What's New - American Society for Radiation ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

SPRING 2021
I N
What’s New
R A D I ATION ONCOLOGY
This issue takes you into the clinic and lab for updates on exciting
developments underway. From current research to innovative educational
offerings, look inside to see what’s new in radiation oncology.
Improve Patient Setup and Outcomes During
Hypofractionation and SRS Treatment
Solstice™ variable pitch capability provides increased setup options in CT simulation,
MR imaging* and corrective positioning flexibility during treatment setup.
Congratulations to Miulli.ART Advanced Radiation Therapy on their
patient’s successful treatment outcome while using the Solstice SRS System!
Pre-treatment Post-treatment
“In our clinical experience, Solstice™ SRS Immobilization System device allows us to obtain an excellent
stability and reproducibility for the positioning of the patient in the treatment of brain lesions, especially
in the field of Linac-based Radiosurgery. This advantage translates into the possibility of reducing the
“safety margins” between the clinical target volume (CTV) and the planning target volume (PTV) with
sub-millimeter precision, obtaining savings in the irradiation of the healthy brain. Furthermore, patients
report a high level of comfort, availing of a sure non-invasive open-face immobilization system which
ensures highly quality, performing and effective radiation brain treatments.”
F. Gregucci, I. Bonaparte, A. Surgo, M. Caliandro, R. Carbonara, MP. Ciliberti, A. Fiorentino.
Department of Radiation Oncology, Miulli General Regional Hospital, Acquaviva delle Fonti-Bari, Italy
*With fiber glass version
info@CivcoRT.com | www.CivcoRT.com
COPYRIGHT © 2021. CIVCO IS A REGISTERED TRADEMARK OF CIVCO MEDICAL SOLUTIONS. SOLSTICE IS
A TRADEMARK OF CIVCO. ALL PRODUCTS MAY NOT BE LICENSED IN ACCORDANCE WITH CANADIAN LAW.
2021A1564 REV. A
In This Issue VOLUME 24 • NUMBER 1
news
AMERICAN SOCIE T Y FOR RADIATION ONCOLOGY
What’s New ASTROnews (ISSN 1523-4185) is published quarterly at 251
18th Street South, 8th Floor, Arlington, VA 22202. Dues
IN THE LAB for individual membership in the American Society for
16 Radiation Oncology are $640 (U.S.), which includes $38 for
an ASTROnews subscription. Periodicals Postage Paid at
Features
Arlington, 22210-9998 and at additional mailing offices.
Copyright © 2021 ASTRO. All rights reserved.
8 MRI-Guided Radiotherapy: 18 Research Opportunities in NRG POSTMASTER: Send address changes to ASTROnews,
From “Peek and Shoot” to Oncology 251 18th Street South, 8th Floor, Arlington, VA 22202.
Telephone: 703-502-1550; Fax: 703-502-7852; Website:
Real-Time Adaptive Radiation NRG leaders provide an inside look at www.astro.org/astronews
Therapy NRG and how you can participate.
Printed in the U.S.A., by Quad Graphics in West Allis, WI.
Implementing an MRgRT program
18 Highlights of Cutting-Edge
and highlights from ongoing clinical ASTRO accepts paid advertising. Although we make every
trials. NRG Research Underway effort to accept advertising only from reputable sources,
NRG disease site committee leaders publication of such advertising does not constitute
11 SABR Proposed as Noninvasive summarize some of the cutting-edge an endorsement of any product or claim. Readers are
Cardiac Radioablation studies underway. encouraged to review product information currently
provided by the manufacturers and any appropriate
for Improved VT Patient 20 FLASH Radiotherapy: Are We medical literature. Contact the manufacturer with any
Experience Ready for Clinical Translation?
questions about the features or limitations of the products
or services advertised.
Patients with limited treatment options
The latest research findings of this
now have hope of a future without developing treatment method and For all of the most recent news from ASTRO,
arrythmias. technology. please visit www.astro.org.
13 Treatment of Oligometastatic 23 ASTRO 2020 Annual Meeting:
Cancers: Recent Lessons and The Review The ideas and opinions expressed in ASTROnews do not
necessarily reflect those of the American Society for Radiation
New Horizons ASTRO’s VP of Learning and Education Oncology, the editor or the publisher. Practitioners and
Evaluating the lessons learned from the presents what worked, what didn’t researchers must always rely on their own experience and
SABR-COMET trials and what’s to come. knowledge in evaluating and using any information, methods,
and what’s here to stay with virtual
compounds or experiments described herein. Because of rapid
meetings.
15 Mayo Clinic Jacksonville Site of advances in the medical sciences in particular, independent
verification of diagnoses and dosages should be made. To the
First Clinical Carbon Ion 25 Education in the Post-COVID fullest extent of the law, no responsibility is assumed by ASTRO,
Accelerator in the U.S. Era: What’s Here to Stay? the editor or the publisher for any injury and/or damage to
persons or property as a matter of products liability, negligence
The medical director of particle therapy Examining virtual teaching methods, or otherwise, or from any use or operation of any methods,
provides a preview of Mayo Clinic’s including virtual rounds and interviews, products, instructions or ideas contained in the material herein.
future facilities. and what needs to stay in residential
and medical student training.
16 What’s New in the Lab
SENIOR EDITOR: EDITORIAL BOARD:
Researchers from Yale University and
Najeeb Mohideen, H. Joseph Barthold,
the University of Chicago provide MD, FASTRO MD, FASTRO
updates on their labs and the current,
Sushil Beriwal, MD, MBA
exciting research underway. PUBLISHER:
Laura I. Thevenot Amato J. Giaccia, PhD
Society News
Geoffrey S. Ibbott,
EDITORIAL DIRECTOR: PhD, FASTRO
Anna Arnone
Simon N. Powell, MD,
MANAGING EDITOR: PhD, FASTRO
5 Best of ASTRO 5 In Memoriam 6 Advocacy’s 2020 Diane Kean Alexander Spektor,
Licensing Buzzer Beater and MD, PhD
DESIGN/PRODUCTION:
Opportunities 2021 Game Plan Jaimie Hernandez Sewit Teckie, MD
Paul E. Wallner, DO,
ADVERTISING: FASTRO
Departments Kathy Peters
703-839-7342
corporaterelations@
astro.org
3 Editor’s Notes 29 History: Giants of Radiation
CONTRIBUTING
Oncology: Gilbert H. Fletcher, MD EDITORS:
4 Chair’s Update Lisa Braverman
31 Journals Highlights: Recently Natanya Gayle
27 From the ABR: Changes in ABR Published in ASTRO Journals Kevin Jewett
Exam Development and Colin Whitney
Administration
ASTROnews • SPRING 2021 | 1
See clearly
every time you treat.
Elekta Unity changes how you
deliver radiation therapy.
For the first time, using MRI-guided radiotherapy,
you can see the tumor’s movements and its
exact position while you’re treating it. This is the
precision you need to deliver a truly personalized
treatment. Explore what precision radiation
medicine with Elekta Unity can mean for your
patients and your practice.
Focus where it matters.
elekta.com/seeUnity
LADMRL190626
Not commercially available in all markets.
EDITOR’Snotes
BY NA JEEB MOHIDEEN, MD, FASTRO
SENIOR EDITOR, ASTRONEWS
Tomorrow’s World In September 2020, in a groundbreaking rule
recognizing AI, CMS granted the first New Technology
Add-on Payment (NTAP) status to an AI medical
Real-time adaptive treatments.
company for software used to detect strokes on CT scans.
Stereotactic ablative radiation
This program pays hospitals up to $1,040 per use, time-
therapy to minimize sudden
limited to three years. The AI company charges a yearly
cardiac death. Expanding
fee, and the NTAP reimbursement is designed to support
radiation therapy indications in
health systems in covering that. How did they get to that
metastatic disease. Pioneering
number? How does one decide when to deploy AI, and
research in DNA repair and
can it demonstrably impact outcome? A rapid readout
metabolism. Novel strategies to
of the CT is just one factor in a complex multi-step
decrease immune suppression
algorithm in stroke management and outcome.
and resistance to radiation therapy. A look at FLASH.
The ACR is submitting the first two radiology-specific
Exciting trials coming to the clinic. Transformations in
CPT Category III code proposals (considered tracking
education, training, certification and meetings. These are
codes for new technology, unlike Category 1 codes,
a sample of some of the offerings in this issue on what’s
Category III codes do not get valued at the RUC) for
new in radiation oncology.
AI analysis for the detection of vertebral fractures and
In a recent informal survey among radiation
quantitative ultrasound tissue characterization. More
oncologists and trainees, the question, “Where must
AI-based codes will almost certainly, in time, make their
radiation oncology go first in the 2020s?”* was posed
way through the current convoluted process. How will
ahead of an online panel discussion of the topic hosted
AI affect our workforce and the financial stability of our
by the Red Journal and the Virtual Visiting Professor
field? That remains to be seen, but organizations must
Network. Artificial intelligence (AI) edged out molecular
appreciate that important steps in good and safe patient
biology, FLASH radiation therapy, diversity, equity and
care now and in the future will not be reflected in the
inclusion, and educational reform in the voting for top
current reimbursement models, be it multidisciplinary
priority issue. During the lively debate, Charles Mayo,
discussions on collaborative care or possibly our cognitive
PhD, elegantly advocated for the need to democratize AI,
interactions and response to the AI output. This reinforces
which, if done properly, can lead to better patient care,
the need for a fair alternative payment model that
expanded access and reduced outcome disparities.1
protects patient access to quality care yet also allows the
AI tools for auto segmentation and auto planning are
appropriate use and adoption of new technology besides
continually improving, and reading between the lines
ensuring financial stability. Unfortunately, the focus of the
of the adaptive process described in this issue, one gets
RO Model released by CMS was to cut payments rather
a glimpse of that future. Establishing the standards to
than smooth the transition of radiation oncology from
validate them and high-quality clinical assessment of
fee-for-service to value-based payment.
these important steps in the patient treatment process
The future is, to put it mildly, exciting. You get a sense
are vital. How will these tools impact our work process
of how exciting from the enthusiasm of NRG disease site
and interaction with the patient? Hunyh and colleagues
leaders commenting on new trials exploring many themes:
addressed this in a recent thought-provoking perspective.2
incorporating novel biomarkers and therapeutics, making
If AI or machine learning tools reach the threshold for
inroads into metastatic disease, reducing intensity and
a Category 1 CPT code (have supporting peer-reviewed
morbidity, exploring combinations of immunotherapy and
clinical research and validation), or if our work changes
radiation (page 18). Hopefully, many of them will prove
significantly for an existing code, they would then need
practice changing. Ensuring a better outcome for our
to be valued by the AMA Relative Value Scale Update
patients — that’s the real promise of the future.
Committee (RUC). The RUC values physician work
(professional component) of a medical procedure based
on time, skill, mental effort and judgment. They also value References
the technical component — physicist, dosimetry, therapist 1 The Big Debate: Where must Radiation Oncology go First in the 2020s?
work and equipment costs. When time is saved, unless YouTube. Published February 11, 2021. https://www.youtube.com/
watch?v=ifnDiLxuCEw
the intensity of the work goes up, the value of the code 2 Huynh E., Hosny A., Guthier C. et al. Artificial intelligence in radiation
generally goes down. But whether the true cost of AI and oncology. Nat Rev Clin Oncol. 2020 Dec;17(12):771-781.
the work associated with it can be captured in the current *Look for a forthcoming summary (and results of a post-debate survey) in the Red
system is uncharted territory. Journal from co-hosts Kaleigh Doke, MD; Sue Yom, MD, PhD, FASTRO; and
Brian Kavanagh, MD, MPH, FASTRO.
ASTROnews • SPRING 2021 | 3
CHAIR’Supdate
T H OM A S J. EI CH LER , M D, FA S T R O
CHAIR, BOARD OF DIREC TORS
some momentum for such a council, both financial and
practical considerations made this unrealistic. This was
Our Expanding not, however, the end of the discussion. On the larger
stage, May Abdel-Wahab, MD, PhD, director of the
Role on the Department of Nuclear Sciences and Applications in the
Global Stage Division of Human Health at the International Atomic
Energy Agency (IAEA) in Vienna, Austria, and the
current ASTRO IEC chair, has led an impressive effort
to coordinate specialty societies globally to populate
four workgroups: research, education, communication
HELLO, EVERYONE! Those of you who were kind
and global information sharing. These workgroups are
enough to tune in to my Presidential Address last
a direct result of the three-day Challenges in Global
October may recall that I focused on several discrete
Cancer Care virtual meeting last July, in which ASTRO
themes: the future of the workforce; diversity, equity and
played a highly visible role. We have continued to
inclusion; and global oncology, the theme of the Annual
be supportive of the IAEA mission and have shared
Meeting. The last time I spoke with you on these pages,
appropriate education and communication resources
I returned to the workforce question and the evolution
with the respective workgroups.
of today’s radiation oncologist into tomorrow’s clinical
In the wake of the Annual Meeting and the advent
oncologist. This is a long-haul concern, recognizing
of the IAEA efforts, the ASTRO Board of Directors
that we are in a period of flux within the specialty that
voted unanimously on December 18, 2020, to elevate
will require insightful management by our physician
the IES to full committee status. This new International
volunteer leaders in conjunction with the voices and
Committee (IC) is well positioned for meaningful
experiences of the membership.
interaction with the IAEA under Dr. Abdel-Wahab’s
Today, I want to return to another of those topics:
dual role leadership for the next two years. It will be
global oncology. To quickly review, ASTRO has
incumbent, however, on those ASTRO members who
been involved in global oncology for the past decade.
are interested in global oncology — and there are many
Perhaps the most successful program has been a joint
— to channel your passion by volunteering on the IC
venture with ARRO that began in 2011 to provide
as ASTRO deepens its commitment to alleviating
funding for three senior residents to acquire hands-on
cancer disparities in LMICs and rural and urban
experience in global radiation oncology. The Global
America. I also call upon my colleagues in academia,
Health Scholars program has placed 24 individuals in
especially those in SCAROP and ADROP, to explore
a variety of settings, giving them valuable exposure to
the possibility of adding a global health component
diverse clinical environments and an opportunity to
to resident education programs (a great undertaking
consider careers in global health, as some have done. In
for a junior faculty member!), as well as investigating
September 2019, the ASTRO Board of Directors voted
creative avenues for attending physicians to volunteer
unanimously to fund the program for another five years
for overseas assignments without penalty to their tenure
and to identify opportunities to increase that funding
track. It is an entirely achievable proposition as outlined
and potentially expand the program. Our International
in some detail by University of Pennsylvania Chair, Jim
Education Subcommittee (IES) has worked with a
Metz, MD, during the Presidential Symposium last
variety of stakeholders, including other specialty groups,
October. Reach out to him — he remains a valuable
to help realize the objectives of the Global Task Force on
resource!
Radiotherapy Cancer Control, which I discussed in great
As I write this, the first steps are being taken by the
depth during my Presidential Symposium, by expanding
IAEA to create a new International Radiation Oncology
radiotherapy resources in low- and middle-income
Society, an umbrella organization that would comprise
countries (LMICs) to help mitigate access disparity.
various specialty societies — ASTRO, ESTRO, AAPM,
Prior to the pandemic, I proposed the creation of
among others — to coordinate activities and prevent
an International Council to spotlight the issue and
deepen ASTRO’s commitment, and while there was Continued on page 28
4 | ASTROnews • SPRING 2021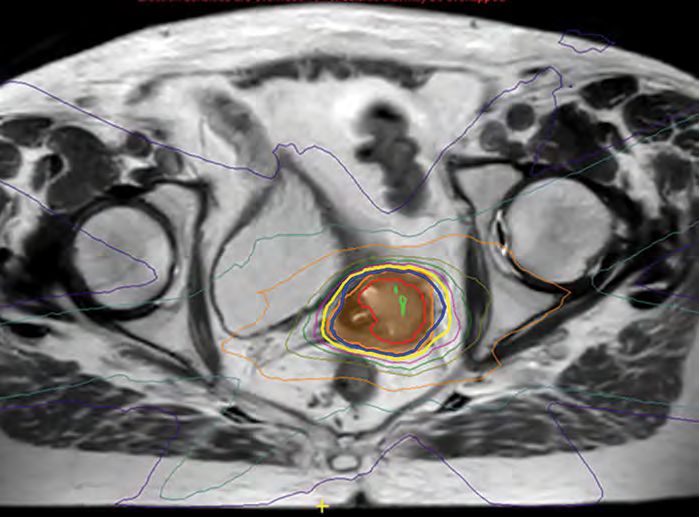
SOCIETY
SOCIETY NEWS
NEWS
Best of ASTRO licensing opportunities available
BY UĞUR SELEK , MD, FASTRO
I HAVE HAD THE PRIVILEGE provides new approaches to help them manage patient
of being coordinator of one of care, and over 60% say they intend to change their
the pilot programs, along with practice and/or patient care as a result.
India and Mexico, for the Best The Best of ASTRO meeting content comes from
of ASTRO Licensing program, which started the ASTRO Annual Meeting, where the Scientific
in 2014. The Turkish Society for Radiation Program Committee selects the “best of ”
Oncology has held a Best of ASTRO A L LY L I C ASTRO presentations, resulting in up to
I EN
IC
meeting annually since then. 100 abstracts in the major disease sites
F
SE
OF
The event in Istanbul, organized plus the faculty discussant presentations.
by the Turkish Society for Radiation D We are pleased to be a part of this
Oncology, is presented in Turkish by ongoing commitment by ASTRO
NG
Turkish faculty who have attended the to extend the reach of educational
20
ASTRO Annual Meeting. This event 1 opportunities around the world and
TI
2
AN EE
is considered one of the Society’s annual NUAL M ® look forward to a continued partnership
courses and allows a friendly gathering with ASTRO on behalf of our local
for attendees. Although the overall expenses, physician community. For more information
including the ASTRO fee, are a little over the on the Best of ASTRO Licensing program, visit
total revenue supplied by corporate sponsorship, no www.astro.org/BOAlicensing.
registration fee is required, as expenses are covered by
the Society for its members. Uğur Selek, MD, FASTRO, is chair at American Hospital,
Attendance is typically around 200-250 MD Anderson Department of Radiation Oncology,
practitioners and faculty, about a third of all Society Istanbul; professor, Koc University, Department of
members. We are pleased to report that over 95% Radiation Oncology, Istanbul; and adjunct professor,
of attendees would recommend the meeting to a University of Texas, MD Anderson Cancer Center,
colleague. Over 90% of attendees say that the meeting Department of Radiation Oncology, Houston.
In Memoriam
ASTRO has learned that the following members have passed away.
Our thoughts go out to their family and friends.
Alexander K.P. Chan, MD, Calgary, Alberta, Canada
Hermann van der Vyver, MD, Palmerston North, New Zealand
The Radiation Oncology Institute (ROI) graciously accepts gifts in memory of or in tribute to individuals.
For more information, visit www.roinstitute.org.
ASTROnews • SPRING 2021 | 5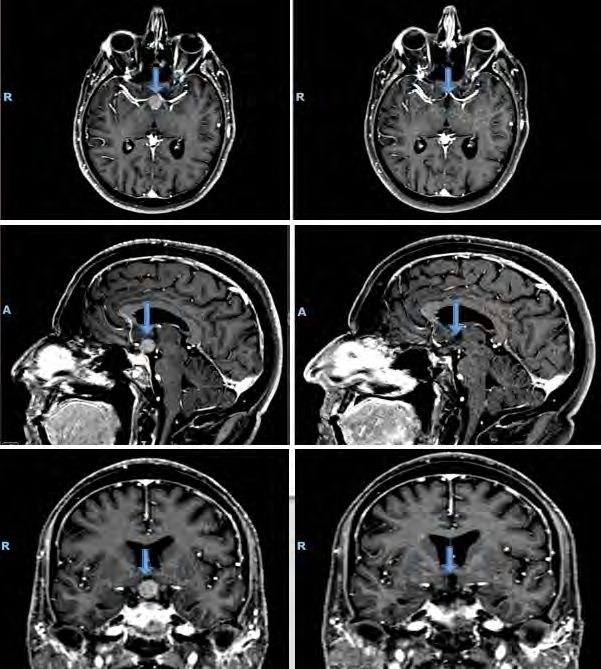
SOCIETY NEWS
Advocacy’s 2020 buzzer beater and 2021 game plan
BY COLIN WHITNEY, ASTRO GOVERNMENT RELATIONS SPECIALIST
LAST YEAR WAS ONE FOR THE RADIATION ASTRO staff, these efforts resulted in a delay in the
ONCOLOGY RECORD BOOK, thanks not only to implementation date of the RO Model until January
historic struggles, but also historic triumphs. Life- 1, 2022, saving model participants approximately $45
altering developments came seemingly every month, million in 2021. In addition, by partnering with other
making uncertainty and oftentimes pessimism the affected medical specialty societies, ASTRO secured a
norm. But as the year came to its end, things started to significant reduction in the E/M payment cuts, saving
turn for the better. radiation oncology approximately $100 million in
ASTRO Advocacy faced a similar timeline of 2021. While the delay of the RO Model start date is a
challenges in 2020. With a flawed radiation oncology welcome win for would be participants, ASTRO will
alternative payment model (RO Model) and Medicare not settle for just the delay and will continue to work
payment cuts set to start in January 2021, the waning toward fixing the RO Model before it’s implemented.
days of 2020 were looking bleak, as progress stalled. “This is a prime example of the power of grassroots
The ASTRO Advocacy team of volunteers and staff did advocacy,” said ASTRO Chair Thomas Eichler, MD,
not let that discourage them, though, and continued to FASTRO. “Engagement is crucial to our efforts to
work toward the Society’s goals. Thankfully, the hard effectively influence Congress in a rapidly evolving
work paid off, and ASTRO secured crucial year-end and often hostile regulatory environment. ASTRO
wins for radiation oncology. Here’s a breakdown of how members need to understand the importance and value
2020 shook out and what lies of taking action and raising their
ahead for ASTRO Advocacy in collective voices. Supporting
2021. “Engagement is crucial to our efforts ASTRO’s advocacy efforts is the
Between the release of the to effectively influence Congress in responsibility of every domestic
RO Model and the payment a rapidly evolving and often hostile member.”
cuts triggered by evaluation regulatory environment.” Another priority for
and management (E/M) ASTRO Advocacy in 2020 was
coding changes as part of the advancing the fight to fix prior
2021 Medicare Physician Fee Schedule (MPFS), authorization. ASTRO continued its push for members
Medicare related priorities required a lot of energy of Congress to support legislation that would take
last year. Given the financial instability caused by the the first steps in fixing runaway prior authorization
COVID-19 public health emergency, the drastic cuts requirements. House legislation now boasts more than
in both the RO Model and E/M would have added 280 bipartisan co-sponsors. Additionally, ASTRO
unnecessary burden to already struggling providers. helped foster the introduction of a companion prior
To combat these cuts, ASTRO mobilized authorization bill in the Senate, which sets the stage for
campaigns to delay the implementation of the RO ASTRO’s 2021 push to have the new Congress finally
Model and reduce the E/M cuts. The Advocacy team take action on much needed prior authorization reform.
organized two RO Model oversight letters to the While these are all great achievements, ASTRO
Department of Health and Human Services (HHS) Advocacy will not be resting on its laurels, and we
signed by 22 bipartisan members of Congress, sent hope members won’t either. The RO Model still needs
countless letters to HHS and the Centers for Medicare vast improvements, and prior authorization reform is
and Medicaid Services (CMS) advocating for changes a battle far from won. The powerful collaboration of
and secured support from key stakeholders, including Advocacy leadership and ASTRO members, shared
the American Medical Association and the American through our grassroots advocacy platform, is the key
Hospital Association. ASTRO membership also rallied for future success. Keep an eye out for ASTRO action
to send over 2,000 messages to their representatives alerts, and make sure your representatives and senators
and senators as part of five grassroots campaigns aimed know how they can support the radiation oncology
at urging Congress to take action. community, and together we can make 2021 another
When combined with direct lobbying from successful year.
6 | ASTROnews • SPRING 2021
WHAT’S NEW
I N R A D I AT I O N O N C O L O G Y
The following articles take you into the clinic and lab to learn the
latest advancements in current practice and research, as well as a
realistic look at what’s working (and not) for virtual meetings and
what’s here to stay in virtual education and training.
READ MORE »
In order to specifically address what's new in radiation oncology, specific vendors and equipment have been identified by authors
in some of the following articles. ASTRO does not endorse specific vendors or equipment. In addition, these articles present the
views of the authors and do not necessarily represent the views of ASTRO.
ASTROnews • SPRING 2021 | 7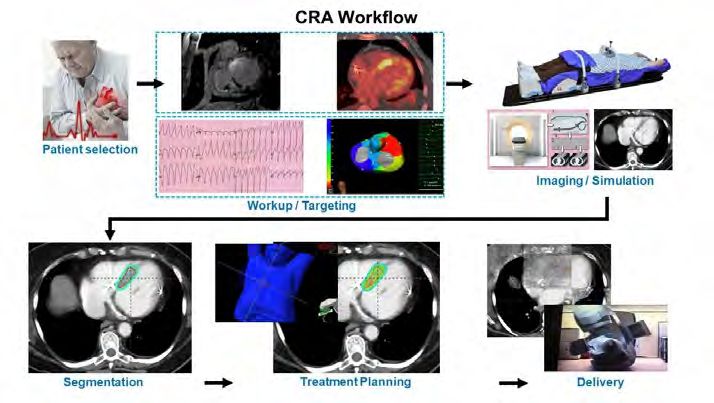
MRI-GUIDED RADIOTHERAPY: FROM “PEEK AND SHOOT”
TO REAL-TIME ADAPTIVE RADIATION THERAPY
BY AMAR U. KISHAN, MD, MINSONG CAO, PHD, AND MICHAEL L. STEINBERG, MD, FASTRO
THE LATE 1990s AND EARLY 2000s witnessed the deformation and stochastic motion, ART provides the
emergence of novel radiation therapy technologies at ability to minimize toxicity while allowing focused
an almost unprecedented pace, with the advent and intensification or de-intensification.5, 6 For online
widespread implementation of intensity-modulated MRgRT ART, an on-board MRI image is obtained
radiation therapy, modern image-guided radiation prior to treatment and used to evaluate target and
therapy and stereotactic body radiation OAR anatomy. Our workflow has required a
therapy. All of these advancements improved dosimetrist, physicist and physician to review
the therapeutic ratio. We believe that MRI- OAR and target dosimetry based on either rigid
guided radiation therapy (MRgRT), which or deformed transfer of contours and manual
is a nascent technology as we enter this new refining of critical structures (Figure 1). If
decade, will be the next such technology. As deemed appropriate per pre-specified criteria,
of 2021, there are two commercially available a new plan is generated for consideration of
linear accelerators that can deliver MRgRT: delivery. However, this process does significantly
the Viewray MRIdian MR Linac (Viewray Amar U. Kishan, MD extend treatment time, likely necessitating auto-
Inc, Oakwood, Ohio), which uses a 0.35 segmentation tools for streamlining widespread
Tesla MRI, and the Elekta Unity (Elekta implementation.7
AB, Stockholm, Sweden), which uses a 1.5 We have primarily explored MRgRT for the
Tesla MRI. The purpose of this article is treatment of prostate cancer and hepatobiliary/
to provide an overview of the operational pancreatic malignancies. MRgRT has multiple
process of implementing an MRgRT potential benefits with regard to prostate
program and briefly discuss ongoing clinical radiotherapy.8 These include allowing smaller
trials investigating novel applications of this planning target volumes due to improved motion
technology. management, lower uncertainty from superior
Our department began using the Minsong Cao, PhD soft-tissue contrast, lower contouring uncertainty
legacy tri-60Co-teletherapy platform from from MRI-MRI registration versus MRI-CT
ViewRay in December 2014. In December fusion, the capacity for online ART, the lack of
2019, we implemented the MRIdian LINAC. need for fiducial markers and auxiliary diagnostic
All patients undergo consecutive CT MRIs for treatment planning and lack of
simulation scans and MR simulation scans radiation dose from on-board imaging. These
on the MRIdian LINAC. While MRI-only advantages could be leveraged to improve quality
workflows have been described,1, 2 we have of life following treatment and/or intensify
retained an in-department CT simulator treatments (e.g., with simultaneous integrated
for reasons of practicality and expanded boosting of MRI-defined lesions). ART may be
access. Particular challenges to an MRI- particularly important for post-prostatectomy
Michael L. Steinberg,
only workflow are difficulties with electron MD, FASTRO radiotherapy given the considerable organ
density information required for accurate deformation in that clinical context.9 While
dose calculation and the delivery of treatments that several smaller reports have been published, the only
are directed by radiopaque fiducial markers. MRgRT- prospective data to date for prostate SBRT with
specific phantoms and MR-safe devices are required for MRgRT technology come from a recently reported
quality assurance as well. 3, 4
phase II trial (NCT03961321) of 101 patients.10
A major advantage of both MRgRT platforms Bruynzeel et al. delivered MRI-guided SBRT in 5
is the ability to perform online adaptive radiation fractions of 7.25 Gy to the target volume using daily
therapy (ART). By actively integrating information plan adaptation, simultaneously limiting the urethra
regarding interfractional changes in anatomy, organ dose to 6.5 Gy per fraction. Acute CTCAE version
8 | ASTROnews • SPRING 2021Figure 1. Online Adaptive Radiotherapy Schema
INITIAL PLANNING ONLINE ADAPTIVE PLANNING Treatment fraction n
MR and CT simulation Patient Setup
MRI Scan and
MR/CT fusion
Position Correction
for electron density
Target/OAR contouring N Anatomic change
deems adaption?
Plan optimization and Y
dose calculation
Rigid/Deformable Registration
and Contour propagation
N
Plan Evaluation Review and Refine Contours
IN THE CLINIC
Y
Predict dose
N
Plan QA
N
Dose change significant?
Y
Y
Re-planning
4.0 grade ≥2 genitourinary and gastrointestinal
Y
toxicity incidences were 19.8% and 3.0% at the
end of MRgRT-SBRT; these compare favorably
to the rates of 27.4% and 15.3% with modern, N
Adaptive Plan Evaluation
IMRT-based planning reported in the SBRT
arm of the PACE-B trial.11 Our institution
is currently running the phase III MIRAGE Y
trial (NCT04384770), which is designed to
rigorously evaluate whether MRI-guided SBRT
N
offers an improved acute GU toxicity profile Adaptive Plan QA
over CT-guided SBRT. This trial allows, but
does not mandate, ART on the MRgRT arm
(Figure 2). We have recently accrued to the Y
phase II SCIMITAR trial (NCT03541850),
which explored SBRT in the post-radical Pre-TX Motion Assessment
prostatectomy setting.
MRgRT, particularly with ART, also is
Continued on following page Beam On
ASTROnews • SPRING 2021 | 9Figure 2. Potential for Adaptive Prostate SBT
Amar U. Kishan, MD, is the vice-chair of Clinical
and Translational Research and chief of the
Genitourinary Oncology Service in the Department
of Radiation Oncology at UCLA.
Minsong Cao, PhD, is an associate professor at the
Department of Radiation Oncology at UCLA,
where he also serves as the program director of the
Medical Physics residency program.
Michael Steinberg, MD, FASTRO, is a professor
and chair of the Department of Radiation Oncology
at UCLA and a former ASTRO President, as well
as a recipient of the ASTRO Gold Medal in 2017.
References
conceptually attractive for hepatobiliary/ 1 Paulson ES, Crijns SPM, Keller BM, et al. Consensus opinion
pancreatic malignancies.12 The complex motion on MRI simulation for external beam radiation treatment
planning. Radiother Oncol. 2016;121(2):187-192. doi:10.1016/j.
and deformation patterns of the target, liver, radonc.2016.09.018.
2 Tyagi N, Zelefsky MJ, Wibmer A, et al. Clinical experience and
bowel and stomach limit the delivery of workflow challenges with magnetic resonance-only radiation therapy
adequate doses of radiation without risking simulation and planning for prostate cancer. Phys Imaging Radiat
Oncol. 2020;16:43-49. doi:10.1016/j.phro.2020.09.009.
catastrophic toxicities. The tumors themselves 3 Singhrao K, Fu J, Wu HH, et al. A novel anthropomorphic
can be impossible to see with CT-based imaging, multimodality phantom for MRI-based radiotherapy quality assurance
testing. Med Phys. 2020;47(4):1443-1451. doi:10.1002/mp.14027.
requiring surrogate-based image-guided 4 Hu Q, Yu VY, Yang Y, et al. Practical Safety Considerations
radiotherapy (e.g., with alignment to implanted for Integration of Magnetic Resonance Imaging in Radiation
Therapy. Pract Radiat Oncol. 2020;10(6):443-453. doi:10.1016/j.
fiducial markers) and introducing errors from prro.2020.07.008.
MRI-CT fusions for contouring. A recent 5 Yan D, Vicini F, Wong J, Martinez A. Adaptive radiation therapy. Phys
Med Biol. 1997;42(1):123-32. doi:10.1088/0031-9155/42/1/008.
multi-institutional study of 26 patients receiving 6 Glide-Hurst CK, Lee P, Yock AD, et al. Adaptive radiation therapy
MRgRT-based liver SBRT found excellent (ART) strategies and technical considerations: A state of the ART
review from NRG Oncology. Int J Radiat Oncol Biol Phys. 2020;In
local control rates withClifford Robinson, MD Geoffrey Hugo, PhD Phillip Cuculich, MD
shocks. This procedure requires several hours of
mapping and ablation using heat generated by
radiofrequency energy. In patients with advanced
cardiomyopathy, risk of serious procedural
complications (i.e., bleeding, stroke, heart failure
and death) approaches 10%, VT recurrence is
~40% and one-year survival is under 50%. In
increasingly high risk patients, VT recurrence
rates and survival parallel metastatic lung cancer.1
Stereotactic ablative radiotherapy (SABR)
has been proposed as one option to deliver
noninvasive ablation for VT. In theory, SABR
SABR PROPOSED AS improves the patient experience by both reducing
IN THE CLINIC
procedural risk and providing a more complete
NONINVASIVE CARDIAC homogenization of the scar than can be achieved
RADIOABLATION (CRA) with a small RF catheter tip. In more than a
dozen preclinical animal studies, single doses of
FOR IMPROVED VT radiation ranging 5-160 Gy were delivered to
portions of myocardium with few serious adverse
PATIENT EXPERIENCE events. Cardiac structural changes were noted
around 25-30 Gy.2
BY CLIFFORD ROBINSON, MD, GEOFFREY HUGO, PHD,
AND PHILLIP CUCULICH, MD In 2015, we published our initial experience
with a totally noninvasive cardiac radioablation
(CRA) workflow (see figure on following page)
SUDDEN CARDIAC DEATH (SCD) represents
using noninvasive scar and electrical imaging
a major worldwide public health problem,
combined with a single SABR dose of 25
accounting for 15-20% of all deaths. Ventricular
Gy in five patients with high risk refractory
tachycardia (VT), the most common source
VT.3 Overall VT reduction was 99%, with no
of SCD, is caused by abnormal electrical
serious radiation related toxicity. Subsequently,
circuits formed within scarred heart muscle,
we carried out a prospective phase I/II trial
frequently from a previous myocardial infarction.
(ENCORE-VT, NCT02919618) of 19
Treatment for individuals with VT is limited
additional patients with high risk refractory
to a combination of an implantable cardiac
VT using the same CRA workflow. Overall
defibrillator (ICD) and an antiarrhythmic drug,
VT reduction of 94% was achieved, with
such as amiodarone. If the medication fails to
concomitant reductions in antiarrhythmic
prevent VT, then the ICD delivers a life-saving,
drug use and improvements in QoL.4 CRA-
high-energy shock.
related late adverse events included two
Unfortunately, ICD shocks are painful and
grade 3 pericardial effusions and one grade 3
have a substantial negative impact on quality
gastropericardial fistula, all of which presented
of life. Catheter ablation (CA) is an invasive
two years after treatment. More than a dozen
procedure used to treat the electrical short
additional case series have been reported to date
circuits in scarred heart tissue and prevent ICD
Continued on following page
ASTROnews • SPRING 2021 | 11in patients with high risk refractory VT, largely echoing of experience in radiation oncology have shown us
the results achieved in ENCORE-VT. 2 the perils of introducing new technologies without
Many questions remain about CRA. What is the carefully controlled clinical trials. With careful
biologic mechanism for VT response? How can we scientific collaboration, standardization of targeting
reproducibly target the VT circuits without catheters? and treatment approaches, and robust enrollment
And how can we leverage existing radiation oncology on prospective clinical trials, patients with limited
infrastructure to extend access to VT treatment treatment options now have hope for a future without
in countries where CA is not available? To answer arrhythmias.
these and other questions, we recently created the
Center for Noninvasive Cardiac Radioablation Clifford Robinson, MD, is a professor of Radiation
(http://cncr.wustl.edu) at Washington University. Oncology and Internal Medicine (Cardiology) at
Targeting VT, unlike contouring a visible nodule Washington University in St. Louis. He is director
in the lung to generate a GTV, involves close of Clinical Trials for Radiation Oncology, chief of
collaboration between the radiation oncologist and Cardiothoracic Radiation Oncology and Stereotactic
electrophysiologist to integrate scar (CT, MRI, PET/ Radiotherapy, and co-director of the Center for
SPECT, Echo) and electrical (12-lead ECG, prior Noninvasive Cardiac Radioablation (CNCR).
catheter maps) data to define a target on the planning
Geoffrey Hugo, PhD, is a professor of Radiation
CT. This exercise is more akin to defining a CTV,
Oncology at Washington University in St. Louis. He is
where the multimodality data suggests a “zone”
interim director of Medical Physics and director of the
of microscopic disease harboring the VT circuits.
Computational Radiotherapy Lab (CORAL).
This process does not easily lend itself to image co-
registration, due to different scan scenarios (e.g., Phillip Cuculich, MD, is an associate professor of Internal
breath-hold/ECG-gated vs. free-breathing/non- Medicine (Cardiology) and Radiation Oncology at
gated), ubiquitous artifact from the ICD and leads, Washington University in St. Louis. He is co-director of the
different scan orientations and routine use of non-3-D Center for Noninvasive Cardiac Radioablation (CNCR).
acquisitions in cardiac imaging, and lack of imaging
data to co-register (ECG). To address this, our group
has devised a robust method to integrate data based on References
the American Heart Association 17-segment model, 1 Tzou WS, Tung R, Frankel DS, et al. Ventricular Tachycardia Ablation in
Severe Heart Failure: An International Ventricular Tachycardia Ablation
which is more geometrically stable and readily defined Center Collaboration Analysis [published correction appears in Circ Arrhythm
Electrophysiol. 2018 Aug;11(8):e000029]. Circ Arrhythm Electrophysiol.
on the planning CT without the need for image co- 2017;10(1):e004494.
registration. 2 van der Ree MH, Blanck O, Limpens J, et al. Cardiac radioablation-A
systematic review. Heart Rhythm. 2020;17(8):1381-1392.
There is an urgent need to confirm efficacy and 3 Cuculich PS, Schill MR, Kashani R, et al. Noninvasive Cardiac Radiation for
safety of CRA in prospective trials before this Ablation of Ventricular Tachycardia. N Engl J Med. 2017;377(24):2325-2336.
4 Robinson CG, Samson PP, Moore KMS, et al. Phase I/II Trial of
treatment becomes readily available off-label. Decades Electrophysiology-Guided Noninvasive Cardiac Radioablation for Ventricular
Tachycardia. Circulation. 2019;139(3):313-321.
12 | ASTROnews • SPRING 2021TREATMENT OF OLIGOMETASTATIC CANCERS:
RECENT LESSONS AND NEW HORIZONS
BY DAVID PALMA, MD, PHD
NINE YEARS AGO, in February 2012, I was to undertake removal of the metastasis as well
18 months into my new practice as radiation as the primary growth”.1 Viewed through the
oncologist, and my new trial, called SABR- modern lens of evidence-based medicine, such
COMET, was not accruing well. Actually, it was a strong conclusion from a case report seems
not accruing at all. We were four months in with irresponsible. But they might have been right
a grand total of zero patients enrolled. I was (apart, of course, from neglecting to predict
getting worried. that SABR would come along to challenge the
That February, I met a patient who seemed surgical approach).
like a good candidate. He had a single adrenal Although the oligometastatic paradigm has
metastasis from colorectal cancer that had grown been around for decades, it’s only in the past
quickly to 4.9 cm. He was interested in the few years that we’ve seen a concerted effort to
trial, but I was nervous. I had never treated an test the paradigm in randomized trials. While
adrenal metastasis, and the lesion was big, just there isn’t space here to discuss them all (for
a hair below the 5 cm cutoff. I called one of my that, I encourage you to read an excellent recent
mentors, George Rodrigues, MD, PhD, for some review2), now is a good time to reflect and ask:
IN THE CLINIC
advice. “Sometimes, you just have to put the first What have we learned?
patient on trial,” he told me. We needed to start The first lesson is that the outcome achieved
somewhere, and as long as we could do it safely, by my first COMET patient is not typical. Most
we should proceed. He made two points. First, patients with oligometastases are not cured with
in his experience, he had learned that once a first SABR, but they progress at some point with
patient enrolls, the trial comes to the forefront new metastases. In SABR-COMET, fewer than
of everyone’s mind and accrual increases quickly. 20% of patients made it to five years without
Second, he would help me with the planning to progression. This lesson has impacted my consent
ensure it was safe. discussions with patients. I now tell them that,
Fast forward to today, and it turns out that although we hope the cancer doesn’t come back,
Dr. Rodrigues was right on both counts. After unfortunately most times it does. In some cases,
my patient enrolled, accrual took off, and the we can do SABR again, but only a minority of
trial completed pretty much on time. The people will be free of disease long term.
treatment worked perfectly in this patient, with A second lesson is that safety should always
no toxicity and no recurrence. I’m due to see him be our first priority, just as it was for that 4.9
next month for his nine-year follow-up. cm adrenal lesion. Although many patients
The treatment of patients with have no toxicity from SABR, the treatment
oligometastases is a hot topic today, but it’s is not harmless. In the SABR-COMET trial,
not a new idea. The term “oligometastasis” was we reported a 4.5% risk of treatment-related
coined over 25 years ago by Sam Hellman, MD, mortality. In the Alliance A021501 trial of
FASTRO, and Ralph Weichselbaum, MD, but chemotherapy +/- SABR (or hypofractionated
the paradigm goes back decades further. The radiation) for borderline-resectable pancreatic
earliest record, as far as I’m aware, is from 1939, cancer, overall survival was 20% lower in the
in a case report of a 55-year-old woman cured SABR arm.3 In planning SABR, most radiation
of primary renal cancer and lung metastasis by oncologists will compromise the dose to areas of
surgical resection of both lesions. The surgeons the PTV if there is any concern about normal
concluded with characteristic certainty: “If a structures, but a decade ago, that approach wasn’t
metastasis is apparently solitary and accessible clearly established. It went against radiation
to surgical removal, it is definitely worthwhile Continued on following page
ASTROnews • SPRING 2021 | 13Figure 1. Value of IV Contrast
oncology planning orthodoxy to leave some areas of specific data for oligometastatic lung and breast
the PTV “cold.” Overall, we need to remain cautious in cancers. The histology-agnostic SABR-COMET-3
our radiation planning and dose selection. The use of (1-3 mets) and SABR-COMET-10 (4-10 mets), both
contrast (intravenous or oral, depending on the target’s powered for a primary endpoint of overall survival, are
location) can be very helpful. The figure above shows also expected to complete in the next few years. While
the value of IV contrast (right) in visualizing a hilar we’ve learned a lot in the past few years about treating
node, compared to a scan without contrast (left). oligometastatic cancers, we are certain to learn a whole
A final lesson to highlight is that SABR does affect lot more very soon.
the immune system, but there’s more to be learned
before we can use SABR merely for a hypothesized David Palma, MD, PhD, is a professor in the Department
abscopal effect. The ORIOLE phase II trial of of Oncology at Western University in Ontario, Canada.
observation vs. SABR in patients with oligometastatic
cancers showed not only an improvement in References
1 Barney J, Churchill E. Adenocarcinoma of the kidney with metastasis to the lung
progression-free survival with SABR, but also an cured by nephrectomy and lobectomy. J Urol. 1939;42:269-276.
increase in T cell clonotypic expansion after SABR.4 2 Onderdonk BE, Gutiontov SI, Chmura SJ. The Evolution (and Future)
of Stereotactic Body Radiotherapy in the Treatment of Oligometastatic
There are tantalizing hints that SABR can modulate Disease. Hematol Oncol Clin North Am. 2020;34(1):307-320.
the immune system, but there is much more to be 3 Katz M, Shi Q, Meyers J, et al. Alliance A021501: Preoperative
mFOLFIRINOXor mFOLFIRINOX plus hypofractionated radiation
learned. therapy (RT) for borderline resectable (BR) adenocarcinoma of the
We are about to enter the era of phase III data for pancreas. J Clin Oncol. 2021;39(suppl 3)377-377.
4 Phillps R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic
SABR in oligometastatic cancers. The NRG trials LU- Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2
002 and BR-002 will provide important histologically Randomized Clinical Trial. JAMA Oncol. 2020;6(5):650-659.
ASTRO staff donated
ASTRO STAFF GIVES BACK more than 1,631
pounds of food —
the largest single
In February, ASTRO staff donated $2,632, contribution of the
week for AFAC!
plus an additional $500 donation
from ASTRO, for a total of $3,132 to
purchase food for the local food bank,
Arlington Food Assistance Center
(AFAC). AFAC serves Arlington County,
Virginia, residents in need. Annually,
ASTRO donates food and time through
volunteering to the AFAC.
14 | ASTROnews • SPRING 2021MAYO CLINIC JACKSONVILLE SITE OF FIRST
CLINICAL CARBON ION ACCELERATOR IN THE U.S.
BY BRADFORD HOPPE, MD, MPH
ON NOVEMBER 15, 2019, Mayo Clinic Currently, carbon ion therapy is offered
announced plans to expand their particle therapy at centers in Japan, China, Germany, Austria
footprint in Florida with a new proton therapy and Italy. Carbon ion therapy has most often
and the first clinical carbon ion accelerator been used to treat unresectable bone and soft
in the United States to be built at the Mayo tissue sarcomas, prostate cancer, hepatocellular
Clinic campus in Jacksonville, Florida. While carcinomas, recurrent rectal cancer, pancreatic
heavy ion therapy was first developed at the cancer, non-squamous head and neck cancers,
Lawrence Livermore laboratories in the 70s and lung cancer and high-grade gliomas. However, it
80s using helium, carbon, argon and neon, the is being explored in the management of several
center closed in 1993 and no center in the U.S. other types of cancers and may be more effective
IN THE CLINIC
since then has offered treatment with heavy ion in priming the immune system to establish an
therapy. abscopal effect.
Mayo Clinic is well positioned to lead the The integrative oncology building on the
effort to bring heavy particle therapy back into Mayo Clinic Jacksonville campus will be the
clinical practice in the U.S., given its clinical and new home for the Department of Radiation
research work in proton therapy at the Mayo Oncology with linear accelerators, two proton
Clinic campuses in Rochester, Minnesota, and gantries and a carbon ion fixed beam room. It
Phoenix, Arizona. Furthermore, carbon ion is expected to be completed in 2024, with the
therapy has been an area of keen interest for first proton patients treated in 2025 and the first
development by Mayo Clinic for the last decade, carbon ion therapy patients in 2027.
with close collaboration with QST Hospital In preparation for the expansion, Mayo Clinic
(formerly NIRS Hospital) in Chiba, Japan, investigators are developing collaborations with
which was the first and longest-dedicated carbon other carbon ion centers to conduct pre-clinical
ion therapy (CIT) center in the world. research projects to better understand the physics
CIT is similar to proton therapy in that the and radiobiology of carbon ion therapy. They are
charged particle beam can be delivered to specific also working together to develop comparative
depths to ensure that most of the radiation dose effectiveness research studies to better qualify
falls within the target as opposed to normal the benefits of carbon ion therapy over other
tissue, which is the main problem with photon treatment approaches. Additionally, over the next
radiation. Carbon ion therapy differentiates itself few years Mayo Clinic will develop phase I/II
from proton therapy in that the LET (linear trials, which will be ready to launch once carbon
energy transfer) is higher, leading to a higher ion therapy is ready for clinical use.
relative biologic effectiveness (RBE), which
translates into more DNA double strand breaks Bradford Hoppe MD, MPH is professor of
within the target cells. The higher RBE of CIT Radiation Oncology and the medical director of
makes it especially important in the management Particle Therapy at Mayo Clinic in Jacksonville,
of radioresistant cancers, such as hypoxic tumors, Florida.
locally recurrent tumors and specific histologies,
like sarcomas, adenoid cystic carcinomas and
non-small cell lung cancer.
ASTROnews • SPRING 2021 | 15WHAT’S NEW IN THE LAB
Synopses of current research underway in labs at Yale University and the University of Chicago
against IDH1/2-mutant gliomas and other solid
tumors, based our group’s discoveries above.
Ranjit Bindra, MD, PhD, is a physician-scientist at the
Yale School of Medicine. He is a professor of Therapeutic
Radiology and co-director of the Yale Brain Tumor Center.
Cancer Metabolism and
DNA Repair
BY RANJIT BINDRA, MD, PHD
THE BINDRA LABORATORY is focused on the
development of synthetic lethal targeting strategies
to treat a wide range of cancers. We are particularly
interested in developing tumor-selective radio- and Biological Basis for
chemo-sensitizers, using inhibitors of both DNA Oligometastasis
repair and cellular metabolism. In addition, our group BY SEAN PITRODA, MD
is interested in novel, nanoparticle-based drug delivery
strategies to bypass the blood-brain barrier and to allow
THE PITRODA LABORATORY is working toward
more efficacious drug combinations.
improving the treatment of metastatic disease through
Our group recently made the seminal discovery
translational research. Our current investigations
that oncometabolites induce a BRCAness state, which
specifically pertain to establishing the molecular basis
can be exploited by PARP inhibitors. This work was
for curable metastatic disease — termed oligometastasis
published in Science Translational Medicine and
— with a particular emphasis on tumor-host
Nature Genetics. Most recently, we have further
interactions that influence metastatic proclivity.
elucidated the mechanistic basis for mutant IDH1/2-
We believe these investigations will have important
induced BRCAness, and this work was published
implications in the discovery of novel biomarkers and
recently in Nature.
targets used for personalization of cancer treatment.
We have also identified two novel synthetic
We utilized integrated molecular subtyping to
lethal interactions in recent work: DIPG-associated
define the metastatic spectrum of colorectal liver
PPM1D mutations confer exquisite NAMPT inhibitor
metastases, which predicted clinical outcomes for
(NAMPTi) sensitivity via NAPRT silencing, and loss
patients who underwent surgical resection of limited
of MGMT confers synergistic tumor cell killing with
de novo liver metastases independently of established
ATR inhibitor and TMZ combinations. These two
clinical and pathological factors. Importantly, this
studies were published in Nature Communications and
work identified a curable oligometastatic subset of
Cancer Research, respectively.
patients with an immune-activated phenotype that
A unique feature of our program is that we actively
achieved a 95% survival at 10 years following surgical
translate our work from the laboratory directly into
metastasectomy. This study was published in Nature
investigator-initiated (IIT) phase I/II trials. To this
Communications and reviewed in Nature Reviews
end, we recently designed and executed a phase I trial
Clinical Oncology and Journal of Clinical Oncology.
in glioma, which tested a DNA repair inhibitor that
Our present work examines the mechanisms that lead
our laboratory identified in a high-throughput drug
to failed immune activation and poor prognoses in
screen. This trial included a phase 0 component, in
clinical metastases.
which we assessed CNS penetration of the drug. I am
In concert with investigating the biological
also the PI or co-PI of three biomarker-driven phase I/
mechanisms that govern immune evasion in clinical
II trials, which are testing the use of PARP inhibitors
metastases, we are investigating translational
biomarkers that predict immunotherapy responses in
16 | ASTROnews • SPRING 2021patients with metastatic cancers. Building upon reprogrammed by the tumor microenvironment
our recent work on the intratumoral interactions to promote survival after ablative doses of
of radiotherapy and immunotherapy in patients radiotherapy. Our studies identified TGFβ as
with metastatic disease published in Clinical a critical regulator of T cell reprogramming of
Cancer Research and reviewed in Lancet intratumoral T cells. This work was published in
Oncology, I was given a Career Development Nature Communications.
Award from the LUNGevity Foundation to In addition, we identified two novel
characterize tumor and host determinants as mechanisms by which the commensal microbiota
they relate to the survival of non-small cell lung impact the anti-tumor immune responses
cancer patients treated with ablative radiotherapy to radiotherapy. In one study, we found that
combined with immune checkpoint inhibitors. accumulation of the anaerobic Bifidobacterium
We anticipate these findings will ultimately have within the tumor microenvironment converted
important implications in the delineation of non-responder mice into responders by inducing
those patients with potentially curable metastatic type I interferon-STING signaling and
disease from those whose few metastases are part increasing dendritic cell cross-priming in the
of a large cascade of widespread disease, thereby response to anti-CD47 immunotherapy. In an
advancing the paradigm for the treatment of independent study, we showed that depletion
metastatic cancers. of gut Lachnospiraceae through oral vancomycin
administration decreased systemic and
Sean Pitroda, MD, is jointly appointed as an
intratumoral butyric acid levels and augmented
assistant professor in the Department of Radiation
type I interferon-STING signaling by
and Cellular Oncology and Committee on Cancer
promoting a cytotoxic T cell immune response,
Biology. He also serves as a principal investigator in
which improved the efficacy of radiotherapy.
IN THE LAB
the Ludwig Center for Metastasis Research at the
These two studies were published in the Journal
University of Chicago.
of Experimental Medicine.
More recently, we identified a previously
unknown abscopal mechanism of local tumor
irradiation, which synergized with systemic anti-
PD-L1 immunotherapy to kill tumor-induced
Ter cells. Ter cells are erythroid progenitor cells
that promote tumor progression by secreting
artemin, a neurotropic peptide that activates
RET signaling. Importantly, we found that
Radiation-Immunotherapy a decrease in the Ter cell-artemin axis was
Interactions associated with favorable treatment responses to
BY RALPH WEICHSELBAUM, MD, PHD radiotherapy, immune checkpoint blockade or
the combination in patients with advanced or
THE WEICHSELBAUM LABORATORY metastatic solid tumors. This study was published
investigates the importance of host anti-tumor in Science Translational Medicine. Collectively,
immunity in the response to radiotherapy. these studies have elucidated novel strategies to
Specifically, we study the effects of immune target immune cell populations and commensal
cell populations and commensal microbiota microbiota to decrease immune suppression
on the anti-tumor effects of ionizing and resistance to radiotherapy and immune
radiation. Ultimately, our group is interested checkpoint blockade.
in novel mechanisms to abrogate resistance to
radiotherapy by alleviating immunosuppression Ralph Weichselbaum, MD, PhD, is currently the
generated by particular immune cells or Daniel K. Ludwig Distinguished Service Professor
microbiota. and chairman of the Department of Radiation and
Our group recently made a discovery using Cellular Oncology and co-director of the Ludwig
longitudinal in vivo imaging and functional Center for Metastasis Research at the University of
analyses that tumor-resident T cells are Chicago.
ASTROnews • SPRING 2021 | 17You can also read