions. In
for patient transport. You may want
the first workshop we will spend most of
to make sure you have someone to
the session helping you to identify how
help out at home for the first couple of
weeks after surgery, especially if you you can prepare for surgery, for example,
have children. by identifying changes you can introduce
now.
• Look at your post-operative diet sheet
and make some plans about what you We will also cover problem eating (eg
need to buy prior to admission. You comfort eating, emotional eating).
will need to buy or borrow a blender
or liquidiser. Preparing some meals in There will be a chance to hear testimonials
advance and freezing them is a good from patients who have had surgery here
way of making sure you can cope with and to speak to post-surgery patients.
the diet initially after surgery.
The follow up session will be held a month
• Start to think about your coping later and will allow you to bring back to the
strategies. If you cope with stress group any difficulties you have had since
or boredom by eating, you need to the previous session.
think about how you can divert your
focus from food onto something else
The final session will also include a
(exercise, reading, hobbies).Your
appointment with the psychologist will question and answer panel consisting of
help you with this. expert patients, surgeon, nurse specialist,
dietitian and psychologist.
Getting Ready for Bariatric
Surgery workshop To book a place on the workshop or to find
out more information please contact the
The team may suggest that you attend Bariatric Surgery Psychology department
this workshop prior to surgery. on 020 3315 3319.
25You can also read