Case Report Clear cell chondrosarcoma of the talus in Von Hippel-Lindau disease: a rare tumor in an unusual location and uncommon co-presentation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int J Clin Exp Pathol 2020;13(2):266-271
www.ijcep.com /ISSN:1936-2625/IJCEP0105389
Case Report
Clear cell chondrosarcoma of the talus
in Von Hippel-Lindau disease: a rare tumor in
an unusual location and uncommon co-presentation
Min Jeong Song1, Kyu Yeoun Won1, Soonchan Park2
Departments of 1Pathology, 2Radiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University College
of Medicine, Seoul, Republic of Korea
Received November 24, 2019; Accepted January 23, 2020; Epub February 1, 2020; Published February 15, 2020
Abstract: Von Hippel-Lindau (VHL) disease is an autosomal dominant inherited tumor syndrome. Clear cell chon-
drosarcoma (CCCS) is a rare variant of chondrosarcoma. Here, we report a case of CCCS in the talus occurring in
a patient with VHL disease. A 32-year-old man presented with ankle pain for 2 years. MRI revealed a 4.2 cm mass
in the talus, and needle biopsy was performed. The patient underwent curettage but the final diagnosis was CCCS.
Adjuvant radiation therapy was performed without additional talectomy and the patient was alive without recurrence
for a follow-up period of 2 years. To our knowledge, this is the first case in the English medical literature of a co-
presentation of this rare disease and condition: i.e. CCCS with VHL disease in the unusual location of the talus. We
cautiously suggest that CCCS may be associated with VHL disease based on their histologic similarity.
Keywords: Clear cell chondrosarcoma, talus, Von Hippel-Lindau disease
Introduction of our knowledge, this is the first such case to
be reported in the English literature.
Clear cell chondrosarcoma (CCCS) is a rare vari-
ant of chondrosarcoma, first described by Unni Case presentation
et al in 1976 [1] and characterized by prolifera-
tion of tumor cells with clear cytoplasm. CCCS Clinical features
comprises approximately 2% of all chondrosar-
comas [2]. This tumor is most common in A 32-year-old man presented with right ankle
patients in the third to sixth decade, has a pre- pain for 2 years, with symptoms aggravated
dilection for men, and typically arises at the over the previous 5 months. He had already
ends of long bones [3]. undergone surgical removal of an hemangio-
blastoma in the medulla, and a bilateral partial
Von Hippel-Lindau (VHL) disease is an autoso- nephrectomy for clear cell renal cell carcinoma
mal dominant inherited tumor syndrome asso- 7 years prior, and a right adrenalectomy for
ciated with germline mutation of the VHL tumor pheochromocytoma 3 years prior. Cytogenetic
suppressor gene located on chromosome 3p25 analysis on peripheral blood at the time of the
[4]. It is characterized by the development of diagnosis for hemangioblastoma and renal cell
capillary hemangioblastoma of the central ner- carcinoma indicated VHL disease. On the initial
vous system and retina, clear cell renal cell car- bone scan during a metastasis work-up for the
cinoma, pheochromocytoma, and pancreatic hemangioblastoma and renal cell carcinoma
and inner ear tumors [4]. VHL disease is es- that were treated 7 years previously, a focal
timated to occur at rates of 1:36,000 to mildly increased uptake was observed in the
1:45,500 of the population [5]. talus, but this appeared non-specific. Two years
later, a follow-up bone scan revealed a focally
We experienced an extremely rare case of increased uptake in the right talus compared to
CCCS in the talus with VHL disease. To the best the previous initial bone scan (Figure 1G) and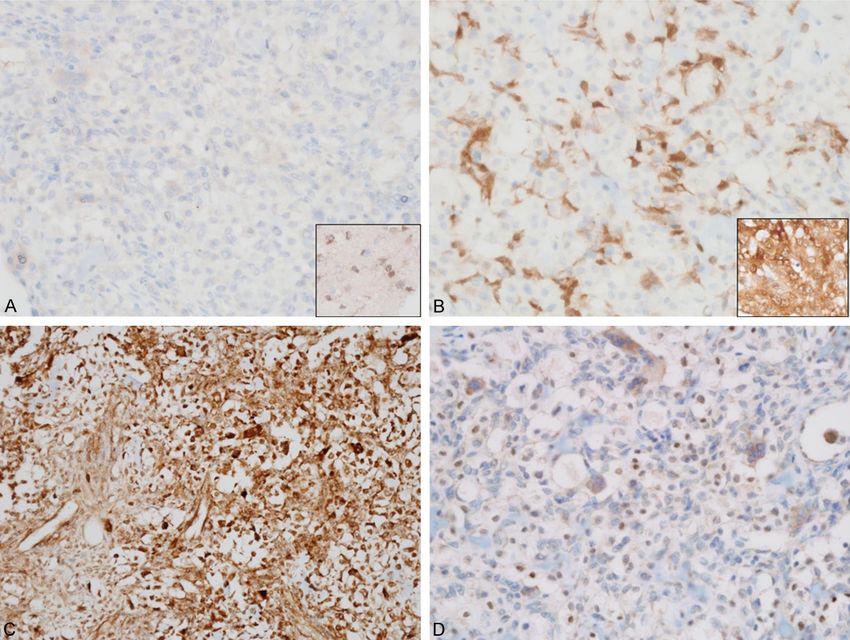
Clear cell chondrosarcoma in VHL disease Figure 1. Radiologic findings. (A-F) Axial T1 weighted (A) and sagittal fat-saturated T2 weighted (B) images show a well-defined 0.8 cm, round mass with intermediate signal intensities eccentrically located in the right talar neck. (C) It shows prominent enhancement on sagittal enhanced fat-saturated T1 weighted image. Axial T1 weighted (D) and sagittal fat-saturated T2 weighted (E) images taken 5 years later show a slightly lobulated expansile 4.4 cm mass in the medial aspect of the talus. (F) The mass shows strong enhancement on sagittal enhanced fat-saturated T1 image. (G, H) Bone scans show focal increased uptake in the right talus initially (G) and an increased extent of hot uptake after 5 years (H), suggesting progression of the bone tumor. the patient underwent magnetic resonance scans over 5 years revealed a slowly growing imaging (MRI). A round, eccentrically located, mass in the talus (Figure 1H) and the last MRI avidly-enhanced, 0.8 cm mass was detected in revealed a well-marginated, slightly lobulated the right talar neck with a sclerotic rim on T1 bony mass in the medial aspect of the talus, and T2 weighted images (Figure 1A-C). Under measuring about 4.4 × 2.0 × 4.2 cm (Figure the impression of a benign bone tumor such as 1D-F). The mass showed slightly inhomoge- osteoid osteoma or involvement of hemagio- neous intermediate to high signal intensity with blastoma, the clinician decided to proceed with slightly inhomogeneous solid enhancement, close follow-up observation. Follow-up bone containing focal hyper and low signal lesions. 267 Int J Clin Exp Pathol 2020;13(2):266-271
Clear cell chondrosarcoma in VHL disease
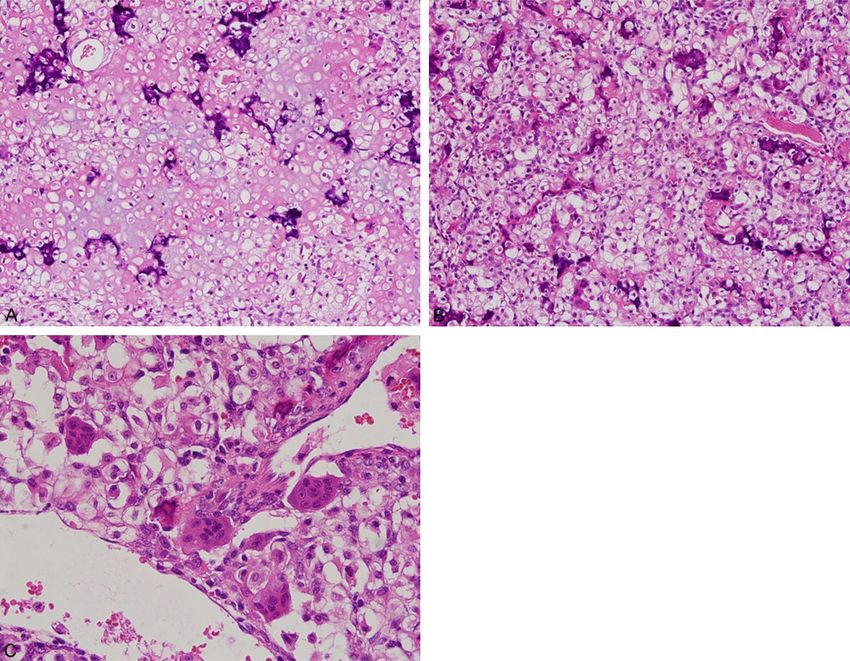
Figure 2. Microscopic findings. A. Low pow-
er photomicrograph shows sheets of clear
cells with cartilaginous stroma. B. Sheets
of clear cells are admixed with seams of
woven bone. C. Osteoclastic type giant cells
are scattered throughout the clear cells.
The radiologic impressions were primary bone Osteoclast-like giant cells were occasionally
tumor such as giant cell tumor, chondroblasto- present (Figure 2C). Mature hyaline cartilage
ma, or osteoblastoma and less likely metasta- was occasionally identified. No cystic changes
sis from renal cell carcinoma. A needle biopsy were noted.
was performed and the tumor was initially diag-
nosed as chondroblastoma. After bone curet- Immunohistochemistry
tage, the diagnosis was changed to clear cell
chondrosarcoma. Considering the patient’s his- Tissues were fixed in buffered 10% formalin
tory of renal cell carcinoma, no additional sur- with decalcified solution and embedded in par-
gery for the talus was performed but additional affin. The tissue blocks were sectioned at a
radiation therapy was given. There has been no thickness of 4 μm and mounted on precoated
evidence of disease recurrence for 2 years. glass slides. The sections were deparaffinized,
rehydrated and rinsed in distilled water. Im-
Pathologic features munohistochemical staining was performed for
HIF1α (1:10,000, EPITOMICS, Cambridge, UK),
Grossly, the specimen was fragmented, pinkish IDH1 (1:100, DIANOVA, Hamburg, Germany),
brown, and soft but partly gritty. Microscopically, VEGF (1:500, PHARMINGEN, San Diego, CA),
the tumor consisted of sheets of cells with P16 (1:500, SANTACRUZ Biotechnology, Santa
large, round nuclei with central nucleoli. The Cruz, CA), and S-100 protein (1:200, ZYMED,
cells had pale, clear or slightly eosinophilic San Francisco, CA) using the Ventana NX auto-
cytoplasm with distinct cytoplasmic mem- mated immunohistochemistry system (Ventana
branes (Figure 2A). The nuclear atypia was Medical Systems, Tucson, AZ, USA). The tumor
mild, and mitotic figures were seldom observed. showed diffuse strong positivity for S-100 pro-
Fine benign osteoid formation or woven bone tein (data not shown) and, VEGF, and nuclear
was seen among the clear cells (Figure 2B). positivity for HIF1α with cytoplasmic staining of
268 Int J Clin Exp Pathol 2020;13(2):266-271Clear cell chondrosarcoma in VHL disease
Figure 3. The tumor cells show immunonegativity for IDH1 (A) and p16 (B). The insets are control tissues: astrocy-
toma and cervical squamous cell carcinoma, respectively. (C, D) The tumor cells shows immunopositivity for VEGF
(C) and HIF-1α (D), suggesting an indirect association of VHL disease.
osteolclast-like giant cells. No IDH1 and p16 monary metastases and died [8]. However,
immunopositive tumor cells were identified Present et al [2] reported that none of their
(Figure 3A-D). patients with marginal or intralesional excision
had recurrence during 5 to 9 years of follow-up.
Discussion Based on the 5-year survival rates of stage I
renal cell carcinoma is known to 81%, clear cell
CCCS has been reported in long tubular bones chondrosarcoma will not affect the survival of
including the skull, spine, hands and feet. The our patient. Thus, conservative surgery with
most frequent locations are the proximal femur adjuvant radiation therapy was acceptable in
(56%) and the head and neck area [6]. Only two this case.
cases of CCCS arising in talus have been
reported in English [2, 7]. Recognition of the Radiologically, CCCS is typically lytic, although
usual site involvement of CCCS is important the lesion has areas of dense mineralization.
to prevent underdiagnosis and insufficient Because this tumor extends to the epiphysis
treatment. and articular cartilage, lytic lesions mimic chon-
droblastoma or giant cell tumor of the bone.
Generally, CCCS belongs to the class of low Giant cell tumor of bone is easily excluded on
grade sarcomas, and en-bloc excision with microscopic examination. Histologically, major
clear margin is usually curative. Marginal exci- differential diagnoses are chondroblastoma,
sion or curettage has been reported to have a and chondroblastic osteosarcoma. In contrast
high rate of local recurrence (86%) [3], with a to the marked pleomorphism, nuclear hyper-
number of patients eventually developing pul- chromasia, and brisk mitotic activity of chon-
269 Int J Clin Exp Pathol 2020;13(2):266-271Clear cell chondrosarcoma in VHL disease
droblastic osteosarcoma, the cells in CCCS are Similar to conventional chondrosarcoma, RB
monomorphic and mitoses are rare. Compared pathway is affected in the vast majority of
to chondroblastoma, obviously malignant chon- CCCS, primarily through the loss of p16 protein
drocytes and large cells with clear cytoplasm expression [13]. In addition, it has been report-
often in a background of ossified bone are ed that mutations in IDH1/2 are absent in clear
observed in CCCS. cell chondrosarcoma [14]. More specifically,
protein expression of IDH1 by immunohis-
VHL disease is an autosomal dominant multi- tochemistry correlates with mutation in the
system syndrome associated with germline IDH1 R132H gene (sensitivity 98% and specific-
mutation of the VHL tumor suppressor gene at ity 100%) [15]. Our case showed also immuno-
chromosome 3p25 [4]. The loss of functional negativity for p16 and IDH1, sharing common
VHL protein contributes to tumorigenesis in the genetics with general clear cell chondro-
central nervous system and internal organs, sarcoma.
including the kidney, adrenal gland, and pan-
creas [4]. The current patient showed synchro- In conclusion, clear cell chondrosarcoma can
nous and metachronous existence of three pri- occur in VHL syndrome patients, and this is the
mary tumors: hemangioblastoma, clear cell first case to be reported in the English medical
renal cell carcinoma, and pheochromocytoma. literature of this extremely rare combination,
The relationship between VHL disease and i.e. a rare subtype of chondrosarcoma, unusual
CCCS is not well defined, because only one location of the talus, and association with VHL
case report, which described chondrosarcoma disease.
and not clear cell chondrosarcoma, has been
reported for VHL disease patient [9]. The mech- Acknowledgements
anism of VHL syndrome in tumorigenesis
involves hypoxia inducible factors (HIF1 and This work was supported by a grant from
HIF2). Either hypoxia or absent or inactive VHL National Research Foundation of Korea in
protein results in stabilization of HIF1 and HIF2, 2017 (2017R1C1B5076919).
which then act as transcription factors that
initiate the cellular cascade for a hypoxic Disclosure of conflict of interest
response. This hypoxic response affects glu-
None.
cose uptake and metabolism, angiogenesis,
extracellular matrix formation, chemotaxis and Address correspondence to: Dr. Soonchan Park,
cell proliferation, and then activates down- Department of Radiology, Kyung Hee University
stream targets, including vascular endothelial Hospital at Gangdong, Kyung Hee University College
growth factor (VEGF), platelet derived growth of Medicine, 892, Dongnam-ro, Gangdong-gu, Seoul
factor (PDGF), and transforming growth factor 05278, Republic of Korea. Tel: 82-2-440-6952; Fax:
α [10]. Lin et al [11] reported that hypoxia
82-2-440-6932; E-mail: mdpark96@naver.com
induces HIF1α and VEGF expression in chon-
drosarcoma and Chen et al [12] reported that References
decreased VHL protein expression correlates
with high grade chondrosarcoma. Our current [1] Unni KK, Dahlin DC, Beabout JW and Sim FH.
case showed immunoreactivity for HIF1α and Chondrosarcoma: clear-cell variant: a report of
VEGF, indirectly suggesting a relationship be- sixteen cases. J Bone Joint Surg Am 1976; 58:
tween VHL disease and clear cell chond- 676-683.
rosarcoma. [2] Present D, Bacchini P, Pignatti G, Picci P,
Bertoni F and Campanacci M. Clear cell chon-
Clear cell chondrosarcoma also shares histo- drosarcoma of bone: a report of 8 cases.
logic similarity with other VHL disease-related Skeletal Radiol 1991; 20: 187-191.
[3] Bjornsson J, Unni KK, Dahlin DC, Beabout JW
tumors including epithelioid cell with clear cyto-
and Sim FH. Clear cell chondrosarcoma of
plasm and increased vascularity. Therefore, we bone: observations in 47 cases. Am J Surg
cautiously suggest that clear cell chondrosar- Pathol 1984; 8: 223-230.
coma in VHL syndrome is not an incidental [4] Lonser RR, Glenn GM, Walther M, Chew EY,
coexistence, but rather that the VHL mutation Libutti SK, Linehan WM and Oldfield EH. von
may be related to the tumorigenesis of clear Hippel-Lindau disease. Lancet 2003; 361:
cell chondrosarcoma. 2059-2067.
270 Int J Clin Exp Pathol 2020;13(2):266-271Clear cell chondrosarcoma in VHL disease
[5] Maddock IR, Moran A, Maher ER, Teare MD, [12] Chen C, Zhou H, Liu X, Liu Z and Ma Q. Reduced
Norman A, Payne SJ, Whitehouse R, Dodd C, expression of von Hippel-Lindau protein corre-
Lavin M, Hartley N, Super M and Evans DG. A lates with decreased apoptosis and high chon-
genetic register for von Hippel-Lindau disease. drosarcoma grade. J Bone Joint Surg Am 2011;
J Med Genet 1996; 33: 120-127. 93: 1833-1840.
[6] Fletcher CDM, Bridge JA, Hogendoorn P and [13] Meijer D, de Jong D, Pansuriya TC, van den
Mertens F. WHO classification of tumors of soft Akker BE, Picci P, Szuhai K and Bovee JV.
tissue and bone. Lyon: IARC; 2013. Genetic characterization of mesenchymal,
[7] Ogose A, Motoyama T, Hotta T, Emura I, Inoue clear cell, and dedifferentiated chondrosarco-
Y, Morita T and Watanabe H. Clear cell chon- ma. Genes Chromosomes Cancer 2012; 51:
drosarcomas arising from rare sites. Pathol Int 899-909.
1995; 45: 684-690. [14] Nishio J, Reith JD, Ogose A, Maale G, Neff JR
[8] Itala A, Leerapun T, Inwards C, Collins M and and Bridge JA. Cytogenetic findings in clear cell
Scully SP. An institutional review of clear cell chondrosarcoma. Cancer Genet Cytogenet
chondrosarcoma. Clin Orthop Relat Res 2005; 2005; 162: 74-77.
440: 209-212. [15] Jabbar KJ, Luthra R, Patel KP, Singh RR,
[9] Marinozzi A, Papapietro N, Barnaba SA, Di Goswami R, Aldape KD, Medeiros LJ and
Martino A, Tonini G and Denaro V. Chond- Routbort MJ. Comparison of next-generation
rosarcoma of the iliac wing in Von Hippel- sequencing mutation profiling with BRAF and
Lindau disease. J Exp Clin Cancer Res 2007; IDH1 mutation-specific immunohistochemis-
26: 599-601. try. Am J Surg Pathol 2015; 39: 454-461.
[10] Kaelin WG Jr. The von Hippel-Lindau tumour
suppressor protein: O2 sensing and cancer.
Nat Rev Cancer 2008; 8: 865-873.
[11] Lin C, McGough R, Aswad B, Block JA and Terek
R. Hypoxia induces HIF-1alpha and VEGF ex-
pression in chondrosarcoma cells and chon-
drocytes. J Orthop Res 2004; 22: 1175-1181.
271 Int J Clin Exp Pathol 2020;13(2):266-271You can also read

















































