A case of Turner syndrome of special chimeric type with papillary thyroid carcinoma and dislocation of hip joint
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A case of Turner syndrome of special chimeric type
with papillary thyroid carcinoma and dislocation of
hip joint
Jinxin Huang
The Third Affiliated Hospital of Soochow University
Xiaohong Jiang
The Third Affiliated Hospital of Soochow University
Long Wang ( 305783449@163.com )
The Third Affiliated Hospital of Soochow University
Case Report
Keywords: Turner syndrome, special chimeric type, thyroid papillary carcinoma;congenital hip
dislocation, case report
Posted Date: April 5th, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2766245/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Read Full License
Page 1/10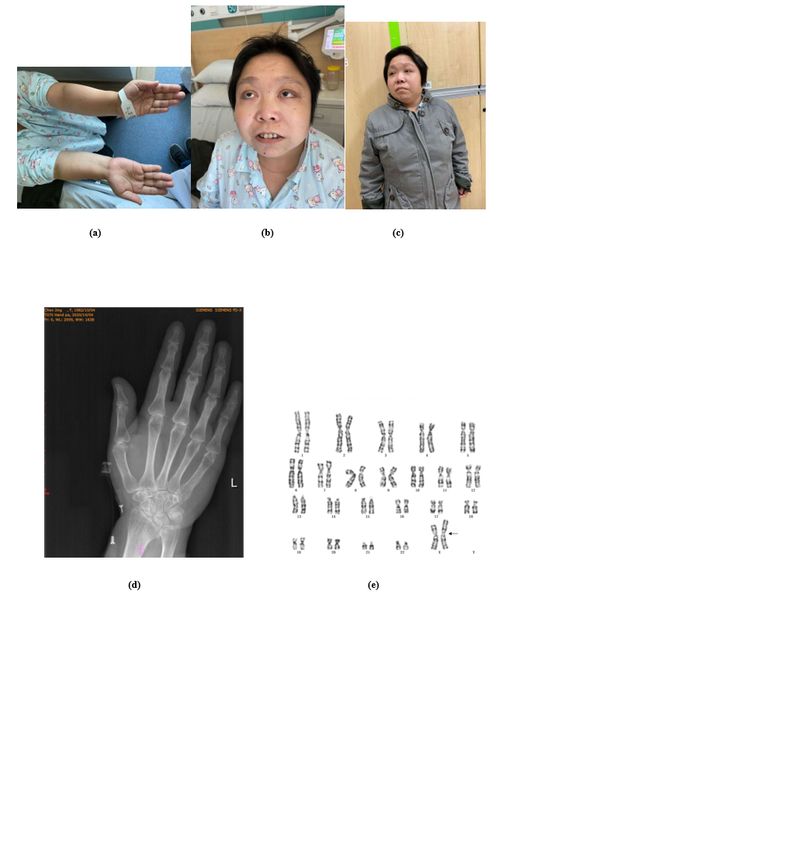
Abstract We found a rare clinical manifestation of Turner syndrome: thyroid papillary carcinoma,dislocation of hip joint with diabetes and osteoporosis . The patient had growth retardation, bone density:
After admitted to the hospital,the fast blood glucose(FPG) was12.04mmol/l,the postprandial blood
glucose(2hPG) was 14mmol/l,Glycosylated hemoglobin(HbA1C) was 10.8%,urinary ketones(+) .The
values of C-peptide (0-30-60-120-180min) were 332.5-697.5-694.7-818.3-790.6pmol/l,
respectively.Gynecological ultrasound: childish uterus, two-sided ovaries are not clear. Cardiac
ultrasound: The aorta is incomplete. Chest lumbar vertebrae positive side: multiple wedge deformation.
Hip X-rays: double hip disloyal (congenital) and short neck [Fig. 2]. Bone density The results of bone
density suggest osteoporosis[Tab1].Follow-up of sex hormone levels was shown in Table 2[Tab2] .
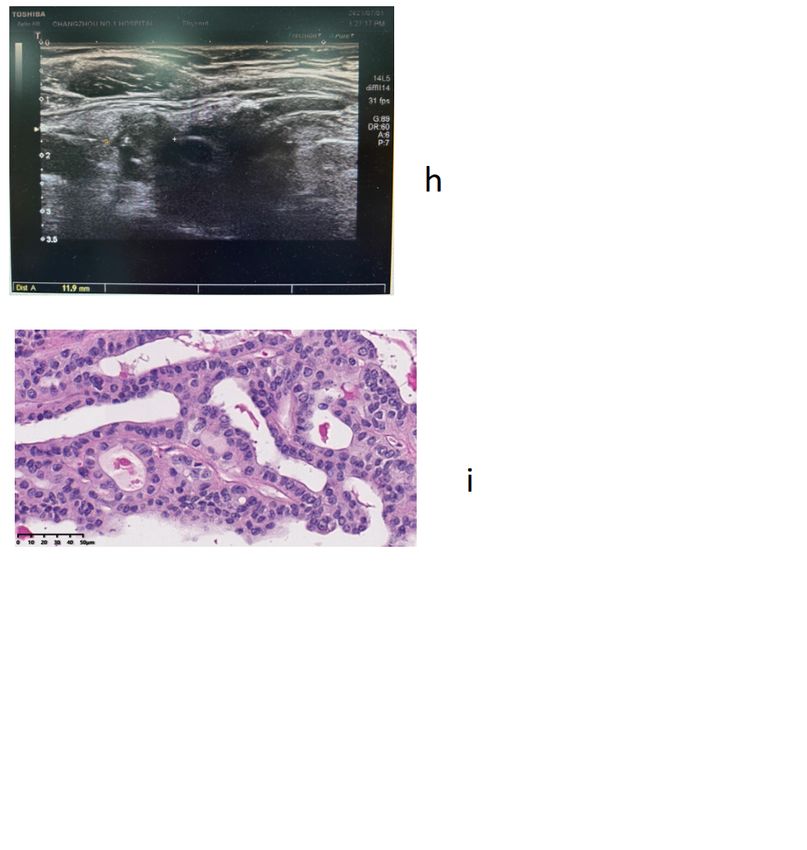
In June 2021, the patient was hospitalized again due to poor blood glucose control. A suspicious thyroid
nodule was found on the left side, about 1.7*1.2cm in size. A thyroid puncture biopsy was performed to
indicate papillary carcinoma of the thyroid, which was positive for BRAF gene. She was referred to the
surgeon for a thyroidectomy. Postoperative pathology revealed left papillary thyroid carcinoma with left
central lymph node metastasis (1/7)[Fig. 3]. So the diaglosis was Turner syndrome combined with
papillary thyroid carcinoma,diabetes, double hip dislocation (congenital) and osteoporosis. In October
2020,we gave Treatment: Insulin 4 IU premeal injections, sitagliptin 100 mg qd, FPG control at 5.7–6.4
mmol/l, 2hPG control at 6.8–9.3 mmol/l, Vitamin D3 calcium carbonate 1 tablet qd, vitamin D 800iu qd.
Levothyroxine sodium tablets 150ug qd. Sex hormone replacement therapy: estradiol valerate tablets
0.25 mg/qd, progestogen not added at this time.By June 2021, we found that the patient's estrogen level
had increased and bone mineral density T-value had increased significantly. In terms of treatment,
Femoston was used to take 1 tablet a day to delay aging[Tab1-2].
Discussion
Papillary thyroid carcinoma is the most common type of thyroid tumor 6. There is an increasing trend of
morbidity in our country, which is a malignant tumor with a relatively good prognosis. However, it should
not be ignored that about 15%-20% of PTC patients will appear recurrence and forward metastasis in the
later stage, especially when they are combined with other gene mutations. So early identification of
patients with multiple mutations is particularly important.
The BRAF gene, located on human chromosome 7, is most commonly mutated in exon 15, the BRAFv600E
mutation, which regulates abnormal activation of the MAPK pathway by encoding RAF family
serine/threonine kinases, leading to differentiated thyroid cancer.
In patients with thyroid papillary carcinoma, there are not only BRAFv600E mutations, but also common
mutations of BRAFv600E and other genes, such as TERT, ALK, etc., among which the common mutations
are accompanied by TERT promoter mutations, accounting for 2.1–9.5% of PTC. Common mutations
may promote the proliferation and distant metastasis of thyroid cancer cells7.
Turner syndrome patients have a complete X chromosome karyotype, complete or partial deletion of
another chromosome, or other structural abnormalities of the X chromosome. The tissue-specific gene
expression analysis of the DEGs revealed that the system with the most highly enriched tissue-specific
Page 3/10gene expression was the hematologic/immune system, followed by the skin/skeletal muscle and
neurologic systems. However, Turner syndrome has rarely been reported to be associated with genetic
mutations in thyroid papillary carcinoma, so we hypothesized that the deletion of chromosomes in this
patient might be related to the BRAF gene mutation. Since M. Papanikolaou found Mosaic Turner
syndrome, papillary thyroid carcinoma, associate with BRAFV600E, which was similar to what we found 8.
In this case, a series of clinical abnormalities such as smallness, ovarian not development, diabetes,
hypertension, intellectual impairment, iaortic insufficiency, osteoporosis can be explained by Turner
syndrome. Skeletal system anomalies are extensive in TS patients as well9 .Turner syndrome patients
often show malformations in the chest shield, some patients have elbow flipping, the short fourth
metacarpal, finger toe bending, femoral and tibia exogenous warts and phalanx dysplasia, occasional
genu valgus and scoliosis10. The majority of patients with TS require examined for many aspects, such
as from structural bone defects for kyphosis, scoliosis, short neck and body proportion. Suna Kilinc11
found that the frequency of skeletal system anomalies was half of their study and scoliosis was the most
common pathology. However, turner syndrome combined hip dislocation is rare and less reported, Infants
with TS have an increased risk of con-genital hip dislocation12,but this situation should also be one of the
joint malformations. Syndromic dysplasia exists also in association with different pathologies such as
Down’s syndrome and neurogenic 13, renal or cardiovascular abnormalities14.When Daniela Duca15
discovered the Coxoauricular Syndrom in 1981,Incidentally, one of the women had Turner syndrome and
congenital dislocation of the hip. If laxity of the femoral head is present after birth, Neonatal Hip
Instability (NHI) can be diagnosed. This instability is usually present for the first few weeks of life,
Persistent joint instability can be caused by a disorder of reflex contraction in soft tissues, which, under
physiological circumstances, fixates the hip joint until six months of age. After the sixth month,
spontaneous resolution is very unlikely16.Patients have missed the best time for treatment when found
hip dislocation,which was not treated in a timely manner affecting the development of their hips resulting
in short stature. Therefore, young children born with combined hip dislocation need to identify Turner
syndrome at an early age.
It is necessary to be vigilant about osteoporosis and screening for thyroid tumors during the growth
process. These children should be given early and clear diagnosis and initial treatment, so as to avoid
misdiagnosis and mistreatment which lead to growth retardation and gonad dysplasia, diabetes,
osteoporosis, and thyroid tumors.
Declarations
[Availability of data and materials]
The datasets used and/or analysed during the current study are available from the corresponding author
on reasonable request.
[Conflict of interests]
Page 4/10The authors declare that there is no conflict of interest.
[Funding]This research did not receive any specific grant from any funding agency in the public,
commercial or not-for-profit sector.
[Author Contributions Statement]
The authors would like to thank the subjects for consenting to participate in this study. Huang wrote the
main manuscript text and prepared figure a-i. Wang performed the clinical examination of the patient,
Jiang developed the treatment plan. All authors reviewed manuscript.
[Human subjects]
This study was approved by the Local Ethics Committee of the Department of Scientific Research at The
Third Affiliated Hospital of Suzhou University. The Chinese patient signed informed consent documents
before entering the study
[Patient consent statement]
Written informed consent was obtained from the patient to publish this report in accordance with the
journal's patient consent policy.
References
1. Turner.H. Classic pages in obstetrics and gynecology by Henry H. Turner. A syndrome of infantilism,
congenital webbed neck, and cubitus valgus. Endocrinology, vol. 23, pp. 566-574, 1938. American
journal of obstetrics and gynecology 113, 279 (1972).
2. Stochholm, K., Juul, S., Juel, K., Naeraa, R. W. & Gravholt, C. H. Prevalence, incidence, diagnostic
delay, and mortality in Turner syndrome. J Clin Endocrinol Metab 91, 3897-3902,
doi:10.1210/jc.2006-0558 (2006).
3. Davenport, M. L. Approach to the patient with Turner syndrome. J Clin Endocrinol Metab 95, 1487-
1495, doi:10.1210/jc.2009-0926 (2010).
4. Godsland, I. F. Oestrogens and insulin secretion. Diabetologia 48, 2213-2220, doi:10.1007/s00125-
005-1930-0 (2005).
5. Mortensen, K. H. et al. Increased prevalence of autoimmunity in Turner syndrome--influence of age.
Clinical and experimental immunology 156, 205-210, doi:10.1111/j.1365-2249.2009.03895.x (2009).
6. Putti, T. C. & Bhuiya, T. A. Mixed columnar cell and tall cell variant of papillary carcinoma of thyroid: a
case report and review of the literature. Pathology 32, 286-289, doi:10.1080/pat.32.4.286.289 (2000).
7. Kim, M. J. et al. TERT Promoter and BRAF V600E Mutations in Papillary Thyroid Cancer: A Single-
Institution Experience in Korea. Cancers 14, doi:10.3390/cancers14194928 (2022).
Page 5/108. Papanikolaou, M., Chohan, T. & Millington, G. W. M. Malignant melanoma, papillary thyroid
carcinoma and Erdheim-Chester disease, associated with both BRAF(V600E) and mosaic Turner
syndrome. Clin Exp Dermatol 45, 512-514, doi:10.1111/ced.14153 (2020).
9. Ricotti, S. et al. Prevalence and incidence of scoliosis in Turner syndrome: a study in 49 girls
followed-up for 4 years. European journal of physical and rehabilitation medicine 47, 447-453 (2011).
10. Bondy, C. A. Heart disease in Turner syndrome. Minerva endocrinologica 32, 245-261 (2007).
11. Kilinc, S., Yildiz, M. & Guven, A. Associated clinical abnormalities among patients with Turner
syndrome. North Clin Istanb 7, 226-230, doi:10.14744/nci.2019.84758 (2020).
12. Bondy, C. A. Care of Girls and Women with Turner Syndrome: A Guideline of the Turner Syndrome
Study Group. The Journal of Clinical Endocrinology & Metabolism 92, 10-25, doi:10.1210/jc.2006-
1374 (2007).
13. Sankar, W. N. Complete redirectional acetabular osteotomies for neurogenic and syndromic hip
dysplasia. Journal of pediatric orthopedics 33 Suppl 1, S39-44,
doi:10.1097/BPO.0b013e3182770a71 (2013).
14. Harsanyi, S., Zamborsky, R., Krajciova, L., Kokavec, M. & Danisovic, L. Developmental Dysplasia of
the Hip: A Review of Etiopathogenesis, Risk Factors, and Genetic Aspects. Medicina (Kaunas) 56,
doi:10.3390/medicina56040153 (2020).
15. Duca, D. et al. A previously unreported, dominantly inherited syndrome of shortness of stature, ear
malformations, and hip dislocation: the coxoauricular syndrome--autosomal or X-linked male-lethal.
Am J Med Genet 8, 173-180, doi:10.1002/ajmg.1320080208 (1981).
16. Kotlarsky, P., Haber, R., Bialik, V. & Eidelman, M. Developmental dysplasia of the hip: What has
changed in the last 20 years? World journal of orthopedics 6, 886-901, doi:10.5312/wjo.v6.i11.886
(2015).
Tables
Table 1:DXA Results Summary
Region Area(cm2) BMC(g) BMD(g/cm2) T-score Z-score
L1(2020-10) 11.1 8.05 0.720 -2.5 -2.3
(2021-06) 10.77 8.30 0.771 -2.0 -1.8
L2(2020-10) 11.11 7.78 0.700 -3.0 -2.8
(2021-06) 11.07 7.75 0.700 -3.0 -2.8
L3(2020-10) 12.57 9.37 0.745 -3.1 -2.9
(2021-06) 12.39 9.27 0.748 -3.1 -2.9
L4(2020-10) 10.99 7.78 0.708 -3.2 -3.0
(2021-06) 11.62 8.12 0.699 -3.3 -3.1
Total(2020-10) 45.84 32.98 0.719 -3.0 -2.8
(2021-06) 45.85 33.45 0.730 -2.9 -2.7
Page 6/10Region Area(cm2) BMC(g) BMD(g/cm2) T-score Z-score
Neck(2020-10) 5.34 2.49 0.466 -3.4 -3.2
(2021-06) 6.85 4.02 0.586 -2.4 -2.1
Troch(2020-10) 3.50 2.50 0.715 0.1 0.2
(2021-06) 38.58 20.22 0.524 -1.8 -1.7
Inter(2020-10) 21.07 13.69 0.650 -2.9 -2.8
(2021-06) 7.97 7.41 0.929 -1.1 -1.0
Wards(2020-10) 0.93 0.26 0.273 -3.9 -3.4
(2021-06) 1.18 0.79 0.667 -0.6 0.0
Table 2:Follow-up of sex hormone levels
Items(Sex homone) Date Date Date Reference value
(2020-10) (2021-06) (2022-08)
SDBG(nmol/l) 47.7 149.6 233.3 18.2-135.5
E2(pg/ml) <15 63 63.67 15-127
Prog(ng/ml) 0.26 0.26 0.62 0.31-1.52
Testo(ng/ml) 0.41 0.33 0.43 0.1-0.75
LH(mIU/ml) 16.87 2.62 2.31 2.12-10.89
FSH(mIU/ML) 85.98 10.2 11.18 3.85-8.78
Figures
Page 7/10Figure 1
Mild elbow valgus(a),epicanthus(b),pygmyism(c),The epiphysis is closed(d)
the chromosomekaryotype46,X,i(X)(q10)[45]/45,X[15](e).
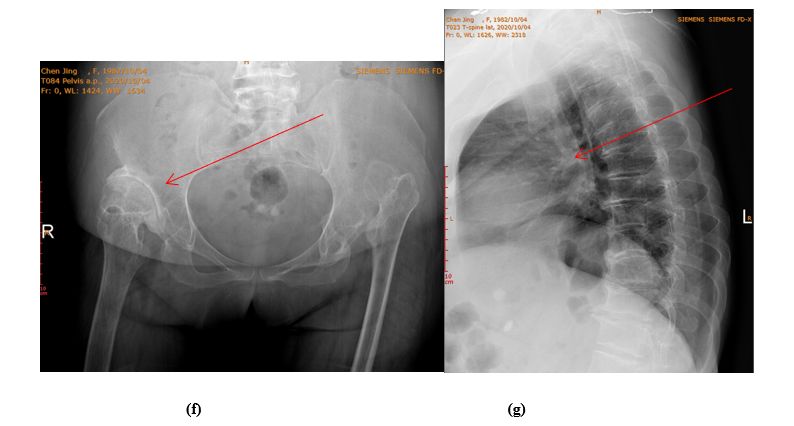
Page 8/10Figure 2
Double dislocation of hip joint, short neck of femur.(f)
Thoracolumbar anterior and lateral position: multiple wedge changes(g)
Page 9/10Figure 3
Left thyroid nodule(h)
(Left) papillary thyroid carcinoma, 1.3*1.2cm in size, with metastasis in the left central lymph node (1/7)
(i)
Page 10/10You can also read