Applications of indocyanine green in brain tumor surgery: review of clinical evidence and emerging technologies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NEUROSURGICAL
FOCUS Neurosurg Focus 50 (1):E4, 2021
Applications of indocyanine green in brain tumor surgery:
review of clinical evidence and emerging technologies
*Clare W. Teng, BA,1,2 Vincent Huang, BA,1,2 Gabriel R. Arguelles, BA,1,2 Cecilia Zhou, BS,1,2
Steve S. Cho, MD, MTR,1 Stefan Harmsen, PhD,1 and John Y. K. Lee, MD, MSCE1
1
Department of Neurosurgery, Hospital of the University of Pennsylvania, Philadelphia; and 2Perelman School of Medicine,
University of Pennsylvania, Philadelphia, Pennsylvania
Indocyanine green (ICG) is a water-soluble dye that was approved by the FDA for biomedical purposes in 1956. Initially
used to measure cardiocirculatory and hepatic functions, ICG’s fluorescent properties in the near-infrared (NIR) spec-
trum soon led to its application in ophthalmic angiography. In the early 2000s, ICG was formally introduced in neurosur-
gery as an angiographic tool. In 2016, the authors’ group pioneered a novel technique with ICG named second-window
ICG (SWIG), which involves infusion of a high dose of ICG (5.0 mg/kg) in patients 24 hours prior to surgery. To date,
applications of SWIG have been reported in patients with high-grade gliomas, meningiomas, brain metastases, pituitary
adenomas, craniopharyngiomas, chordomas, and pinealomas.
The applications of ICG have clearly expanded rapidly across different specialties since its initial development. As an
NIR fluorophore, ICG has advantages over other FDA-approved fluorophores, all of which are currently in the visible-light
spectrum, because of NIR fluorescence’s increased tissue penetration and decreased autofluorescence. Recently, inter-
est in the latest applications of ICG in brain tumor surgery has grown beyond its role as an NIR fluorophore, extending
into shortwave infrared imaging and integration into nanotechnology. This review aims to summarize reported clinical
studies on ICG fluorescence–guided surgery of intracranial tumors, as well as to provide an overview of the literature on
emerging technologies related to the utility of ICG in neuro-oncological surgeries, including the following aspects: 1) ICG
fluorescence in the NIR-II window; 2) ICG for photoacoustic imaging; and 3) ICG nanoparticles for combined diagnostic
imaging and therapy (theranostic) applications.
https://thejns.org/doi/abs/10.3171/2020.10.FOCUS20782
KEYWORDS indocyanine green; fluorescence-guided surgery; brain tumor; NIR-II window; photoacoustic imaging;
theranostics
I
ndocyanine green (ICG), a tricarbocyanine, is a water- et al., and it has since become a popular tool in vascular
soluble dye originally developed by Kodak Research neurosurgery for intraoperative evaluation of aneurysms,
Laboratories for near-infrared (NIR) photography in arteriovenous malformations, and cortical perfusion3 (for
1955. Biomedical applications of ICG began in 1956, when the ICG timeline see Fig. 1).
it received FDA approval for diagnostic use in determin- The use of ICG in brain tumor surgery, in contrast,
ing cardiocirculatory and hepatic functions.1 Whereas has remained at modest levels in clinical practice over the
early studies focused on tracking ICG levels in the serum, years. As early as 1996, Haglund et al. had described en-
discovery of ICG’s fluorescent properties in the 1970s ex- hanced optical imaging by using ICG in 9 patients under-
panded its use to ophthalmic angiography. This develop- going resection of high-grade gliomas (HGGs).4 Fluores-
ment truly revealed the potential of ICG to provide visual cence-guided surgery (FGS) of brain tumors only began
guidance in anatomical structures during surgical proce- to accrue more interest in the early 2000s, culminating
dures, which built a foundation for image-guided surgery.2 in a phase III trial by Stummer et al. demonstrating im-
In 2003, ICG was formally introduced in neurosurgery as proved progression-free survival in patients with malig-
an angiographic agent with a landmark study by Raabe nant glioma treated with 5-aminolevulinic acid (5-ALA)
ABBREVIATIONS 5-ALA = 5-aminolevulinic acid; BBB = blood-brain barrier; DOX = doxorubicin; EPR = enhanced permeability and retention; FGS = fluorescence-guided
surgery; GBM = glioblastoma; GTR = gross-total resection; HGG = high-grade glioma; ICG = indocyanine green; NIR = near infrared; PAI = photoacoustic imaging; PDT
= photodynamic therapy; PTT = photothermal therapy; SBR = signal-to-background ratio; SPIO = superparamagnetic iron oxide; SPION = SPIO nanoparticle; SWIG =
second-window ICG; SWIR = shortwave infrared.
SUBMITTED September 1, 2020. ACCEPTED October 23, 2020.
INCLUDE WHEN CITING DOI: 10.3171/2020.10.FOCUS20782.
* V.H. and G.R.A. contributed equally to this work.
©AANS 2021, except where prohibited by US copyright law Neurosurg Focus Volume 50 • January 2021 1
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
FIG. 1. Milestones of ICG for brain tumor surgery.
FGS.5 This led to a revival of interest in ICG as an op- illumination, due to existing capability in real-time over-
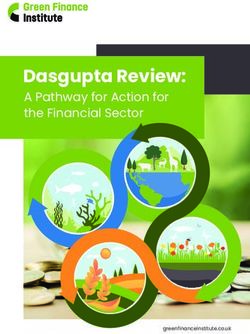
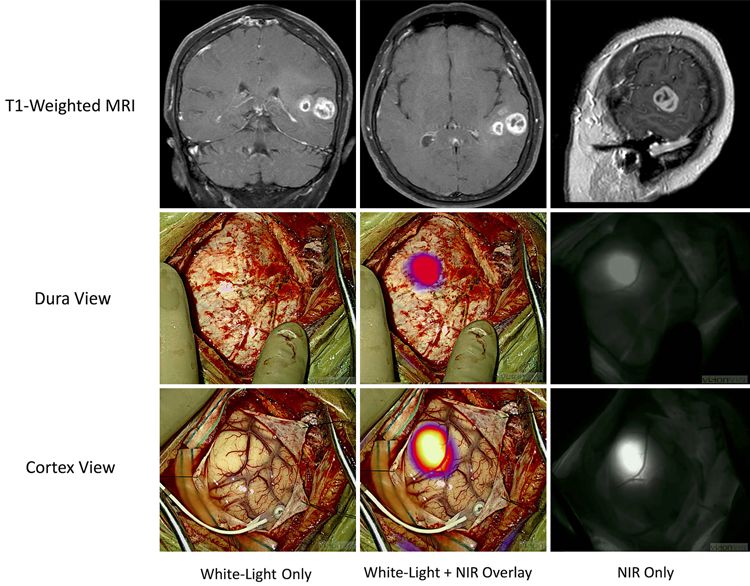
tical imaging agent. A breakthrough took place in 2012, lay with both visible light and NIR fluorescence15 (Fig.
when Madajewski et al. proposed that administration of 2). SWIG was first used to visualize gliomas in 2016.
high-dose ICG (7.5 mg/kg) 24 hours before surgery al- This study and subsequent reports in skull base tumors
lowed residual neoplasm detection in murine flank tu- found that Gd enhancement on T1-weighted MRI was
mors.6 From this principle, our group pioneered a novel the strongest predictor of positive fluorescence, whereas
technique named second-window ICG (SWIG), in which nonenhancing tumors did not fluoresce, providing insight
high-dose ICG (5 mg/kg) is administered 24 hours prior into the mechanism of ICG localization.7,16 In 2012, Er-
to intraoperative imaging. In 2016, we conducted the first- gin et al. had proposed using intravenous ICG injections
in-human study, which demonstrated significant NIR con- to optically monitor blood-brain barrier (BBB) disrup-
trast in Gd-enhancing gliomas in the operating room.7 To tion, taking advantage of the same EPR effect proposed
date, applications of SWIG have been reported in HGGs, to underpin ICG accumulation in the tumor microenvi-
meningiomas, brain metastases, pituitary adenomas, cra- ronment.17 In the initial SWIG study from 2016, findings
niopharyngiomas, chordomas, and pinealomas.8–10 in patients with contrast-enhancing gliomas (12/15) were
ICG remains the first and only FDA-approved NIR used to calculate diagnostic test characteristics. Using tu-
fluorophore. After intravenous administration, this small, mor pathology as the gold standard, SWIG demonstrated
amphiphilic molecule rapidly binds to albumin and other higher sensitivity and a negative predictive value but lower
plasma proteins.11 ICG is almost exclusively metabolized specificity and a positive predictive value compared with
by the liver and excreted into bile, with a mean initial de- visualization under white light; these test characteristics
cay rate of 18.5% per minute in healthy individuals.12 ICG were later corroborated in intracranial metastases, menin-
fluorescence is excited by 778- to 806-nm light, with a giomas, and pituitary adenomas.18–20 Enhanced sensitivity
peak emission of 835 nm in biological tissues. NIR fluo- and a negative predictive value may give neurosurgeons
rescent emission of ICG can penetrate tissue up to 15 mm, more confidence in detecting remaining neoplastic tissue
compared with 3 mm for visible-light fluorophores.13 Be- and thus facilitating gross-total resection (GTR).
sides, ICG suffers from less tissue autofluorescence be- Establishing the novel clinical utility of ICG set the
cause it operates in the NIR spectrum, in which biological stage for studies in other brain tumor types. In 2018, ICG
tissue mostly does not demonstrate fluorescence.
was used to successfully localize tumors displaying a high
The tumor-targeting mechanism behind SWIG is
known as the enhanced permeability and retention (EPR) signal-to-background ratio (SBR) in 14/18 patients with
effect, which stipulates that vascular permeability around meningioma.19 In the remaining minority of patients, the
solid tumors is pathologically enhanced due to structural surrounding brain parenchyma displayed a higher NIR
breakdown, impaired lymphatic drainage, and increased signal than the tumor, an interesting phenomenon cur-
permeability mediators.14 rently only seen in meningiomas. We hypothesized that
Lately, the application of ICG in brain tumor surgery this phenomenon of signal inversion may be due to auto-
has been extended beyond its role as simply an NIR fluo- quenching of ICG that can occur at high concentrations.21
rophore. This turning point has been fueled by two key At approximately the same time, ICG was demonstrated
developments: the investigation of the shortwave infrared to localize intraparenchymal metastases in 13 patients
(SWIR) window and the rapid growth of nanotechnology. with primary pathologies that included melanoma, lung,
In this review, we provide an overview of the clinical stud- breast, colon, ovarian, and renal cancers.18
ies on ICG FGS of intracranial tumors conducted by our Of note, melanoma metastases had the lowest mean
group and others (Table 1). We then summarize the lit- SBR at 3.65, which is attributed to melanin’s absorption of
erature on emerging technologies and their implications light, compared with a mean SBR of 7.2 for other metas-
for the potential utility of ICG in neuro-oncological pro- tases. This observation was also corroborated by updated
cedures. data in progress for publication. Other studies have dem-
onstrated ICG’s ability to visualize chordoma, craniopha-
Clinical Trials of ICG for Fluorescence- ryngioma, pineocytoma, and intraventricular tumors.16,22,23
Because the ultimate goal of FGS is to maximize ex-
Guided Intracranial Tumor Surgery tent of resection, studies by Cho et al. in 202024 and Teng
ICG visualization can be accomplished without dis- et al.76 comparing NIR fluorescence to the gold stan-
rupting the surgeon’s usual workflow under white-light dard postoperative MRI showed that the absence of re-
2 Neurosurg Focus Volume 50 • January 2021
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
TABLE 1. Summary of clinical studies of ICG application in brain tumors
Authors & Year Tumor or Structure Key Findings
Lee et al., 2016 7
Glioma Mean SBR of 9.5 w/ 5.0 mg/kg SWIG in 12 pts w/ Gd-enhancing tumors, deepest tumor visualized was
13 mm from dural surface, Gd enhancement on MRI correlates to SBR (p = 0.03)
Ferroli et al., Glioma 25 mg ICG video angiography in 54 HGGs, 17 LGGs, 14 meningiomas, 12 metastases, & 3 hemangio-
20118 blastomas can monitor blood flow in exposed tumoral & peritumoral vessels
Zeh et al., 20179 HGG Mean SBR of 7.5 w/ 2.5–5.0 mg/kg SWIG in 10 pts, plateau of ICG NIRF up to 48 hrs postinfusion
Cho et al., 202024 Newly diagnosed Mean SBR of 6.8 w/ 2.5–5.0 mg/kg SWIG in 36 pts, 90% (27/30) of tumors ≤15 mm from dural surface
HGG were visualized, clean final NIR view correlated to GTR on postop MRI (p < 0.0001)
Lee et al., 201819 Meningioma Mean SBR of 5.6 w/ 5.0 mg/kg SWIG in 14/18 pts; 4/18 pts demonstrated “inversion” in which immediate
parenchyma had higher SBR than the tumor
Kim et al., 201925 Meningioma 12.5 mg ICG video angiography in 42 pts allows real-time monitoring of peritumoral blood flow, detection
of collateral venous circulation, & flow restoration
Lee et al., 201718 Metastases Mean SBR of 6.62 w/ 5.0 mg/kg SWIG in 13 pts, melanoma metastases had lower SBR signal, deepest
tumor visualized was 7 mm from dural surface
Teng et al., in Metastases Mean SBR of 4.9 w/ 2.5–5.0 mg/kg SWIG in 47 pts, melanoma metastases had lower SBR signal, clean
press76 final NIR view correlated to GTR on postop MRI (p = 0.007)
Jeon et al., 201916 Skull base tumors Mean SBR of 3.9 w/ 5.0 mg/kg SWIG in 8 pituitary adenomas, mean SBR of 4.1 in 3 craniopharyngio-
mas, mean SBR of 2.1 in 4 chordomas, Gd enhancement on MRI correlates to SBR (p = 0.0003)
Hide et al., 201526 Skull base tumors 12.5 mg ICG video angiography in 26 pituitary adenomas, 4 tuberculum sellae meningiomas, 3 cranio-
pharyngiomas, 2 chordomas, 1 Rathke cleft cyst, 1 dermoid cyst, & 1 fibrous dysplasia strongly labels
landmark blood vessels in real time
Amano et al., Skull base tumors 6.25–12.5 mg ICG video angiography in 15 pituitary adenomas, 3 Rathke cleft cysts, 1 meningioma, & 1
201927 pituicytoma can differentiate tumor margin & define local vessel structure
Sandow et al., Skull base tumors 25 mg ICG video angiography in 22 pituitary adenomas can either directly visualize tumor fluorescence
201510 or indirectly detect tumor w/ higher background fluorescence
Cho et al., 202022 Pineocytoma SBR of 2.9 w/ 5.0 mg/kg SWIG in 1 pt
Cho et al., 202031 Pituitary stalk 2.5 mg/kg SWIG allows for visualization of normal pituitary stalk despite distorted anatomy in 1 pt w/
pituitary macroadenoma
Hitti & Lee, 201823 Intraventricular tumor SWIG localizes to both normal choroid plexus & choroid plexus papilloma for endoscopic resection in 1 pt
Hojo et al., 201428 Hemangioblastoma 8–12.5 mg ICG video angiography in 12 pts facilitates preresection visualization of tumor & feeder arter-
ies, & postresection confirmation of total resection & normal blood flow
HGG = high-grade glioma; LGG = low-grade glioma; NIRF = near-infrared fluorescence; pt = patient.
sidual NIR signal postresection closely correlated to GTR ernous sinus with high resolution.26 Monitoring of these
of HGGs (p < 0.0001) and intracranial metastases (p = vessels and perforators may contribute to preservation of
0.007) on MRI. One limitation of these findings, however, optic nerve and pituitary function. ICG video angiogra-
is intrinsic to the SWIG technique itself. Although ICG phy also distinguished pituitary adenomas from normal
is FDA approved, its current dosage of 2.5–5.0 mg/kg in pituitary through differential timelines for peak fluores-
SWIG clinical trials exceeds the 2.0 mg/kg limit. Nev- cence intensities. For example, nonfunctioning pituitary
ertheless, Haglund et al. and unpublished data from our adenomas were best visualized 7 minutes postinjection,
group suggest that doses approaching 2.0 mg/kg can still whereas normal pituitary was best visualized 15 minutes
localize HGGs, meningiomas, and metastases with accu- postinjection and onward.27 Finally, as a highly vascular-
racy intraoperatively4 and could also be used to predict ized tumor, hemangioblastoma can be directly visualized
GTR on postoperative MRI for HGGs and metastases. by ICG when used in an angiographic capacity. Preresec-
In addition to SWIG, ICG can also be used for its more tion ICG video angiography allowed for visualization of
conventional role as an angiography agent in brain tumor hemangioblastoma in all patients (8/8), whereas postresec-
surgeries. Kim et al. showed that ICG can identify small tion video angiography confirmed complete resection in
peritumoral blood vessels in patients with intracranial all patients (10/10).28
meningiomas.25 Its advantage over the standard microvas- Furthermore, because 5-ALA is a more established
cular Doppler sonography is an ability to image vessels agent in the field of FGS, Cho et al.29 performed coadmin-
with less blood flow or smaller diameter. Similarly, ICG istration of 5-ALA and ICG in 4 patients with HGGs to
video angiography has extensive utility for resection of pi- benchmark the comparative performance of ICG. The two
tuitary tumors. ICG video angiography during endoscopic agents were found to have 90% concordant distributions
endonasal transsphenoidal surgery can orient surgeons to and similar diagnostic accuracies, whereas tumor-associ-
the internal carotid artery, intercavernous sinus, and cav- ated necrosis demonstrated the most distinct difference,
Neurosurg Focus Volume 50 • January 2021 3
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
FIG. 2. FGS performed using SWIG. Demonstration of SWIG in a patient with a Gd contrast–enhancing GBM on preoperative T1-
weighted MRI. Transdural visualization is achieved, assisting neurosurgeons to better plan tumor access. The GBM demonstrates
strong NIR fluorescence in the operating room after durotomy.
showing weak or no protoporphyrin-IX fluorescence but immunogenic responses, and hence are subjected to con-
strong SWIG fluorescence.29 Another comparison study siderable regulatory hurdles prior to clinical translation.
demonstrated that ICG was superior to 5-ALA in visual- In 2018, Carr et al.35 first demonstrated that ICG, with an
izing areas of increased angiogenesis, a process essential emission spectra peak in NIR-I, has an off-peak > 1000-
for metastasis of solid tumors.30 nm tail emission. Specifically, high-contrast mesoscopic
Finally, ICG has applications in tumor surgeries when imaging of the brain vasculature was demonstrated in
not used to directly localize the tumor. Because it lacks a mice through intact skin by using ICG (0.2 mg/kg) in the
BBB, the normal pituitary stalk has been observed to up- NIR-II window (excitation 808 nm, emission 1300–1620
take ICG and fluoresce, allowing identification and pres- nm).35 Starosolski et al. had made a similar observation
ervation of the structure in complex skull base surgeries.31 independently both in vitro and in vivo.36 Subsequently,
Hu et al. reported the first-in-human application of NIR-II
ICG in the NIR-II Window imaging using ICG in 23 patients undergoing resection of
One of the most promising advances in optical imag- hepatic neoplasms. Compared with NIR-I imaging, NIR-
ing research is the discovery of the SWIR/NIR-II window, II imaging exhibited higher tumor detection sensitivity
broadly defined as wavelengths in the range of 1000–2000 (100% vs 90.6%) and SBR (5.33 vs 1.45).37 To date, no
nm. Whereas fluorophores in the NIR region (i.e., NIR- clinical trials have been conducted on NIR-II imaging us-
I; 700–900 nm) generally demonstrate favorable SBR ing ICG in neurosurgery.
and penetration depth when compared with visible-light It has been acknowledged that ICG offers an unprec-
probes (400–700 nm), the SWIR window is characterized edented opportunity for the clinical translation of NIR-II
by an up to 1000-fold reduction in photon scattering and imaging technology.32,38 However, its major limitations in-
the potential to offer micron-scale imaging resolution and clude relatively low photon utilization because NIR-II is
centimeters of penetration depth, making it a powerful only the tail portion of the emission spectrum, as well as
technique for the prospect of image-guided surgery.32 the nonspecific targeting mechanism of the EPR effect;39
Until recently, SWIR fluorophores had consisted en- hence, researchers continue to identify strategies to im-
tirely of semiconducting inorganic nanomaterials (e.g., prove characteristics of NIR-II imaging probes, such as
single-walled carbon nanotubes, quantum dots, and rare synthesizing organic small molecules with a rapid excre-
earth–doped nanoparticles).33,34 Despite respectable results tion profile and higher imaging quality compared with
in preclinical studies, these agents raise safety concerns free ICG,40 and conjugating ICG to antibodies targeting
due to retention in the liver and/or spleen and potential overexpressed receptors on cancer cells.41
4 Neurosurg Focus Volume 50 • January 2021
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTABLE 2. ICG nanoparticles for image-guided therapy in brain tumors
Authors & Year NP Diameter (nm) Cell Line Model Tumor Site Imaging Therapy Targeting Mechanism
Shibata et al., Liposomally formulated phospholipid-conju- 191 9L gliosarcoma Nude rats Rt hemisphere NIRF PDT EPR
201959 gated ICG (LP-iDOPE) cells of brain
Hao et al., Angiopep-2 modified PLGA/DTX/ICG NPs 221.7 ± 1.6 U87MG cells Nude mice Rt frontal lobe NIRF PDT + PTT Low-density lipoprotein recep-
201563 (ANG/PLGA/DTX/ICG NPs) of brain + chemo tor–related protein-1 (LRP1)
Hu et al., ICG/SN38 NP (self-assembly w/ π-π stacking 35–60 U87MG cells Nude mice Rt flank NIRF PDT + EPR
202060 & hydrophobic interactions) chemo
Huang et al., CaCO3/TPGS NPs delivering ICG, PDA, & 180 U87MG cells Nude mice Back NIRF PDT + PTT Integrin αvβ3
2019 62 TPZ (ICG-PDA-TPZ NPs) + chemo
Liu et al., c(RGDfk)-modified glycolipid-like micelles 93.5 ± 1.4 U87MG cells Nude mice Rt flank NIRF PDT + PTT Dual targeting of tumor &
201964 encapsulating ICG (cRGD-CSOSA/ICG) neovascular endothelial cells
Yang et al., Catalase-integrated-albumin phototheranostic 78.8 U87MG cells Nude mice Rt armpit/hind leg & NIRF, PA, IR PDT + PTT EPR & SPARC-mediated
202050 nanoprobe (ICG/AuNR@BCNP) rt striatum of brain thermal imaging albumin-based active targeting
Zhu et al., Holo-transferrin–based nanoassembly 12 U87MG cells Nude mice Rt flank & rt hemi- NIRF, PA, IR PTT Transferrin receptor (TfR)
201748 encapsulating ICG (holo-Tf-ICG) sphere of brain thermal imaging
Jia et al., Biomimetic ICG-loaded liposome 104 C6-Luc glioma Nude mice Hind paw & brain NIRF PTT Homotypic targeting
201971 (BLIPO-ICG) NPs cells striatum
Xu et al., ICG encapsulated in silk fibroin nanoparticles 209.4 ± 1.4 C6 glioma cells Nude mice Rt flank NIRF PTT EPR
201870 (ICG-SFNPs)
Maziukiewicz Nanodiamonds (NDs) conjugated w/ 357.6 ± 8.6 U118MG cells NA NA NIRF PTT EPR
et al., 201969 biomimetic PDA & ICG (NDs@PDA@ICG)
Gao et al., RGD peptide–modified bisulfite-zincII- 7 U87MG cells Nude mice Rt hemisphere NIRF PTT Integrin αvβ3/αvβ5
202072 dipicolylamine-Arg-Gly-Asp (Bis(DPA-Zn)- of brain
RGD) & ultrasmall Au-ICG NPs (R-Au-ICG)
Shen et al., Coating hydrophobic SPIO core w/ 22.9 C6 glioma cells Nude mice Rt hemisphere NIRF, MRI Chemo EPR
201875 DSPE-PEG2000 & hydrophobic DOX & Wistar of brain
followed by ICG loading into lipid shell rats
layers (SPIO@DSPE-PEG/DOX/ICG NPs)
Kwon et al., TMZ- & ICG-loaded Fe3O4 magnetic NPs (i.e., 159.5 ± 34.2 U87MG cells NA NA NIRF Chemo + EPR
2019 68 Fe3O4‑TMZ‑ICG MNPs) PTT
Chemo = chemotherapy; IR = infrared; MG = malignant glioma; NA = not applicable; NP = nanoparticle; PDA = polydopamine; SN38 = 7-ethyl-10-hydroxycamptothecin; SPARC = secreted protein acidic and rich in cys-
teine; TMZ = temozolomide; TPZ = tirapazamine.
Neurosurg Focus Volume 50 • January 2021
5
Teng et al.
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
In neurosurgery, Byrd et al. recently reported the first acoustic imaging, to image orthotopic glioma models.48 At
NIR-II ICG angiography study in a large animal, demon- 24 hours postinjection of the imaging agent, PAI of ICG-
strating higher spatial and contrast resolutions throughout holo-transferrin nanoassemblies achieved high spatial res-
the dynamic sequence of the pig intracranial vasculature, olution and a PAI signal in the tumor region 10-fold higher
particularly in the smallest vessels.42 The application of than that at the preinjection time point. In 2018, Liu et al.
NIR-II imaging in brain tumor surgery has been explored demonstrated the ability of ICG to improve the imaging
in preclinical studies. Namely, Kurbegovic et al. per- depth of an existing PAI contrast agent in an orthotopic
formed FGS on orthotopic glioblastoma (GBM)–bearing brain glioma.49 Molybdenum disulfide nanosheets loaded
nude mice by using a targeted NIR-II fluorescent probe with ICG achieved a 3.5-mm imaging depth at 800 nm,
consisting of an in-house synthesized NIR-II fluorophore which was 2-fold deeper than with molybdenum disulfide
(CH1055) and a uPAR-targeting peptide (AE105).43 Al- alone. Most recently, in 2020, Yang et al. demonstrated an
though NIR-II imaging with free ICG applied in brain tu- SBR of 6.6 at 3.1 mm of depth 4 hours postinjection using
mor surgery has not been reported in either preclinical or a biomimetic catalase-integrated-albumin phototheranos-
clinical studies, it may represent an important forthcoming tic nanoprobe with simultaneous encapsulation of ICG and
opportunity in image-guided neurosurgery. gold nanoparticles.50
Therefore, ICG has been successfully used for PAI of
brain tumors in animal models. Its ability to increase reso-
ICG for Photoacoustic Imaging lution and depth of penetration over optical imaging make
Photoacoustic imaging (PAI) for use in image-guided it a promising imaging modality.
surgery has recently been investigated as a means to im-
prove intraoperative visualization and resection of brain
tumors. Also known as optoacoustic imaging, PAI is a hy-
ICG Nanoparticles: Transition to
brid imaging modality that combines the strong contrast Theranostics
of optical imaging with the high spatial resolution of ultra- Theranostics combines diagnostic imaging and therapy.
sound.44 The principle underlying PAI—the photoacous- Much of the development in this emerging field is powered
tic effect—occurs when molecules interact with photons. by the recent advances in nanotechnology, which have en-
Optical absorption results in thermoelastic expansion, cre- abled flexible synthesis of multimodal nanoparticles. Late-
ating pressure perturbations that propagate as ultrasound ly, the favorable imaging/biological characteristics of ICG
waves. These waves are detected by an array of ultrasound as an NIR fluorophore have garnered interest in the incor-
transducers, which then construct an image that represents poration of ICG into nanoparticles for the development of
the initial photoacoustic pressure distribution based on the cancer theranostic tools. Theranostic nanomedicine is still
ultrasound waves’ amplitudes and arrival times.45 PAI sys- in its infancy, primarily confined to academic settings and
tems for use in image-guided surgery consist of a source of with few early-stage clinical studies.51 In this section, we
nonionizing light, usually in the form of a pulsating laser, review the synthesis and application of ICG nanoparticles
and an array of ultrasound transducers.44 in brain tumors and summarize several major therapeutic
PAI has the capability to provide higher resolution at modalities that have been explored (Table 2).
increased penetration depths when compared with NIR
fluorescence imaging, which is due to the decreased scat- Photodynamic Therapy
tering of ultrasound waves compared with optical sig- Photodynamic therapy (PDT) uses a photosensitizer,
nals.44 Importantly, PAI can use exogenous dyes such as which upon excitation by light produces reactive oxygen
ICG, leveraging the decreased background signal inherent species that are cytotoxic to selected cells. Several pho-
to NIR dyes to provide high tumor contrast. In studies in tosensitizers have been approved by the FDA; these in-
which brain and nonbrain tumors have been imaged, ICG clude porfimer sodium (Photofrin) for esophageal cancer
has been combined with other contrast agents, such as gold and lung cancer and 5-ALA for actinic keratosis.52 PDT
nanoparticles, due to their superior PAI absorbance, which research in the brain has mainly focused on gliomas. A
is orders of magnitude higher than that of ICG and other number of early-phase clinical trials have been conducted
NIR dyes.46 using 5-ALA or Photofrin as photosensitizers.53,54 Notably,
Regardless of these findings, ICG both as the sole PAI a phase III trial in 2018 demonstrated that FGS comple-
contrast dye and in combination with other agents has mented by repetitive PDT with 5-ALA and Photofrin led
been demonstrated to successfully image brain tumors in to survival benefits in patients with GBM, compared with
animal studies. In 2017, Thawani et al. constructed a dual- surgery and radiotherapy.55
modality imaging agent using ICG-coated superparamag- The question of whether ICG is a good photosensitizer
netic iron oxide nanoparticle (SPION) clusters, which were for PDT remains controversial. In preclinical/early clini-
used for in vivo tumor imaging in a murine flank GBM cal studies for a variety of diseases in which PDT with
model.47 The SPIONs enabled preoperative MRI detection, ICG was investigated, some found that ICG is active in
whereas the ICG enabled intraoperative PAI guidance 24 PDT, whereas others claimed that it is not particularly
hours after tail-vein injection. This study also demonstrat- effective.56 A study by Keller et al. found no significant
ed increased progression-free survival of mice undergoing temperature elevation or brain damage on histological in-
PAI-guided surgery compared with microscopic surgery. vestigation following 1-hour NIR light exposure after ICG
Also in 2017, Zhu et al. demonstrated the ability of another injection in rats.57 In an in vitro study, the singlet oxygen
dual-modality agent, this time for fluorescent and photo- quantum yield of ICG is fairly low (Φ25 = 0.00949) and
6 Neurosurg Focus Volume 50 • January 2021
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
decreases with increased concentrations, probably due to ery have been two main approaches to bypass the BBB.
the aggregation problems of ICG at high concentrations.58 The recent development of so-called BBB-crossing nan-
However, modifications of the dye can improve its char- otechnology offers a new opportunity to integrate this
acteristics, and ICG has been incorporated in a number conventional therapy with other emerging therapies on a
of nanoparticle formulations as a fluorescent and PDT nanoplatform designed to target the BBB.74 Besides the
agent. For gliomas specifically, Shibata et al. developed multifunctional nanoparticles incorporating a chemother-
a liposomally formulated phospholipid-conjugated ICG apeutic moiety mentioned in the above studies, Shen et al.
(LP-iDOPE) nanoparticle and found significant tumor coated hydrophobic SPIO core with DSPE-PEG2000 and
growth suppression after using NIR irradiation in an or- hydrophobic doxorubicin (DOX), followed by ICG load-
thotopic rat GBM model.59 Hu et al. aimed to combine ing into lipid shell layers surrounding the surface, to yield
chemo- and phototherapy with an ICG/SN38 nanoformu- SPIO@DSPE-PEG/DOX/ICG nanoparticles with NIR
lation synthesized through self-assembly via hydrophobic fluorescence and MRI capabilities, along with the chemo-
interactions and demonstrated higher fluorescent intensity therapeutic efficacy to glioma provided by DOX.75 Hence,
compared with free ICG, as well as enhanced antitumor by packaging traditional chemotherapy drugs in novel
activity of the dual therapy in a U87MG nude mouse flank nanoparticle vehicles, the dual benefit of enhancing drug
tumor model.60 Liu et al. targeted neovascular endothelial delivery and adding synergy with imaging agents like ICG
cells in addition to tumor cells by using encapsulated- can be expected.
ICG c(RGDfk)-modified glycolipid-like micelles (cRGD- In general, ICG has been a popular agent to be included
CSOSA/ICG) for dual PDT/photothermal therapy (PTT).61 in nanoparticle formulations as a versatile molecule con-
Several recent studies have opted for an all-in-one cocktail ferring the theoretical basis for allowing NIR fluorescence
approach by designing complex nanoparticles that enable imaging, PAI, PDT, and PTT. While other properties of
imaging and therapy by using multiple modalities.50,62,63 ICG have been investigated in various degrees, its capa-
bility for NIR fluorescence imaging remains the most
Photothermal Therapy common reason to incorporate ICG in novel nanoagents.
PTT is a fairly new cancer treatment that uses the heat Another advantage provided by nanoparticles is the op-
generated from the absorbed optical energy by photother- portunity for designing active cellular targeting by using
mal transforming agents to achieve controlled thermal affinity ligands to bind tumor cells without accumulating
damage in tumor tissue. Whereas PDT is oxygen depen- in normal tissue, in contrast to free ICG, which targets
dent for the generation of reactive oxygen species, PTT neoplastic tissue through the nonspecific EPR property.
does not rely on oxygen and can be effective in ablating This area of research would become essential for improv-
hypoxic tumors.64 Sensitizing agents under investigation ing the precision of imaging as well as offering safe and
include NIR light–triggered inorganic materials (transi- effective application of phototherapy using ICG. With the
tion metals, sulfide, gold, and platinum nanoparticles)65 rapid growth of nanomedicine and synthesis of a plethora
as well as small organic molecules (cyanines, porphyrins, of nanoparticles, one issue that comes up is the lack of a
and polymers).66 Phase I/II trials of PTT have been con- uniform metric to compare their efficacies. And as pre-
ducted since 2011 for prostate cancer treatment.67 viously stated, the main challenge to bringing these new
ICG is an effective NIR-absorbing PTT agent with ex- theranostic technologies to patient care remains the dem-
cellent light-to-heat conversion efficiency, and numerous onstration of safety and the regulatory approvals required
groups have incorporated ICG into nanoparticle formula- prior to clinical translation. Because ICG has already been
tions to enable PTT.68,69 In glioma research, Xu et al. dem- approved by the FDA for human use and its feasibility to
onstrated that ICG encapsulated in silk fibroin nanoparti- be loaded on nanoparticle vehicles has been well docu-
cles exhibited a more stable photothermal effect compared mented, it presents as a compelling choice for future re-
with free ICG on NIR irradiation.70 Jia et al. developed a search on nanotherapy as the field marches closer toward
biomimetic ICG-loaded liposome (BLIPO-ICG) nanopar- translation to clinical application.
ticle with embedded glioma cell membrane proteins and
demonstrated strong NIR fluorescence 12 hours postin-
jection, proof-of-concept image-guided resection, and Conclusions
94.2% tumor growth inhibition by photothermal effect.71 ICG is a safe, cheap, FDA-approved NIR fluorescent
Recently, Gao et al. designed a two-step system in which contrast agent that has been proven useful for intraop-
Bis(DPA-Zn)-RGD is administered first as a prodrug, fol- erative visualization of the most common brain tumors.
lowed by administration of Au-ICG nanoparticles as a sec- Clinical results with SWIG thus far are encouraging, yet
ondary agent, yielding an ultrasmall R-Au-ICG nanoclus- large-scale randomized trials are still required to prove its
ter in vivo (approximately 7 nm) that can efficiently cross outcome benefits in patients with brain tumors. The re-
the BBB to enable enhanced fluorescence, PAI, and PTT.72 cent discovery of ICG’s tail emission in the SWIR window
has opened up exciting possibilities for ICG as an NIR-II
Chemotherapy fluorophore; yet, clinical studies have not been reported for
Traditional chemotherapy in brain tumors is limited this application in intracranial tumors. Additionally, ICG,
due to several factors, including genotypic heterogene- both in its free form and in combination with other agents,
ity, high drug resistance, and, most significantly, the low has been successfully used for PAI of brain tumors in ani-
BBB permeability of most chemotherapy agents.73 Poly- mal models. The phototherapeutic properties of ICG have
meric controlled release and convection-enhanced deliv- also been discovered and exploited mainly in the form of
Neurosurg Focus Volume 50 • January 2021 7
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
ICG nanoparticles to improve circulation time and enable 15. DSouza AV. Lin H, Henderson ER, Samkoe KS, Pogue BW.
active tumor targeting. Although these emerging technolo- Review of fluorescence guided surgery systems:identification
gies are still in the preclinical stage and may require time of key performance capabilities beyond indocyanine green
imaging. J Biomed Opt. 2016;21(8):080901.
before reaching the bedside, they continue to expand the 16. Jeon JW, Cho SS, Nag S, et al. Near-infrared optical contrast
possibility of ICG beyond its role as a simple NIR-I optical of skull base tumors during endoscopic endonasal surgery.
fluorophore and to offer novel solutions to neuro-oncology Oper Neurosurg (Hagerstown). 2019;17(1):32–42.
patients. 17. Ergin A, Wang M, Zhang JY, et al. The feasibility of real-time
in vivo optical detection of blood-brain barrier disruption with
indocyanine green. J Neurooncol. 2012;106(3):551–560.
Acknowledgments 18. Lee JYK, Pierce JT, Zeh R, et al. Intraoperative near-infrared
This work was supported in part by the Institute for Trans- optical contrast can localize brain metastases. World Neuro-
lational Medicine and Therapeutics of the Perelman School of surg. 2017;106:120–130.
Medicine at the University of Pennsylvania (Dr. Lee). In addition, 19. Lee JYK, Pierce JT, Thawani JP, et al. Near-infrared fluo-
research reported in this publication was supported by the Nation- rescent image-guided surgery for intracranial meningioma. J
al Center for Advancing Translational Sciences of the NIH under Neurosurg. 2018;128(2):380–390.
award number UL1TR000003 (Dr. Lee). The content is solely the 20. Cho SS, Jeon J, Buch L, et al. Intraoperative near-infrared
responsibility of the authors and does not necessarily represent imaging with receptor-specific versus passive delivery of
the official views of the NIH. fluorescent agents in pituitary adenomas. J Neurosurg. 2018;
131(6):1974–1984.
21. Cho SS, Zeh R, Pierce JT, et al. Comparison of near-infrared
References imaging camera systems for intracranial tumor detection.
1. Yannuzzi LA. Indocyanine green angiography:a perspective Mol Imaging Biol. 2018;20(2):213–220.
on use in the clinical setting. Am J Ophthalmol. 2011;151(5): 22. Cho A, Cho SS, Buch VP, et al. Second window indocyanine
745–751.e1. green (SWIG) near infrared fluorescent transventricular bi-
2. Lau CT, Au DM, Wong KKY. Application of indocyanine opsy of pineal tumor. World Neurosurg. 2020;134:196–200.
green in pediatric surgery. Pediatr Surg Int. 2019;35(10): 23. Hitti FL, Lee JYK. Endoscopic resection of an intraventricu-
1035–1041. lar tumor with second window indocyanine green:2-dimen-
3. Raabe A, Beck J, Gerlach R, et al. Near-infrared indocyanine sional operative video. Oper Neurosurg (Hagerstown). 2018;
green video angiography:a new method for intraoperative as- 15(5):E53–E54.
sessment of vascular flow. Neurosurgery. 2003;52(1):132–139. 24. Cho SS, Salinas R, De Ravin E, et al. Near-infrared imaging
4. Haglund MM, Berger MS, Hochman DW. Enhanced optical with second-window indocyanine green in newly diagnosed
imaging of human gliomas and tumor margins. Neurosur- high-grade gliomas predicts gadolinium enhancement on
gery. 1996;38(2):308–317. postoperative magnetic resonance imaging. Mol Imaging
5. Stummer W, Pichlmeier U, Meinel T, et al. Fluorescence- Biol. 2020;22(5):1427–1437.
guided surgery with 5-aminolevulinic acid for resection of 25. Kim J-H, Moon K-S, Jung J-H, et al. Importance of collateral
malignant glioma:a randomised controlled multicentre phase venous circulation on indocyanine green videoangiography
III trial. Lancet Oncol. 2006;7(5):392–401. in intracranial meningioma resection:direct evidence for
6. Madajewski B, Judy BF, Mouchli A, et al. Intraoperative venous compression theory in peritumoral edema formation.
near-infrared imaging of surgical wounds after tumor resec- J Neurosurg. 2019;132(6):1715–1723.
tions can detect residual disease. Clin Cancer Res. 2012; 26. Hide T, Yano S, Shinojima N, Kuratsu J. Usefulness of the in-
18(20):5741–5751. docyanine green fluorescence endoscope in endonasal trans-
7. Lee JYK, Thawani JP, Pierce J, et al. Intraoperative near- sphenoidal surgery. J Neurosurg. 2015;122(5):1185–1192.
infrared optical imaging can localize gadolinium-enhancing 27. Amano K, Aihara Y, Tsuzuki S, et al. Application of indo-
gliomas during surgery. Neurosurgery. 2016;79(6):856–871. cyanine green fluorescence endoscopic system in transsphe-
8. Ferroli P, Acerbi F, Albanese E, et al. Application of intraop- noidal surgery for pituitary tumors. Acta Neurochir (Wien).
erative indocyanine green angiography for CNS tumors:re- 2019;161(4):695–706.
sults on the first 100 cases. Acta Neurochir Suppl. 2011;109: 28. Hojo M, Arakawa Y, Funaki T, et al. Usefulness of tumor
251–257. blood flow imaging by intraoperative indocyanine green vid-
9. Zeh R, Sheikh S, Xia L, et al. The second window ICG tech- eoangiography in hemangioblastoma surgery. World Neuro-
nique demonstrates a broad plateau period for near infrared surg. 2014;82(3-4):e495–e501.
fluorescence tumor contrast in glioblastoma. PLoS One. 2017; 29. Cho SS, Sheikh S, Teng CW, et al. Evaluation of diagnostic
12(7):e0182034. accuracy following the coadministration of delta-aminolev-
10. Sandow N, Klene W, Elbelt U, et al. Intraoperative indocya- ulinic acid and second window indocyanine green in rodent
nine green videoangiography for identification of pituitary and human glioblastomas. Mol Imaging Biol. 2020;22(5):
adenomas using a microscopic transsphenoidal approach. 1266–1279.
Pituitary. 2015;18(5):613–620. 30. Bielenberg DR, Zetter BR. The contribution of angiogenesis
11. Baker KJ. Binding of sulfobromophthalein (BSP) sodium to the process of metastasis. Cancer J. 2015;21(4):267–273.
and indocyanine green (ICG) by plasma alpha-1 lipoproteins. 31. Cho SS, Buch VP, Teng CW, et al. Near-infrared fluorescence
Proc Soc Exp Biol Med. 1966;122(4):957–963. with second-window indocyanine green as an adjunct to
12. Cherrick GR, Stein SW, Leevy CM, Davidson CS. Indocya- localize the pituitary stalk during skull base surgery. World
nine green:observations on its physical properties, plasma Neurosurg. 2020;136:326.
decay, and hepatic extraction. J Clin Invest. 1960;39(4): 32. He S, Song J, Qu J, Cheng Z. Crucial breakthrough of second
592–600. near-infrared biological window fluorophores:design and
13. Stepp H, Stummer W. 5-ALA in the management of malig- synthesis toward multimodal imaging and theranostics. Chem
nant glioma. Lasers Surg Med. 2018;50(5):399–419. Soc Rev. 2018;47(12):4258–4278.
14. Cho SS, Salinas R, Lee JYK. Indocyanine-green for fluores- 33. Jain A, Homayoun A, Bannister CW, Yum K. Single-walled
cence-guided surgery of brain tumors:evidence, techniques, carbon nanotubes as near-infrared optical biosensors for life
and practical experience. Front Surg. 2019;6:11. sciences and biomedicine. Biotechnol J. 2015;10(3):447–459.
8 Neurosurg Focus Volume 50 • January 2021
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
34. McHugh KJ, Jing L, Behrens AM, et al. Biocompatible semi- blastoma multiforme:a single centre Phase III randomised
conductor quantum dots as cancer imaging agents. Adv Ma- controlled trial. Lasers Med Sci. 2008;23(4):361–367.
ter. 2018;30(18):e1706356. 56. Giraudeau C, Moussaron A, Stallivieri A, et al. Indocyanine
35. Carr JA, Franke D, Caram JR, et al. Shortwave infrared fluo- green:photosensitizer or chromophore? Still a debate. Curr
rescence imaging with the clinically approved near-infrared Med Chem. 2014;21(16):1871–1897.
dye indocyanine green. Proc Natl Acad Sci U S A. 2018; 57. Keller E, Ishihara H, Nadler A, et al. Evaluation of brain
115(17):4465–4470. toxicity following near infrared light exposure after
36. Starosolski Z, Bhavane R, Ghaghada KB, et al. Indocyanine indocyanine green dye injection. J Neurosci Methods. 2002;
green fluorescence in second near-infrared (NIR-II) window. 117(1):23–31.
PLoS One. 2017;12(11):e0187563. 58. Ruhi MK, Ak A, Gülsoy M. Dose-dependent photochemical/
37. Hu Z, Fang C, Li B, et al. First-in-human liver-tumour sur- photothermal toxicity of indocyanine green-based therapy on
gery guided by multispectral fluorescence imaging in the vis- three different cancer cell lines. Photodiagn Photodyn Ther.
ible and near-infrared-I/II windows. Nat Biomed Eng. 2020; 2018;21:334–343.
4(3):259–271. 59. Shibata S, Shinozaki N, Suganami A, et al. Photo-immune
38. Zhu S, Yung BC, Chandra S, et al. Near-infrared-II (NIR-II) therapy with liposomally formulated phospholipid-conjugat-
bioimaging via off-peak NIR-I fluorescence emission. Ther- ed indocyanine green induces specific antitumor responses
anostics. 2018;8(15):4141–4151. with heat shock protein-70 expression in a glioblastoma
39. Li J-B, Liu H-W, Fu T, et al. Recent progress in small-mole- model. Oncotarget. 2019;10(2):175–183.
cule near-IR probes for bioimaging. Trends Chem. 2019;1(2): 60. Hu S, Dong C, Wang J, et al. Assemblies of indocyanine
224–234. green and chemotherapeutic drug to cure established tumors
40. Antaris AL, Chen H, Cheng K, et al. A small-molecule dye by synergistic chemo-photo therapy. J Control Release. 2020;
for NIR-II imaging. Nat Mater. 2016;15(2):235–242. 324:250–259.
41. Tsuboi S, Jin T. Shortwave-infrared (SWIR) fluorescence 61. Liu Y, Dai S, Wen L, et al. Enhancing drug delivery for over-
molecular imaging using indocyanine green–antibody conju- coming angiogenesis and improving the phototherapy effi-
gates for the optical diagnostics of cancerous tumours. RSC cacy of glioblastoma by ICG-loaded glycolipid-like micelles.
Adv. 2020;10(47):28171–28179. Int J Nanomedicine. 2020;15:2717–2732.
42. Byrd BK, Marois M, Tichauer KM, et al. First experience 62. Huang X, Wu J, He M, et al. Combined cancer chemo-
imaging short-wave infrared fluorescence in a large animal: photodynamic and photothermal therapy based on ICG/
indocyanine green angiography of a pig brain. J Biomed Opt. PDA/TPZ-loaded nanoparticles. Mol Pharm. 2019;16(5):
2019;24(8):080501. 2172–2183.
43. Kurbegovic S, Juhl K, Chen H, et al. Molecular targeted NIR- 63. Hao Y, Wang L, Zhao Y, et al. Targeted imaging and chemo-
II probe for image-guided brain tumor surgery. Bioconjug phototherapy of brain cancer by a multifunctional drug deliv-
Chem. 2018;29(11):3833–3840. ery system. Macromol Biosci. 2015;15(11):1571–1585.
44. Moore C, Jokerst JV. Strategies for image-guided therapy, 64. Liu Y, Bhattarai P, Dai Z, Chen X. Photothermal therapy and
surgery, and drug delivery using photoacoustic imaging. photoacoustic imaging via nanotheranostics in fighting can-
Theranostics. 2019;9(6):1550–1571. cer. Chem Soc Rev. 2019;48(7):2053–2108.
45. Mallidi S, Luke GP, Emelianov S. Photoacoustic imaging in 65. Day ES, Morton JG, West JL. Nanoparticles for thermal can-
cancer detection, diagnosis, and treatment guidance. Trends cer therapy. J Biomech Eng. 2009;131(7):074001.
Biotechnol. 2011;29(5):213–221. 66. Jung HS, Verwilst P, Sharma A, et al. Organic molecule-
46. Li W, Chen X. Gold nanoparticles for photoacoustic imaging. based photothermal agents:an expanding photothermal ther-
Nanomedicine (Lond). 2015;10(2):299–320. apy universe. Chem Soc Rev. 2018;47(7):2280–2297.
47. Thawani JP, Amirshaghaghi A, Yan L, et al. Photoacoustic- 67. Rastinehad AR, Anastos H, Wajswol E, et al. Gold nanoshell-
guided surgery with indocyanine green-coated superpara- localized photothermal ablation of prostate tumors in a
magnetic iron oxide nanoparticle clusters. Small. 2017;13(37). clinical pilot device study. Proc Natl Acad Sci U S A. 2019;
48. Zhu M, Sheng Z, Jia Y, et al. Indocyanine green-holo-trans- 116(37):18590–18596.
ferrin nanoassemblies for tumor-targeted dual-modal imag- 68. Kwon YM, Je J-Y, Cha SH, et al. Synergistic combination of
ing and photothermal therapy of glioma. ACS Appl Mater chemo‑phototherapy based on temozolomide/ICG‑loaded
Interfaces. 2017;9(45):39249–39258. iron oxide nanoparticles for brain cancer treatment. Oncol
49. Liu C, Chen J, Zhu Y, et al. Highly sensitive MoS2-indocy- Rep. 2019;42(5):1709–1724.
anine green hybrid for photoacoustic imaging of orthotopic 69. Maziukiewicz D, Grześkowiak BF, Coy E, et al. NDs@
brain glioma at deep site. Nanomicro Lett. 2018;10(3):48. PDA@ICG conjugates for photothermal therapy of glioblas-
50. Yang Z, Du Y, Sun Q, et al. Albumin-based nanotheranostic toma multiforme. Biomimetics (Basel). 2019;4(1):3.
probe with hypoxia alleviating potentiates synchronous mul- 70. Xu H-L, ZhuGe DL, Chen PP, et al. Silk fibroin nanoparticles
timodal imaging and phototherapy for glioma. ACS Nano. dyeing indocyanine green for imaging-guided photo-thermal
2020;14(5):6191–6212. therapy of glioblastoma. Drug Deliv. 2018;25(1):364–375.
51. Singh D, Dilnawaz F, Sahoo SK. Challenges of moving ther- 71. Jia Y, Wang X, Hu D, et al. Phototheranostics:active tar-
anostic nanomedicine into the clinic. Nanomedicine (Lond). geting of orthotopic glioma using biomimetic proteolipid
2020;15(2):111–114. nanoparticles. ACS Nano. 2019;13(1):386–398.
52. Mahmoudi K, Garvey KL, Bouras A, et al. 5-aminolevulinic 72. Gao H, Chu C, Cheng Y, et al. In Situ formation of nanother-
acid photodynamic therapy for the treatment of high-grade anostics to overcome the blood-brain barrier and enhance
gliomas. J Neurooncol. 2019;141(3):595–607. treatment of orthotopic glioma. ACS Appl Mater Interfaces.
53. Muller PJ, Wilson BC. Photodynamic therapy of brain 2020;12(24):26880–26892.
tumors—a work in progress. Lasers Surg Med. 2006;38(5): 73. Tang W, Fan W, Lau J, et al. Emerging blood-brain-barrier-
384–389. crossing nanotechnology for brain cancer theranostics. Chem
54. Aziz F, Telara S, Moseley H, et al. Photodynamic therapy Soc Rev. 2019;48(11):2967–3014.
adjuvant to surgery in metastatic carcinoma in brain. Photo- 74. Belykh E, Shaffer KV, Lin C, et al. Blood-brain barrier,
diagn Photodyn Ther. 2009;6(3-4):227–230. blood-brain tumor barrier, and fluorescence-guided neuro-
55. Eljamel MS, Goodman C, Moseley H. ALA and Photofrin surgical oncology:delivering optical labels to brain tumors.
fluorescence-guided resection and repetitive PDT in glio- Front Oncol. 2020;10:739.
Neurosurg Focus Volume 50 • January 2021 9
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCTeng et al.
75. Shen C, Wang X, Zheng Z, et al. Doxorubicin and indocya- the article: Teng, Huang, Arguelles, Zhou. Reviewed submitted
nine green loaded superparamagnetic iron oxide nanopar- version of manuscript: all authors. Approved the final version of
ticles with PEGylated phospholipid coating for magnetic the manuscript on behalf of all authors: Lee. Study supervision:
resonance with fluorescence imaging and chemotherapy of Lee, Teng, Harmsen.
glioma. Int J Nanomedicine. 2018;14:101–117.
76. Teng CW, Cho SS, Singh Y, et al. Second window ICG pre- Supplemental Information
dicts gross-total resection and progression-free survival dur- Video
ing brain metastasis surgery. J Neurosurg. In press.
Video Abstract. https://vimeo.com/488051911.
Disclosures Correspondence
The authors report no conflict of interest concerning the materi- John Y. K. Lee: Hospital of the University of Pennsylvania, Phila-
als or methods used in this study or the findings specified in this delphia, PA. leejohn@pennmedicine.upenn.edu.
paper.
Author Contributions
Conception and design: Teng. Acquisition of data: Teng. Analysis
and interpretation of data: Teng, Huang, Arguelles, Zhou. Draft-
ing the article: Teng, Huang, Arguelles, Zhou. Critically revising
10 Neurosurg Focus Volume 50 • January 2021
Unauthenticated | Downloaded 05/05/21 08:17 PM UTCYou can also read