A Practical Approach to the Diagnosis of Hodgkin Lymphoma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pathology Patterns Reviews
A Practical Approach to the Diagnosis of Hodgkin
Lymphoma
Catherine M. Listinsky, MD
Key Words: Hodgkin lymphoma; Progressive transformation of germinal centers; PTGC; T-cell–rich large B-cell lymphoma; TCRBCL;
Anaplastic large cell lymphoma; ALCL; Peripheral T-cell lymphoma; PTCL; Richter transformation; Composite lymphoma
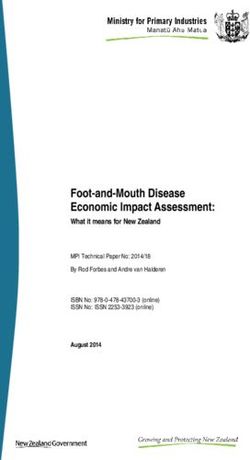
Abstract Hodgkin lymphoma commonly comes to the attention of
The diagnosis of Hodgkin lymphoma has become the morphologist with an unmistakable image of solitary
more difficult in recent years, paradoxically because of gigantic atypical cells looming over sheets of small, mixed
great strides made in the understanding of the molecular inflammatory cells ❚Image 1❚. This is the paradigm of diagnosis
mechanisms driving the lymphomas. Extensive panels of in Hodgkin lymphoma, basic since the time of Sternberg1 and
monoclonal antibodies, coupled with flow cytometric Reed,2 familiar to students and former students of clinical patho-
analyses and molecular diagnostic studies, have served physiology, and deceptively simple. Nevertheless, in clinical
to define more lymphoma subtypes that cannot be diagnostic practice, Hodgkin lymphoma has long been notorious
identified based on morphologic evidence alone. This for a broad range of morphologic features that can challenge the
overview is intended to provide useful criteria for the most experienced pathologist. On one end of the spectrum,
recognition of Hodgkin lymphoma and to recommend subtypes of Hodgkin lymphoma can be mistaken for a variety of
tools that will aid in separating Hodgkin lymphoma benign conditions, including lymphoid follicular hyperplasia,
from a series of common benign and malignant look- progressive transformation of germinal centers (PTGCs), plasma
alikes. The relationships among Hodgkin lymphoma, the cell variant of Castleman disease, and granulomatous reactions.3-5
B-cell non-Hodgkin lymphomas, and the T-cell non- On the other end of the spectrum, they might mimic non-
Hodgkin lymphomas are discussed, and useful Hodgkin lymphoma, poorly differentiated carcinoma, malignant
immunohistochemical markers for the routine diagnosis melanoma, or high-grade sarcoma. The reverse problem, the
of Hodgkin lymphoma are suggested. mistaken diagnosis of Hodgkin lymphoma, was common before
the availability of immunohistochemical studies. Such misdiag-
noses were reported to occur in from 13% to 47% of cases
reevaluated by expert panels.6,7 Most of these cases represented
non-Hodgkin lymphomas that were misclassified as Hodgkin
lymphomas; however, a substantial minority of cases includes
benign entities. A more recent study of cases diagnosed between
1988 and 1994 found only 11 cases of 362 that were misdiag-
nosed as Hodgkin lymphoma.8
The morphologic diagnosis of Hodgkin lymphoma has
become more difficult in recent years, paradoxically because of
the progress made in understanding molecular mechanisms
driving the lymphomas and the immune system in general.
Expanded panels of monoclonal antibodies, coupled with flow
cytometric analyses and molecular diagnostic studies, have
served to define more lymphoma subtypes. Nodular lymphocyte
S76 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical Pathology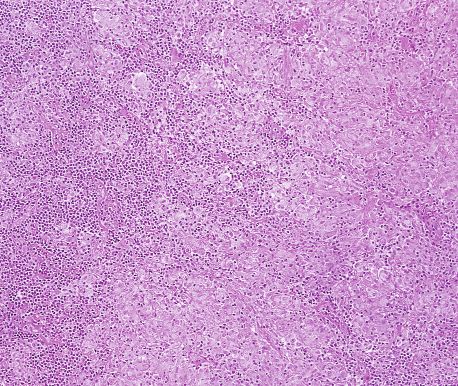
Pathology Patterns Reviews
disease is a true malignant lymphoma—a clonal neoplasm of
lymphoid origin. Hence, the nomenclature has been changed
from Hodgkin disease to Hodgkin lymphoma in the new
WHO classification.13,32
Lymphocyte predominant Hodgkin lymphoma was the
first subtype to be closely linked to lymphoid malignant
neoplasms because it frequently was associated with diffuse
large B-cell non-Hodgkin lymphomas in composite and
sequential malignant neoplasms arising within the same
patient.33-40 Proof of a clonal relationship, however, awaited
the development of special techniques. In 1993, Küppers et
al41 reported the isolation of single cells from frozen sections
of human germinal centers that they studied by sensitive
polymerase chain reaction (PCR) techniques. These tech-
niques permitted the later molecular study of individual
L&H (“lymphocytic and histiocytic”) cells in lymphocyte
❚Image 1❚ Classic Reed-Sternberg cell, dwarfing the benign predominant Hodgkin lymphoma and demonstrated the
lymphocytes of the background milieu (H&E, ×250). clonal identity of these cells and their homology with the
cells of the associated diffuse large B-cell lymphoma.42-45
Subsequent molecular studies have established the clonal B-
predominant Hodgkin lymphoma (NLPHL) has emerged as a lineage nature of NLPHL.46-49 The presence of immunoglob-
clinicopathologic entity, distinctly different from classic ulin gene hypermutations in the isolated, clonal L&H cells
Hodgkin lymphoma (CHL).9-13 Lymphocyte-rich CHL has led to the conclusion that these cells were derived from the
been defined; it histologically resembles and must be distin- germinal center stage of B-cell development, nicely tying the
guished from NLPHL.14-16 T-cell–rich large B-cell lymphoma molecular biologic features to the morphologic features.47-50
has been described17,18 and, in many cases, has an important Unlike the cells of follicular non-Hodgkin lymphoma, there
relationship with NLPHL.19-23 The separation of T-cell–rich is no evidence of bcl-2 gene rearrangement or overexpres-
large B-cell lymphoma from NLPHL and peripheral T cell sion of bcl-2 protein in lymphocyte predominant Hodgkin
lymphomas is difficult but clinically important.17,18,21,22,24-29 lymphoma.51 Unlike the Reed-Sternberg (R-S) cells of CHL,
Anaplastic large cell lymphoma has been described and closely the L&H cells exhibit the ability to express immunoglobulin
resembles some types of lymphocyte depletion Hodgkin on their surfaces.41,50
lymphoma.30,31 Since 1990, these latter problems have been, CHL also has been shown to arise from clonal cells of
and they continue to be, the subjects of intense study. follicular center origin by using PCR on single R-S
My aim is to present an overview of problems in the diag- cells.50,52-59 These cells differ from L&H cells of lymphocyte
nosis of Hodgkin lymphoma that will be of practical value to a predominant Hodgkin lymphoma in that the R-S cells fail to
morphologist studying a new case, using a limited panel of express surface immunoglobulin; this recently has been
immunoperoxidase reagents for use in paraffin-embedded tissue. shown to be secondary to a defect in the transcription of
This overview will consider a mixture of problems—some that messenger RNA rather than to a crippling mutation of the
were well known before the introduction of molecular methods immunoglobulin genes themselves.50,60 Therefore the R-S
in understanding lymphomas and some that have arisen more cells of CHL constitute a population of end-stage cells that
recently in distinguishing newly defined entities. I briefly review ordinarily would undergo apoptosis in a normal germinal
important changes in our understanding of Hodgkin lymphoma center environment.61 Recent studies, reviewed by Izban et
since 1990 and the current World Health Organization (WHO) al,62 have shown that R-S cells constitutively overexpress
classification as it applies to Hodgkin lymphoma. high levels of active nuclear NF kappa B, which is an impor-
tant regulator of genes expressed during inflammatory
responses. Izban et al62 demonstrated that NF kappa B has a
critical role as an apoptosis blocker in R-S cells. Postulated
Overview of Recent Changes in the
mechanisms to account for the increased NF kappa B include
Understanding of Hodgkin Lymphoma
activation of NF kappa B (for example, by Epstein-Barr virus
Since 1990, our understanding of the nature of Hodgkin [EBV] latent membrane protein [LMP] through tumor
lymphoma has evolved considerably. While its cell of origin necrosis factor–associated factor), and abnormalities of regu-
was controversial in 1990, it is now widely accepted that the latory (inhibitory) proteins I kappa B alpha (described in
© American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S77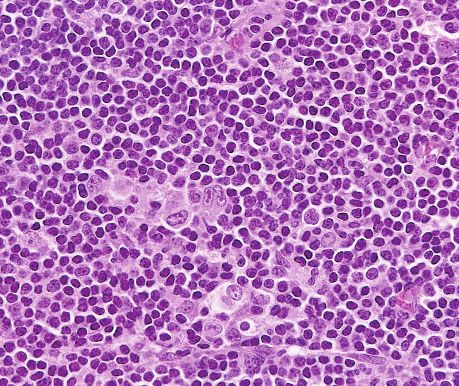
Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
some Hodgkin disease cell lines). Mutations of the I kappa B ❚Table 1❚
alpha gene have been found in some R-S cells.62,63 World Health Organization Classification of Hodgkin
Lymphoma
The aforementioned mechanisms seem to underlie the
majority of cases of CHL; however, rare cases of CHL have Nodular lymphocyte predominant
been shown to arise from the T-cell lineage.59,64,65 Classic
Lymphocyte-rich classic
Nodular sclerosis
Mixed cellularity
Lymphocyte depletion
Hodgkin lymphoma, unclassifiable
Hodgkin Lymphoma in the New WHO
Classification
The new WHO classification of tumors of hematopoi-
etic and lymphoid tissues13,32,66 recognizes that Hodgkin plasma cells, fibroblasts and collagen fibers.”32 ❚Image 3❚
lymphoma is a true lymphoma, but preserves its separation illustrates the morphologic and immunohistochemical
from non-Hodgkin lymphomas because of important clin- features of CHL. Recognition of CHL requires the identifi-
ical differences in disease distribution and treatment cation of classic R-S cells and their variants. Classic R-S
response. Hodgkin lymphoma is divided into 2 main cate- cells characteristically are gigantic cells with 2 or more
gories, NLPHL and CHL, in keeping with the different nuclear lobes; prominent, mirror-image, eosinophilic, inclu-
immunophenotypes and molecular events demonstrated in sion-like nucleoli; and abundant amphophilic cytoplasm
these malignant neoplasms ❚Table 1❚ . Still, these main (Image 1 and Image 3B). However, atypical variants and
disease categories share some histologic similarities, suboptimally processed variants can be recognized by their
including their cytokine-induced milieu of abundant reactive characteristic immunophenotype even when ideal, classic
inflammatory cells with malignant cells in the minority. In cells are not seen (Table 2).66
fact, in some cases, the morphologic distinction between In the WHO classification, CHL continues to include
NLPHL and CHL is not possible without supporting the subgroups of nodular sclerosing Hodgkin lymphoma
immunohistochemical studies.13,14,16,32,66 (NSHL, characterized by bands of birefringent collagen and
lacunar cell variants of R-S cells), mixed cellularity Hodgkin
Definitions According to the WHO32 lymphoma (MCHL, with variable mixes of lymphocytes,
“Nodular lymphocyte predominant Hodgkin lymphoma eosinophils, plasma cells, neutrophils, and histiocytes), and
(NLPHL) is a monoclonal B-cell neoplasm characterized by lymphocyte depletion Hodgkin lymphoma (LDHL, see
a nodular, or a nodular and diffuse, polymorphous prolifera- “Recognition of LDHL and Its Distinction From Non-
tion of scattered neoplastic cells known as popcorn or L&H Hodgkin Lymphomas”) as in the previous Rye classification.
cells (lymphocytic and/or histiocytic Reed-Sternberg cell CHL also includes the new subgroup of lymphocyte-rich
variants). These cells reside in large spherical meshworks of CHL (LRCHL). This subgroup morphologically resembles
follicular dendritic cell processes that are filled with non- NLPHL; however, the malignant cells exhibit the
neoplastic lymphocytes.”32 ❚Image 2❚ illustrates the charac- immunophenotype of classic R-S cells. The WHO committee
teristic morphologic and immunohistologic findings seen in recommended further that cases that do not strictly fit the
NLPHL. An essential part of the recognition of NLPHL is aforementioned categories be termed Hodgkin lymphoma,
the identification of L&H cells. These variants, in their most unclassifiable, rather than placed by default into the MCHL
distinctive form, have multilobated nuclei with pale, vesic- class. This would avoid the use of MCHL as a “wastebasket”
ular chromatin resembling popcorn. Usually nucleoli are category (which it was in previous classifications).13
indistinct and cytoplasm is delicate, pale, and retracted;
however, there are exceptions in which L&H cells have
prominent nucleoli and their appearance can approach the
Immunohistochemical Markers Useful
morphologic appearance of R-S cells.10,13,16,32,66-68 In these
for Diagnosing Hodgkin Lymphoma
cases, they are recognized as NLPHL-derived L&H cells by
their distinctive immunophenotype and the immunopheno- The most useful immunohistochemical markers in the
type of the cells in the surrounding milieu ❚Table 2❚. routine diagnosis of Hodgkin lymphoma are listed in Table 2.
“Classical Hodgkin lymphoma (CHL) is a monoclonal In NLPHL, the L&H cells are positive for the mature B-
lymphoid neoplasm composed of mononuclear Hodgkin cell marker CD20 (Image 2C), negative for CD15 (Leu M1),
cells and multinucleated Reed-Sternberg … cells residing in and usually negative for CD30 (Ki-1).32 Each cellular nodule
an infiltrate containing a variable mixture of non-neoplastic of the milieu has a broad dendritic cell network (which may
small lymphocytes, eosinophils, neutrophils, histiocytes, be visualized with the CD21 immunostain). In most cases,
S78 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical Pathology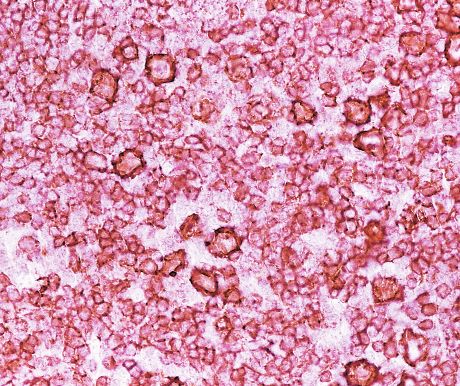
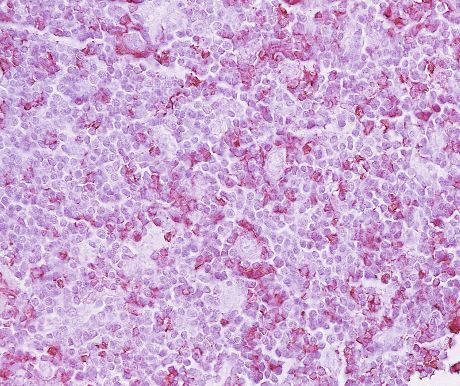
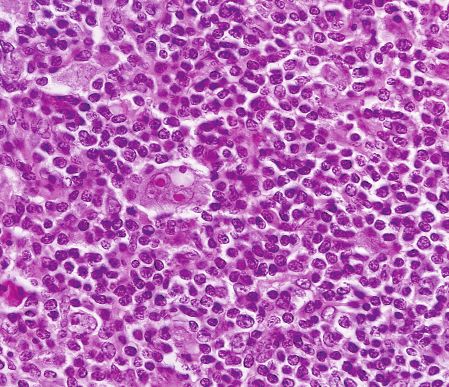
Pathology Patterns Reviews A B C D ❚Image 2❚ The characteristic features of nodular lymphocyte predominant Hodgkin lymphoma (NLPHL). A, Large, rounded, mottled cellular nodules (H&E, ×25). B, L&H (lymphocytic and histiocytic) cells often have “popcorn” nuclei (H&E, ×625). C, Mature B-lineage marker CD20 is strongly positive in the large L&H cells and in most of the small lymphocytes in the background. There is a ring of CD20– cells around many of the large L&H cells (CD20, ×250). D, CD57 often is expressed in rosettes of T cells that surround the L&H cells (a pan–T cell marker, such as CD3, would give a similar pattern; however, the CD57+ T-cell rosettes are virtually specific for NLPHL). The L&H cells are negative for CD15 and (usually) CD30 (CD57, ×250). the majority of small lymphoid cells of the nodules are poly- In CHL, independent of subtype, R-S cells are usually clonal, CD20+ B cells (although T cells may predominate in positive for CD15, an antigen normally expressed in granulo- later stages of the disease). However, there is a distinctive cytes and monocytes but not in lymphocytes. A pattern of tendency for CD57+ T cells to surround the L&H cells, both Golgi zone and cell membrane positivity by CD15 is forming rosettes69 (Image 2D). CD57+ T cells normally are the most specific for R-S cells (Image 3E). However, expres- present in small numbers in benign lymphoid germinal sion of CD15 is variable and present in only 75% to 85% of centers, where they are postulated to have a part in regulation cases, and in some of these, the staining is focal and some- of the immune response.69 The numbers of these cells are times seen only in rare cells.70 Therefore, negativity for increased in reactive follicles and are present as scattered CD15 does not rule out Hodgkin lymphoma. CD30 antigen single cells within low-grade follicular lymphomas. The (Image 3F) is expressed strongly on R-S cells in almost all largest numbers of CD57+ cells are seen in NLPHL. cases of CHL71,72; however, CD30 is an activation antigen © American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S79
Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
❚Table 2❚
Tools Useful for the Diagnosis of Hodgkin Lymphoma
Classic Type (Lymphocyte-Rich Classic, Nodular
Nodular Lymphocyte Predominant Type Sclerosis, Mixed Cellularity, Lymphocyte Depletion)
Immunoperoxidase
Reaction on Paraffin- Lymphocytic and
Embedded Tissue Histiocytic Cell Milieu Reed-Sternberg Cell Milieu
CD15 (Leu M1) Negative Negative Golgi zone positive; Neutrophils positive
membrane positive
CD30 (Ki-1) Negative Negative Positive Negative
Pan–T-cell markers Negative Few lymphocytes positive Usually negative Most lymphocytes positive
(UCHL-1 or CD3)
Pan–B-cell marker Positive Most lymphocytes positive Usually negative Few lymphocytes positive
(CD20)
CD57 (activated T cells) Negative T lymphocytes positive Negative Negative
around L&H cells
CD21 Negative Follicular dendritic cell Negative Negative
network positive
that also is expressed in benign cells responding to a stim- eosinophils, small histiocyte aggregates, or scattered atypical
ulus (for example, CD30 is expressed in the transformed cells (knowing that early involvement may manifest as
cells of EBV infection). It also is expressed in non-Hodgkin “interfollicular Hodgkin lymphoma”; see “Focal Involve-
lymphomas, including anaplastic lymphoma kinase (ALK)+ ment of a Lymph Node by Hodgkin Lymphoma [Interfollic-
anaplastic large cell lymphomas and in some aggressive ular Hodgkin Lymphoma]”). If “suspicious” but nondiag-
diffuse large B-cell lymphomas. Therefore, while CD30 is a nostic areas are found, 3 additional levels of the block should
sensitive marker for R-S cells, it is not specific. R-S cells be scanned in a similar manner, looking for satisfactory diag-
express a mixture of antigens relating to B cells, T cells, nostic R-S cells.74
myeloid cells, and natural killer (NK) cells72,73; however, The diagnosis may be very difficult if the histologic
they usually are negative for common leukocyte antigen sections are too thick, such that they obscure the presence of
CD45, CD20, and pan–T-cell markers. The cells of the the large cells; in this case, thin recut sections often provide
milieu in CHL are predominantly polyclonal T cells with a the correct diagnosis ❚Image 4❚.
prominent CD4 subset.66 Other artifactual problems may obscure the morpho-
logic features of a biopsy specimen, such as poor fixation or
a crush artifact in a minute specimen, which often is a
problem in core, mediastinoscopic, or transbronchial biopsy
Problems in the Diagnosis of Hodgkin
specimens. In these cases, immunoperoxidase studies can
Lymphoma: A Practical Approach
help to detect or confirm the identity of the atypical cells or
CHL often is easy to recognize, especially in the to heighten the index of suspicion to justify a repeated
common nodular sclerosing form with its striking low-power biopsy ❚Image 5❚.66 Immunoperoxidase reactions for CD15
architecture and in the mixed cellularity form when there are and CD30 are both useful; however, if tissue is scant, the
abundant eosinophils in the milieu along with classic R-S CD30 reaction is one’s most valuable ally as it will be more
cells.6-8 In these cases, the diagnosis of Hodgkin lymphoma likely to detect rare R-S cells.
is not a problem, and special studies usually are not Even with excellent sections, the histologic diagnosis of
required.66 For the remainder of the cases, the most powerful Hodgkin lymphoma can be difficult in cases that contain few
diagnostic tools are a high index of suspicion and a careful R-S cells, when the histologic pattern of the benign milieu
histopathologic examination performed on technically satis- mimics benign disorders and the R-S cells are not noticed
factory H&E-stained sections. ❚Image 6❚ , and when R-S cells are overabundant and
When there is a strong clinical suspicion of Hodgkin resemble other neoplasms. Our main defense against missing
lymphoma and the histopathologic findings in the lymph these forms of Hodgkin lymphoma is familiarity with them:
node are equivocal, one knows to scan the tissue section once Hodgkin lymphoma is included in the differential diag-
slowly at intermediate magnification in a search for R-S nosis of these look-alikes, the appropriate scan for R-S vari-
cells, their variants, or any large atypical cells that seem out ants is undertaken and the appropriate diagnostic
of place. In an apparently reactive lymph node, one should immunoperoxidase reactions are sought. Examples of several
look closely in the parafollicular zones for areas of increased of these difficult problems follow.
S80 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical Pathology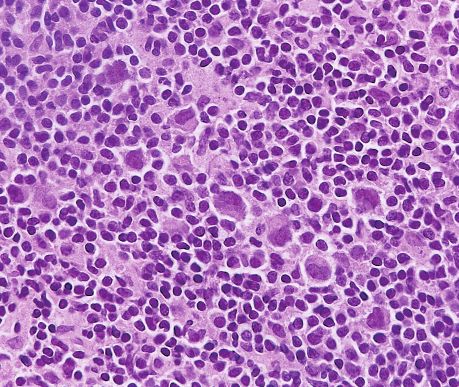
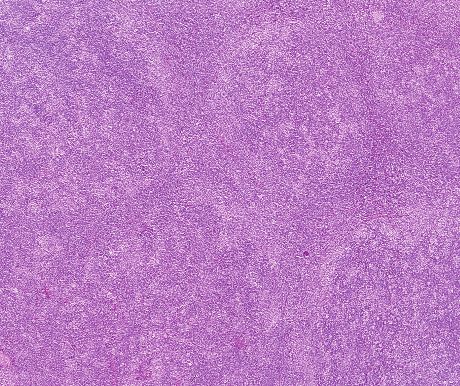
Pathology Patterns Reviews A B C D E F ❚Image 3❚ The characteristic features of classic Hodgkin lymphoma (mixed cellularity type). A, Classic Reed-Sternberg (R-S) cells and their mononuclear variants have large eosinophilic inclusion-like nucleoli and abundant amphophilic cytoplasm (see also Image 1) (H&E, ×250). B, Benign lymphocytes, plasma cells, eosinophils, and histiocytes are noted in the milieu (H&E, ×625). C, CD20 shows few B cells in the background (×250). D, CD3 shows numerous small T cells in the milieu, some surrounding the R-S cells (these are negative for CD57) (×250). E, CD15 (Leu M1) exhibits a Golgi and membrane pattern (×250). F, CD30 (Ki-1) also exhibits Golgi and membrane staining (×250). © American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S81
Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
A B
C D
❚Image 4❚ Thick sections (A and C) and respective thin sections (B and D) are from the same block of tissue. Flow cytometry
showed B-cell small lymphocytic lymphoma. The thin recut sections revealed easily found Reed-Sternberg cells and variants;
however, these were difficult to detect on the original thick sections, even in retrospect. (A and B, H&E, ×250; C and D, H&E, ×625)
Recognition of NLPHL
NLPHL accounts for only 5% of cases of Hodgkin benign histiocytes. The malignant cells (L&H cells) are
lymphoma and, therefore, is not seen regularly in many most concentrated near the centers of the nodules, and,
general diagnostic practices. Morphologically, it may be while their nuclei are large and atypical, the L&H cells
mistaken for a benign reactive lymph node or for a low- tend to be pale and vesicular, lacking inclusion-like
grade non-Hodgkin lymphoma. NLPHL is best recog- nucleoli and having only moderate amounts of delicate,
nized on low-power examination of a lymph node, in pale cytoplasm. Sometimes they are multilobated, often
which it appears as a mass with at least partial obliteration resembling popcorn; thus, they may not offer the degree
of the lymph node architecture (Image 2). The lesions are of instant recognition that classic R-S cells provide.
composed of large back-to-back, somewhat vaguely (Compare Image 2B and Image 3B, which were taken at
defined nodules of cells; however, on high-power exami- the same magnification).
nation the cells are mainly small, unremarkable lympho- L&H cells express pan–B-cell antigens and CD45 and
cytes that are polyclonal on flow cytometric examination, are negative for CD15 and CD30. The CD20 immunostain is
mixed with variable proportions of loosely clustered particularly informative: the large atypical cells usually are
S82 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical Pathology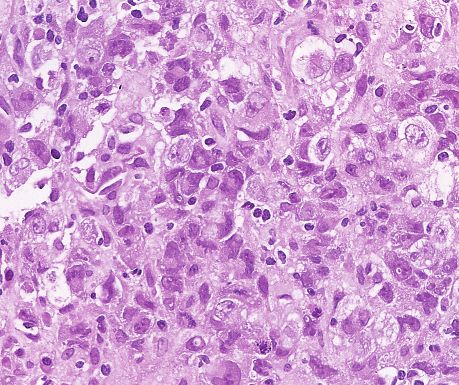
Pathology Patterns Reviews A B ❚Image 5❚ A, A thymic cyst in a 17-year-old girl contained an atypical cellular and fibrotic area in its wall, highly suggestive of involvement by Hodgkin lymphoma, but with suboptimal morphologic preservation (H&E, ×250). B, Immunoperoxidase reactions confirmed the Reed-Sternberg immunophenotype of the large atypical cells (CD30 is illustrated, showing Golgi and membrane staining) (CD30, ×625). A B ❚Image 6❚ A, Recurrent adenopathy in a patient whose previous biopsies were called “consistent with sarcoidosis” or “granulomatous inflammation” (H&E, ×125). B, Closer examination showed mononuclear Reed-Sternberg (R-S) variants. Immunoperoxidase reactions showed many cells with the characteristic R-S immunophenotype, and additional levels revealed diagnostic R-S cells (H&E, ×250). strongly positive, as are most of the background cells in the ❚Figure 1❚ provides a simplified scheme for working nodules (Image 2C). However, there often is a halo of through the differential diagnosis of cases that morphologi- CD20– small lymphocytes surrounding the large cells, and cally resemble NLPHL, in that the nodular infiltrate includes these small lymphocytes are T cells that express surface a minor population of large atypical lymphoid cells that are CD57 and appear as rosettes around the large cells (Image surrounded by abundant small lymphocytes. The diagnosis 2D). The presence of these rosettes is variable and some- relies heavily on immunoperoxidase reactions in paraffin- times focal in distribution; therefore, absence of CD57 embedded tissue, since some of the diseases in question have rosettes does not rule out NLPHL. very low proportions of malignant cells. Flow cytometry is © American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S83
Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
of little use in view of the abundant benign polyclonal Large: CD20–, Large: CD20+ Large: CD20+
milieu, and the labels must be correlated with the morpho- CD3+, or CD3– Small: CD3+ Small: Mostly CD20+
Small: CD3+ or CD3– except CD3+ rosettes
logic features of the cells. Immunoglobulin gene rearrange-
around large
ment studies do not detect these low levels of clonal cells
when performed on whole tissue. The CD20 and CD3 reac- +TCR gene +TCR gene Large: CD20+,
Large: CD20+,
tions effectively stratify these cases into 3 groups (top row in rearrangement rearrangement CD30–, CD15– CD30+,
Figure 1) when the staining patterns of the large vs the small PTCL PTCL with CD15+ or CD15–
activated B cells LRCHL
cells are noted separately. Additional CD15, CD30, and CD57+ rosettes or
CD57 reactions and occasionally CD21 stains can help to No CD21+ FDC CLL with
CD57+ rosettes
?DLPHL? RS-like cells
establish the diagnosis among NLPHL, diffuse lymphocyte CD21+ FDC network
NLPHL (clonal by
predominant Hodgkin lymphoma, T-cell/histiocyte–rich flow cytometry
large B-cell lymphoma (TC/HRLBCL), LRCHL, or chronic No CD57+ or gene
rosettes rearrangement)
lymphocytic leukemia (CLL) with R-S–like cells (see
No CD21+ DRC
“Chronic Lymphocytic Leukemia With R-S–Like Cells TCRBCL
Mimicking Hodgkin Lymphoma”). Figure 1 indicates that
peripheral T-cell lymphomas also can share these morpho- ❚Figure 1❚ Large atypical cells among small cells. CLL, chronic
logic features. When T-cell lymphomas exhibit a normal lymphocytic leukemia; DLPHL, diffuse lymphocyte
surface immunophenotype, only molecular methods can predominant Hodgkin lymphoma; FDC, follicular dendritic
confirm the diagnosis. If necessary, T-cell receptor gene cells; LRCHL, lymphocyte-rich classic Hodgkin lymphoma;
rearrangements can be evaluated in material extracted from NLPHL, nodular lymphocyte predominant Hodgkin lymphoma;
paraffin-embedded tissue. PTCL, peripheral T-cell lymphoma; RS, Reed-Sternberg; TCR, T-
Since 1997, it has been recognized that “Lymphocyte cell receptor; TCRBCL, T-cell–rich large B-cell lymphoma.
predominant Hodgkin disease is a more immunohistochem-
ical rather than a purely morphological diagnosis.”75 Cases
of lymphocyte predominant Hodgkin disease (n = 104), only by immunohistochemical analysis in two thirds of the
initially diagnosed purely on a morphologic basis by the cases. Of the cases, 21% exhibited the antigen profile of
expert panel of the German Hodgkin Study Group (GHSG), CHL and were termed lymphocyte-rich classic Hodgkin
included 25 cases in which the atypical cells demonstrated lymphoma. Most of these cases were nodular and a few were
the immunophenotype of R-S cells of classic Hodgkin diffuse. The LRCHL cases bore a clinical resemblance to
disease.75 These were reclassified as classic Hodgkin disease NLPHL but on average affected an older group of people
and would fall into the LRCHL category in the WHO classi- and had more frequent occurrence of a large mediastinal
fication. The remaining cases would fall into the NLPHL mass.15 Relapse was less frequent than for NLPHL, but
group of tumors. when present was associated with a less favorable
prognosis.15 Among cases of Hodgkin lymphoma, the inci-
Recognition of LRCHL dence of LRCHL was approximately 6%, and the incidence
In 1995, Ashton-Key et al14 reported a group of cases of of NLPHL was approximately 5%, calculated from the
Hodgkin lymphoma in which the architecture resembled the GHSG reports.13,75,76
nodular architecture of NLPHL, and the small cells in the
nodules were predominantly small B lymphocytes, but the Distinction of NLPHL From PTGCs
scattered atypical cells reacted with the antibodies usually PTGCs refers to 1 or more scattered, markedly
expressed by the R-S cells of CHL. Unlike NLPHL, these enlarged germinal centers that occur in the context of a
nodules included eccentric clusters of follicular dendritic lymph node with florid reactive lymphoid follicular hyper-
cells associated with atrophic germinal centers. Thus, this plasia. These gigantic germinal centers lose the distinct
morphologic mimicker of NLPHL had immunophenotypic mantle zone as mantle cells migrate into the germinal
features distinctly different from NLPHL and was termed center and separate islands of follicular center cells in an
follicular Hodgkin disease.14 This study led to a retrospective irregular pattern. These transformed germinal centers are
multi-institutional review (with 16 oncology centers partici- the same size as the large indistinct nodules of NLPHL.
pating), considering 388 patients who initially were diag- Through single-cell analysis of the proliferating (Ki-67+)
nosed with lymphocyte predominant Hodgkin disease (Euro- cells in these PTGCs, Bräuninger et al 77 were able to
pean Task Force on Lymphoma).15,16 Like the study of the demonstrate clonal expansion within each nodule but not
GHSG,75 this review demonstrated that the morphologic clonal identity of cells from different nodules, unlike
diagnosis of NLPHL by an expert panel could be confirmed studies of NLPHL.
S84 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical Pathology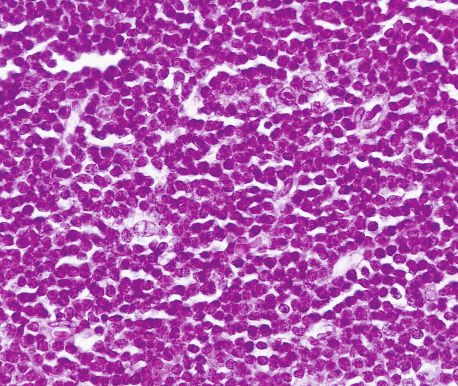
Pathology Patterns Reviews
Since both PTGCs and NLPHL are disorders of diagnosis, 5 had generalized adenopathy, 4 had splenomegaly
germinal center cell derivation, they both contain many of and/or hepatomegaly, and 4 had bone marrow involvement.
the components of normal germinal centers, including a Other authors had previously described a similar clinical
network of dendritic cells and the presence of many CD57+ course, with a male predominance and advanced stage
T cells. While it is more likely that one will find rosettes of including hepatosplenomegaly and bone marrow involve-
CD57+ T cells around the L&H cells of NLPHL and not in ment,17,18,20,23,25,26,29,80,83 although bone marrow involvement
PTGCs, this reaction may not be helpful for diagnosis in was not present in pediatric cases.84
individual cases for the following 2 reasons. First, in many TC/HRLBCL has been variously described as a de novo
cases of NLPHL the rosettes of CD57+ T cells are rare and non-Hodgkin lymphoma, as a type of transformation of low-
widely separated. Second, CD57+ T cells may be abundant grade follicular lymphoma,39 and as a type of transformation
in benign reactive germinal centers and surround the benign in patients with NLPHL.20-22 In 2 studies, single-cell PCR
transformed follicular center cells (centroblasts), giving the has shown clonal identity between L&H cells of NLPHL and
misleading suggestion of a rosette. Kraus et al78 identified subsequent or simultaneous TC/HRLBCL.45,57 Therefore, it
CD57+ rosettes of T cells in 2 cases of PTGCs; however, is not surprising that NLPHL may have a strong histologic
they found no “true” rosettes, which they defined as bcl-6+ B and immunophenotypic resemblance to TC/HRLBCL or
cells rimmed by CD57+ T cells, by using dual-labeling of even overlap with it. This is one of the “gray zones” in
specimens. Therefore, the best practical way to distinguish lymphoma diagnosis in which there may be a true biologic
PTGCs from NLPHL is by low-power microscopic examina- transition between the diseases.85 Owing to the striking
tion of routine H&E-stained sections. PTGCs occur as 1 or 2 difference in the clinical implications of these 2 diagnoses,
gigantic follicles in the context of florid lymphoid follicular they must be distinguished from one another, if possible.
hyperplasia, whereas NLPHL is a mass-forming lesion that The immunophenotype of the large B cells of
causes at least partial obscuring of the lymph node architec- TC/HRLBCL is similar to that of L&H cells of NLPHL:
ture.79 In the extreme case, a hypothetical very small focus of CD20+ but CD15– and CD30–.13,86 Sometimes they express
NLPHL in a reactive lymph node could not be diagnosed cytoplasmic light chains and sometimes epithelial membrane
with certainty, since the markers and features might be iden- antigen. However, the architecture and the type of T cells in
tical with the features of the cells in PTGCs. the milieu should be helpful in making the distinction. If the
pan–B-cell antigen shows nodular aggregates of the large
Distinction of Hodgkin Lymphoma From T-Cell–Rich cells or abundant small B lymphocytes in the background, or
Large B-Cell Lymphoma if a CD21 reaction shows clusters of follicular dendritic cells
The term T-cell–rich large B-cell lymphoma originally indicating a nodular architecture, the diagnosis is NLPHL
was a general term for any diffuse malignant lymphoma with (TC/HRLBCL is, by definition, a diffuse process). Also, the
neoplastic large B cells in a background of more than 50% presence of abundant CD57+ T cells in the milieu with
small reactive T cells. In current usage, according to Harris,13 “rosetting” around the large B cells indicates NLPHL.13,86
“T-cell/histiocyte-rich large B cell lymphoma (TC/HRLBCL) However, when NLPHL shows areas of diffuse architecture,
is a diffuse lymphoma with a lymphocyte-rich background, those areas contain increased proportions of reactive small T
with small clusters of epithelioid histiocytes and numerous cells and fewer CD57+ T cells. Therefore, in the extreme,
scattered large mononuclear cells, suggesting either NLPHL NLPHL may be indistinguishable from TC/HRLBCL (or
or CHL” (emphasis added). The atypical B cells can exhibit equal to a subset of this disease).20,21,79,87
the cytomorphologic features of L&H cells, R-S cells, or In cases of TC/HRLBCL with cells resembling R-S
centroblasts, and there may be an admixture of these cell cells, the histologic features mimic CHL. In these cases, the
types.80 The abundant T-cell infiltrate seems to be due to diagnosis may be recognized because the large atypical cells
interleukin-4 production by the tumor cells and histiocytes.81 are positive for pan–B-cell antigens and negative for CD15,
At present, there is no consensus as to the percentage of reac- CD30, and epithelial membrane antigen.
tive T cells required in the background infiltrate, and different
studies have used cutoffs ranging from 50% to more than Recognition of Focal Transformation of NLPHL
90%.26,27 The WHO includes cases with fewer than 10% large Into Diffuse Large B-Cell Lymphoma
neoplastic B cells in this category.32 In 2% to 10% of patients with NLPHL, large B-cell
Several series of cases have suggested that the lymphoma develops.13,35,88,89 In some cases of NLPHL, the
TC/HRLBCL pattern corresponds to a disease that is “biolog- proportions of L&H cells within the nodules can be high.
ically distinct” from other lymphomas. For example, in the According to the consensus of participants in the Work-
recent series of 8 cases studied by Vidovic et al,82 5 patients shop on the Interrelationship of Hodgkin’s Disease and the
were male, 5 had stage IV disease and 2 had stage III disease at Non-Hodgkin’s Lymphomas (Society for Hematopathology,
© American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S85Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
San Antonio, TX, 1991), an increase in large cells that is Chronic Lymphocytic Leukemia With R-S–Like Cells
confined to the nodules is not considered sufficient for the Mimicking Hodgkin Lymphoma
diagnosis of transformation to large B-cell lymphoma. The For many years it has been observed that occasional
presence of separate areas with solid sheets of large cells is cases of B-cell chronic lymphocytic leukemia (B-CLL)
required.40 contain cells that morphologically resemble the R-S cells of
Hodgkin lymphoma (termed R-S–like cells). Sometimes
Hodgkin Lymphoma Subtypes (NSHL, NLPHL, and these cells appear scattered singly within the monotonous
MCHL) With a Milieu Resembling a Common Benign sheets of small CLL cells (Image 4),92-94 and sometimes they
Entity appear surrounded by a zone of Hodgkin milieu.95-97 In the
Another cause of difficulty in recognizing Hodgkin latter cases, the cells mark as CD15+ R-S cells, and the
lymphoma occurs when the milieu resembles a common disease essentially behaves as a Hodgkin transformation (the
benign entity, so that Hodgkin cells are not sought. Small Hodgkin disease variant of Richter syndrome) and responds
biopsy specimens may sample neutrophils, abscesses, or to Hodgkin therapy, unlike the large B-cell form of Richter
caseating necrotic areas in NSHL, leading to a focus on syndrome.92,93,96,97 However, the clinical significance of
inflammatory or infectious differential diagnoses. Fine- cases with R-S–like cells scattered singly, without the
needle aspiration biopsies in Hodgkin lymphoma have been Hodgkin milieu, is uncertain. Sometimes the cells of these
reported to have diagnostic accuracy spanning a range from cases express the classic markers of R-S cells,92,93,96-98 and
30% to 92%, limited mainly by the abundant benign milieu sometimes they express the CD20+, CD15– immunopheno-
and fibrosis of Hodgkin lymphoma.90 type of the surrounding B-CLL cells.93,94,99 Among the cases
Sometimes the florid proliferation of histiocytes in the that were reported separately in 2 series,92,93 4 of 10 CD15+
Hodgkin milieu leads first to the differential diagnosis of cases transformed into CHL and none of 13 CD20+CD15–
granulomatous diseases (one case initially called sarcoidosis cases transformed into Hodgkin lymphoma. It originally was
is shown in Image 6). Hodgkin lymphoma has long been speculated that these latter cases, although morphologically
notorious for granulomatous appearances (Hodgkin granu- identical to the former cases, were unrelated and did not
loma and Hodgkin paragranuloma are terms from the earlier imply an impending Hodgkin transformation. There was a
classification scheme of Jackson and Parker91). Usually the close association of the R-S–like morphologic features with
histiocyte clusters of the milieu of Hodgkin lymphoma are expression of EBV LMP-1, implying an immune reaction in
small, fairly loose aggregates of nonepithelioid cells, which these cells.93
lack the cohesive, well-defined margins of well-formed By using single-cell microdissection, amplification of
sarcoid granulomas. Our best diagnostic weapon is a high rearranged immunoglobulin genes, and sequence analysis,
degree of suspicion in new granulomatous lesions, especially Ohno et al100 demonstrated the clonal identity of CLL B cells
when the granulomas are small and poorly formed and when with the R-S cells of subsequent CHL in 2 of 3 cases (mate-
the nodal architecture is obliterated. In the case illustrated rial from case 3 was uninformative). Kanzler et al101 subse-
(Image 6), an intermediate-power scan (retrospectively) quently reported 3 cases in which the R-S–like cells were
revealed the presence of atypical cells in the biopsy spec- within the background of otherwise typical CLL. In 1 case,
imen. This finding should have led to the suspicion of the R-S–like cells were confirmed to be clonal and identical
Hodgkin lymphoma and to the performance of the appro- to the clone of the CLL cells. In the other 2 cases, the R-
priate special stains for diagnosis. S–like cells were confirmed to be clonal but not related to
the CLL clone; that is, the presence of 2 distinct expanded B-
Focal Involvement of a Lymph Node by Hodgkin cell clones was identified. These last 2 cases, however,
Lymphoma (Interfollicular Hodgkin Lymphoma) showed the presence of EBV in the R-S cells (indicating
Sometimes Hodgkin lymphoma partially and subtly clonal expansion of an EBV-harboring B cell in the setting of
infiltrates the interfollicular area of lymph nodes, eliciting a B-CLL).101 In 1 EBV+ R-S cell clone, somatic mutations
florid lymphoid follicular hyperplasia and immune prolifera- rendered an originally functional immunoglobulin variable
tion in the surrounding lymph node parenchyma. This may chain gene (V gene) rearrangement (in CLL) nonfunctional
resemble a benign lymphoid hyperplasia or a “plasmacel- (in R-S cells). Kanzler et al101 concluded that the R-S–like
lular” variant of Castleman disease.4,5 In cases such as this, cells in B-CLL are potential precursors for authentic R-S
the diagnosis is made by identifying the R-S cells and cells causing Hodgkin disease. The English language litera-
confirming their presence by immunohistochemical analysis. ture also has included reports of 2 cases of CLL that were
Extreme caution is required if numerous immunoblasts are associated with NLPHL rather than CHL.96
present in the background, since R-S–like cells may be seen Finally, a subset of CLL cases are known to undergo
in a florid immune response.4,5 high-grade transformation in which the CLL is interspersed
S86 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical PathologyPathology Patterns Reviews
with sheets and irregular aggregates of CD15+ R-S–like cells, controversial than the reticular subtype, is extremely
sometimes with geographic necrosis, resembling LDHL.98 rare.31,79 Some of the nodes are markedly depleted of cells
Two such cases, described by Rubin et al,98 were associated and replaced by amorphous, eosinophilic, fibrillar but
with EBV, with EBV LMP positivity recognized in the R-S nonbirefringent material.105 In some cases, the fibrosis may
cells and in occasional CLL cells before transformation. In be “partially or prominently fibroblastic,” and in these the
these cases, the results of light chain studies were consistent mass may resemble fibromatosis (when the R-S cells are rare
with a single clonal origin of the R-S cells and CLL cells.98 and inconspicuous) or malignant fibrous histiocytoma (when
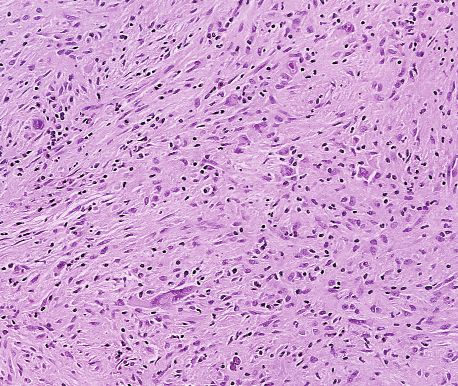
Viewing these transformed cases of CLL in retrospect, bizarre R-S variants are found).105 LDHL has a tendency for
given our current understanding that the malignant cells of retroperitoneal origination and must be considered in the
CHL usually are derived from B-lineage cells, it seems cred- differential diagnosis of retroperitoneal sarcomas. The
ible that CLL can transform into Hodgkin lymphoma of any patient whose tissue is illustrated in ❚Image 7❚ had
of the classic subtypes or into NLPHL. Furthermore, it pulmonary and retroperitoneal masses at diagnosis. There
follows that the cases in which the R-S–like cells exhibit a were large cellular areas of predominantly spindle cell prolif-
B-cell immunophenotype seem to merit watchful follow-up eration in a storiform architecture, highly suggestive of
rather than immediate treatment for transformation.93 malignant fibrous histiocytoma (Image 7A). A few fields
contained bizarre multinucleated cells with prominent, inclu-
Recognition of LDHL and Its Distinction From sion-like, eosinophilic nucleoli (Image 7B). Such inclusion-
Non-Hodgkin Lymphomas like nucleoli are not characteristic of malignant fibrous histi-
The most rare subtype of Hodgkin lymphoma, LDHL, ocytoma. The presence of these cells provided a clue that
has been a controversial subject since the early 1980s. In the prompted the appropriate immunoperoxidase studies. The
past, this category was shown to contain many improperly atypical cells were CD15+ and CD30+, and negative for
classified non-Hodgkin lymphomas when the cases were histiocyte markers and broad-spectrum cytokeratin, estab-
subjected to expert panel review.6,102 In a retrospective lishing the diagnosis of Hodgkin lymphoma (Image 7C).
analysis of 39 cases that were classified as LDHL at the The reticular form of LDHL is characterized by infil-
National Institutes of Health before 1986,102 only 9 could be trating sheets of R-S cells and variants. It now is suspected
verified as LDHL. These 9 cases responded to MOPP therapy that most cases that originally were classified as reticular
(mechlorethamine, vincristine, procarbazine, and prednisone) LDHL (on morphologic grounds) were examples of the
with 67% achieving complete remission, and a median entity that since has been termed anaplastic large cell
survival not reached in 14 years of follow-up. Twenty cases lymphoma (ALCL).13,79 Therefore, the evolution of diag-
were reclassified as either NSHL or other CHL and achieved nostic criteria for ALCL, recently reviewed in detail by Stein
an 85% rate of complete remission. Ten cases were non- et al106,107 and Jaffe,108 is relevant to the story of LDHL.
Hodgkin lymphomas, with only 3 achieving complete remis- ALCL was first described as a morphologically distinctive
sion and a median survival of 7 months after MOPP therapy. lymphoma consisting of large, bizarre (“anaplastic”) cells,
Similarly, the review panel of the German Hodgkin Therapy with a propensity to sinusoidal infiltration of lymph nodes,
Trial found that most cases misdiagnosed as Hodgkin but also infiltrating as sheets of cells.106 Characteristic “hall-
lymphoma were, in fact, non-Hodgkin lymphomas that had mark” cells exhibited kidney-shaped, horseshoe-shaped, or
been mistakenly classified as LDHL or MCHL.103 Eghbali et even ring nuclei, and possessed irregular eosinophilic
al104 used immunohistochemical studies on cases that were nucleoli and often a prominent pale or eosinophilic Golgi
previously classified as LDHL and treated at their institution zone ❚Image 8❚.30,31,106,109 Cells were strongly positive for
between 1960 and 1991. All 31 cases required reclassifica- CD30 (Ki-1) antigen, and this was established as a criterion
tion, 14 into other subtypes of Hodgkin lymphoma and 17 for diagnosis; subsequently, the term Ki-1+ ALCL came into
into non-Hodgkin lymphomas.104 These authors further noted use.30,31,107 The disease was shown to manifest with several
that the diagnosis of LDHL had not been made in their insti- distinctly different clinical pictures, including an adult nodal
tution since 1985 and that a similar downward trend in the form, an adult cutaneous form, and a pediatric form.30 A
use of the category had been reported in several other institu- subset of these cases was found to have the distinctive
tions. It was postulated, for a time, that LDHL may not exist translocation between chromosomes 2 and 5.107,108,110-113
as a distinct entity; however, there are cases that seem to best This resulted in production of an abnormal fusion protein
fit in the LDHL category.102,104 between the nucleophosmin gene on chromosome 5 (NPM)
Assuming LDHL exists as a unique subclass, it can be and a gene for a novel kinase on chromosome 2 (termed
divided into the 2 morphologic subtypes that were part of the anaplastic lymphoma kinase, or ALK).114 This and other
original Lukes and Butler classification, diffuse fibrosis and described translocations involving chromosome 5q35 can be
reticular.105 The diffuse fibrosis subtype of LDHL, less detected by an immunoperoxidase reaction for ALK-1
© American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S87Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
A B
C ❚Image 7❚ A, Retroperitoneal mass with storiform
architecture and scattered gigantic atypical cells, suggesting
malignant fibrous histiocytoma (MFH) (H&E, ×125). B, The
atypical cells have prominent inclusion-like eosinophilic
nucleoli, not usually seen in MFH (H&E, ×250). C, The cells
have the Reed-Sternberg immunophenotype (CD15, ×625).
protein.66 The ALK+ cases have been found to constitute a entity has been ascertained to be nearly always (99%) a B-
distinctive clinicopathologic entity that includes younger lineage neoplasm. LDHL, as one of the CHLs, includes R-S
patients with node-based disease, T- or NK-cell immunophe- cells that usually express CD15, almost always express
notype, and a significantly better response to therapy CD30, and occasionally express CD20 and other pan–B-cell
compared with ALK– ALCL or diffuse large T- or B-cell antigens. Most notably, T- and NK-lineage lymphomas that
lymphoma.107,115,116 The ALK– cases include cutaneous express the ALK protein are excluded from Hodgkin
cases, anaplastic large B-cell lymphomas, and cases of lymphoma. LDHL also excludes large B-cell lymphomas
anaplastic large T- and NK-cell lymphomas that behave as and T-cell lymphomas that have detectable immunoglobulin
aggressive lymphomas. In the revised European-American gene or T-cell receptor gene rearrangements on whole
classification of lymphoid neoplasms, ALCL was applied tissue. 13 Cases with lymphoid depletion and a nodular
only to T- and NK-cell neoplasms. Large B-cell lymphomas pattern of sclerosis (which tend to manifest as mediastinal
with similar morphologic features were classified among the disease) have been reassigned to NSHL (see “Gray Zones
large B-cell lymphomas.108 Between ALCL and Hodgkin Lymphoma”).13
The “shifting sands of diagnostic hematopathology” so Appropriate immunoperoxidase reactions for the evalua-
aptly applied to the evolution of ALCL by Jaffe,108 have tion of possible LDHL include CD15, CD30, ALK-1, pan–B
shifted as well under LDHL. While the morphologic criteria cell, and pan–T cell. If these markers are negative, molecular
for Hodgkin lymphoma have not changed substantially, the studies for immunoglobulin gene rearrangements or T-cell
S88 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical PathologyPathology Patterns Reviews
A B
❚Image 8❚ A, Anaplastic large cell lymphoma with “hallmark
C
cells” (H&E, ×312). B, Many of the cells in this case have
apparent “doughnut” nuclei surrounding deeply eosinophilic
Golgi zones (H&E, ×625). C. Anaplastic lymphoma kinase
(ALK-1) shows Golgi and membrane staining. Lack of nuclear
staining by ALK in this case indicates that the ALK is
activated by a mechanism other than the translocation with
the nucleophosmin gene on chromosome 5 (×625).
receptor gene rearrangements should be performed to rule was denoted Hodgkin-like ALCL as a provisional entity in
out non-Hodgkin lymphoma. the revised European-American classification of lymphoid
Finally, it is easy to mistake the morphologic features of neoplasms.13 These cases may contain a heterogeneous mix
LDHL for much more common entities (such as metastatic of ALCL and Hodgkin lymphoma, and at present, most are
poorly differentiated carcinoma, metastatic malignant thought to be related more closely to Hodgkin lymphoma
melanoma, and ALCL, as shown in Image 8), all of which (termed ALCL-like Hodgkin lymphoma in the new WHO
may have R-S–like cells. The diagnostic panel of immunoper- classification).13,32,107,109,120 Some cases demonstrate CD15+
oxidase reactions in these cases also requires a broad-spectrum R-S cells. Most are ALK–.115 Many have aggressive nodal
cytokeratin (for carcinoma) and S-100 protein (for melanoma). disease and bulky mediastinal masses.13 Some cases cannot
be resolved and are termed unclassifiable.13
Gray Zones Between ALCL and Hodgkin Lymphoma
There is a group of lymphomas with morphologic archi- Relationship of Hodgkin Lymphoma to Mediastinal
tectural features of both ALCL and NSHL, and these origi- Large B-Cell Lymphoma
nally were termed Hodgkin-related ALCL30 or Hodgkin-like In the report of the Workshop on Hodgkin’s Disease and
ALCL.79,117-119 The neoplastic cells are arranged in cohesive Related Diseases (“gray zone” lymphoma), Rudiger et al85
sheets with a sinusoidal infiltration, and sclerotic bands of identified 7 cases of mediastinal lymphoma that showed
collagen divide the node into cellular nodules. This group overlap between diffuse large B-cell lymphoma and NSHL.
© American Society for Clinical Pathology Am J Clin Pathol 2002;117(Suppl 1):S76-S94 S89Listinsky / A PRACTICAL APPROACH TO THE DIAGNOSIS OF HODGKIN LYMPHOMA
Some cases showed composite presentation with separate Problems in the diagnosis of Hodgkin lymphoma are not
areas fulfilling the diagnostic criteria for each entity; some trivial and continue to be a subject of intense study among
were considered borderline. In all cases there were sheets of hematopathologists. While morphologic examination
malignant tumor cells that were strongly positive for CD30 remains the mainstay (“gold standard”) of diagnostic work, it
and CD20. In 3 of 7 cases, the cells also expressed CD15, is clear that the new molecular findings have served to illu-
and in 1 they were positive for EBV LMP. They were nega- minate and explain both the morphologic and the clinical
tive for ALK protein. Interestingly, in his series, Pileri31 differences between major classes of malignant lymphomas.
noted that 20% of the “Hodgkin-related subtype of ALCL” Molecular studies have brought greater insight into the
expressed B-cell markers. These may be related to the 7 nature of lymphomas that behave differently from each other.
cases described by Rudiger et al.85 As noted by Harris,13 we now know that the cell of origin of
a lymphoma is less important in determining the behavior of
Distinction of Peripheral T-Cell Lymphoma With a neoplasm than is the transforming event that occurred in
R-S–like Cells From CHL the cell. This is clearly illustrated by the example of 5 malig-
Peripheral T-cell lymphomas frequently contain large nant lymphomas that now are known to arise from follicular
R-S–like cells that are CD15+ and CD30+. Also, it is not center cells: follicular lymphomas, Burkitt lymphoma,
unusual for the reactive T lymphocytes in the milieu of NLPHL, CHL, and an aggressive subcategory of diffuse
Hodgkin lymphoma to appear somewhat atypical. Therefore, large B-cell lymphoma. In addition to these insights, molec-
to rule out a peripheral T-cell lymphoma, studies for T-cell ular studies have resulted in the development of tools that
receptor gene rearrangements usually are needed for patients have been refined and are available for routine diagnosis and
with new MCHL or LDHL. classification of the lymphomas.
From the Department of Pathology, University of Alabama at
Birmingham, and the Birmingham Veterans Affairs Medical Center.
Discussion Address reprint requests to Dr Listinsky: Dept of Pathology,
This review is intended to provide useful criteria for the University of Alabama at Birmingham, 1922 7th Ave South,
Kracke Bldg, Room 506, Birmingham, AL 35233.
recognition of Hodgkin lymphoma and to recommend tools
that will aid in separating Hodgkin lymphoma from a series
of common benign and malignant look-alikes. Clearly, the
References
task has been more complex than one might expect from a
1. Sternberg C. Uber eine eigenartige unter dem Bilde der
clinical perspective; however the effort is deemed worthwhile Pseudoleukamie verlaufende Tuberculose des lymphatischen
since, at present, the treatment of Hodgkin lymphoma is Apparates. Ztschr Heilk. 1898;19:21-90.
specific and has a high success rate for all histologic subtypes 2. Reed D. On the pathological changes in Hodgkin disease,
when compared with mimicking non-Hodgkin lymphomas. with especial reference to its relation to tuberculosis. Johns
Hopkins Hosp Rep. 1902;10:133-196.
Conversely, unnecessarily harsh therapy might be instituted if
3. Miettinen M, Franssila K. Malignant lymphoma simulating
Hodgkin lymphoma is misdiagnosed as non-Hodgkin lymph node toxoplasmosis. Histopathology. 1982;6:129-140.
lymphoma. This said, there is nevertheless a clear relationship 4. Doggett RS, Colby TV, Dorfman RF. Interfollicular Hodgkin’s
among Hodgkin lymphoma, the B-cell non-Hodgkin disease. Am J Surg Pathol. 1983;7:145-149.
lymphomas, and the T-cell non-Hodgkin lymphomas. Gray 5. Wilson CS, Chang KL, Weiss LM. Malignant lymphomas
zones remain where occasional lymphomas show features of that mimic benign lymphoid lesions: a review of four
lymphomas. Semin Diagn Pathol. 1995;12:77-86.
both types (eg, the ill-defined border of NLPHL with
6. Miller TP, Byrne GE, Jones SE. Mistaken clinical and
TC/HRLBCL, the rare T-cell variant of CHL and its ill-
pathologic diagnoses of Hodgkin’s disease: a Southwest
defined border with peripheral T-cell lymphoma). Composite Oncology Group study. Cancer Treat Rep. 1982;66:645-651.
or sequential lymphomas arise in a background of CHL and 7. Kim H, Zelman RJ, Fox MA, et al. Pathology Panel for
NLPHL to further reinforce the relationships among these Lymphoma Clinical Studies: a comprehensive analysis of cases
disorders: composites of NLPHL and TC/HRLBCL,39,40,79,121 accumulated since its inception. J Natl Cancer Inst.
1982;68:43-67.
follicular lymphoma and Hodgkin lymphoma,39 composites
8. Glaser SL, Dorfman RF, Clarke CA. Expert review of the
of T-cell lymphomas and Hodgkin lymphoma,39,40,65,122,123 diagnosis and histologic classification of Hodgkin disease in a
and even possible composites of NLPHL with both B-cell population-based cancer registry: interobserver reliability and
and T-cell lymphomas.68 It is important to recognize the inter- impact on incidence and survival rates. Cancer. 2001;92:218-224.
relationships that are revealed through these composite 9. Stein H, Hansmann ML, Lennert K, et al. Reed-Sternberg
and Hodgkin cells in lymphocyte-predominant Hodgkin’s
presentations and thereby to choose criteria that enable clini- disease of nodular subtype contain J chain. Am J Clin Pathol.
cally relevant distinctions for treatment and prognostication. 1986;86:292-297.
S90 Am J Clin Pathol 2002;117(Suppl 1):S76-S94 © American Society for Clinical PathologyYou can also read