A Case of Lower Extremity Weakness with Foot Drop Following Intramedullary Nailing of a Pathologic Femoral Fracture - Cureus
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Open Access Case
Report DOI: 10.7759/cureus.6561
A Case of Lower Extremity Weakness with
Foot Drop Following Intramedullary Nailing
of a Pathologic Femoral Fracture
Charles A. Gusho 1
1. Orthopaedic Surgery, Medical College of Wisconsin, Green Bay, USA
Corresponding author: Charles A. Gusho, cgusho@mcw.edu
Abstract
A 62-year-old woman presented with a pathologic femoral fracture. She underwent bilateral
femoral intramedullary nailing (IMN) fixation, and her postoperative course was complicated by
worsening lower extremity weakness and foot drop. Lumbar imaging identified vertebral
compression fractures with foraminal encroachment. The patient was thereafter started on a
radiotherapy regimen and discharged home. Pathologic fractures most commonly occur in the
proximal femur. In some patients, contralateral weakness suggests an additional fracture,
though it may represent spinal involvement. This case explores multiple current treatment
options for pathologic fractures of the femur and spine and suggests that prophylactic
endoprostheses may have greater selective benefit than IMN fixation.
Categories: Oncology, Orthopedics
Keywords: intramedullary nailing, metastasis, pathologic fracture
Introduction
The incidence of metastatic disease will likely increase in the next 20 years with the aging
population. Bony metastasis most commonly occurs in the proximal third of the femur,
resulting in a pathologic or impending fracture [1]. When one presents with a pathologic
femoral fracture, however, it is important to discern lower extremity weakness from a spinal
etiology, as this may differentially affect the surgical plan and necessitate a more
expeditious intervention. Presented here is a case of bilateral lower extremity weakness
following a pathologic femoral fracture secondary to breast metastasis. However, this patient
had weakness from multiple lumbar fractures and delay in spinal MRI permitted the
development of worsening weakness and cauda equina compression. Principally, orthopedic
workup of lower extremity weakness in the setting of a pathologic femoral fracture should
include a spinal evaluation, especially if bilateral weakness is present. Additionally described
Received 12/25/2019
are multiple, currently recommended treatment modalities for prophylaxis or the correction of
Review began 12/27/2019
Review ended 01/02/2020
pathologic fractures of the femur and spine.
Published 01/04/2020
© Copyright 2020 Case Presentation
Gusho. This is an open access article
distributed under the terms of the A 62-year-old woman with no past medical history presented at the behest of her children
Creative Commons Attribution License following an audible “snap” in her right leg while walking at home. Physical examination of the
CC-BY 3.0., which permits lower extremities was remarkable for bilateral weakness and markedly decreased active range
unrestricted use, distribution, and
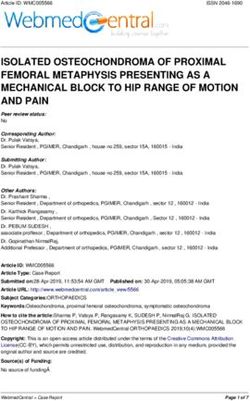
of motion on the right. Imaging revealed an acute, transverse, displaced, and angulated right
reproduction in any medium, provided
femoral fracture, with multiple ill-defined lytic lesions to the pelvis and left proximal femur
the original author and source are
credited. (Figure 1, Figure 2).
How to cite this article
Gusho C A (January 04, 2020) A Case of Lower Extremity Weakness with Foot Drop Following
Intramedullary Nailing of a Pathologic Femoral Fracture. Cureus 12(1): e6561. DOI 10.7759/cureus.6561
FIGURE 1: Pathologic fracture of the right proximal femur
Acute, transverse, displaced, and angulated right femoral fracture (arrow), with multiple, ill-defined
lytic lesions to the right pelvis
FIGURE 2: Bony metastasis of the left femur
Diffuse bone demineralization, with numerous lytic lesions, noted throughout proximal left femur
(arrow). Scattered, metastatic foci likely placing the patient at a higher risk for pathologic fracture.
2020 Gusho et al. Cureus 12(1): e6561. DOI 10.7759/cureus.6561 2 of 7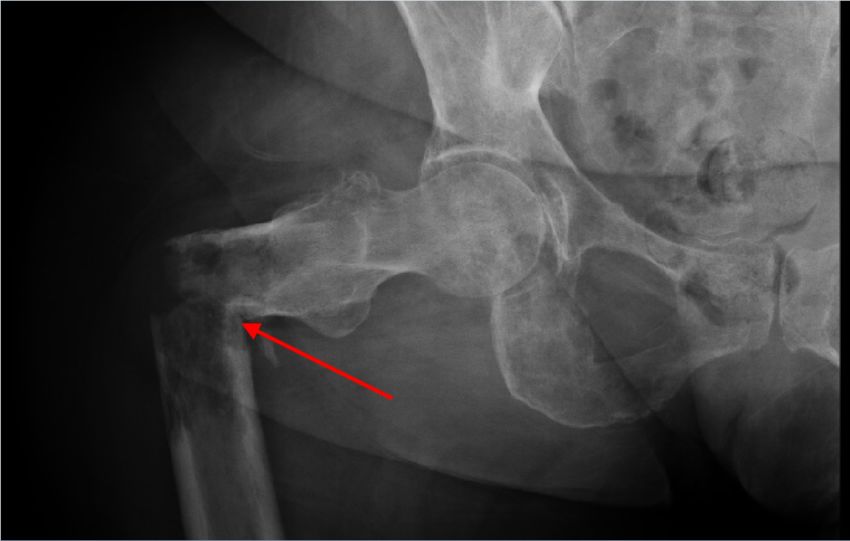
There was no identifiable fracture on the left side. Further examination exposed a necrotic,
fungating left chest wall mass (Figure 3), with left axillary lymphadenopathy suggestive of
metastatic breast disease.
FIGURE 3: Left chest wall mass
12.5 cm x 16.5 cm x 1.0 cm necrotic, fungating left chest wall wound suggestive of metastatic
breast disease
The following day, the patient underwent right femoral IMN fixation using a 12 mm x 420 mm
titanium cannulated nail. Thereafter, she was neurovascularly intact throughout her right lower
extremity and postoperative films showed anatomic alignment (Figure 4).
FIGURE 4: Postoperative right femur
2020 Gusho et al. Cureus 12(1): e6561. DOI 10.7759/cureus.6561 3 of 7
Anterograde intramedullary rod with proximal and distal (not seen) interlocking screws stabilizing
the fracture site. Anatomic alignment.
Then, two days later, with a Mirels’ score of 8, she underwent prophylactic left femoral IMN
fixation. Postoperative films showed anatomic alignment (Figure 5). Following the procedure,
she was neurovascularly intact throughout her left lower extremity. On postoperative Day 3
from the left IMN fixation, she was discharged from the orthopedic service.
FIGURE 5: Postoperative left femur
Intramedullary rod in the left femur extending from the greater trochanter to the distal metaphysis
with proximal interlocking screws and a single distal interlocking screw (not seen). Alignment
appears anatomic. No fractures are identified.
On postoperative Day 5, the patient presented to the rehabilitation unit with worsening
bilateral lower extremity weakness and left foot drop. For the next seven days, she showed no
improvement, and on the eighth day, she developed urinary frequency and incontinence.
Subsequent lumbar MR imaging revealed pathologic compression fractures of L4 and L5, with
epidural tumor invasion and neural foraminal encroachment (Figure 6). She was thereafter
initiated on a palliative radiotherapy regimen and discharged without any further orthopedic or
neurosurgical intervention.
2020 Gusho et al. Cureus 12(1): e6561. DOI 10.7759/cureus.6561 4 of 7
FIGURE 6: Vertebral compression fractures
Severe extensive metastatic disease with pathologic compression fractures of L4 and L5
(arrows) and extensive epidural tumor invasion at L4 and L5 with foraminal neuronal encroachment.
Discussion
IMN fixation or hip arthroplasty (HA) are two treatment options for pathologic femur fractures
that have proven results in providing pain relief and improved functional mobility. In their
prospective study, Picciolo et al. demonstrated the efficacy of IMN fixation for pathologic,
proximal femoral diaphyseal fractures through subjective pain relief and general postoperative
improvement up to six to 10 months [2]. Additionally, research by Guzik et al. identified 122
patients with proximal femoral metastasis who underwent standard or modular endoprosthetic
replacement of the proximal femur. Their data highlight a moderate reduction in visual analog
scale (VAS) pain scores and improved quality of life at 27 months following surgery, suggesting
HA as a viable treatment option [3]. Therefore, there is no doubt that surgical correction is an
evidenced-based option for the treatment of pathologic fractures of the proximal femur.
Similarly, IMN fixation or HA can treat impending fractures. Prophylactic surgical fixation of
the proximal femur is commonly offered to patients with metastatic disease to mitigate the risk
of an impending pathologic fracture. However, as was highlighted in research by McLynn et al.,
the perioperative complication profile has received little attention. In their retrospective study
of 332 cases of prophylactic femoral fixation and 288 cases of pathologic fracture fixation, they
report that when controlling for disseminated cancer, the odds of experiencing an adverse
event (major or minor), death, or prolonged hospital stay were no greater in prophylactic
fixation than in fracture fixation for up to 30 days [4]. Recent data further suggest that patients
who undergo prophylactic stabilization have a lower risk of major complications within 30 days
postoperatively, and shorter hospital stays when compared to patients who underwent post-
fracture stabilization [5]. Despite positive short-term outcomes for both prophylactic and
corrective fixation, however, nonunion and/or tumor progression may lead to long-term
hardware failure. Additionally, implant fatigue can occur as a result of repetitive radiotherapy.
In a study by Johnson et al., 26 patients were noted to undergo conversion hip arthroplasty for
2020 Gusho et al. Cureus 12(1): e6561. DOI 10.7759/cureus.6561 5 of 7the salvage of failed fixation of a pathologic femur fracture, with a greater number of failed
patients having undergone IMN fixation (n=18) [6]. Their data report conversion HA at a mean
13 months after initial fixation, most commonly due to disease progression (n=12), hardware
failure (n=8), and nonunion (n=6) [6]. Therefore, in the era of prolonged cancer survival,
endoprostheses may serve as a reasonable alternative to prophylactic IMN fixation if the
patient portends a relatively favorable prognosis.
Our patient was a 62-year-old female who underwent right open-reduction and IMN fixation of
a pathologic fracture and prophylactic IMN fixation of the left femur. Given her age and lack of
comorbid disease aside from metastatic breast cancer, the initial orthopedic management was
likely appropriate, though incomplete. The original films identified heterogeneous, ill-defined
lytic lesions of the pelvis. Therefore, the question is whether this patient should have had a
more thorough oncologic workup or staging prior to prophylactic surgery on the left, which may
have made her a better candidate for endoprostheses. In a study conducted by Wedin and Bauer
in 2005, 142 patients were treated surgically for proximal femoral metastatic lesions and, not
surprisingly, those treated with IMN fixation had a higher rate of failure (16.2%) when
compared to endoprostheses (13.6%) [7]. This data, in conjunction with the anticipated failure
rate at 13 months in a similar age-matched cohort as described above, suggest endoprostheses
have a greater long-term benefit than prophylactic cephalomedullary nailing. I would argue
that our patient may have had more benefit from an endoprosthesis than IMN fixation.
Second, would the earlier identification of severe lumbar degeneration with cord involvement
have warranted a more aggressive orthopedic workup such as kyphoplasty, vertebroplasty,
and/or fusion with instrumentation? As was mentioned, a delay in lumbar imaging likely lent
itself to worsening lower extremity weakness and neurologic compromise, including foot drop
and urinary incontinence. Taken about 2.5 weeks after initial presentation, MR imaging
identified pathologic compression fractures of L4 and L5, with epidural tumor invasion and
neural foraminal encroachment. Despite its insidious time course, the premature introduction
of rehabilitation without the identification of spinal pathology may have exacerbated the
patient’s symptoms. Additionally, the development of impaired left-sided dorsiflexion with
urinary incontinence would likely have been prevented with a more aggressive spinal workup. A
review of the current literature on the orthopedic management of malignant vertebral
compression fractures (MCVF) suggests surgical intervention, such as kyphoplasty, may be of
benefit. In a retrospective study of 48 patients with MVCF treated with kyphoplasty, significant
improvements in all outcome measurements were observed postoperatively up to two years
following treatment [8]. Additionally, minimally invasive stabilization and circumferential
spinal cord decompression exemplified postoperative efficacy in a case report of a patient with
osteolytic destruction of the vertebral column from metastatic, epidural spinal cord
compression [9]. Therefore, our patient certainly may have benefitted from earlier recognition
of her lumbar fractures, which, with proper orthopedic intervention, such as cord
decompression or kyphoplasty, may have prevented subsequent neurologic dysfunction. This
course of action would likely have decreased her hospital stay, reduced rehabilitation costs, and
led to more prompt adjunct radiotherapy.
Conclusions
Pathologic fractures most commonly occur in the proximal femur, for which there are well-
described, orthopedic surgical treatments. In some patients, contralateral weakness suggests an
additional fracture. However, bilateral weakness may also indicate spinal involvement, and
prompt recognition and/or correction is essential to preserve neurologic function. In this case,
lumbar compression fractures were missed, likely permitting neurologic compromise. This case
not only emphasizes the importance of a thorough musculoskeletal workup for lower extremity
weakness but explores multiple current treatment options for pathologic fractures of the femur
and spine and suggests that within the context of a favorable prognosis, endoprostheses may
2020 Gusho et al. Cureus 12(1): e6561. DOI 10.7759/cureus.6561 6 of 7prove advantageous to IMN fixation of the femur.
Additional Information
Disclosures
Human subjects: Consent was obtained by all participants in this study. Conflicts of interest:
In compliance with the ICMJE uniform disclosure form, all authors declare the following:
Payment/services info: All authors have declared that no financial support was received from
any organization for the submitted work. Financial relationships: All authors have declared
that they have no financial relationships at present or within the previous three years with any
organizations that might have an interest in the submitted work. Other relationships: All
authors have declared that there are no other relationships or activities that could appear to
have influenced the submitted work.
References
1. Jonas SC, Mehendale SM, Bick SM, Baker RP: Current orthopaedic management of bony
metastases in the proximal third of the femur. Hip Int. 2017, 27:1-7.
2. Piccioli A, Rossi B, Scaramuzzo L, Spinelli MS, Yang Z, Maccauro G: Intramedullary nailing for
treatment of pathologic femoral fractures due to metastases. Injury. 2014, 45:412-417.
3. Guzik G: Oncological and functional results after surgical treatment of bone metastases at the
proximal femur. BMC Surgery. 2018, 18:5. 10.1186/s12893-018-0336-0
4. McLynn RP, Ondeck NT, Grauer JN, Lindskog DM: What is the adverse event profile after
prophylactic treatment of femoral shaft or distal femur metastases?. Clin Orthop Relat Res.
2018, 476:2381-2388. 10.1097/corr.0000000000000489
5. El Abiad JM, Raad M, Puvanesarajah V, Rao S, Morris C, Levin A: Prophylactic versus
postfracture stabilization for metastatic lesions of the long bones. J Am Acad Orthop Surg.
2019, 27:709-716. 10.5435/JAAOS-D-18-00345
6. Johnson JD, Perry KI, Yuan BJ, Rose PS, Houdek MT: Outcomes of endoprosthetic replacement
for salvage of failed fixation of malignant pathologic proximal femur fractures. J Arthroplasty.
2019, 34:700-703. 10.1016/j.arth.2018.12.009
7. Wedin R, Bauer HCF: Surgical treatment of skeletal metastatic lesions of the proximal femur.
Endoprosthesis or reconstruction nail. J Bone Jt Surg. 2005, 87:1653-1657. 10.1302/0301-
620X.87B12.16629
8. Qian Z, Sun Z, Yang H, Gu Y, Chen K, Wu G: Kyphoplasty for the treatment of malignant
vertebral compression fractures caused by metastases. J Clin Neurosci. 2011, 18:763-767.
10.1016/j.jocn.2010.09.021
9. Hansen-Algenstaedt N, Knight R, Beyerlein J, Gessler R, Wiesner L, Schaefer C: Minimal-
invasive stabilization and circumferential spinal cord decompression in metastatic epidural
spinal cord compression (MESCC). Eur Spine J. 2013, 22:2142-2144. 10.1007/s00586-013-
2959-2
2020 Gusho et al. Cureus 12(1): e6561. DOI 10.7759/cureus.6561 7 of 7You can also read