Antibody Response to COVID-19 Vaccination in Patients Receiving Dialysis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Antibody Response to COVID-19 Vaccination in Patients
Receiving Dialysis
Journal: Journal of the American Society of Nephrology
Manuscript ID JASN-2021-05-0611.R2
Manuscript Type: Research Letters
Date Submitted by the
24-May-2021
Author:
Complete List of Authors: Anand, Shuchi; Stanford University, Department of Medicine
(Nephrology)
Montez-Rath, Maria; Stanford University, Department of Medicine
(Nephrology)
Han, Jialin; Stanford University, Department of Medicine (Nephrology)
Garcia, Pablo; Stanford University, Department of Medicine (Nephrology)
Cadden, LinaCel; Ascend Clinical Laboratory
Hunsader, Patti; Ascend Clinical Laboratory
Kerschmann, Russell; Ascend Clinical Laboratory
Beyer, Paul; Ascend Clinical Laboratory
Dittrich, Mary ; US Renal Care
Block, Geoffrey; US Renal Care
Boyd, Scott; Stanford University, Department of Pathology
Parsonnet, Julie; Stanford University, Departments of Medicine
(Infectious Diseases and Geographic Medicine), and Epidemiology and
Population Health
Chertow, Glenn; Stanford University, Departments of Medicine
(Nephrology), and Epidemiology and Population Health
immunology, chronic dialysis, clinical nephrology, immunosuppression,
Keywords:
COVID-19, Antibody Formation, renal dialysis, Vaccination
Journal of the American Society of Nephrology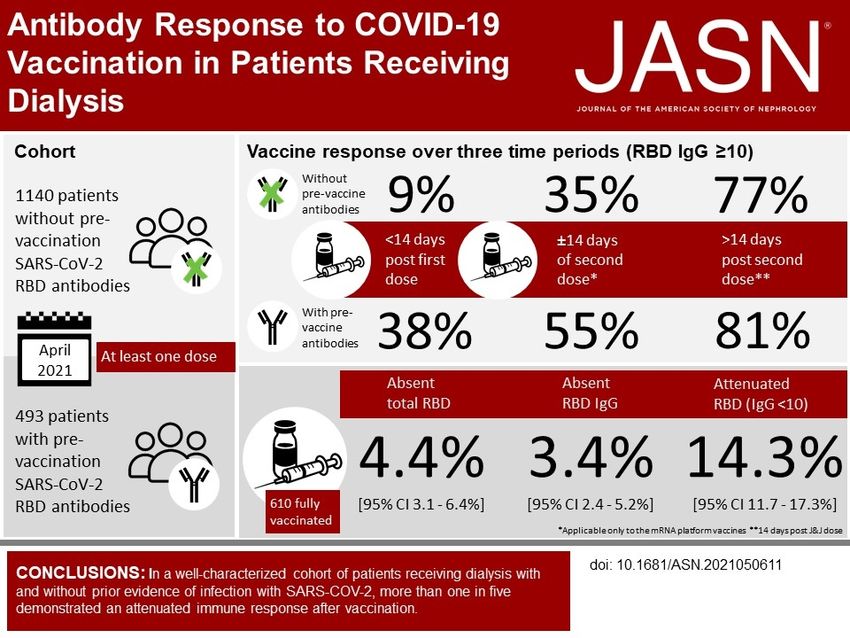
Page 1 of 22
1
2
3 Authors: Anand, Shuchi; Montez-Rath, Maria; Han, Jialin; Garcia, Pablo; Cadden, LinaCel; Hunsader,
4
Patti; Kerschmann, Russell; Beyer, Paul; Dittrich, Mary ; Block, Geoffrey; Boyd, Scott; Parsonnet, Julie;
5
6
Chertow, Glenn
7
8 Title: Antibody Response to COVID-19 Vaccination in Patients Receiving Dialysis
9
10 Running title: Antibody Response to COVID-19 Vaccination
11
12 Manuscript Type: Research Letters
13
14
15 Funders: Ascend Clinical Laboratory, (Grant / Award Number: )
16 National Institutes of Health, (Grant / Award Number: 'K24DK085446','R01DK127138')
17
18 Financial Disclosure: CUST_FINANCIAL_DISCLOSURE :No data available. LC, PH, RK and PB are employed
19 by Ascend Clinical Laboratories. GC is on the Board of Satellite Healthcare, a not for profit dialysis
20 organization. S. Anand reports Research Funding from Applied Pragmatic Research Grant, from Satellite
21
healthcare; Honoraria from American Kidney Fund; and Scientific Advisor or Membership with i3C (ISN)
22
23
& CENCAM. M. Montez-Rath reports Research Funding from Sanofi. G. Block reports current
24 employment with US Renal Care; Consultancy Agreements with Kirin, Akebia, Keryx, Reata; Ownership
25 Interest in Ardelyx, Reata; Research Funding from Akebia, Ardelyx, GSK; Honoraria from Kirin, Amgen;
26 Scientific Advisor or Membership with Reata, Kirin, Ardelyx, CJASN; and Other Interests/Relationships as
27 prior member on ESC of KDIGO, prior Medical Director at Davita, and prior employment with Reata. G.
28 Chertow reports Consultancy Agreements with Akebia, Amgen, Ardelyx, Astra Zeneca, Baxter, Cricket,
29 DiaMedica, Gilead, Miromatrix, Reata, Sanifit, Unicycive, Vertex; Ownership Interest in Ardelyx,
30 CloudCath, Durect, DxNow, Eliaz Therapeutics, Outset, Physiowave, PuraCath; Research Funding from
31
NIDDK, NIAID; Scientific Advisor or Membership as Co-Editor of Brenner & Rector's The Kidney (Elsevier);
32
33 an dOther Interests/Relationships via DSMB service, NIDDK, Angion, Bayer, and ReCor. S. Boyd reports
34 Consultancy Agreements with Regeneron, Sanofi, Novartis; Ownership Interest in AbCellera, CareDx;
35 Honoraria from NIH, Karolinska Institutet; Patents and Inventions from U.S. Patent No. 9,068,224,
36 licensed to Adaptive Biotechnologies; and Scientific Advisor or Membership with Food Allergy Fund. R.
37 Kerschmann reports Consultancy Agreements with Ascend Clinical, Grail, Inc., Notable Labs, and Octave
38 Bioscience. M. Dittrich is employed by US Renal Care; and has Ownership Interest in US Renal Care,
39 Signify Health, and Multiple dialysis units.
40
41
42 Study Group/Organization Name: CUST_STUDY_GROUP/ORGANIZATION_NAME :No data available.
43
44 Study Group Members’ Names: CUST_STUDY_GROUP_MEMBERS :No data available.
45
46 Total number of words: 886
47
48 Abstract: DOCUMENT_ABSTRACT :No data available.
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of Nephrology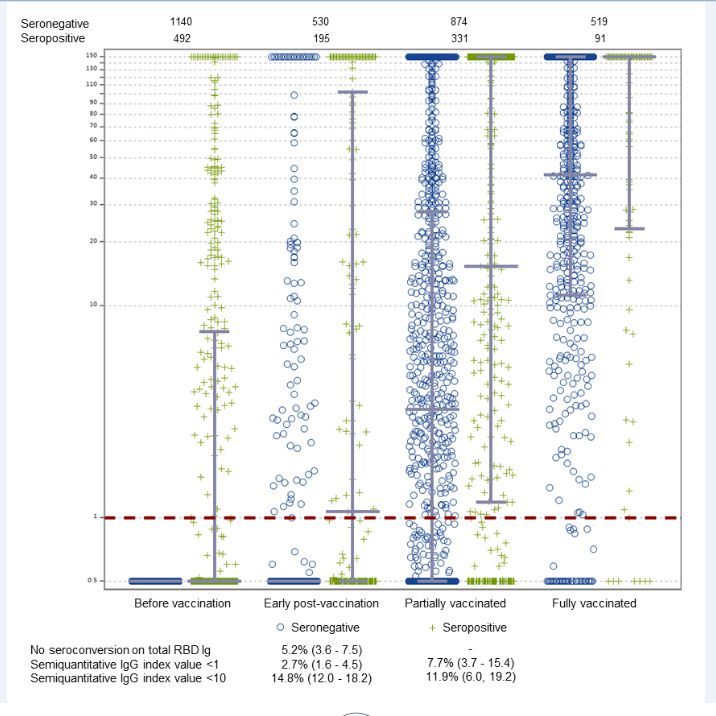
Page 2 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 Antibody Response to COVID-19 vaccination in Patients Receiving Dialysis
4
5
6
7 Authors:
8
9 Shuchi Anand, MD, Department of Medicine (Nephrology), Stanford University
10 Maria E. Montez-Rath, PhD, Department of Medicine (Nephrology), Stanford University
11 Jialin Han, MS, Department of Medicine (Nephrology), Stanford University
12 Pablo Garcia, MD, Department of Medicine (Nephrology), Stanford University
13 LinaCel Cadden, CLS, Ascend Clinical Laboratory
14 Patti Hunsader, CLS, Ascend Clinical Laboratory
15
Russell Kerschmann, MD, Ascend Clinical Laboratory
16
17 Paul Beyer, MBA, Ascend Clinical Laboratory
18 Mary Dittrich, MD, US Renal Care
19 Geoffrey A Block, MD, US Renal Care
20 Scott D Boyd, MD, PhD, Department of Pathology, Stanford University
21 Julie Parsonnet, MD, Departments of Medicine (Infectious Diseases and Geographic Medicine), and
22 Epidemiology and Population Health, Stanford University
23
Glenn M Chertow, MD, Departments of Medicine (Nephrology), and Epidemiology and Population
24
25 Health, Stanford University
26
27 Corresponding author:
28 Shuchi Anand, MD
29 777 Welch Road Suite DE
30 Palo Alto California, US 94304
31 sanand2@stanford.edu
32 ph: 650 725 2207
33
34
35
36
37 Running title: Antibody Response to COVID-19 Vaccination
38
39 Keywords: immunology, chronic dialysis, clinical nephrology, immunosuppression, COVID-19, antibody
40 formation, renal dialysis, vaccination
41
42
43
44 Word count: 961
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of Nephrology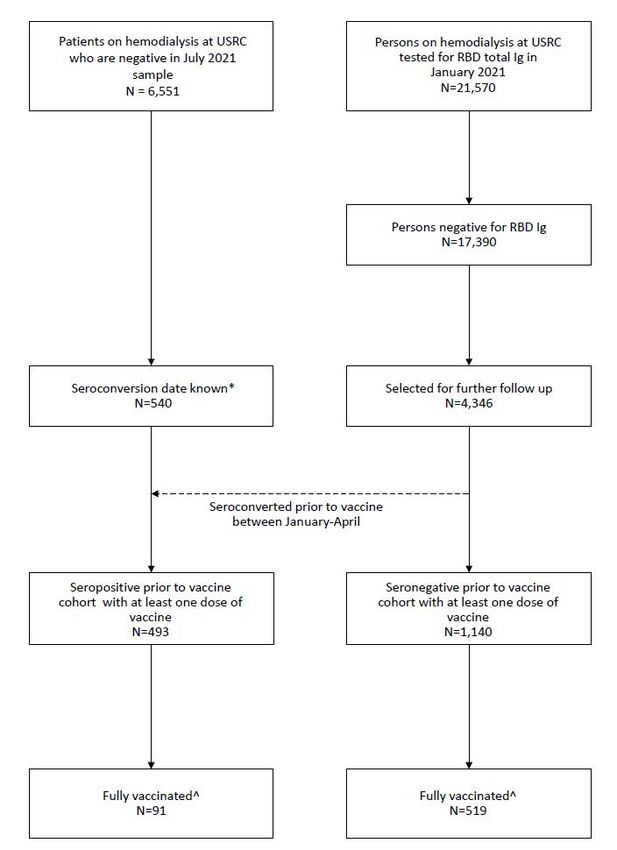
Page 3 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 Data from hepatitis B1 and influenza vaccination2 studies indicate blunted and foreshortened response to
4
5 immunization in patients receiving dialysis, raising the worrisome possibility that the SARS-CoV-2
6
7
vaccine may also yield lower efficacy in this population. We report early data on receptor binding domain
8
9
10 (RBD) seroconversion and semi-quantitative IgG values post vaccination in 1140 patients without, and
11
12 493 patients with, pre-vaccination SARS-CoV-2 RBD antibody. Among the subset who completed two
13
14 doses of vaccination, we assess rates of and risk factors for absent or attenuated response.
15
16
17 Our study was conducted in partnership with the dialysis network US Renal Care and Ascend Clinical
18
19 Laboratory. In the first two weeks of January 2021—prior to widespread vaccine roll out—we tested
20
21 SARS-CoV-2 antibody status of 21,570 patients receiving dialysis. From among the 17,390 seronegative
22
23 patients in January 2021, we used systematic sampling with fraction intervals stratified by age to
24
25 randomly select 4,346 persons to follow with monthly SARS-CoV-2 serology assays, in association with
26
27 type and date of vaccination(s) (see Supplemental Methods for assay characteristics and sample size
28
29 details). We also followed 540 patients seropositive as of January 2021, and any additional patients who
30
31 seroconverted prior to vaccination (see Supplemental Figure 1 for “seropositive prior to vaccination”
32
33
and “seronegative prior to vaccination” cohorts). We tested remainder samples using the Siemens’ total
34
35
36 RBD Ig assay, which measures IgG and IgM antibodies, in January 2021 and monthly thereafter in the
37
38 seronegative prior to vaccination cohort. Subsequent to a positive total RBD Ig result in the seronegative
39
40 and among all patients in the seropositive prior to vaccination cohorts, we tested samples only using a
41
42 semiquantitative Siemens RBD IgG assay monthly.
43
44
45 We evaluated response over three time periods: 14 days post the Johnson and Johnson vaccine or second dose of the
50
51 mRNA platform vaccines or (fully vaccinated). We classified responses as absent total RBD Ig antibody,
52
53 absent semiquantitative IgG antibody (index valuePage 4 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 As of April 2021, 1140 patients on dialysis without prior SARS-CoV-2 antibodies and 493 patients with
4
5 extant antibodies received a dose of vaccine (Supplemental Table 1). In the seronegative prior to
6
7
vaccination cohort, 9%, 35%, and 77% of patients had RBD IgG values ≥10 in the early post-vaccine,
8
9
10 partially vaccinated, and fully vaccinated groups, respectively. In the seropositive cohort, the proportions
11
12 were higher in the earlier periods (38%, 55%, and 81%, respectively). Median IgG levels were lower in
13
14 the seronegative compared with the seropositive cohorts (Figure 1). Among the seronegative prior to
15
16 vaccine cohort, median IgG index values post vaccination were 0.5 (25th, 75th percentile 0.5, 0.5), 3.2 (0.5,
17
18 27.8), and 41.6 (11.3, 150.0) in the early, partially and fully vaccinated periods respectively. Among the
19
20 seropositive prior to vaccine cohorts, median IgG index values post vaccination were 0.5 (0.5, 7.6), 1.1
21
22 (0.5, 102.3), 15.3 (1.2, 150), and 150 (23.2, 150) in the prior to, early, partially and fully vaccinated
23
24 periods respectively.
25
26
27 We assessed vaccine response among fully vaccinated patients a median of 29 (25th, 75th percentile 22,
28
29 39) days post vaccine completion. Of the 610 fully-vaccinated patients, 27 (prevalence 4.4% [95% CI 3.
30
31 1, 6.4%]), 21 (3.4% [2.4, 5.2%]), and 87 (14.3% [11.7, 17.3%]) had absent total RBD, absent
32
33
semiquantitive IgG, and attenuated IgG response, respectively. The prevalence of absent or attenuated
34
35
36 response was similar in seronegative and seropositive cohorts (Figure 1). Supplemental Tables 2 and 3
37
38 show results stratified by age and pre-vaccination seropositive status and sensitivity analysis assessing
39
40 responses at least 28 or more days post vaccine completion.
41
42
43
Non-white race and Hispanic ethnicity were associated with a lower risk of absent or attenuated response;
44
45 longer dialysis vintage and lower serum albumin were associated with a higher risk (Supplemental Table
46
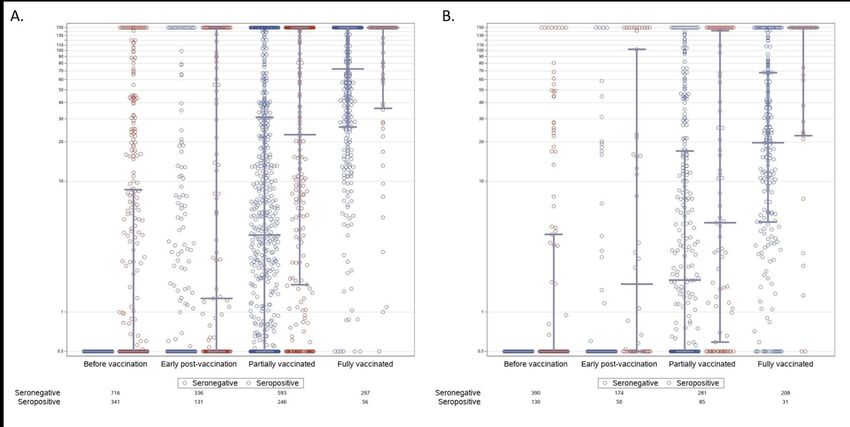
47 4). Median RBD IgG levels were modestly lower for Pfizer than for the Moderna vaccine (Supplemental
48
49 Figure 2a & b), and correspondingly, there was a modestly higher prevalence of absent or attenuated
50
51 response in the subgroup receiving Pfizer compared with Moderna (Supplemental Table 5). Data on the
52
53 Johnson and Johnson vaccination were sparse (n=18), but suggested higher prevalence of absent response
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 5 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 among fully-vaccinated patients (83.3% [95% CI: 59.1, 94.5%] without detectable response on total RBD
4
5 or RBD IgG, and 5.6% [0.8, 30.7%] attenuated IgG).
6
7
8 Limitations of the study include the modest sample size. Our assessment was performed during the early
9
10 phase of vaccine roll out, a time period during which elderly or persons with comorbidities were
11
12 prioritized. Estimates for vaccine response may improve over time as a broader patient population
13
14
receives vaccination, although 40% of our cohort was < 65 years of age indicating reasonable
15
16
17 representativeness by age of patients receiving dialysis. Antibody titers are only one way to assess
18
19 immunologic response to vaccination. We do not yet know whether a measurable antibody response
20
21 correlates with protection from infection.
22
23
24 In summary, in a well-characterized cohort of patients receiving dialysis with and without prior evidence
25
26 of infection with SARS-COV-2, more than one in five demonstrated an attenuated immune response after
27
28 vaccination with one of three vaccines granted emergency use authorization by FDA. There were
29
30 differences in responses by vaccine type that require further study. Although median IgG titers are higher
31
32 among patients with evidence of prior SARS-CoV-2 infection compared with those without, rates of
33
34 absent- or attenuated response to vaccination were similar between the two groups. These data are in line
35
36 with some recently published reports4,5, and portend the critical need for studies evaluating real-world
37
38 efficacy of vaccination in the end-stage kidney disease population and other vulnerable populations with
39
40
chronic diseases, and for trials evaluating modified schedules of vaccination.
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 6 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 Disclosures:
4
5 LC, PH, RK and PB are employed by Ascend Clinical Laboratories. GC is on the Board of Satellite
6 Healthcare, a not for profit dialysis organization. S. Anand reports Research Funding from Applied
7 Pragmatic Research Grant, from Satellite healthcare; Honoraria from American Kidney Fund; and
8
Scientific Advisor or Membership with i3C (ISN) & CENCAM. M. Montez-Rath reports Research
9
10 Funding from Sanofi. G. Block reports current employment with US Renal Care; Consultancy
11 Agreements with Kirin, Akebia, Keryx, Reata; Ownership Interest in Ardelyx, Reata; Research Funding
12 from Akebia, Ardelyx, GSK; Honoraria from Kirin, Amgen; Scientific Advisor or Membership with
13 Reata, Kirin, Ardelyx, CJASN; and Other Interests/Relationships as prior member on ESC of KDIGO,
14 prior Medical Director at Davita, and prior employment with Reata. G. Chertow reports Consultancy
15 Agreements with Akebia, Amgen, Ardelyx, Astra Zeneca, Baxter, Cricket, DiaMedica, Gilead,
16
Miromatrix, Reata, Sanifit, Unicycive, Vertex; Ownership Interest in Ardelyx, CloudCath, Durect,
17
18 DxNow, Eliaz Therapeutics, Outset, Physiowave, PuraCath; Research Funding from NIDDK, NIAID;
19 Scientific Advisor or Membership as Co-Editor of Brenner & Rector's The Kidney (Elsevier); an dOther
20 Interests/Relationships via DSMB service, NIDDK, Angion, Bayer, and ReCor. S. Boyd reports
21 Consultancy Agreements with Regeneron, Sanofi, Novartis; Ownership Interest in AbCellera, CareDx;
22 Honoraria from NIH, Karolinska Institutet; Patents and Inventions from U.S. Patent No. 9,068,224,
23 licensed to Adaptive Biotechnologies; and Scientific Advisor or Membership with Food Allergy Fund. R.
24
Kerschmann reports Consultancy Agreements with Ascend Clinical, Grail, Inc., Notable Labs, and
25
26
Octave Bioscience. M. Dittrich is employed by US Renal Care; and has Ownership Interest in US Renal
27 Care, Signify Health, and Multiple dialysis units.
28
29
30 Funding Support:
31
32 Dr. Anand was supported by R01DK127138. Dr Chertow was supported by K24DK085446. Ascend
33 Clinical Laboratory supported the remainder plasma testing for SARS-CoV2 antibodies.
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 7 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 References
4
5
6 1. Edey M, Barraclough K, Johnson DW. Review article: Hepatitis B and dialysis. Nephrology
7 (Carlton). 2010;15(2):137-145.
8 2. Broeders NE, Hombrouck A, Lemy A, et al. Influenza A/H1N1 vaccine in patients treated by
9
kidney transplant or dialysis: a cohort study. Clin J Am Soc Nephrol. 2011;6(11):2573-2578.
10
11
3. Anand S, Montez-Rath ME, Han J, et al. Serial SARS-CoV-2 Receptor-Binding Domain Antibody
12 Responses in Patients Receiving Dialysis. Ann Intern Med. 2021.
13 4. Grupper A, Sharon N, Finn T, et al. Humoral Response to the Pfizer BNT162b2 Vaccine in Patients
14 Undergoing Maintenance Hemodialysis. Clin J Am Soc Nephrol. 2021.
15 5. Attias P, Sakhi H, Rieu P, et al. Antibody response to the BNT162b2 vaccine in maintenance
16 hemodialysis patients. Kidney Int. 2021.
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 8 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 Figure 1. IgG responses following COVID19 vaccination among patients receiving dialysis
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33 In this figure, each marker represents an individual semiquantitative RBD IgG index value in the time
34 period related to vaccination. Blue circles represent persons who did not have evidence of SARS-CoV-2
35 infection prior to vaccination (seronegative); green markers represent persons who did have evidence of
36 SARS-CoV-2 infection prior to vaccination (seropositive). The overlying grey lines represent median
37
with interquartile range. We defined early post vaccination as within 14 days of first dose, partially
38
39 vaccinated as between 14 days after first dose to 14 days post second dose (applicable to mRNA vaccines
40 only), and fully vaccinated as more than 14 days post second dose for Moderna and Pfizer, or post dose
41 for Johnson and Johnson. The IgG index values assay range is from 0.5 to 150 but index values > 1 are
42 considered reactive. In the seropositive prior to vaccination cohort, the RBD IgG value closest to
43 vaccination is graphed; otherwise for both cohorts, the value most proximal to the start of each time
44 period is graphed. Although 1140 and 493 patients were included in the two cohorts (since they received
45
at least one vaccine dose at the time of the study), all patients do not have values available for each time
46
47 period, since these depend on the timing of the vaccination and the routine monthly blood draw. The
48 numbers above the figure show the numbers of persons with a result available in the seronegative and
49 seropositive cohorts for each time period.
50
51 The table below provides estimates for prevalence of no seroconversion on the total RBD Ig assay, and
52 absent (index value < 1) and attenuated (1< index value < 10) semiquantitative RBD IgG, respectively.
53
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 9 of 22
Copyright 2021 by ASN, Published Ahead of Print on 6/11/21, Accepted/Unedited Version
1
2
3 Supplemental Table of Contents
4
5
6
7 Supplemental Methods
8
9 Supplemental Table 1 Participant characteristics according to SARS-CoV-2 spike protein receptor
10 binding domain antibody status prior to vaccination
11
12 Supplemental Table 2 Prevalence of absent or attenuated response among fully vaccinated individuals
13 overall and by age group, at least 14 days after completion of vaccine
14
15 Supplemental Table 3 Prevalence of absent or attenuated response among fully vaccinated individuals
16 overall and by age group, at least 28 days after completion of vaccine
17
Supplemental Table 4 Risk factors for absent or attenuated response to SARS-CoV-2 vaccination in
18
19 fully vaccinated patients receiving dialysis
20
Supplemental Table 5 Prevalence of absent or attenuated response among fully vaccinated individuals
21
22 by vaccine type, at least 14 days after completion of vaccine*
23 Supplemental Figure 1 Study flowchart of participants
24
25 Supplemental Figure 2a&b Semiquantitative IgG values in patients receiving Moderna (a) or Pfizer (b)
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 10 of 22
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
254x190mm (96 x 96 DPI)
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60 Journal of the American Society of NephrologyPage 11 of 22
1
2
3 Antibody Response to COVID-19 vaccination in Patients on Dialysis
4
5
6
7
8
9 Table of Contents
10
11
12 Supplemental Methods p2
13
14 Supplemental Table 1 Participant characteristics according to SARS-CoV-2 spike protein receptor
15 binding domain antibody status prior to vaccination p5
16
17 Supplemental Table 2 Prevalence of absent or attenuated response among fully vaccinated individuals
18 overall and by age group, at least 14 days after completion of vaccine p7
19
20 Supplemental Table 3 Prevalence of absent or attenuated response among fully vaccinated individuals
21 overall and by age group, at least 28 days after completion of vaccine p8
22
23 Supplemental Table 4 Risk factors for absent or attenuated response to SARS-CoV-2 vaccination in
24 fully vaccinated patients receiving dialysis p9
25
26 Supplemental Table 5 Prevalence of absent or attenuated response among fully vaccinated individuals
27 by vaccine type, at least 14 days after completion of vaccine* p10
28
29 Supplemental Figure 1 Study flowchart of participants p11
30
31 Supplemental Figure 2a&b Semiquantitative IgG values in patients receiving Moderna (a) or Pfizer (b)
32
p12
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58 1
59
60 Journal of the American Society of NephrologyPage 12 of 22
1
2
3 Supplemental Methods
4
5 Our study was conducted in partnership with the dialysis network US Renal Care and Ascend Clinical
6
7 Laboratory. Ascend Clinical tested remainder plasma of patients for SARS-CoV-2 antibody, and
8
9 anonymized all patient demographic, comorbidity, and laboratory data prior to transfer to Stanford
10
11
University. The Institutional Review Board at Stanford University reviewed and approved the study.
12
13
14 Sample size
15
16
17 We selected 4,348 patients on follow from the 17,390 patients on dialysis without prior evidence of
18
19 SARS-CoV-2 infection (as of January 2021) in US Renal Care network. To estimate sample size, we used
20
21 previously published data on hepatitis B vaccination non-response, as available by age strata from
22
23 Bruguera et al.1, who evaluated immune response in 270 patients. In this study, the rate of non-response
24
25 among persons age 20-40, 40-60, and >60 years was 7%, 13%, and 35% respectively. Correspondingly,
26
27
our estimates of non-response among persons age 18-44, 45-64, ≥65 years was 5%, 15%, and 30%
28
29
30 respectively. Estimating these proportions of non-response with an absolute precision of 2%, and
31
32 oversampling by 15%, resulted in a sample size estimate of 4222 (see Table).
33
34 Population and subpopulation sizes by age and number of patients required to obtain a prevalence estimate with the specified
35 absolute precision assuming and the specified proportion of non-response to the vaccine.
36
37 Proportion of
US Renal Care Over sample
Age group non-response to Absolute precision USRDS Population count Sample size required
38 vaccine
Population size (15%)
39
18 to 44 5% 2% 60,540 2,871 453 521
40
41
45 to 64 15% 2% 207,022 10,605 1,218 1,401
42
43 ≥ 65 30% 2% 231,588 12,777 2,000 2,300
44
45 Total 499,150 26,253 3,671 4,222
46
47
48 We used systematic sampling with fractional intervals. In systematic sampling the patients are selected
49
50
from the list using a fixed selection interval, calculated by dividing the total number of patients in the list
51
52
by the desired number (i.e., 17390/4222 = 4.1). We thus randomly selected one number between 1 and 4
53
54
55 and then selected every 4th patient in the sampling frame sorted by zip code, age, sex and race. This
56
57
58 2
59
60 Journal of the American Society of NephrologyPage 13 of 22
1
2
3 resulted in a sample size of 4348 patients on dialysis; however two sampled patients seroconverted prior
4
5 to vaccination, thus we followed 4346 patients from January 2021. This cohort comprised the
6
7
seronegative prior to vaccination cohort (see Supplemental Figure 1).
8
9
10 In addition, since August 2020, we have followed 6551 patients among whom a subset seroconverted
11
12 prior to vaccination (i.e., developed evidence of natural infection). All 540 patients seropositive as of
13
14
January 2021, and any additional patients who seroconverted prior to vaccination comprised the
15
16
17 “seropositive prior to vaccination cohort” (see Supplemental Figure 1).
18
19 Assay Characteristics: We tested remainder samples using the Siemens’ total RBD Ig assay, which
20
21
measures IgG and IgM antibodies, in January 2021 and monthly thereafter in the seronegative prior to
22
23
24 vaccination cohort. This assay is reported by the manufacture to have 100% sensitivity and 99.8%
25
26 specificity for tests performed ≥14 days after a positive reverse transcriptase polymerase chain reaction
27
28 test2; it has been validated independently with similar performance characteristics3,4. Subsequent to a
29
30 positive total RBD Ig result in the seronegative and among all patients in the seropositive prior to
31
32 vaccination cohorts, we tested samples only using a semiquantitative Siemens RBD IgG assay monthly.
33
34 The Siemens RBD IgG assay is semiquantitative two-step sandwich indirect chemiluminescent assay with
35
36 a manufacturer reported 95.6% (95% CI: 92.2-97.8%) sensitivity and 99.9% (95% CI 99.6-99.9%)
37
38 specificity for tests performed ≥21 days post positive reverse transcriptase polymerase chain reaction test.
39
40
An index value ≥1.0 is considered reactive and an index value of 150 is the upper limit of quantification.
41
42
43 We classified responses as absent total RBD Ig antibody, absent semiquantitative IgG antibody (index
44
45 value 1:80 7,8. Finally, in an
55
56 external study of patients with inflammatory bowel disease on biologic therapy post SARS-CoV-2
57
58 3
59
60 Journal of the American Society of NephrologyPage 14 of 22
1
2
3 vaccination, 22 of 26 patients with inflammatory bowel disease and all 14 healthcare workers who had
4
5 completed vaccination exhibited semiquantitive titers with index values > 109.
6
7
8 Correlates: We extracted electronic health record data on age, sex, self-reported race and ethnicity, years
9
10 with end-stage kidney disease, diabetes status, and nursing home status as available. We also extracted
11
12 monthly laboratory results for serum albumin—a valid surrogate of health status10-13. We used the
13
14
laboratory value closest to the date prior to vaccination.
15
16
17 Statistical analysis: We present demographic data and laboratory values using proportions, mean ±
18
19 standard deviation (SD) or median, 25th-75th percentile, as applicable. We present the range of
20
21
semiquantitative IgG titers by vaccine period in the seronegative and seropositive prior to vaccination
22
23
24 cohorts. Among patients in the ‘fully vaccinated’ window, we present prevalence and 95% confidence
25
26 intervals, overall and by age group, of absent or attenuated antibody response in the overall, and
27
28 seronegative and seropositive prior to vaccination cohorts. Finally, we present these parameters by
29
30 vaccine type. In a sensitivity analysis, we assessed prevalence of absent or attenuated antibody response
31
32 after at least 28 days post completion of vaccination. Among participants who completed vaccination, we
33
34 used a Poisson model with robust standard error to assess risk factors for absent or attenuated antibody
35
36 response. Data missingness was low (5%), and exclusively due to missing self-reported race/ethnicity. We
37
38 therefore present results of a complete case analysis inclusive of both cohorts, in which we a priori
39
40
selected the following correlates to test: age, sex, race/ethnicity, diabetes status, vintage of ESKD, and
41
42
43 serum albumin. We considered statistical significance at Page 15 of 22
1
2
3 Supplemental Table 1 Participant characteristics according to SARS-CoV-2 spike protein receptor
4
binding domain antibody status prior to vaccination
5
6 RBD Seronegative prior to RBD Seropositive prior to
7
vaccination vaccination
8
9 N=1140 N=493
10
Age (years)
11
12 18 to 44 67 (5.9) 41 (8.3)
13 45 to 64 369 (32.3) 175 (35.5)
14 65 to 79 491 (43.1) 198 (40.2)
15
≥ 80 213 (18.7) 79 (16.0)
16
17 Gender
18 M 685 (60.1) 280 (56.8)
19 F 455 (39.9) 213 (43.2)
20
Race and Ethnicity
21
22 Hispanic 225 (19.7) 116 (23.5)
23 Non-Hispanic white 431 (37.8) 169 (34.3)
24 Non-Hispanic Black 245 (21.5) 111 (22.5)
25
26 Non-Hispanic Other 184 (16.2) 80 (16.2)
27 Missing 55 (4.8) 17 (3.5)
28 Region
29 Northeast 161 (14.1) 59 (12.0)
30
31
South 314 (27.6) 120 (24.3)
32 Midwest 194 (17.0) 85 (17.2)
33 West 471 (41.3) 229 (46.5)
34 ESKD Vintage (years)
35Page 16 of 22
1
2
3 Moderna 716 (62.8) 341 (69.2)
4
Pfizer-BNT 390 (34.2) 131 (26.6)
5
6 Johnson & Johnson 34 (3.0) 21 (4.2)
7
8 RBD-receptor binding domain, ESKD-end-stage kidney disease
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58 6
59
60 Journal of the American Society of NephrologyPage 17 of 22
1
2
3 Supplemental Table 2 Prevalence of absent or attenuated response among fully vaccinated individuals overall and by age group, at least 14 days
4
after completion of vaccine*
5
6 Seronegative prior to vaccination cohort Seropositive prior to vaccination
7
8 N=519 N=91
9
10 No seroconversion on No detectable response on No detectable response on
11
Attenuated IgG Attenuated IgG
total RBD Ig RBD IgG RBD IgG
12
13 Age (years)
14 18 to 44 9.1% (2.8, 30) 0% (0, 0) 4.5% (0.6, 26.2) 0% (0, 0) 0% (0, 0)
15
45 to 64 6.8% (3.5, 13.1) 0.9% (0.1, 5.8) 9.4% (5.3, 16.2) 5.6% (0.8, 31.2) 5.6% (0.8, 31.2)
16
17 65 to 79 5.5% (3.2, 9.3) 3.8% (2.0, 7.2) 16.5% (12.3, 21.8) 8.3% (3.1, 20.4) 12.5% (5.7, 25.4)
18 ≥ 80 2.8% (1.0, 7.2) 2.8% (1.0, 7.2) 18.1% (12.6, 25.2) 8.7% (2.1,29.3) 13.0% (4.2, 33.9)
19 Overall 5.2% (3.6. 7.5) 2.7% (1.6, 4.5) 14.8% (12.0, 18.2) 7.7% (3.7, 15.4) 11.9% (6.0, 19.2)
20
21 *Data are percentage (95% CI) obtained at least 14 days after two doses of either Moderna or Pfizer-BNT vaccines and 14 days after a single dose
22 of Johnson & Johnson vaccine. Median duration since completion of vaccination was 29 days [25th, 75th percentile: 22, 39 days]. We performed
23
total RBD Ig among all patients in the seronegative prior to vaccination cohort; once a patient seroconverted, we performed the semiquantitative
24
25 RBD IgG monthly. We performed semiquantitative RBG IgG only among patients known to have a positive total RBD Ig prior to vaccination
26 (seropositive prior to vaccination cohort).
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43 7
44
45 Journal of the American Society of Nephrology
46
47Page 18 of 22
1
2
3
4
5 Supplemental Table 3 Prevalence of absent or attenuated response among fully vaccinated individuals overall and by age group, at least 28 days
6 after completion of vaccine*
7
8 Seronegative prior to vaccination cohort Seropositive prior to vaccination
9
10 N=355 N=48
11
12 No seroconversion on No detectable response on No detectable response on
Attenuated IgG Attenuated IgG
13 total RBD Ig RBD IgG RBD IgG
14
15 Age (years)
16 18 to 44 7.1% (1, 37.2) 0% (0, 0) 0% (0, 0) 0% (0, 0) 0% (0, 0)
17 45 to 64 1.4% (0.2, 9) 0% (0, 0) 14.9% (8.4, 24.9) 0% (0, 0) 10% (1.3, 48.1)
18 65 to 79 3.8% (1.7, 8.2) 3.1% (1.3, 7.4) 24.5% (18.4, 31.8) 13% (4.1, 34.3) 17.4% (6.5, 38.9)
19
20 ≥ 80 1.9% (0.5, 7.1) 4.6% (1.9, 10.7) 25.0% (17.7, 34.0) 0% (0, 0) 14.3% (3.5, 43.7)
21 Overall 2.5% (1.3, 4.6) 3.2% (1.9, 5.5) 20.8% (17.1, 25.1) 6.3% (2.0, 18.1) 14.6% (7.0, 28.0)
22
23 *Data are percentage (95% CI) obtained at least 28 days after two full doses of either Moderna or Pfizer-BNT vaccines and 28 days after a single
24 dose of Johnson & Johnson vaccine. We performed total RBD Ig among all patients in the seronegative prior to vaccination cohort; once a patient
25 seroconverted, we performed the semiquantitative RBD IgG monthly. We performed semiquantitative RBG IgG only among patients known to
26 have a positive total RBD Ig prior to vaccination (seropositive prior to vaccination cohort). Among both cohorts the prevalence of no
27
seroconversion on total RBD Ig, no detectable response on RBD IgG and attenuated IgG was 2.8% (1.5, 5.2), 2.8% (1.5, 5.2) and 72.7 (67.8, 77.1)
28
29
respectively.
30
31
32
33
34
35
36
37
38
39
40
41
42
43 8
44
45 Journal of the American Society of Nephrology
46
47Page 19 of 22
1
2
3 Supplemental Table 4 Risk factors for absent or attenuated response to SARS-CoV-2 vaccination in fully vaccinated patients receiving dialysis
4
5 Risk Ratio^
6
Age (years)
7
8Page 20 of 22
Supplemental Table 5 Prevalence of absent or attenuated response among fully vaccinated individuals by vaccine type,
1
at least 14 days after completion of vaccine*
2
3 Fully vaccinated
4
5 N=610
6
7 No detectable
8 response on total RBD Attenuated IgG
9 or RBD IgG
10
11 Moderna 353 2.8% (1.5, 5.2) 9.1% (6.5, 12.5)
12 Pfizer-BNT 239 9.6% (6.5, 14.1) 22.6% (17.7, 28.3)
13 Johnson & Johnson 18 83.3% (59.1, 94.5) 5.6% (0.8, 30.7)
14
15
16
17 *Data are percentage (95% CI) obtained at least 14 days after two full doses of either Moderna or Pfizer-BNT vaccines
18 and 14 days after a single dose of Johnson & Johnson vaccine. We performed total RBD Ig among all patients in the
19 seronegative prior to vaccination cohort; once a patient seroconverted, we performed the semiquantitative RBD IgG
20 monthly. We performed semiquantitative RBG IgG only among patients known to have a positive total RBD Ig prior to
21
22
vaccination (seropositive prior to vaccination cohort).
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58 10
59
60 Journal of the American Society of NephrologyPage 21 of 22
Supplemental Figure 1 Study flowchart of participants
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
*Seroconversion between August to January
49
^Semiquantitative IgG titer 14 days post second dose
50
51
52
53
54
55
56
57
58 11
59
60 Journal of the American Society of NephrologyPage 22 of 22 1 2 Supplemental Figure 2a&b: Semiquantitative IgG values in patients receiving Moderna (a) or Pfizer-BNT (b) 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 12 44 45 Journal of the American Society of Nephrology 46 47
Page 23 of 22
References
1
2 1. Bruguera M, Rodicio JL, Alcazar JM, Oliver A, Del Rio G, Esteban-Mur R. Effects of different dose levels and
3 vaccination schedules on immune response to a recombinant DNA hepatitis B vaccine in haemodialysis patients.
4 Vaccine. 1990;8 Suppl:S47-49; discussion S60-42.
5 2. U.S. Food & Drug Administration. EUA Authorized Serology Test Performance. https://wwwfdagov/medical-
6 devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/eua-authorized-
7 serology-test-performance. 2020;Date Last Accessed: March 18 2021.
8
3. Schnurra C, Reiners N, Biemann R, Kaiser T, Trawinski H, Jassoy C. Comparison of the diagnostic sensitivity of
9
SARS-CoV-2 nucleoprotein and glycoprotein-based antibody tests. J Clin Virol. 2020;129:104544.
10
4. Public Health England. Evaluation of sensitivity and specificity of 4 commercially available SARS-CoV-2
11
12 antibody immunoassays. https://wwwgovuk/government/publications/covid-19-head-to-head-laboratory-
13 evaluation-of-4-commercial-serological-assays. 2020;Date Last Accessed: July 8 2020.
14 5. Anand S, Montez-Rath, M., Han, J., Garcia, P. Serial SARS-CoV-2 Receptor Binding Domain Antibody
15 Responses in Patients on Dialysis. Annals of Internal Medicine. 2021;In press.
16 6. Legros V, Denolly S, Vogrig M, et al. A longitudinal study of SARS-CoV-2 infected patients shows high
17 correlation between neutralizing antibodies and COVID-19 severity. medRxiv. 2020:2020.2008.2027.20182493.
18 7. Lee WT, Girardin RC, Dupuis AP, et al. Neutralizing Antibody Responses in COVID-19 Convalescent Sera. J
19 Infect Dis. 2021;223(1):47-55.
20 8. Addetia A, Crawford KH, Dingens A, et al. Neutralizing antibodies correlate with protection from SARS-CoV-2
21 in humans during a fishery vessel outbreak with high attack rate. medRxiv. 2020.
22 9. Wong SY, Dixon R, Pazos VM, et al. Serological response to mRNA COVID-19 vaccines in IBD patients
23 receiving biological therapies. Gastroenterology. 2021.
24 10. Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables
25 and an evaluation of death rate differences between facilities. Am J Kidney Dis. 1990;15(5):458-482.
26 11. Rocco MV, Soucie JM, Reboussin DM, McClellan WM. Risk factors for hospital utilization in chronic dialysis
27 patients. Southeastern Kidney Council (Network 6). J Am Soc Nephrol. 1996;7(6):889-896.
28
12. Iseki K, Kawazoe N, Fukiyama K. Serum albumin is a strong predictor of death in chronic dialysis patients.
29
Kidney Int. 1993;44(1):115-119.
30
31
13. Xia H, Ebben J, Ma JZ, Collins AJ. Hematocrit levels and hospitalization risks in hemodialysis patients. J Am Soc
32 Nephrol. 1999;10(6):1309-1316.
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58 13
59
60 Journal of the American Society of NephrologyYou can also read