Brain and Body: A Review of Central Nervous System Contributions to Movement Impairments in Diabetes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Diabetes Volume 69, January 2020 3
Brain and Body: A Review of Central Nervous System
Contributions to Movement Impairments in Diabetes
Jennifer K. Ferris,1 J. Timothy Inglis,2 Kenneth M. Madden,3 and Lara A. Boyd1
Diabetes 2020;69:3–11 | https://doi.org/10.2337/db19-0321
Diabetes is associated with a loss of somatosensory and analyses (i.e., voxel-based morphometry or tract-based spa-
motor function, leading to impairments in gait, balance, tial statistics) to explore regional impacts of diabetes on the
and manual dexterity. Data-driven neuroimaging studies brain, and in these studies movement-related centers in the
frequently report a negative impact of diabetes on sen- brain frequently emerge as impacted by diabetes status (2,3).
sorimotor regions in the brain; however, relationships However, the impact of degeneration in movement centers
with sensorimotor behavior are rarely considered. The of the brain on motor behavior remains largely overlooked,
goal of this review is to consider existing diabetes neuro- despite the high prevalence of motor impairments in indi-
PERSPECTIVES IN DIABETES
imaging evidence through the lens of sensorimotor neu- viduals with diabetes (4).
roscience. We review evidence for diabetes-related While the impact of diabetes on central nervous system
disruptions to three critical circuits for movement con- (CNS) sensorimotor regions is understudied, disease com-
trol: the cerebral cortex, the cerebellum, and the basal plications in peripheral sensorimotor neurons are well
ganglia. In addition, we discuss how central nervous recognized. Diabetic peripheral neuropathy (DPN) is caused
system (CNS) degeneration might interact with the loss
by degeneration of peripheral somatic nerves and affects
of sensory feedback from the limbs due to peripheral
30–50% of individuals with diabetes (5). Movement impair-
neuropathy to result in motor impairments in individuals
ments in individuals with diabetes have historically been
with diabetes. We argue that our understanding of move-
attributed to DPN; however, motor impairments also occur
ment impairments in individuals with diabetes is incom-
plete without the consideration of disease complications in individuals with diabetes who do not have DPN, includ-
in both the central and peripheral nervous systems. ing poor balance (6), altered gait (7), and compromised grip
Neuroimaging evidence for disrupted central sensorimo- control (8). These findings suggest that pathology beyond
tor circuitry suggests that there may be unrecognized the peripheral somatic nervous system contributes to di-
behavioral impairments in individuals with diabetes. Ap- abetes-related sensorimotor impairments, and disease com-
plying knowledge from the existing literature on CNS plications in CNS sensorimotor regions are consequential
contributions to motor control and motor learning in for physical function.
healthy individuals provides a framework for hypothesis Control of motor behavior relies on reciprocal inter-
generation for future research on this topic. actions between the peripheral nervous system (PNS) and
CNS. Since there is evidence of both peripheral and central
neurodegeneration in individuals with diabetes, both sys-
Diabetes is associated with microvascular complications in tems must be considered in the study of sensorimotor
the nervous system. The link between diabetes and de- impairments. Sensorimotor research in individuals with
generative disease of the brain is well established, and an diabetes largely focuses on the PNS, whereas research on
intensive research effort has linked cognitive decline in CNS function in diabetes has mostly considered cognitive
individuals with diabetes to regional degeneration in the brain regions. Here, we attempt to bridge this gap by
brain (for review see Biessels and Reijmer, 2014 [1]). contextualizing recent neuroimaging findings of the
Multiple studies have employed hypothesis-free, data-driven effects of diabetes on the brain within a framework of
1Department of Physical Therapy, Faculty of Medicine, University of British Received 27 March 2019 and accepted 20 October 2019
Columbia, Vancouver, Canada © 2019 by the American Diabetes Association. Readers may use this article as
2Department of Kinesiology, Faculty of Education, University of British Columbia,
long as the work is properly cited, the use is educational and not for profit, and the
Vancouver, Canada work is not altered. More information is available at http://www.diabetesjournals
3Department of Medicine, Faculty of Medicine, University of British Columbia,
.org/content/license.
Vancouver, Canada
Corresponding author: Lara A. Boyd, lara.boyd@ubc.ca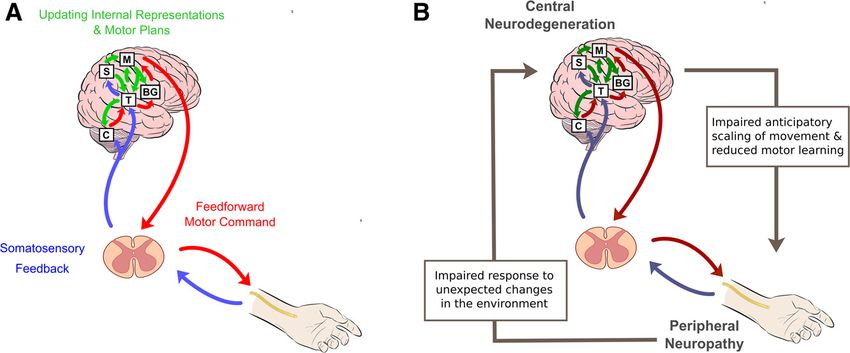
4 CNS Contributions to Movement Impairments Diabetes Volume 69, January 2020
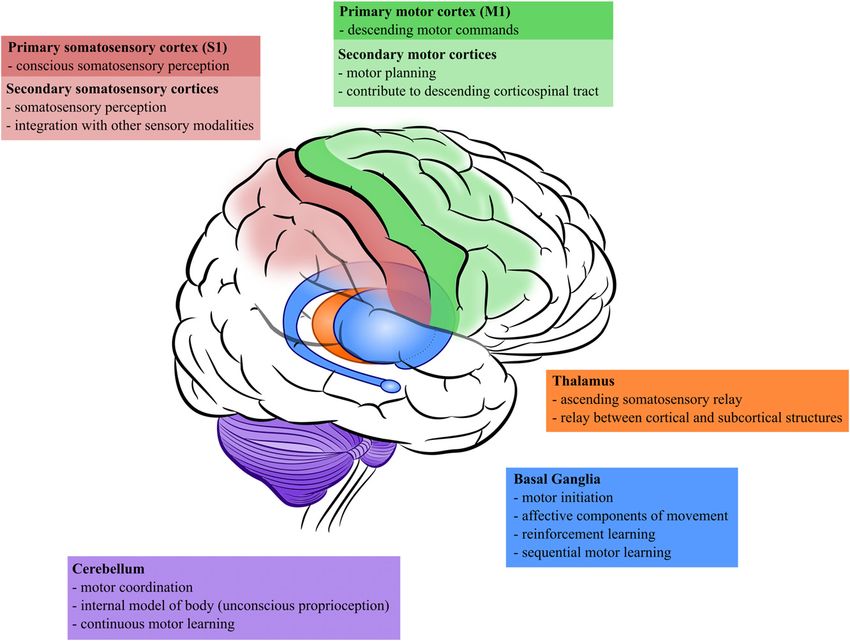
neural control of movement. For the purposes of this planning of voluntary movements. Descending outputs
review, we consider data from both populations with from the cortex travel via the corticospinal tract (CST) to
type 1 diabetes and populations with type 2 diabetes. synapse on efferent neurons of the spinal cord and initiate
We will use the term “diabetes” to refer to both forms muscle contractions. The primary somatosensory cortex
of diabetes and will differentiate between diabetes types (S1) contributes to the conscious awareness of somatosen-
where appropriate. sory information. Ascending somatosensory inputs from
spinal afferents synapse in the thalamus onto thalamocort-
Central Sensorimotor Dysfunction in Diabetes ical neurons projecting to S1. The sensorimotor cortex
Diabetes-related microvascular complications affect multi- operates as a functional unit due to substantial integration
ple tissue classes, including the retinas, kidneys, peripheral of processing between cortical regions, and between the
somatic nerves, and the brain. Microvascular disease in cortex and thalamus, reflecting the importance of sensori-
diabetes has similar mechanisms regardless of the tissue motor integration for motor function (14).
site; chronic hyperglycemia and loss of insulin signaling Diabetes is associated with atrophy and altered activity
cause a cascade of inflammatory pathway activation, oxi- of the somatosensory and motor cortices and their asso-
dative stress, and endothelial dysfunction (9). Inflammatory ciated white matter projections. At the level of the cortex,
endothelial dysfunction and subsequent loss of blood-brain gray matter volumes decrease in primary motor cortex
barrier integrity cause the development of cerebral micro- (11,15–17), the secondary motor cortices (17), and pri-
vascular lesions, resulting in an increased load of white mary somatosensory cortex (17). Cortical volume loss in
matter hyperintensities, lacunar infarcts, and microbleeds sensorimotor cortices is independently associated with
(for review see Wardlaw et al., 2013 [10]). Individuals with diabetes after correction for comorbid cardiometabolic
diabetes also show indicators of gross neurodegenerative risk factors (17), and sensorimotor cortex atrophy is
pathology, such as accelerated cortical atrophy (11). slowed in individuals undergoing intensive glycemic con-
The etiology of cerebral microvascular damage is com- trol (11), suggestive of an independent effect of diabetes
plex, and diabetes is one of many cardiometabolic risk status on cortical atrophy. Cortical activity is also impacted
factors that have been associated with an increased load by diabetes status. Resting state functional MRI (fMRI)
of cerebral microvascular complications; other risk factors studies of local spontaneous activity consistently report
include hypertension, smoking, and hyperlipidemia (12). lower activity in S1 (18–21), and S1 activity relates neg-
The presence of multiple risk factors will increase the atively to fasting glucose levels (20). Primary (22) and
incidence of cerebral microvascular complications (10), secondary (23) motor cortex activity is decreased in indi-
a consideration that deserves careful examination in this viduals with diabetes, including reduced excitability in M1
population. However, diabetes has independent negative regions specific to control of the upper extremity (24). The
impacts on CNS tissues. Specific to diabetes is the frequent time course of changes in volume and activity of the
cooccurrence of microvascular pathology in nerves of the cortical gray matter is unclear; cortical activity may de-
peripheral somatic nervous system (5). Additionally, animal crease as a direct consequence of cortical atrophy, or
research has revealed a role of insulin signaling in neuro- conversely, changes in the metabolic activity of the cortex
plasticity and consequently a loss of neuroplasticity in may be an early indicator of regions vulnerable to neuronal
insulin-resistant animals (13). These processes, in addition death.
to gross neurodegeneration, have implications for motor Several lines of evidence indicate that diabetes is related
function in individuals with diabetes. to degeneration of white matter projections between the
Recent advances in neuroimaging allow for highly sensorimotor cortices and subcortical structures. At the
region-specific investigations of cerebral structure and level of the spinal cord, individuals with diabetes show
function, and these have provided emerging evidence gross atrophy in the cervical spine that is most severe in
that diabetes impacts areas of the brain involved in per- individuals with DPN but is also present in individuals
ceiving ascending somatosensory information and generat- with diabetes without DPN (25,26). This suggests that loss
ing descending motor output. The study of regional brain of spinal white matter results from a dual contribution of
networks may yield insights into the behavioral declines degeneration of peripheral afferents in DPN and degen-
seen in this population. To guide this review of CNS eration of ascending and descending CNS spinal pathways.
contributions to movement impairment in diabetes, we For descending corticospinal projections from M1, diffu-
focused our discussion on three critical regions for volun- sion tensor imaging studies report decreases in micro-
tary sensorimotor control and their associated white mat- structural integrity in the descending white matter of the
ter projections: 1) the cerebral cortex, specifically, the CST (27–31), which relates to cortical atrophy in M1 (2).
motor and somatosensory cortices; 2) the cerebellum; The conduction velocity of upper motor neurons of the
and 3) the basal ganglia (Fig. 1). CST is delayed in humans (32,33) and in rodent models of
diabetes (34). Loss of microstructural integrity and delays
Somatosensory and Motor Cortex in conduction velocity are indicative of neuronal loss or
The primary motor cortex (M1) and associated secondary demyelination in this critical motor pathway. White mat-
motor cortices play a critical role in the initiation and ter tracts between the cortex and thalamus are alsodiabetes.diabetesjournals.org Ferris and Associates 5
Figure 1—Sensorimotor regions in the CNS with evidence for diabetes-related neurodegeneration.
impacted by diabetes status. Functional connectivity is to be an important mechanism in the acquisition and
decreased between the thalamus and M1 (35), suggesting consolidation of skilled movements (38). Although there
reduced communication between the thalamus and motor is evidence that diabetes decreases capacity for long-term
cortex. In terms of somatosensory inputs to the thalamus, potentiation-like plasticity in the human motor cortex
there is a decrease in the conduction velocity of ascending (39), the relationship of neuroplasticity with motor func-
afferent signals specific to the thalamus-S1 relay (36,37), tion has not been examined in individuals with diabetes. In
indicating that thalamocortical projections are impacted by summary, while there exists some evidence that diabetes-
diabetes independently from delays in peripheral afferent related motor impairments relate to cortical neurodegen-
conduction velocity caused by peripheral neuropathy. eration, many behavioral metrics that are known to rely on
Evidence from multiple modalities indicates that di- sensorimotor cortical function remain unexplored in indi-
abetes impacts both the structure and function of senso- viduals with diabetes.
rimotor cortical gray matter and projection fibers to
associated subcortical and spinal structures. Diabetes- Cerebellum
related degeneration to sensorimotor cortex may impact The cerebellum is involved in motor coordination and
the behaviors supported by these regions during sensori- unconscious proprioception and is organized into anatom-
motor function. Investigations of cortical function in re- ically and functionally distinct regions. The cerebellum
lation to motor function in individuals with diabetes have receives sensory inputs from the spinal cord and projects
been performed with pegboard assessments of manual output onto descending motor pathways. Furthermore,
dexterity. Manual dexterity relates to M1 thickness (2), the cerebellum has extensive bidirectional connectivity
and white matter microstructure of the CST (27), with with the cerebral cortex via thalamic relays. The cerebellum
markers of decreased structural integrity relating to poorer is responsible for maintaining an internal representation
manual dexterity in individuals with diabetes. In addition, of the body, predicting the sensory consequences of move-
neuroplasticity within the sensorimotor cortices is known ment, and updating motor plans generated by the cortex in6 CNS Contributions to Movement Impairments Diabetes Volume 69, January 2020
response to movement errors (40). Corticocerebellar net- for diabetes-related disruptions (18,46,47). These regions
works play an important role in both motor coordination of the cerebellum have connectivity with the cerebral
and motor learning (41). cortex and are involved in voluntary control of distal
Glucose metabolism is more efficient in the cerebellum muscles, as in the coordination of reaching movements.
compared with the cerebrum, meaning the cerebellum is The implications of changes to lateral cerebellar lobes for
relatively protected from hypoglycemic damage (42); how- motor function have been neglected, despite the rich
ever, the cerebellum is vulnerable to hyperglycemia-related literature demonstrating the importance of these regions
toxicity over the course of diabetes progression (43). Total in error-based motor learning, anticipatory control of
cerebellar volume is reduced in individuals with diabetes movement, and spatial and temporal patterning of motor
(44,45), and there is a negative linear relationship between coordination (54).
cerebellar volume and fasting plasma glucose (44). De-
creased cerebellar volume is accompanied by changes to Basal Ganglia
white matter microstructure within the anterior and pos- The basal ganglia contribute to the initiation and exe-
terior cerebellar lobes (46,47) and the vermis (3,47). White cution of voluntary movement, as well as the affective
matter microstructure in the cerebellar lobes decreases components of movement. The basal ganglia are a group
with greater disease duration (46,47), indicating a negative of subcortical nuclei comprising the caudate, putamen,
cumulative impact of hyperglycemia exposure to cerebellar globus pallidus, and subthalamic nucleus. These nuclei
structure. Tracts between the cerebellum and the cortex receive projections from the cortex, thalamus, and brain-
are also broadly affected by diabetes status; notably, there stem, and their major output returns to the cortex via
is decreased white matter integrity in tracts traveling from the thalamus. The best studied basal ganglia–cortical
the cerebellum to the thalamus and M1 (47). loop is a motor circuit formed with the primary and
The impact of diabetes on cerebellar activity is unclear. association motor cortices. This loop is important for
Resting state studies of local spontaneous brain activity the selection and initiation of motor actions, guided by
report both increased (18,23,48) and decreased (19,23,49) environmental reinforcement (55). The basal ganglia are
spontaneous activity within anterior and posterior lobes of involved in learning and performance of discrete se-
the cerebellum. However, these studies all employed data- quences of movements—in contrast to the cerebellum,
driven whole-brain approaches, which involve spatial which is involved in smoothing and coordinating contin-
smoothing of brain regions across subjects for alignment uous movements (56).
to an atlas space. While these approaches allow for ex- There are very few investigations of the basal ganglia in
ploratory analyses of brain activity, inconsistencies in individuals with diabetes. Gray matter volumes are re-
previous activations studies may be a result of the high duced in the caudate (57,58) and the putamen (58–60),
interindividual variability in corticocerebellar anatomy, and there is lower cerebral blood perfusion in the caudate
which makes alignment to a common template space (53,61). Additionally, there is some evidence for decreased
problematic (50). Connectivity-based resting state anal- connectivity between basal ganglia and cortical networks
yses comparing networks of brain activity show re- (52). Consistent with the basal ganglia’s role in response
duced cerebellar connectivity in multiple cerebral-cerebellar selection, basal ganglia atrophy (60) and decreased basal
brain networks (51,52). Cerebellar connectivity negatively ganglia blood flow (61) relate to reduced psychomotor
relates both to diabetes disease duration and HbA1c levels speed in individuals with diabetes. Given the known
(51). To resolve incongruencies in previous findings, future functions of the basal ganglia, alterations in these struc-
fMRI studies should perform regional analyses of the cere- tures in individuals with diabetes may contribute to
bellum that are robust to individual differences in cerebellar diabetes-related delays in reaction time (62) or slowed gait
anatomy. speed (63).
Cerebellar damage is associated with abnormal control
of movement, and movement abnormalities vary depend- The Impact of Diabetic Neuropathy on the CNS
ing on which specialized region of the cerebellum is Diabetes-related disease complications exist in both pe-
impacted. For example, diabetes affects the vermis and ripheral and central sensorimotor nervous tissues. An
intermediate hemispheres of the cerebellar lobes (3,47). open question is the degree to which loss of peripheral
These cerebellar regions receive ascending inputs from signaling caused by DPN impacts CNS somatosensory and
spinal cord and brainstem centers and are principally motor function. It is possible that the loss of afferent
involved in the control of proximal muscles and coordi- information from the periphery directly causes remodeling
nation of movement during gait, and individuals with of central sensory circuits, as observed in individuals with
diabetes show gait abnormalities that relate to decreased loss of afferent input after limb amputation (64). Reduced
blood flow in the vermis and intermediate lobe of the primary somatosensory cortex activity in individuals with
cerebellum (53). However, the majority of diabetes cere- diabetes (18–21) may occur as a direct result of loss of
bellar research has detected alterations in the lateral hemi- peripheral afferent signal or, conversely, may reflect an
spheres of the cerebellum. Specifically, posterior regions of independent process of cortical atrophy occurring due to
the lateral cerebellar hemispheres have the most evidence central complications of diabetes. Selvarajah et al. (65)diabetes.diabetesjournals.org Ferris and Associates 7
(2014) reported decreased S1 volumes in individuals with gating and hyperexcitability of the thalamus (67). Research
DPN. However, the comparison group consisted of a mix of into the effects of diabetic neuropathy on the CNS should
individuals with diabetes and no DPN and healthy control therefore consider painful and nonpainful neuropathy
subjects without diabetes; therefore, this study did not subtypes separately, as chronic neuropathic pain may
consider the impact that diabetes alone may have on S1 produce a central sensitization that results in a different
volumes. Conversely, resting state fMRI studies report no neurological phenotype.
differences in S1 activity between patients with DPN and In summary, neuroimaging evidence from individuals
those without (18,19). These data are suggestive of an with DPN indicates that diabetes damages central senso-
independent process of central neurodegeneration caused rimotor regions in a process concurrent with but separate
by diabetes, but future research must better control for from peripheral microvascular complications (Table 1).
confounding effects of loss of peripheral signaling from More research is required to establish the typical pro-
DPN. gression of microvascular complications in the PNS and
An important caveat to this assertion is the presence of CNS. If diabetes disease complications in the CNS precede
chronic neuropathic pain. There is evidence that, in con- PNS complications, sensorimotor impairments may be
trast to insensate forms of neuropathy, painful subtypes present even in individuals who do not show diagnostic
of peripheral neuropathy have a direct impact on CNS indicators of peripheral neuropathy. On the other hand, if
function (for a detailed review see Fischer and Waxman, peripheral neuropathy typically precedes CNS degenera-
2010 [66]). Pain in diabetic neuropathy is partially neu- tion there may be a progressive decline in the ability of the
ropathic in origin and relates to altered somatosensory CNS to compensate for loss of sensorimotor control in the
Table 1—Summary of neuroimaging findings of disrupted central sensorimotor circuits in individuals with diabetes
Imaging characteristics in individuals with diabetes
Method and relationships with sensorimotor function
Motor and somatosensory cortices
Structural volumetrics Decreased cortical gray matter volume in:
c M1 (11,15–17); manual dexterity is decreased in individuals with lower
M1 thickness (2)
c Secondary motor cortex (17)
c S1 (17)
Diffusion tensor imaging Decreased microstructural integrity in CST white matter (27–31); manual
dexterity is decreased in individuals with lower CST integrity (27)
Resting state fMRI Decreased spontaneous activity in:
c M1 (22)
c Supplementary motor area (23)
c S1 (18–21)
Decreased connectivity between M1 and thalamus (35)
Neurophysiology Decreased excitability in upper-extremity representations of M1 (24)
Decreased cortical plasticity in M1 (39)
Decreased central conduction velocity of the CST (32–34)
Decreased central conduction velocity of thalamus-S1 afferent relay (36,37)
Cerebellum
Structural volumetrics Decreased cerebellar gray matter volume (44,45); gait impairments in
individuals with lower cerebellar gray matter (45)
Diffusion tensor imaging Decreased microstructural integrity in cerebellar white matter (3,46)
Decreased microstructural integrity in:
c Intracerebellar white matter tracts (47)
c Corticocerebellar tracts to thalamus and M1 (47)
Resting state fMRI Changes to regional spontaneous brain activity (ALFF and ReHo):
c Increased in posterior cerebellum (18,23)
c Decreased in posterior cerebellum (19,23,49)
c Increased in anterior cerebellum (48)
c Decreased in anterior cerebellum (49) and vermis (23)
Decreased connectivity between posterior cerebellum and cerebrum (51)
Basal ganglia
Structural volumetrics Decreased gray matter volume in:
c Caudate (57,58)
c Putamen (58–60)
Resting state fMRI Functional connectivity altered in caudate, putamen, and thalamus (52)
Cerebral perfusion (ASL) Cerebral perfusion decreased in caudate (53,61); psychomotor speed is
decreased in individuals with lower blood perfusion in the caudate (61)
ALFF, amplitude of low-frequency fluctuations; ASL, arterial spin labeling; ReHo, regional homogeneity.8 CNS Contributions to Movement Impairments Diabetes Volume 69, January 2020
periphery, creating an additive burden on sensorimotor motor control are clinically significant, as individuals with
impairments. peripheral neuropathy are at highest risk of falls after
unexpected gait perturbances (73).
The Implications of Diabetes-Related Feedforward control from the CNS provides descending
Neurodegeneration for Neural Control of Movement commands for voluntary movement. Feedforward motor
Modern theories of motor control and motor learning control is the initiation and anticipatory scaling of move-
emphasize reciprocal relationships between peripheral ments that occurs before sensory feedback on the move-
(feedback) and central (feedforward) control of movement ment is received by peripheral receptors (74). Movement
(for review see Scott et al., 2015 [68]). Damage to either impairments in individuals with diabetes have primarily
the PNS or CNS will lead to characteristic impairments in been interpreted as a result of loss of feedback signaling
movement abilities, and these theoretical frameworks can from peripheral neuropathy, neglecting potential contri-
inform our understanding of movement impairments in butions of feedforward mechanisms. For instance, gait is
individuals with diabetes. under relatively greater feedforward control than quiet
Feedback from peripheral afferents provides information stance (75), and thus gait abnormalities observed in individuals
about the current state of the body and the success of ongoing with diabetes who do not have peripheral neuropathy (7)
goal-oriented movements. Peripheral neuropathy causes loss may result from a loss of feedforward control rather than
of afferent inputs and thus a loss of feedback motor control, feedback errors. This also may contribute to dual-task gait
which manifests in multiple behavioral metrics. A simple impairments in individuals with diabetes (76). Moreover,
example of loss of feedback motor control is an increase in considering feedforward contributions to motor control
body sway during quiet stance, which is a result of decreased may help to resolve contradictory findings in previous
tactile and proprioceptive inputs from the feet and ankles research. For example, the counterintuitive finding of
(69). More complex feedback motor control occurs in con- reduced grip force applied during object manipulation in
ditions of unexpected environmental changes, which neces- individuals with diabetes (77) might be explained by a loss
sitate rapid correction of ongoing movements. Peripheral of feedforward grip control. Finally, there are possibly
neuropathy causes decreased muscle responses to unexpected unrecognized motor deficits in individuals with diabetes
lower-extremity perturbations (70), indicating an impaired in view of evidence for degeneration to brain networks
ability to adapt motor patterns in response to somatosen- involved in feedforward motor control; notably, the
sory feedback. A loss of afferent feedback results in de- impact of diabetes on motor adaptation and motor learn-
creased movement stability, which causes compensatory ing is currently unknown.
increases in feedforward motor control strategies. In indi- Although the prevalence and progression of central
viduals with peripheral neuropathy, this may be seen as an complications relative to peripheral complications are not
increase in postural anticipation of surface changes during well characterized, individuals with diabetes could present
gait (71) or a higher grip force being applied when man- with central microvascular disease, peripheral neuropathy,
ually manipulating objects (72). Impairments in feedback or a combination of both. An interesting question is how
Figure 2—A: Schematic of feedback and feedforward motor control between the peripheral and central sensorimotor nervous systems. B:
Effects of interactions between PNS and CNS degeneration on sensorimotor function in individuals with diabetes. BG, basal ganglia; C,
cerebellum; M, motor cortices; S, somatosensory cortices; T, thalamus.diabetes.diabetesjournals.org Ferris and Associates 9
both the loss of feedforward control and the loss of feedback motor performance also impacts cognitive function, as in
control would interact to influence sensorimotor function in reports showing that slowed gait speed is an early predictor
individuals with diabetes. Very few studies have considered of cognitive impairment in older adults (79). The purpose of
both peripheral and central diabetes complications in the this review is not to suggest that cognitive function is separate
study of motor function. Manor et al. (45) (2012) from, or less important than, sensorimotor function, partic-
reported decreased cerebellar volumes in individuals ularly in individuals with diabetes who are expected to
with diabetes related to slowed gait speed and decreased show both cognitive and sensorimotor symptoms. In-
stability during gait; however, this relationship was stron- stead, our goal is to draw attention to existing neuro-
ger in individuals with peripheral neuropathy. Nunley et al. imaging evidence for CNS contributions to sensorimotor
(60) (2017) reported that putamen volumes and peripheral disability. Future work on diabetes disease complications
neuropathy related to psychomotor slowing in individuals must consider the complex interactions between cognitive
with type 1 diabetes, but putamen volumes did not relate and sensorimotor impairment.
to psychomotor speed in control subjects without diabetes.
These data suggest an increased reliance on central feed- Conclusions
forward control in individuals with loss of afferent feed- The current review highlights evidence that diabetes-
back from DPN. In both of these studies, individuals with related CNS degeneration may contribute to impairments
diabetes and DPN had poorer motor function than indi- in motor control, motor performance, and motor learning.
viduals without DPN (45,60); thus, adequate feedforward We argue that the central contributions to motor deficits
compensation for loss of somatosensory inputs may not be in individuals with diabetes are more profound than pre-
possible due to CNS degeneration. There is likely an viously recognized. Existing data suggest that changes in
additive burden of central and peripheral sensorimotor central sensorimotor signaling in diabetes are not simply
changes on motor behavior; our understanding of the a passive response to loss of afferent signaling from the
neurological sources of motor impairments is incomplete PNS but, rather, reflect an independent and additive pro-
without interrogation of feedforward motor deficits in cess of regional neurodegeneration. There is a critical need
individuals with diabetes (Fig. 2). for controlled behavioral experiments linking cerebral
markers of sensorimotor degeneration with movement
Role of Cognitive Impairment in Motor Function impairments in individuals with diabetes. We identify
Diabetes is a major risk factor for cognitive decline and several areas in need of more research (Table 2) including
dementia (1). This topic has received considerable research 1) identifying novel motor control and motor learning
attention; indeed, the primary aim of many of the studies deficits in individuals with diabetes, 2) evaluating the
presented in this review was to identify relationships be- extent to which CNS complications relate to sensorimotor
tween brain metrics and cognitive decline in individuals with impairments in this population, and 3) delineating the
diabetes. Cognition and mobility are inextricably linked, and interactions between progression of diabetic neuropathy
therefore impairments in attention or executive functions and CNS sensorimotor complications.
could impact motor performance. For example, in dual- The research outlined in this review has implications
task paradigms, older adults show decreased motor for the clinical management of diabetes complications.
performance with increasing attentional load (78). Conversely, Most importantly, diabetes-related CNS complications
may have a significant and unrecognized contribution
Table 2—Recommendations for future research on CNS to the high rates of physical disability and dependency
contributions to movement impairments in individuals in activities of daily living in this population (4).
with diabetes However, current clinical screening batteries are not
c Move toward hypothesis-driven ROI-based designed to identify individuals with sensorimotor
neuroimaging analyses to delineate regional impacts of impairments originating in the CNS, and the preva-
diabetes on sensorimotor circuits
lence of CNS complications is unknown. Exploring
c Include appropriate healthy control groups to evaluate
sensorimotor impairments attributable to diabetes relationships between central sensorimotor circuits and
c Control for comorbid cardiometabolic risk factors impaired behavioral function could therefore lead to the
(i.e., hypertension, dyslipidemia) to elucidate the identification of novel markers of sensorimotor decline in
neuropathological profile specific to diabetes individuals with diabetes. In conclusion, the impact of
c Relate markers of CNS degeneration to movement
diabetes on central sensorimotor function is a promising,
impairments in individuals with diabetes
c Explore the degree of diabetes-related impairment in but still underdeveloped, area of research. Future work
sensorimotor domains under CNS control delineating the nature and extent of sensorimotor deficits
(i.e., feedforward motor control) in this population is required for the effective management
c Consider how DPN interacts with central degeneration in of physical disability in individuals with diabetes.
relation to sensorimotor impairments
c Consider painful and nonpainful subtypes of DPN
separately, as they have different central phenotypes
Funding. This work was funded by the Canadian Institutes of Health Research
ROI, region of interest.
(GD-146283).10 CNS Contributions to Movement Impairments Diabetes Volume 69, January 2020
Duality of Interest. No potential conflicts of interest relevant to this article 22. Liu D, Duan S, Zhang J, et al. Aberrant brain regional homogeneity and
were reported. functional connectivity in middle-aged T2DM patients: a resting-state functional
MRI study. Front Hum Neurosci 2016;10:490
References 23. Wang CX, Fu KL, Liu HJ, Xing F, Zhang SY. Spontaneous brain activity in type
1. Biessels GJ, Reijmer YD. Brain changes underlying cognitive dysfunction in 2 diabetics revealed by amplitude of low-frequency fluctuations and its association
diabetes: what can we learn from MRI? Diabetes 2014;63:2244–2252 with diabetic vascular disease: a resting-state FMRI study. PLoS One 2014;9:
2. Franc DT, Kodl CT, Mueller BA, Muetzel RL, Lim KO, Seaquist ER. High e108883
connectivity between reduced cortical thickness and disrupted white matter tracts 24. Andersen H, Nielsen JF, Poulsen PL, Mogensen CE, Jakobsen J. Motor pathway
in long-standing type 1 diabetes. Diabetes 2011;60:315–319 function in normoalbuminuric IDDM patients. Diabetologia 1995;38:1191–1196
3. Tan X, Fang P, An J, et al. Micro-structural white matter abnormalities in type 25. Selvarajah D, Wilkinson ID, Emery CJ, et al. Early involvement of the spinal
2 diabetic patients: a DTI study using TBSS analysis. Neuroradiology 2016;58: cord in diabetic peripheral neuropathy. Diabetes Care 2006;29:2664–2669
1209–1216 26. Eaton SEM, Harris ND, Rajbhandari SM, et al. Spinal-cord involvement in
4. Wong E, Backholer K, Gearon E, et al. Diabetes and risk of physical disability diabetic peripheral neuropathy. Lancet 2001;358:35–36
in adults: a systematic review and meta-analysis. Lancet Diabetes Endocrinol 27. Kodl CT, Franc DT, Rao JP, et al. Diffusion tensor imaging identifies deficits in
2013;1:106–114 white matter microstructure in subjects with type 1 diabetes that correlate with
5. Dyck PJ, Kratz KM, Karnes JL, et al. The prevalence by staged severity of reduced neurocognitive function. Diabetes 2008;57:3083–3089
various types of diabetic neuropathy, retinopathy, and nephropathy in a pop- 28. Sun Q, Chen GQ, Wang XB, et al. Alterations of white matter integrity and
ulation-based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993; hippocampal functional connectivity in type 2 diabetes without mild cognitive
43:817–824 impairment. Front Neuroanat 2018;12:21
6. Centomo H, Termoz N, Savoie S, Béliveau L, Prince F. Postural control 29. van Bloemendaal L, Ijzerman RG, Ten Kulve JS, et al. Alterations in white
following a self-initiated reaching task in type 2 diabetic patients and age-matched matter volume and integrity in obesity and type 2 diabetes. Metab Brain Dis 2016;
controls. Gait Posture 2007;25:509–514 31:621–629
7. Allet L, Armand S, de Bie RA, et al. Gait alterations of diabetic patients while 30. Xiong Y, Sui Y, Xu Z, et al. A diffusion tensor imaging study on white matter
walking on different surfaces. Gait Posture 2009;29:488–493 abnormalities in patients with type 2 diabetes using tract-based spatial statistics.
8. Ochoa N, Gogola GR, Gorniak SL. Contribution of tactile dysfunction to AJNR Am J Neuroradiol 2016;37:1462–1469
manual motor dysfunction in type II diabetes. Muscle Nerve 2016;54:895– 31. Zhang J, Wang Y, Wang J, et al. White matter integrity disruptions associated
902 with cognitive impairments in type 2 diabetic patients. Diabetes 2014;63:3596–
9. Goldberg RB. Cytokine and cytokine-like inflammation markers, endothelial 3605
dysfunction, and imbalanced coagulation in development of diabetes and its 32. Abbruzzese G, Schenone A, Scramuzza G, et al. Impairment of central motor
complications. J Clin Endocrinol Metab 2009;94:3171–3182 conduction in diabetic patients. Electroencephalogr Clin Neurophysiol 1993;89:
10. Wardlaw JM, Smith C, Dichgans M. Mechanisms of sporadic cerebral small 335–340
vessel disease: insights from neuroimaging. Lancet Neurol 2013;12:483–497 33. Moglia A, Arrigo A, Maurelli M, et al. Central motor conduction after magnetic
11. Erus G, Battapady H, Zhang T, et al. Spatial patterns of structural brain stimulation in diabetes. Ital J Neurol Sci 1998;19:10–14
changes in type 2 diabetic patients and their longitudinal progression with in- 34. Muramatsu K, Ikutomo M, Tamaki T, Shimo S, Niwa M. Effect of strepto-
tensive control of blood glucose. Diabetes Care 2015;38:97–104 zotocin-induced diabetes on motor representations in the motor cortex and
12. Vermeer SE, Den Heijer T, Koudstaal PJ, Oudkerk M, Hofman A, Breteler MM; corticospinal tract in rats. Brain Res 2018;1680:115–126
Rotterdam Scan Study. Incidence and risk factors of silent brain infarcts in the 35. Chen Y-C, Xia W, Qian C, Ding J, Ju S, Teng GJ. Thalamic resting-state
population-based Rotterdam Scan Study. Stroke 2003;34:392–396 functional connectivity: disruption in patients with type 2 diabetes. Metab Brain Dis
13. Stranahan AM, Norman ED, Lee K, et al. Diet-induced insulin resistance 2015;30:1227–1236
impairs hippocampal synaptic plasticity and cognition in middle-aged rats. Hip- 36. Nakamura R, Noritake M, Hosoda Y, Kamakura K, Nagata N, Shibasaki H.
pocampus 2008;18:1085–1088 Somatosensory conduction delay in central and peripheral nervous system of
14. Petrof I, Viaene AN, Sherman SM. Properties of the primary somatosensory diabetic patients. Diabetes Care 1992;15:532–535
cortex projection to the primary motor cortex in the mouse. J Neurophysiol 2015; 37. Piriz J, Torres-Aleman I, Nuñez A. Independent alterations in the central and
113:2400–2407 peripheral somatosensory pathways in rat diabetic neuropathy. Neuroscience
15. Bernardes G, IJzerman RG, Ten Kulve JS, et al. Cortical and subcortical gray 2009;160:402–411
matter structural alterations in normoglycemic obese and type 2 diabetes patients: 38. Nudo RJ, Milliken GW, Jenkins WM, Merzenich MM. Use-dependent al-
relationship with adiposity, glucose, and insulin. Metab Brain Dis 2018;33:1211–1222 terations of movement representations in primary motor cortex of adult squirrel
16. Chen Z, Li L, Sun J, Ma L. Mapping the brain in type II diabetes: voxel-based monkeys. J Neurosci 1996;16:785–807
morphometry using DARTEL. Eur J Radiol 2012;81:1870–1876 39. Fried PJ, Schilberg L, Brem AK, et al. Humans with type-2 diabetes show
17. Hughes TM, Ryan CM, Aizenstein HJ, et al. Frontal gray matter atrophy in abnormal long-term potentiation-like cortical plasticity associated with verbal
middle aged adults with type 1 diabetes is independent of cardiovascular risk learning deficits. J Alzheimers Dis 2017;55:89–100
factors and diabetes complications. J Diabetes Complications 2013;27:558– 40. Ramnani N. The primate cortico-cerebellar system: anatomy and function.
564 Nat Rev Neurosci 2006;7:511–522
18. Cui Y, Jiao Y, Chen YC, et al. Altered spontaneous brain activity in type 41. Doyon J, Penhune V, Ungerleider LG. Distinct contribution of the cortico-
2 diabetes: a resting-state functional MRI study. Diabetes 2014;63:749–760 striatal and cortico-cerebellar systems to motor skill learning. Neuropsychologia
19. Peng J, Qu H, Peng J, et al. Abnormal spontaneous brain activity in type 2003;41:252–262
2 diabetes with and without microangiopathy revealed by regional homogeneity. 42. Cranston I, Marsden P, Matyka K, et al. Regional differences in cerebral blood
Eur J Radiol 2016;85:607–615 flow and glucose utilization in diabetic man: the effect of insulin. J Cereb Blood
20. Chen Y, Liu Z, Zhang J, et al. Selectively disrupted functional connectivity Flow Metab 1998;18:130–140
networks in type 2 diabetes mellitus. Front Aging Neurosci 2015;7:233 43. Nagayach A, Patro N, Patro I. Experimentally induced diabetes causes glial
21. Xia W, Chen YC, Ma J. Resting-state brain anomalies in type 2 diabetes: activation, glutamate toxicity and cellular damage leading to changes in motor
a meta-analysis. Front Aging Neurosci 2017;9:14 function. Front Cell Neurosci 2014;8:355diabetes.diabetesjournals.org Ferris and Associates 11 44. Hoogendam YY, van der Geest JN, van der Lijn F, et al. Determinants of 62. Morrison S, Colberg SR, Parson HK, Vinik AI. Exercise improves gait, reaction cerebellar and cerebral volume in the general elderly population. Neurobiol Aging time and postural stability in older adults with type 2 diabetes and neuropathy. J 2012;33:2774–2781 Diabetes Complications 2014;28:715–722 45. Manor B, Newton E, Abduljalil A, Novak V. The relationship between brain 63. Allet L, Armand S, Golay A, Monnin D, de Bie RA, de Bruin ED. Gait volume and walking outcomes in older adults with and without diabetic peripheral characteristics of diabetic patients: a systematic review. Diabetes Metab Res Rev neuropathy. Diabetes Care 2012;35:1907–1912 2008;24:173–191 46. Hsu J-L, Chen YL, Leu JG, et al. Microstructural white matter abnormalities in 64. Florence SL, Hackett TA, Strata F. Thalamic and cortical contributions to type 2 diabetes mellitus: a diffusion tensor imaging study. Neuroimage 2012;59: neural plasticity after limb amputation. J Neurophysiol 2000;83:3154–3159 1098–1105 65. Selvarajah D, Wilkinson ID, Maxwell M, et al. Magnetic resonance neuro- 47. Fang P, An J, Tan X, et al. Changes in the cerebellar and cerebro-cerebellar imaging study of brain structural differences in diabetic peripheral neuropathy. circuit in type 2 diabetes. Brain Res Bull 2017;130:95–100 Diabetes Care 2014;37:1681–1688 48. Xia W, Wang S, Sun Z, et al. Altered baseline brain activity in type 2 diabetes: 66. Fischer TZ, Waxman SG. Neuropathic pain in diabetes–evidence for a central a resting-state fMRI study. Psychoneuroendocrinology 2013;38:2493–2501 mechanism. Nat Rev Neurol 2010;6:462–466 49. Wang ZL, Zou L, Lu ZW, et al. Abnormal spontaneous brain activity in type 67. Selvarajah D, Wilkinson ID, Gandhi R, Griffiths PD, Tesfaye S. Microvascular 2 diabetic retinopathy revealed by amplitude of low-frequency fluctuations: perfusion abnormalities of the thalamus in painful but not painless diabetic a resting-state fMRI study. Clin Radiol 2017;72:340.e1–340.e7 polyneuropathy: a clue to the pathogenesis of pain in type 1 diabetes. Diabetes 50. Diedrichsen J, Balsters JH, Flavell J, Cussans E, Ramnani N. A probabilistic Care 2011;34:718–720 MR atlas of the human cerebellum. Neuroimage 2009;46:39–46 68. Scott SH, Cluff T, Lowrey CR, Takei T. Feedback control during voluntary 51. Yang SQ, Xu ZP, Xiong Y, et al. Altered intranetwork and internetwork motor actions. Curr Opin Neurobiol 2015;33:85–94 functional connectivity in type 2 diabetes mellitus with and without cognitive 69. Lafond D, Corriveau H, Prince F. Postural control mechanisms during quiet impairment. Sci Rep 2016;6:32980 standing in patients with diabetic sensory neuropathy. Diabetes Care 2004;27: 52. van Duinkerken E, Schoonheim MM, IJzerman RG, et al. Altered eigenvector 173–178 centrality is related to local resting-state network functional connectivity in patients 70. Nardone A, Schieppati M. Group II spindle fibres and afferent control of with longstanding type 1 diabetes mellitus. Hum Brain Mapp 2017;38:3623–3636 stance. Clues from diabetic neuropathy. Clin Neurophysiol 2004;115:779–789 53. Dai W, Duan W, Alfaro FJ, Gavrieli A, Kourtelidis F, Novak V. The resting 71. Bunday KL, Bronstein AM. Locomotor adaptation and aftereffects in patients perfusion pattern associates with functional decline in type 2 diabetes. Neurobiol with reduced somatosensory input due to peripheral neuropathy. J Neurophysiol Aging 2017;60:192–202 2009;102:3119–3128 54. Manto M, Bower JM, Conforto AB, et al. Consensus paper: roles of the 72. Chiu HY, Hsu HY, Kuo LC, et al. How the impact of median neuropathy on cerebellum in motor control–the diversity of ideas on cerebellar involvement in sensorimotor control capability of hands for diabetes: an achievable assessment movement. Cerebellum 2012;11:457–487 from functional perspectives. PLoS One 2014;9:e94452 55. Doya K. Complementary roles of basal ganglia and cerebellum in learning and 73. DeMott TK, Richardson JK, Thies SB, Ashton-Miller JA. Falls and gait motor control. Curr Opin Neurobiol 2000;10:732–739 characteristics among older persons with peripheral neuropathy. Am J Phys Med 56. Lohse KR, Wadden K, Boyd LA, Hodges NJ. Motor skill acquisition across Rehabil 2007;86:125–132 short and long time scales: a meta-analysis of neuroimaging data. Neuro- 74. Scott SH. Optimal feedback control and the neural basis of volitional motor psychologia 2014;59:130–141 control. Nat Rev Neurosci 2004;5:532–546 57. Moran C, Phan TG, Chen J, et al. Brain atrophy in type 2 diabetes: regional 75. Morton SM, Bastian AJ. Cerebellar contributions to locomotor adaptations distribution and influence on cognition. Diabetes Care 2013;36:4036–4042 during splitbelt treadmill walking. J Neurosci 2006;26:9107–9116 58. Chen J, Zhang J, Liu X, et al. Abnormal subcortical nuclei shapes in patients 76. Roman de Mettelinge T, Delbaere K, Calders P, Gysel T, Van Den Noortgate N, with type 2 diabetes mellitus. Eur Radiol 2017;27:4247–4256 Cambier D. The impact of peripheral neuropathy and cognitive decrements on gait 59. van Duinkerken E, Schoonheim MM, Steenwijk MD, et al. Ventral in older adults with type 2 diabetes mellitus. Arch Phys Med Rehabil 2013;94: striatum, but not cortical volume loss, is related to cognitive dysfunction in 1074–1079 type 1 diabetic patients with and without microangiopathy. Diabetes Care 77. de Freitas PB, Lima KCA. Grip force control during simple manipulation 2014;37:2483–2490 tasks in non-neuropathic diabetic individuals. Clin Neurophysiol 2013;124: 60. Nunley KA, Ryan CM, Aizenstein HJ, et al. Regional gray matter volumes as 1904–1910 related to psychomotor slowing in adults with type 1 diabetes. Psychosom Med 78. Ruffieux J, Keller M, Lauber B, Taube W. Changes in standing and walking 2017;79:533–540 performance under dual-task conditions across the lifespan. Sports Med 2015;45: 61. Ryan JP, Aizenstein HJ, Orchard TJ, Nunley KA, Karim H, Rosano C. Basal 1739–1758 ganglia cerebral blood flow associates with psychomotor speed in adults with type 79. Buracchio T, Dodge HH, Howieson D, Wasserman D, Kaye J. The trajectory of 1 diabetes. Brain Imaging Behav 2018;12:1271–1278 gait speed preceding mild cognitive impairment. Arch Neurol 2010;67:980–986
You can also read