A NOTE FROM MATT KELLY - Gosford Private Maternity Services
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CENTRAL COAST NEWS
DECEMBER 2019
A NOTE FROM MATT KELLY
REGIONAL MANAGER AND GOSFORD PRIVATE HOSPITAL CEO
Since our last newsletter in July there a publication read across 80 countries
have been a lot of great achievements with regards to our engagement with
made at Gosford Private Hospital. The staff and patients, as well as winning
first sod was turned on our $32million several awards this year with the NSW
expansion which will see three more Business Chamber at a local, regional
theatre spaces, a new recovery and and State level. The staff also are
day surgery, a new purpose-built dedicating their own time to their
maternity ward, expanded surgical love of sustainable practices, and we
beds and capacity for more beds have had contact now from around
into the future. It will mean that our the country and the globe about
site will be a construction zone all how we are working to achieve our
of next year, but services will not be sustainability goals. information that we send out with
interrupted at all. We are spending patients, and to you as their GP. We
a lot of time focusing on way finding We also continue to invest in the will hopefully be enhancing that
so that patients’ and relatives’ latest technology and provide our discharge information very soon.
experiences here are not hampered. medical staff with everything they
need to care for your patients. I look forward to keeping you
Our staff continue to focus on the This year alone we have spent over updated with the building and
patient’s experience and we are being $2 million on our facility and exciting new services, such as robotic
recognised for the fantastic work that equipment. We are also working at surgery that we will be able to offer
they do. We have been referenced in a national level on improving the with our new facility.
A NOTE FROM KATHY BEVERLEY
BRISBANE WATERS PRIVATE CEO
It’s been a busy time at Brisbane has been pleasing for many GPs
Waters Private Hospital since the being able to refer locally. With more
last GP rounds was delivered to your surgeons attending the Hospital in
practices – with many of you attending plastics, dental, gastroenterology,
our 3rd Mental Health Conference in general and bariatric surgery we have
October at the Crown Plaza Terrigal. seen an increase of 25% in surgical
With such great support from the GP services which has impacted positively
community, our Central Coast Clinic on other aspects of the Hospital. If I would like to thank you all for your
continues to be extremely busy and you are a GP or Referrer from the support of Brisbane Waters Private
now with the recruitment of a new southern end of the coast and wish to during 2019 and look forward to
Nurse Unit Manager with specialist schedule a visit to your practice from working with you in 2020.
qualifications as a Nurse Practitioner one of our Specialists, or join one of
and ten Psychiatrists in private our upcoming Educational events, Finally I would like to wish everyone a
practice, the unit is ready to continue please contact our Regional GP and very Merry Xmas and prosperous New
its phenomenal growth in 2020. Community Relationship Manager, Year and to thank our exceptional staff
Petrina Waddell, at petrina.waddell@ who continue to work extremely hard
Our surgical services have continued healthecare.com.au to provide a great patient experience
to grow over 2019, which I know at Brisbane Waters Private.
GP ROUNDS CENTRAL COAST NEWS 1
IN THIS EDITION A NOTE FROM GLEN AULD
TUGGERAH LAKES PRIVATE CEO
3 HIATAL HERNIAS – WHO Tuggerah Lakes Private Hospital has got off to a flying start and over
the last 6 months has gone from strength to strength. The hard work
BENEFITS FROM REPAIR
in the planning and establishment phase is now paying dividends as
with General Surgeon, we are seeing more surgical cases with increasing acuity and more
Dr Peter Hamer overnight cases. The three theatres are now fully allocated and the
team is working on plans to increase both the theatre and ward
capacity along with new services that are needed in the local area.
4 UPDATE ON BREAST Dr Jim Hasn and Dr Indu Gunawardena provided the first Tuggerah
CANCER TREATMENT Lakes GP education evening and we are looking forward to many
with Breast and General more educational events in 2020.
Surgeon, Dr Mary Ling
If you are a GP or Referrer from the northern end of the Central Coast
or Lake Macquarie area and would like to tour the hospital, schedule
6 ROBOTIC ANTERIOR a visit to your practice from one of our Specialists, or join one of our
TOTAL HIP upcoming Educational events, please contact our Regional GP and
Community Relationship Manager, Petrina Waddell, at
REPLACEMENT petrina.waddell@healthecare.com.au
with Orthopaedic Surgeon,
Dr John Limbers I would like to take this
opportunity to thank the
amazing staff at Tuggerah
8 COMMON (AND LESS Lakes Private Hospital for
COMMON) their dedication and patient
NERVE ENTRAPMENT centred care, the exceptional
specialists who are bringing
SYNDROMES desperately needed services
with Neurosurgeon, to the local area, and our
Dr Vanessa Sammons local GP’s for their fantastic
support. We are looking
forward to continuing to
10 BREAST IMPLANT grow and adding more
RUPTURE, ALCL AND services in 2020.
CAPSULAR
I wish you all a safe and
CONTRACTURE
festive Christmas and
with Plastics and New Year.
Reconstructive Surgeon,
Dr Chaithan Reddy
12 DIAGNOSIS AND Petrina Waddell
REFERRAL FOR TWIN Petrina Waddell is Health Care’s Regional
GP & Community Relationships Manager
PREGNANCIES
for the Central Coast. Petrina helps to
with Obstetrician/ raise the profile of the Specialists and
Gynaecologist, admitting VMO’s across our three private
Dr Amrou Metawa hospitals and is available to support local
GPs, Referrers and the business community
in learning more about the services we
14 MANAGEMENT OF LATE offer, any new procedures, and to facilitate
LIFE DEPRESSION meet and greet opportunities with our
new and experienced Specialists. Petrina
with Psychiatrist, also coordinates our RACGP accredited
Dr Susil Stephen education events. For more information,
contact Petrina on 0459 988 236 or at
petrina.waddell@healthecare.com.au
2 GP ROUNDS
HIATAL HERNIAS – WHO BENEFITS FROM REPAIR
– with General Surgeon, Dr Peter Hamer
Hiatal hernias are common and often 2) Regurgitation and early satiety gastroscopy. Patients with problematic
reported on CT scans, gastroscopy Similar to volume reflux, a hernia that iron deficiency, known large hiatal
and contrast swallows. The majority is large enough can cause mechanical hernias and no other cause for their
are relatively asymptomatic or problems such as regurgitation of food deficiency will often benefit from repair
associated with mild reflux symptoms and early satiety. If this is happening on regardless of whether ulcers are seen at
and should be managed expectantly, a regular basis, repair is the only way of gastroscopy or not.
however there are particular groups fixing this.
of patients with moderate to large 5) Volvulus and pain
hiatal hernias who are better off with a 3) Shortness of breath These patients are relatively easy to
surgical repair, often obtain substantial manage. When a hernia is large enough
improvements in their quality of life, It was long debated whether or not a
hiatus hernia can get large enough to to start volving and causing ischaemic
and are very grateful post operatively. pain symptoms they need early referral
The indications are broader than merely pressure the lungs and cause shortness
of breath. We now know this is both for repair.
reflux disease.
incorrect and correct. A large hiatal
hernia can cause quite significant 6) 40-50 year old males
1) Volume reflux
shortness of breath on exercise, but This group warrants a mention on their
When taking a history of reflux disease, it is due to left atrial compression own. Although most large hiatal hernias
it is important to delineate what the and a decrease in venous return to start causing problems in 60-70yo
patient means by reflux. Patients can the heart (the left atrium sits right up females, there is a younger group of
mean anything from mild retrosternal against a hiatal hernia), rather than male patient who develop large hiatal
discomfort, burping (unlikely to be lung compression. After repair it is not hernias in their 40s and 50s. They are
reflux), through to what can be termed uncommon for patients in their 60s poor at describing their symptoms,
volume or mechanical reflux. It is this and 70s to describe an increase in the and incorrectly attribute a lot of their
latter group that need a mechanical distance they can walk from 2-300m symptoms to middle age rather than
(surgical) solution to a mechanical to 2-3km. Exclusion of cardiac and their hernia. However they almost
problem (their hiatus hernia). Volume respiratory causes is obviously the invariably have moderate to severe
reflux is a term used to describe the first step if you suspect this, it occurs symptoms, which they only recognise
feeling of large volumes of gastric fluid only in hernias large enough to cause fully in hindsight. They are invariably
refluxing into the oesophagus. Patients atrial compression and sometimes the very grateful post surgery and describe
will describe a feeling of fluid rushing patient will notice that their shortness marked improvements in their exercise
up when they bend over to do up of breath is worse after a meal (when tolerance, energy levels, eating patterns
shoelaces or when doing the gardening. food distends the stomach which then and reflux.
On questioning they won’t be able to
pushes on the atrium).
sleep flat, often using pillows or raising
Surgery
the head of the bed to use gravity to
prevent the fluid rush. A PPI will make
4) Iron deficiency anaemia Surgery for hiatal hernia repair is
gastric fluid neutral but it won’t take it Having a hiatus hernia means your laparoscopic and involves a 1-2 night
away, meaning that these patients are stomach is straddling the hiatus and stay in hospital followed by a 4-6 week
often PPI resistant – when on anti- the diaphragmatic crura. This puts pureed diet. It is often tolerated well
reflux medications they still feel gross tension on the stomach mucosa and even by those in their 80s and 90s.
amounts of fluid refluxing into their can cause ischaemic ulceration of the Side effects involve gas-bloat syndrome
oesophagus, it just happens to be pH stomach mucosa known as Camerons in 20-30% so if patients have reflux
neutral fluid rather than acidic. ulcers. These ulcers are intermittent controlled by medications, and none
in nature, coming and going and are of the above symptoms they are often
therefore only sometimes seen on best managed without surgical referral.
Dr Peter Hamer is a General Surgeon with a special interest in conditions
of the oesophagus and stomach, including:
–– Oesophageal and gastric cancer –– Endoscopy and Colonoscopy
–– Hiatus hernias and reflux –– Gall bladder surgery
–– Weight loss surgery –– Hernia repair
Consulting at:
• 33 Etna Street, Gosford Call us: 02 4380 8404
• Kanwal Medical Complex, Ste C 16/654 Pacific Hwy www.drpeterhamer.com.au
CENTRAL COAST NEWS 3
UPDATE ON BREAST CANCER TREATMENT
– with Breast and General Surgeon, Dr Mary Ling
Neoadjuvant chemotherapy and improving aesthetic outcomes for –– Triple negative breast cancer
The treatment sequence for breast patients already suitable for breast < 50 years
cancer is traditionally surgery conserving surgery, as well as time for
–– Male breast cancer at any age
followed by chemotherapy and genetic testing and surgical planning.
–– Jewish ancestry
then radiotherapy. Neoadjuvant
chemotherapy (NACT; chemotherapy –– Two breast cancers, where the
before surgery) was reserved for cases first occurred < 60 years
of locally advanced, inoperable or
Around
–– Two or more different but
inflammatory breast cancer. Nowadays, 1 in 20 women associated cancers at any age
NACT is increasingly being used for with breast cancer (e.g. breast and ovarian cancer)
early breast cancer, specifically triple
negative (oestrogen, progesterone and 1 in 7 women with –– Lobular breast cancer and family
and HER2-receptor negative) and ovarian cancer have an history of lobular breast or
HER2-positive tumours. Studies have diffuse-type gastric cancer
shown overall survival rates are similar inherited genetic
–– Personal history suggestive of
for adjuvant versus NACT, however, mutation.
a major advantage of NACT is that it –– Peutz-Jegher syndrome
has prognostic significance. If NACT is (oral pigmentation and/or
given and no residual cancer is found gastrointestinal polyposis)
in the surgical specimen, the patient is Gene testing –– PTEN hamartoma syndrome
said to have a ‘pathological complete (macrocephaly, specific
Around 1 in 20 women with breast
response (pCR)’ and survival is mucocutaneous lesions,
cancer (and 1 in 7 women with ovarian
significantly improved when compared endometrial or thyroid cancer)
cancer) have an inherited genetic
with a patient who does not achieve
mutation. Patients with a personal
a pCR. If pCR is not achieved, there –– Li Fraumeni syndrome
history of breast cancer that warrant
is an opportunity to give further (breast cancer < 50 years,
a referral to a family cancer clinic for
chemotherapy after surgery. Other adrenocorticocarcinoma,
assessment include:
benefits of NACT are tumour shrinkage sarcoma, brain tumours).
reducing the need for mastectomy –– Breast cancer < 40 years or < 50
and axillary lymph node dissection, years with limited family structure
or knowledge (e.g. adopted)
continued..
Dr Mary Ling provides private - Gastric Band Removals
practice specialisation in: - Gastroscopy & Colonoscopy
- Breast Cancer Surgery
Rapid Access Appointments within 48
- Gallbladder & Hernia Surgery hours are available for patients with a
- Melanoma & Skin Cancer Surgery new diagnosis of breast cancer.
Consulting at: Call us: 02 4321 0302
• Suite 6/16 Hills Street, Gosford
Email: reception@drmaryling.com.au
• Brisbane Waters Private Consulting Rooms
• Tuggerah Lakes Private Consulting Rooms Sign up to GP Update a quarterly
newsletter for Central Coast GPs at
drmaryling.com.au/doctors/gp-update
4 GP ROUNDS
Breast cancer-related lymphoedema Australasian Lymphology Association
Breast cancer-related lymphoedema (ALA) position statement recommends A simple approach to
(BCRL) affects 1 in 5 patients treated all breast cancer patients have pre- “prescribing exercise”:
for breast cancer, and has a significant treatment measurements (prior to
–– Assess current physical
negative impact on patient’s quality surgery or chemotherapy) and repeat
activity at regular intervals
of life after treatment. Established measurements at 3 to 6 monthly
risk factors include axillary surgery intervals for the first 2 years post –– Advise on recommended
(with incidence 4 times higher in treatment. activity levels & convey
patients who have had axillary lymph message that moving matters
node dissection (20%) compared with Exercise
sentinel lymph node biopsy (5%)), –– Refer to appropriate
The Clinical Oncology Society of health care professional
regional lymph node radiation and Australia (COSA) position statement
elevated BMI. (exercise physiologist
on Exercise in Cancer Care or physiotherapist with
recommends all cancer patients aim experience in cancer care) or
Previously, BCRL is diagnosed at the
for 150 minutes of moderate-intensity exercise programs (specific
symptomatic stage when there is
or 75 minutes of vigorous-intensity programs for breast cancer
visible limb swelling. Nowadays, there
aerobic exercise (e.g. walking, jogging, patients include YWCA
is evidence that if BCRL is diagnosed at
cycling, swimming) each week and 2 Encore, Strength After Breast
an early stage, it can be reversible, thus
to 3 resistance exercise sessions (e.g. Cancer & Next Steps).
reducing the need for more complex
weight lifting) each week involving
and costly interventions. Prospective
moderate- to vigorous-intensity
surveillance using bioimpedance
exercises targeting the major muscle
spectroscopy (BIS), which measures Reference: eviq.org.au/cancer-genetics/adult/referral-
groups. Research has shown the
extracellular fluid build up in the guidelines/1620-referral-guidelines-for-breast-cancer-
benefit of exercise on cancer-related risk-as
at risk limb, is capable of detecting
health outcomes, specifically quality
subclinical lymphoedema (prior to Reference: Schmitz K, Campbell A, Stuiver M et al.
of life, anxiety, depression, fatigue,
onset of symptoms and signs). Early Exercise is medicine in oncology: engaging clinicians to
sleep and bone health. There is help patients move through cancer. CA Cancer J Cain
intervention, with physical therapy
also evidence to suggest exercise is 2019; 699: 468-484.
and compression garments, at the
associated with improved cancer-
subclinical stage is effective in reducing
specific survival in breast, colon and
progression to clinical BCRL.
prostate cancer.
NEW – CANCER REHABILITATION PROGRAM
Fight Back, Live Well
Introducing Gosford Private Your patients will be encouraged
Hospital’s all new Cancer to set and achieve their own,
Rehabilitation program – individual goals improving strength
Fight Back, Live Well! and endurance, immune function,
Ideal for before, during and after body composition, self-esteem
cancer treatment, the tailored and overall quality of life.
programs are based on the latest
research, and delivered by an Learn more by calling 4323 8101
experienced multi-disciplinary team. or at gosfordprivate.com.au
CENTRAL COAST NEWS 5
ROBOTIC ANTERIOR TOTAL HIP REPLACEMENT
– with Orthopaedic Surgeon, Dr John Limbers
hospital stays. This is due to the
approach sparing all muscle envelopes,
utilising an internervous plane. There
has been no long term functional
or implant survivorship benefit
demonstrated with this. However,
MRI studies have demonstrated less
residual muscle damage and atrophy
after the anterior approach.
When the direct anterior approach
is combined with MAKO® robotic
technology, a pre-operative CT scan
is performed. This is segmented and
loaded onto the MAKO® system
software, to provide a patient specific
3-D CT model of the total hip
replacement (Figure 1). This virtual total
hip replacement is then reviewed by
MAKO® robot the surgeon and modified as necessary Figure 2
before the initial skin incision.
Total hip replacement has been real time adjustments. The robotic
a highly successful procedure for The surgeon then performs the technology ensures that the acetabular
over 50 years, with numerous new anterior approach to the hip joint. component is inserted with the same
approaches and techniques developed Navigation pins are inserted into anteversion and inclination angles as
over that time. Over the last 10 years the pelvic bone. This is followed the pre-operative plan. The femur is
the direct anterior approach has by mapping the anatomy of the hip then broached and the hip reduced
become popular with many surgeons joint utilising a specialised probe. with a trial femoral stem and head
throughout the world. In the last few This information is detected by a in place. Further measurements are
years this has been combined with specialised camera and passed to the then taken with the specialised probe
MAKO® assisted robotic technology, MAKO® robotic unit. This allows the to check the leg length and offset. If
with the aim of using robotic patient’s hip joint to be matched to the these are correct then the definitive
technology to increase accuracy. individualised plan. The surgeon then femoral stem and head are inserted.
reams the acetabulum (Figures 2 & 3) This technique provides highly
A number of studies have documented and inserts the acetabular component accurate placement of the components
potential benefits of anterior hip under robotic control. The tactile, of the total hip replacement, in terms
replacement in the first 6 weeks auditory and visual feedback of the of acetabular component inclination
following surgery. These include less robotic arm limits the bone preparation and version as well as leg length and
pain in the post-operative period, to the diseased areas and allows hip offset. These are parameters
quicker return to function and shorter
continued..
Figure 1 Figure 3
6 GP ROUNDS
that are critical to having a high
long term hip implant survivorship
rate and a very low dislocation rate.
This potentially results in a lower
500
incidence of leg length inequality and
a reduced chance of post-operative
hip dislocation. It has the potential
to improve long term results of total
th
hip replacement surgery, by ensuring
optimal implant position.
MAKO®
Is Robotic Anterior Total Hip
Replacement of benefit to ROBOT JOINT
patients?
Direct anterior approach total hip
REPLACEMENT
replacement has been shown to have
functional benefits in the first 6 weeks. SURGERY
One issue raised with direct anterior
hip replacement is the learning curve, Gosford Private Hospital recently
with the potential for complications if undertook its 500th MAKO®
the surgery is not performed properly. Robot joint replacement surgery,
However, increasing numbers of positioning the Hospital as the
surgeons experienced in the technique second highest user of the cutting-
are training registrars and surgeons edge technology in NSW.
learning the technique. There are also The $1.7 million MAKO®
many training workshops and courses was first used at Gosford Private at the end of 2017, providing a highly
available. This has allowed adoption accurate, customised solution that allows the surgeon to align and position
of the technique by many surgeons, replacement joints at an angle that optimises outcomes and matches the
with excellent results. With regard unique anatomy of each patient.
to the robotic assisted technique,
the acetabular cup placement was Orthopaedic Surgeons Dr John Limbers, Dr Sarah Hanslow, Dr John Morton
examined in robotically assisted and and Dr Jim Hasn are currently credentialed to use the Robot at Gosford
conventional total hip replacement Private for knee and hip replacements. Learn more about the Orthopaedic
surgery in a comparative study. A Surgeons and the MAKO® at gosfordprivate.com.au/about-us/news
statistically significantly higher number
(30% higher) of acetabular cups were
positioned within the desired range
of anteversion and inclination in the
robotically assisted cases. Whether
this translates into lower revision rates
and increased patient satisfaction
remains to proven.
Dr John Limbers is an Orthopaedic Surgeon who specialises in hip and knee
replacement surgery as well as reconstructive foot and ankle surgery. He has
particular expertise in MAKO® robotic anterior total hip replacement surgery and
MAKO® robotic knee replacement surgery. He was the first surgeon in NSW to
perform robotic total knee replacement after its worldwide launch in September
2017. He has performed over 500 robotically assisted joint replacements.
Consulting at: Call us: 02 4393 3820
Central Coast Orthopaedics, Email: admin@cco.com.au
Tuggerah Lakes Private Consulting Rooms www.drjohnlimbers.com.au
CENTRAL COAST NEWS 7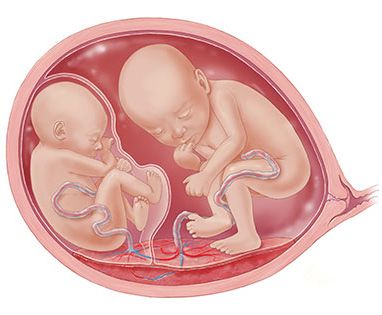
COMMON (AND LESS COMMON)
NERVE ENTRAPMENT SYNDROMES
– with Neurosurgeon, Dr Vanessa Sammons
Ulnar Neuropathy To optimise outcome, I prefer to see It can be confused with a cervical
(Cubital Tunnel Syndrome) these patients sooner rather than radiculopathy (particularly C6). Again,
later, before muscle wasting occurs. a careful history and examination
Ulnar neuropathy is most commonly
can distinguish the two and nerve
caused by compression at the elbow Median Neuropathy conduction studies can help.
(cubital tunnel) and less commonly at
Guyon’s canal at the wrist.
(Carpal Tunnel Syndrome)
Median Neuropathy is most commonly Meralgia Paresthetica
Clinically, patients describe numbness caused by compression at the hand Meralgia Parasthetica is caused by
and paraesthesia to the fourth and (carpal tunnel) and less commonly at compression of the lateral femoral
fifth digits and the ulnar aspect of the other sites in the forearm and arm cutaneous nerve usually at the
hand. The patient will often feel that (with slightly different presentations). inguinal ligament.
the hand is weak and less dextrous
because of loss of innervation to the Clinically, patients describe numbness This has a classic clinical picture: the
hand intrinsic muscles. and paraesthesia to the thumb and patient describes pain, numbness and
next two to three digits. The palm /or paraesthesia to the anterolateral
A basic examination is to check the of the hand should be spared in aspect of the thigh. The sensory
pattern of sensory change (splitting carpal tunnel syndrome. The patient change does not extend below the
of the fourth digit is a big clue), and will often feel that the hand is less knee, is sharply demarcated and
checking abduction of the fingers dextrous because of loss of adequate doesn’t migrate.
(particularly the fifth digit) and flexion sensation. There may be thenar
of the distal joints of the fourth and Nerve conduction studies can
muscle (and so thumb) weakness. A
fifth digit. Wasting of the intrinsic be done and can help. Steroid
feature is forearm, wrist and hand pain
muscles is a sign of severity (look for injections also have a role and can
which is often worse at night.
wasting in the first webspace, dorsally). be diagnostic as well as therapeutic.
A basic examination is to check the Surgical decompression is an option
It can be confused with a cervical pattern of sensory change (splitting for some patients and is a very
radiculopathy. A careful history and of the fourth digit is a big clue), and effective treatment even after years
examination can distinguish the two checking thumb abduction (the thumb of compression.
and nerve conduction studies can help. moves perpendicular to (or away from)
the palm).
continued..
Dr Vanessa Sammons is a Neurosurgeon who treats all neurosurgical
conditions, but with a particular interest in Peripheral Nerve Surgery. She
completed fellowship training in Peripheral Nerve Surgery under the mentorship of
Dr Rajiv Midha, a world renowned Peripheral Nerve Surgeon in Calgary, Canada.
Vanessa prides herself on providing personalised and thoughtful patient care and
utilising her skills to achieve the best outcome possible.
Vanessa consults weekly • Central Coast Neurosciences
in Erina and Woy Woy Level 1/200 Central Coast Hwy, Erina NSW 2250
and operates regularly at • 19 Kingsley Avenue, Woy Woy NSW 2256
both Gosford Private and
Brisbane Waters Private Call us: 02 9436 1818
Hospitals. Email: info@snns.com.au
www.snns.com.au
8 GP ROUNDS
Common Peroneal Neuropathy
Common Peroneal Neuropathy is
caused by compression at the lateral
Revolutionary
knee (neck of the fibula). It is an
Nerve compression technique
underdiagnosed nerve compression
and can be confused with an L5 can be easily overlooked reducing back pain
radiculopathy or knee pathology. as a pain syndrome or Gosford Private Hospital
Clinically, patients describe numbness misdiagnosed as a spine Neurosurgeon, Dr Marc Coughlan,
and paraesthesia to the dorsum of the or other joint problem. has led the way for Neurosurgery
foot and the lateral aspect of the leg in Australia, introducing minimally
(upper two thirds). The patient may invasive endoscopic radio
have weakness of dorsiflexion and of frequency denervation for the
foot eversion (in an L5 radiculopathy treatment of back pain in patients
usually inversion is weak and eversion on the Central Coast.
is spared).
General thoughts Under the revolutionary technique,
A basic examination is to check Nerve compression can be easily radio waves are channeled through
the pattern of sensory change and overlooked as a pain syndrome or a needle inside a long, thin,
movements of the foot (look for misdiagnosed as a spine or other joint flexible tube less than the width
dorsiflexion and eversion weakness). problem. As a Neurosurgeon, I treat of a pencil. The needle is guided
I also look for wasting and fibrillations conditions in all regions, so naturally directly into the affected facet
in tibialis anterior and peroneus look critically at where in the nervous joints of the spine and the radio
longus. The key to this diagnosis is system the pathology may lie. With waves produce small, targeted
keeping it in mind. peripheral nerve problems, the key to areas of heat which desensitise the
the diagnosis is keeping the possibility affected joints, thus alleviating the
A careful history and examination can
in the back of your mind, even if patient’s pain.
distinguish this from spinal and knee
more common causes exist (such as
pathology and, again, nerve conduction
radiculopathy, for example). Unlike traditional radio frequency
studies can help. This is a condition I
techniques, the revolutionary
prefer to evaluate sooner rather than Nerve compressions are best
later since decompression loses its endoscopic approach
evaluated early since the success of
efficacy when done late in the process. includes a video camera, allowing
surgery can be dependent on timing,
the surgeon greater vision and
which differs according on the nature
Tarsal Tunnel Syndrome control, ensuring effective
and location of the problem.
Tarsal tunnel syndrome is caused by treatment, whilst also allowing the
compression of the tibial nerve at the patient to be sedated throughout
tarsal tunnel (medial ankle). The nerve the procedure.
courses under a ligament similar to Learn more at gosfordprivate.com.
that in carpal tunnel syndrome and au/about-us/news
can be compressed.
Clinically, patients describe numbness,
burning pain and paraesthesia to the
plantar aspect of the foot radiating to
the first four toes. Foot cramping can
occur. I look for a Tinel sign between
the medial malleolus and the heel
which is sometimes present. Nerve
conduction studies can help with
establishing the diagnosis.
Tarsal tunnel syndrome can be
confused with plantar fasciitis.
Surgical decompression is effective.
CENTRAL COAST NEWS 9
BREAST IMPLANT RUPTURE, ALCL AND
CAPSULAR CONTRACTURE
– with Plastics and Reconstructive Surgeon, Dr Chaithan Reddy
Breast augmentation remains one of Breast Implant rupture Following breast augmentation, the
the most popular aesthetic procedures Most breast implant ruptures remain body’s response is to form a fibrous
in our country. silent without signs or symptoms. Many capsule around it.
of these cases are detected incidentally –– In the case of intracapsular
at the time of breast imaging or breast rupture, free silicone remains
screening. Symptomatic ruptures may within the capsule layer, and the
While present with pain, hardening, or change decision to proceed with surgery
in breast shape. would be based on symptoms,
generally considered complicating features (e.g. capsular
a safe procedure, The risk and rates of breast implant contracture), and anaesthetic risk.
rupture varies depending upon the
both short term risks age of the implants and the quality of –– In the case of symptomatic
and longer-term the implants used. Rupture rates have extracapsular rupture, silicone
been reported in multiple studies and has leaked out of the capsule
complications vary between 1.1-17% over a 6-10 and into the breast parenchyma,
may arise year period. The rates have generally and surgery is generally indicated
decreased with the advent of newer entailing implant removal and
generation implants which exhibit a capsulectomy.
thicker outer silicone core and a more
There has been increasing media cohesive gel. Capsular Contracture
attention pertaining to the safety of
Implant rupture may be detected by US, Capsular contracture remains
breast implants over the last 12 months,
Mammogram, CT or MRI. MRI is generally one of the most common implant
particularly as more demographic data
considered the preferred method of related complications and refers to
and knowledge is gained about the
evaluation with a high sensitivity and contracture and hardening of the
association between Breast implants and
specificity. US is a good cost-effective breast Implant capsule.
Anaplastic Large Cell Lymphoma.
alternative but operator dependent.
continued..
Dr Chaithan Reddy is a Specialist Plastic, Reconstructive & Cosmetic
Surgeon. He has been consulting and operating on the central coast since 2012.
After receiving his Fellowship, he undertook further training in Microsurgery and
advanced Head & Neck cancer reconstruction and remains an active member of the
Crown Princess Mary MDT Cancer Clinic.
His reconstructive surgery interests include: His cosmetic surgery interests include:
––Skin Cancer surgery ––Breast reduction and breast implant
removal surgery
––Advanced Head & Neck Cancer
reconstruction ––Post weight loss body contouring
––Hand surgery (carpal tunnel syndrome, ––Rhinoseptoplasty
Dupuytrens Disease)
The Plastic Surgery Clinic Call us: 1300 073 339 Fax: 02 8076 3237
Suite 4, 12 Jarrett Street, Email: info@theplasticsurgeryclinic.com.au
North Gosford
www.theplasticsurgeryclinic.com.au
10 GP ROUNDSIt is essentially an excessive fibrotic BIA-ALCL may present as a mass
reaction to a foreign body (implant).
The Baker Scale (1-4) is a common
lesion, capsular contracture,
lymphadenopathy, or effusion World First for
method of classifying the severity
of capsular contracture. In mild
associated with the capsule.
More commonly it manifests as
ENT Patients
forms (grade 2), the breast may
a delayed onset seroma, typically Ear, Nose and Throat specialist, Dr
feel slightly firmer but normal
7-10 years following implant Indu Gunawardena, has become
appearance. In later stages (grade
insertion. the first surgeon in the world to use
4), the breast(s) may feel hard,
the revolutionary Smith & Nephew
tender and appear distorted. Rates
Any suspicion should prompt Werewolf Coblator to treat patients at
of capsular contracture vary from 2%
imaging and US guided FNA of Gosford Private Hospital.
to 20% in various studies, depending
a seroma (or mass) with specific
on the type of implant used and The new technology is set to deliver
pathological testing.
the site of implant placement. The quicker procedure times, higher
incidence of capsular contracture is Once detected, treatment typically accuracy and minimal bleeding
generally lower when implants have a entails removal of the implants, for patients, leading to reduced
textured surface and or are placed in capsulectomies and adjuvant complications post-operatively and
a subpectoral position. therapy when indicated. a quicker recovery. The product’s
ergonomic design also ensures a
Treatment of capsular contracture Medicare, Health Fund and positive experience for the surgeon.
is often dictated by symptoms and
Manufacturer Coverage for
severity. “I am delighted to have the
revision surgery
opportunity to be the first surgeon in
Typically, definitive management of With improvements in implant
the world to use this industry-leading
grade 3 and 4 capsular contracture technology and safety, leading
technology. With the introduction of
involves surgery, entailing implant breast implant manufacturers
the Werewolf we expect to deliver
removal and total capsulectomies. provide warranty policies for their
better outcomes for our patients with
breast prostheses. For complications
Breast Implant associated less concerns in the recovery period,”
such as breast implant rupture, or
said Dr Gunawardena.
ALCL capsular contracture, manufacturers
BIA-ALCL is a rare form of non- may offer complete replacement Learn more at
Hodgkin’s lymphoma and has been cost of the prostheses and a gosfordprivate.com.au/about-us/news
found in a small cohort of women contributing amount towards
with breast implants. The aetiology corrective surgery.
remains uncertain, but It is thought
to develop as a result of bacterial Medicare item numbers and rebates
contamination (‘Biofilm’) leading exist for breast implant removal
to a protracted inflammatory and capsulectomies, enabling
response. The incidence is rare with health funds to potentially provide
approximately 500 cases worldwide rebates (surgery and anaesthesia)
on a background of at least 60 and cover associated hospital costs.
million textured implant insertions. Medicare item numbers (and health
Australia, however accounts for fund coverage) can also apply for
1 in 7 of all global cases. Risk does implant replacement to correct
increase with the degree of implant breast implant related ruptures and
surface texturing and ranges from 1 capsular contracture.
in 4000 (macrotextured implants) to
1 in 60,000 (microtextured implants).
Certain macrotextured implants were
removed from the Australian market
this year but given the extremely low
risk, the current consensus is that
asymptomatic disease-free women
who already textured implants in situ
do not require implant removal.
CENTRAL COAST NEWS 11DIAGNOSIS AND REFERRAL FOR TWIN PREGNANCIES
- with Obstetrician and Gynaecologist, Dr Amrou Metawa
Twin pregnancies bring a great deal of
excitement for parents with General
Practitioners playing an integral role
with early diagnosis through the use
of dating ultrasound scans. Early
screening leads to timely referrals
to specialist Obstetricians which
promotes improved pregnancy care,
fetal surveillance and intrapartum
care, and is particularly important in
the management of twin pregnancies
because of the higher frequency of
complications. Monochorionic Diamniotic (MCDA) twins Dichorionic diamniotic (DCDA) twins
An increased likelihood of twin
pregnancy may be suspected based (TTTS) and twin anaemia-polycythemia Multiple pregnancy results in greater
on the use of assisted reproductive sequence. Both complications increase maternal hemodynamic changes
technology to conceive, large for the risk for neurologic morbidity and including a 20 percent higher
date uterine size, family history or perinatal mortanilty in monochorionic cardiac output and 10 to 20 percent
hyperemesis gravidarum. Other twins. Cord entanglement and greater increase in plasma volume.
influences of dizygotic twins include conjoined twin risks are increased with This may result in increased risk of
maternal age, race/geographic area, monoamniotic twins. pulmonary edema. Physiological
parity, maternal weight/height and diet. anemia is also common. Increased
Chorionicity is more easily identified risk for gestational hypertension and
Twins occur in approximately 1-2% of at ultrasound early in a woman’s preeclampsia are more common in
pregnancies with both physical and pregnancy and can reliably indicate women carrying twins and require
emotional wellbeing of paramount dichorionic twins. Ultrasonography increased surveillance of mother and
importance. Multiple gestation occurs in later gestations is not a reliable baby. Acute fatty liver of pregnancy
from the ovulation and subsequent indicator of chorionicity as placentas is a rare complication occurring more
fertilization of more than one oocyte often appear fused. Inter-twin frequently in multiple gestations.
resulting in genetically different membrane is absent in monochorionic/
dizygotic or non identical fetuses. Two monoamniotic (MCMA) twin
thirds of all twins are dizygotic and pregnancies and becomes more difficult
one third are monozygotic. Genetically to visualise with maturing gestational
identical fetuses occur from splitting age, oligohydramnios and progressive Parents
of one embryonic mass to form two thinning of the membrane. False
diagnosis may occur when separation expecting twins
or more genetically identical fetuses
(monozygotic). Dizygotic twins have of the amnion and chorion is mistaken require tailored clinical
for an inter-twin membrane.
their own amniotic sac (diamniotic) and care, counselling and
placenta (dichorionic). Dichorionic diamniotic (DCDA) is most management
commonly identified at 10 – 14 weeks
Ultrasonography gestation becoming less obvious after
Optimal timing for performing 20 weeks gestation. It is identified with
ultrasound examination for an inter-twin membrane with the ‘twin
chorioamnionicity is in the first peak’ or ‘lambda’ sign. This sign refers
trimester after 7 weeks. Assessment to a triangular tissue that extends
Counselling parents
of fetal membranes is more difficult between layers of the inter-twin
and less accurate in the third trimester membrane from a fused dichorionic Parents expecting twins require
and can be further complicated by placenta. Fetuses of different sex are tailored clinical care, counselling and
oligohydramnios. a highly reliable means of confirming management. Education and discussion
a dichorionic pregnancy. Monochorionic regarding optimal gestational weight
Assessment of chorioamnionicity Diamniotic (MCDA) twins inter-twin gain and nutritional requirements
occurs through ultrasonography and is membrane with the “T” sign is is recommended. Management of
critical to determine specific risks for comprised of two amnions attached to congenital anomalies in one or both
serious pregnancy complications such the placenta at a 90 degree angle. twins requires careful consideration
as twin-twin transfusion syndrome
12 GP ROUNDSof available therapies and delivery
times. Women experiencing multiple
pregnancy require more frequent Dr Amrou Metawa is
checkups to monitor babies growth a devoted expert and well
and development and potential respected Obstetrician and
pregnancy complications. Gynaecologist. Dr Metawa has
extensive experience in every
Increased risk of miscarriage, fetal
aspect of pregnancy care, he will
abnormalities, reduced fetal growth
give you exceptional and unique
and preterm birth and intrauterine
death is considerably higher in twin one on one care throughout
pregnancies rather than singleton your pregnancy.
pregnancies. In fact, twin pregnancies Dr Metawa is dedicated to
are associated with higher rates of providing care in high risk
almost every potential complication of pregnancy, VBAC (Vaginal Birth
pregnancy with the exception of post- after Caesarean section) and
dates and macrosomia. Breech delivery.
Dr Metawa has experience in Dr Metawa also treats all
managing twin pregnancies at Gosford aspects of Gynaecology
Private Maternity Services over the including, incontinence, pelvic
last 10 years. He has expertise caring floor prolapse, pelvic pain,
for women with multiple pregnancies endometriosis, uterine fibroid,
and enjoys providing compassionate
menorrhagia, Polycystic Ovary
care to these families. Expertise to
Syndrome (PCOS), ovarian cysts,
identify complications at an early
stage and collaboration with Gosford family planning and infertility,
Private’s neonatologists ensures menopause, adnormal pap smear,
evidenced based care and decision and colposcopy.
making is received. Dr Metawa
has experience with both vaginal
birth twins and caesarean births. North Gosford Medical Centre Call us: 02 4323 6140
At the time of twin deliveries, Dr Suite 9, Level 1, 12 Jarrett Street Email: info@drmetawa.com.au
Metawa ensures neonatal trained North Gosford NSW 2250
paediatricians are available for birth, www.drmetawa.com.au
care and follow-up appointments.
World renowned Neurosurgeon
visits Gosford Private Hospital
We are honoured to have Professor Marc Sindou visit Gosford Private Hospital
to conduct a dorsal root entry zone (DREZ) lesioning procedure, a pain relief
treatment not previously undertaken in Australia. The precedure involves cutting
part of the spinal cord to relieve pain in instances when nerves have been torn
away from the spinal cord or through spinal cord injury.
Professor Sindou is the Professor of Neurosurgery at the University of Lyon in
France, a Founding Member of International Association for the Study of Pain
(IASP), and Past President of the World Society for Functional and Stereotactic
Neurosurgery (WSSFN). He was also Vice-President of the European Association of
Neurosurgical Societies (EANS) and Teacher in the EANS Training Course.
With 22 visiting Professorships and works in over 640 scientific publications, Professor Sindou
specialises in Functional Neurosurgery, Microneurosurgery of Intracranial vascular malformations,
Skull Base Tumors, Meningiomas, and Neurophysiology Applied to Neurosurgery.
CENTRAL COAST NEWS 13MANAGEMENT OF LATE LIFE DEPRESSION
– with Psychiatrist, Dr Susil Stephen
Management
The overall management of major
depressive disorder in the elderly is
based on RANZCP Clinical Practice
Guidelines for mood disorders (2015).
The guidelines recommend a stepped
approach starting from addressing
sleep, lifestyle, diet and adopting
regular exercise regime. There is good
evidence for Psychological Therapy
including Cognitive Behavioural
Therapy (CBT), Interpersonal Therapy,
Acceptance and Commitment
Therapy (ACT) as well as Mindfulness-
Based Cognitive Therapy. It is
recommended that some form of
psychological intervention accompany
pharmacotherapy whenever possible.
Pharmacotherapy for major depressive
Introduction subtly different to those in younger disorders in the elderly requires
The Australian population is ageing, people. For example, older people careful consideration, by taking into
with older people a growing proportion are less likely to display affective account the age related changes
of the total population. Depression symptoms, but they are more likely in metabolism such as decreased
causes significant emotional suffering to show cognitive difficulties, somatic hepatic metabolism and reduced renal
in old age and is associated with symptoms, sleep disturbances, function. Lean body mass and total
poor quality of life. Key features agitation and anhedonia. The Geriatric body water decreases in old age with
of depression in later life are its Depression Scale (GDS-15) is a very a relative increase in body fat, and
comorbidities with various physical useful and validated screening tool for these changes could prolong the half-
illnesses and risk factors for developing depression. A score of > 5 warrants life of medications and may potentially
depression include deaths of family further assessment and a score of lead to toxicity. The prescriber
members and friends, increased > 10 almost always indicates should also be aware of the potential
isolation, declining health, financial depression. PHQ-9 is another validated drug interactions. The likelihood of
constraints, decreased cognitive screening instrument for depression in cognitive dysfunction with associated
functioning and loss of autonomy and general practice. The Cornell Scale for compliance and safety issues needs to
social roles. Depression in old age is Depression in Dementia (CSSD) is a be addressed by various medication
associated with a higher risk of suicide. tool that is validated to rate depressive management measures. The approach
Older women tend to have higher rates symptomatology in cognitively is “start low and go slow”. Due to
of depression and suicidal ideation impaired patients. the slower treatment response it
than older men, however older men are is important to allow more time
more likely to commit suicide. before switching medications. This
information should be discussed
with the patient and care providers
Clinical features and assessment Prevalence of at treatment initiation in order to
The prevalence of depression varies improve medication adherence.
from 5-15% in those attending
depression varies from
General Practitioner’s rooms and it 5-15% in those attending SSRIs are considered to be the first
increases to 15-25% in residents of choice antidepressants in an older
general practitioner’s person. Citalopram, escitalopram
aged care facilities. Depression in
older people is often missed due to rooms, to 15-25% in or sertraline may be preferred as
they are generally better tolerated.
erroneous perception of some of the residents of aged Paroxetine and fluoxetine can increase
overlapping features as a normal part
of the ageing process or conditions care facilities the risk of drug interactions due
such as dementia. The symptoms of to hepatic enzyme induction and
depression in an older adult can be should be avoided. Other classes of
14 GP ROUNDSantidepressants such as mirtazapine If the above pharmacological Electroconvulsive Therapy (ECT) is a (NaSSA), agomelatine (melatonergic treatments are ineffective, it is safe and very effective treatment for agonist), along with venlafaxine, advisable to seek a specialist opinion. severe depression with melancholic, desvenlafaxine and duloxetine (SNRIs) Further steps in management strategies psychotic or catatonic features are also part of the recommended include augmentation of antidepressant or patients at high risk of suicide. first line treatment. The second line with Lithium and atypical Repetitive Transcranial Magnetic antidepressants include TCAs and antipsychotics or combining certain Stimulation (rTMS) is a treatment MAOIs. Anticholinergic side effects antidepressants. Predictors of likely modality that is gathering momentum of TCAs may be poorly tolerated response to Lithium augmentation but its efficacy in older people is yet to and are dose related. Nortriptyline include recurrent depression with more be seen. In summary, an older person is the preferred choice as it causes than three episodes and family history with depression should be offered the less postural hypotension, sedation of depression in a first degree relative. same range of pharmacological and and anticholinergic effects than the Second generation antipsychotics non-pharmacological therapies and other TCAs. Older persons are more such as aripiprazole, olanzapine, age should not be a barrier to specific prone to antidepressant-induced quetiapine and risperidone can be therapies. hyponatraemia, osteoporosis and effective as augmentation agents, prolonged bleeding and these risks are and are administered at much lower more associated with SSRIs. Regular doses than those recommended for monitoring is recommended. schizophrenia and bipolar disorder. Dr Susil Stephen joined Brisbane Waters Private Hospital in 2018 and manages older patients in the outpatient and inpatient settings. He previously worked as a consultant old age psychiatrist in the UK for a few years. Since moving to Australia in 2015, he has been working as a Senior Staff Specialist Psychiatrist at Wyong Hospital. He is a faculty member of the Old Age Psychiatry division of the RANZCP and an accredited supervisor for trainee psychiatrists. Dr Stephen’s special interests include mood and anxiety disorders as well as organic psychiatry. Central Coast Clinic Brisbane Waters Private Hospital Call us: 02 4343 0265 Level 2/21 Vidler Ave Woy Woy NSW 2256 Email: drsusilstephen@gmail.com Successful 3rd Annual Central Coast Mental Health Conference Over 100 delegates joined esteemed Psychiatrists Dr Tanveer Ahmed, Dr Mark Cross, Dr Greg Pearson (shown) and Dr Ted Cassidy at the 3rd Annual Central Coast Mental Health Conference ‘From Moods to Madness – A Psychological Masterclass for Primary Health’ at the Crowne Plaza Terrigal as part of Mental Health Month in October. With topics covering everything from troubled teens to psychosis, bi-polar disorder to depression, the event has established itself as the pre-eminent Mental Health Conference for practitioners on the Central Coast and beyond. Learn more about the services available at the Central Coast Clinic at centralcoastclinic.com.au CENTRAL COAST NEWS 15
ADMIN UPDATES
GP Provider Numbers
A newly implemented database
in the Endoscopy Unit at Gosford
Private Hospital requires our
patient information to have the
correct GP’s provider number.
This isn’t information that we
have kept in the past and with a
very messy database there was
no other way to tackle it other
than phone you all one by one.
A huge thank you to all the GP
secretaries that have assisted us
with your GP Provider Numbers.
Online Preadmissions
The Gosford Private Hospital
Online Preadmission Portal has
been updated to a more user
friendly program. We still need
to ask our patients all the same
medical questions but the format
is easier to use. If any of your
patients are experiencing difficulty
using the new form, ask them to
give us call and we can help.
Admission Booklets
–– All patients, regardless of recent admission, are required
to complete an admission booklet. However, if the
patient has been a patient at the hospital in the last
3 months, the admission is for the same reason as
previous admission and no details have changed about
medication or medical history then they don’t need
to complete the ‘patient health history’ section of the
admission booklet.
–– Please remind patients to forward the admission paperwork
to the relevant hospital ASAP, preferably two (2) weeks
prior to admission.
Consent Forms
–– Please ensure the original consent forms are left with
the patient admission booklets.
–– To reduce the amount of calls to your rooms, can we
please request that the consent forms are completed
with either the “definitive”, or the “proposed” item
numbers on them.
16 GP ROUNDSYou can also read