Clinical case - www.jaccrafrica.com ISSN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of african clinical cases and reviews / Journal africain des cas cliniques et revues
www.jaccrafrica.com ISSN: 1859-5138 Open access
Clinical case
Sphenoidal aspergillosis, rare cause of pseudo-tumor of the sellar region: case report
Aspergillose sphénoïdale, cause rare de pseudo tumeur de la région sellaire : à propos
d’un cas
AB Thiam1, M Mbaye*1, M Thioub1, LF Barry1, SB Kinata-Bambino2, EHC Ndiaye Sy1, M Faye1, D
Wague1, N Ndoye1, MC Ba1, PM Oussou-Nguiet3, SB Badiane1
Abstract should be provided in order to avoid functional or
Background: Isolated sphenoidal aspergillosis is vital complications
an uncommon pathology of slow evolution and Keywords: invasive aspergillosis, aspergillus
potentially severe due to the risk of neuro-meningeal fumigatus, sphenoidal sinus, pseudo tumor.
and orbital extension. Its diagnosis is difficult and
Résumé
often delayed to complications stage. The treatment
Introduction : L’aspergillose sphénoïdale isolée
relies on medical and surgical approaches.
est une pathologie rare d’évolution lente et
Case description: 35-year-old patient with retro-
potentiellement grave vu le risque d’extension
orbital headache, decreased right visual acuity
neuro-méningée et orbitaire. Son diagnostic est
with palpebral ptosis and ipsilateral diplopia, left
difficile et souvent posé au stade de complications.
hemiparesis and focal seizures of the left hemibody.
Son traitement est médico-chirurgical.
The examination found a right monocular blindness
Observation : patiente de 35 ans ayant consulté pour
with oculomotor impairment (III and VI) and left
des céphalées retro orbitaires, baisse de l’acuité
pyramidal deficiency syndrome. Brain imaging (CT/
visuel droite avec ptose palpébrale et diplopie
MRI) outlined an intra-sphenoidal process strongly
ipsilatérale, hémiparésie gauche et crises focales de
suggestive of invasive sphenoidal fungal sinusitis,
l’hémicorps gauche. L’examen retrouvait une cécité
confirmed by anatomopathological examination.
mono oculaire droite avec atteinte oculomotrice (III
She had an endoscopic biopsy followed by medical
et VI) et un syndrome pyramidal déficitaire gauche.
treatment for 12 weeks.
L’imagerie cérébrale (TDM/IRM) objectivait un
Conclusion: Sphenoidal aspergillosis is one of the
processus intra sphénoïdal fortement évocateur de
differential diagnoses of sphenoidal tumors in the
sinusite fongique sphénoïdale invasive, confirmée
immunocompetent patient. Its diagnosis is difficult
par l’examen anatomopathologique. Elle a bénéficié
and delayed to the stage of complications. An early
d’une biopsie par voie endoscopique suivi d’un
treatment involving surgery and medical approach
traitement médical pendant 2
Jaccr Africa 2020, Vol 4, Num 2 www.jaccrafrica.com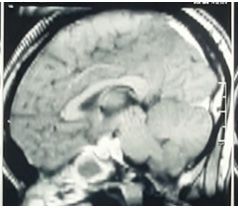
AB Thiam et al. Jaccr Africa 2020; 4(2): 227-231
Conclusion : l’aspergillose sphénoïdale est l’un des blindness. The fundus showed a right-sided optic
diagnostics différentiels des tumeurs sphénoïdales atrophy. The neurological examination also outlined
chez l’immunocompétent. Son diagnostic est a left pyramidal deficiency syndrome at 4/5 in the
difficile et souvent posé au stade de complications. upper limb and 3/5 in the lower limb. Cerebral CT
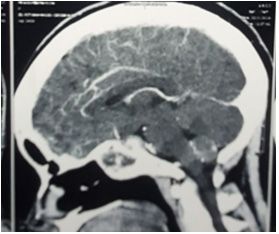
Le traitement doit être précoce associe chirurgie et scan (Fig. 1) showed, on the one hand, a clear filling
un traitement médical afin d’éviter des complications of the sphenoidal sinus with very dense material
fonctionnelles voire vitales and calcifications resulting in partial erosion of
Mots-clés : aspergillose invasive, aspergillus the right wall with extension towards the upper
fumigatus, sinus sphénoïdal, pseudo tumeur. orbital fissure, at the level of the cavernous sinus
and the left lateral-pontic region. On the other hand,
we observed a range of old cortical hypodensity
Introduction under the parieto-tempo-occipital right cortex with
ischemic appearance. Brain magnetic resonance
Aspergillosis is a mycotic infection whose most imaging (MRI) (Fig. 2) outlined an intra-sphenoidal
commonly isolated germ is Aspergillus fumigatus. process in hypo signal T1 and T2 with peripheral
Usually this filamentous fungus colonizes the enhancement after gadolinium injection. This
maxillary and ethmoidal sinuses. Human-to- process extends to the right cavernous compartment,
human transmission is mostly through the air [1]. stenosing the intracavernous carotid artery and
Its intracranial location remains rare. Isolated causing a subacute infarction in the right sylvic
sphenoidal aspergillosis is an uncommon condition region. The process also extends to the posterior
that is potentially serious given the risk of neuro- region in the form of a multi-located formation,
meningeal and orbital extension. Although it is strongly enhanced on the periphery after injection
more frequent in immunocompromised patients, against the cleavus. There was no biological
the damage in immunocompetent patients has been inflammatory syndrome or hyperleukocytosis. Renal
described [2]. Diagnostic wandering is due to the function was normal and HIV serology negative.
absence of specific symptomatology. We report one She had a broad endoscopic endonasal biopsy. The
case of isolated invasive sphenoidal aspergillosis opening of the sphenoidal sinus reveals a reddish
revealed by neurological and ophthalmological lesion that was easily removed with inflammatory
signs. nests and a clear purulent flow. The immediate
postoperative suites was marked by transient
Clinical case diabetes insipidus. The anatomopathological study
was suggestive of invasive aspergillosis. The patient
It was about a 35-year-old patient with no particular was put on antifungal treatment (Voriconazole
medical history who was admitted for retro- ®) and antiepileptic treatment (phenobarbital).
orbital headache, decreased right visual acuity The evolution was marked by the regression of
with palpebral ptosis and ipsilateral diplopia, oculomotor paralysis and headache. However, both
left hemiparesis and simple tonic-clonic focal hemiparesis and right monocular blindness were
seizures of the left hemibody. The clinical course persistent.
gradually evolved over eight months. Neurological
and ophthalmological examination revealed right
palpebral ptosis with oculomotor paralysis (III and
VI), reactive mydriasis and ipsilateral monocular
Jaccr Africa 2020, Vol 4, Num 2 www.jaccrafrica.com
AB Thiam et al. Jaccr Africa 2020; 4(2): 227-231
frequency is on average around 50 years of age. The
most common contributing factors comprise an
underlying immunocompromised condition (AIDS,
long-term corticosteroids or immunosuppressive
drugs, alcoholism, antituberculosis treatment);
local factors such as secretion retention by
ostial dysfunction, intra-sinusal foreign bodies;
environmental factors, such as a hot weather, as it is
in Dakar is also described [1].
The long time-limit management in our context
is simply explained by the fact that clinically, the
Figure 1: Injected Brain CT scan; sagittal signs of sphenoidal aspergillosis are silent and non-
reconstruction: hyperdense intra sphénoïdal lesion. specific, leading to late diagnosis. The main sign
remains retro-orbital headaches that may combine
anterior and/or posterior purulent rhinorrhea and
nasal obstruction [8]. In invasive forms, the clinical
course is dominated by ophthalmological features
(diplopia, ptosis, exophthalmia, ophthalmoplegia)
by orbital extension and invasion of the cavernous
sinus and neuroendocrine signs due to contiguous
invasion of neuro-meningeal structures adjacent
to the sphenoidal sinus, leading to a very serious
condition [9; 10].
Figure 2: T1 SAG MRI: sphenoidal lesion with On radiological approach, standard images are
invasion of the sellar compartment. often unremarkable. CT-scan of the sinuses with
injection is the referential examination. The
Discussion diagnosis is conjured up in the presence of a more
or less heterogeneous hyperdense filling of the
Data on pseudo-tumor invasive sinus aspergillosis sinus, which does not enhance after iodine injection
are very limited in the literature. Some data are and sometimes including a calcium or metal density
collected from explorations of information about image matching with calcium salts and other heavy
isolated sphenoidal sinusitis on the one hand metals (lead, copper, iron, manganese) built up by
and maxillary aspergillosis on the other hand. fungus and a thickening of the walls suggesting a
[3; 4] Patients who develop an invasive pattern chronic form [1; 11]. Orbital or meningo-encephalic
with cavernous sinus involvement are often invasion will be best specified by MRI. It is more
immunocompromised but invasive or pseudo-tumor specific in pseudo tumor forms, showing a non-
forms in immunocompetent patients is possible enhanced heterogeneous lesion on the T1 and T2
as we report in our observation and is described sequences after injection of gadolinium, this aspect
in the literature. [5; 6] The sphenoidal location may vary according to the viscosity and hydration
is exceptional [7]. Indeed, aspergillar spores state of the aspergillar content. Bone CT can be
generally colonize the proximal para-nasal sinuses performed to look for sinus wall lysis in invasive
(maxillary, ethmoidal and frontal sinuses). The peak forms [9; 12]. It is recommended to combine
Jaccr Africa 2020, Vol 4, Num 2 www.jaccrafrica.comAB Thiam et al. Jaccr Africa 2020; 4(2): 227-231
the two investigations for a better diagnostic intracavernous internal carotid artery and by optic
approach [1; 13]. Differential diagnosis usually atrophy.
occurs with bacterial sinusitis, sphenoidal tumors,
granulomatous inflammatory diseases, particularly Conclusion
tuberculosis in endemic areas, infra-solar cell
tumors and, exceptionally, thrombosis of giant Invasive sphenoidal aspergillosis is a rare disease.
carotid aneurysms [7; 14]. However, the presence Its diagnosis is most often made at the stage of
of metallic opacity lend support to the diagnosis. neurological and ophthalmological complications.
Diagnostic confirmation is obtained by direct Imaging lends a major support to diagnosis and
mycological examination of the aspergillar pus and extension assessment. The hyperdense aspect on
by anatomopathological examination, pointing out the CT, the presence of ferromagnetic elements on
the presence of branched, parallel-edged septate MRI and bone lysis are very suggestive of invasive
mycelial filaments, as we do in our series [1; 13]. aspergillar involvement. The treatment is medical
The serology is mostly negative, likewise in our and surgical. Its early onset and over a long period
patient. In the absence of an effective diagnosis or of time is required.
treatment, functional or vital complications may
occur such as the rupture of the intracavernous
internal carotid artery, pan-hypopituitarism or the *Corresponding author :
central nervous system involvement [8; 15]. Maguette Mbaye
Therapeutic approach maguette.mbaye8@gmail.com
The treatment of invasive aspergillosis of the
sphenoidal sinus is both medical and surgical. Available online : April 27, 2020
The endoscopic route should be preferred [16],
if possible with a computer-assisted navigation 1 Neurosurgery department, Fann teaching hospital, Dakar,
Senegal.
system given the proximity of noble structures. Its
2 Department of surgery, division of neurosurgery, Brazzaville
morbidity and mortality rate is low. The treatment academic hospital, Republic of Congo.
of choice is Voriconazole® 200mg twice daily for 3 Neurology department, faculty of health sciences Marien
12 weeks. We would rather use it, when possible, Ngouabi, Brazzaville Academic Hospital, Republic of Congo
than Amphotericin B which has renal toxicity [2].
Prolonged intra-venous treatment is ideal. In our © Journal of african clinical cases and reviews 2020
context, the absence of injectable form and medical
coverage did not allow the use of the parenteral Conflict of interest : None
route in our patient. She received oral antifungal
treatment.
Evolution
Functional recovery is proportionally related to
the degree of initial severity of the neurological References
impairment. They can range from a few days to
[1] Crambert A, Gauthier J, Vignal R, Conessa C, Lombard
several months (up to a year and a half) [17]. In B. [Invasive aspergillosis of sphenoidal sinus in a patient in
our patient, the persistence of hemiparesis and Djibouti, revealed by palsy of cranial nerves: a case report].
monocular blindness is explained by the extent of Medecine et Sante Tropicales. 2013 May;23(2):217-220. DOI:
cerebral infarction caused by occlusion of the right 10.1684/mst.2013.0184.
Jaccr Africa 2020, Vol 4, Num 2 www.jaccrafrica.comAB Thiam et al. Jaccr Africa 2020; 4(2): 227-231
[2] Baumann A, Zimmerli S, Hausler R, Caversaccio M. 83.
Invasive sphenoidal aspergillosis : successful treatment with [16] Yu H, Li H, Chi F, Dai C, Zhang C, Wang Z. Endoscopic
sphenoidotomy and voriconazole. ORL J Otorhinolaryngol surgery with powered instrumentation for isolated spenoid
Relat Spec 2007 ; 69 : 121-6. sinus disease. ORL J Otorhinolaryngol Relat Spec 2006 ; 68
[3] Delbet C, aspergillaires des sinus maxillaires. In: EMC : 129-34.
Médecine buccale. Paris: Elsevier Masson SAS; 2011 [28- [17] Li-Ang Lee MD, Ta-Jen Lee MD, Chi-Che J, Huang MD.
275-I-10. Endoscopic Sinus Surgery for Solitary Abducens Palsy in
[4] Thery A, Espitalier F, Cassagnau E, Durand N, Malard O. Patients with isolated Sphenoid Sinus Disease: Report of four
Clinical features and outcome of sphenoid sinus aspergillosis: Cases. Chang Gung Med J 2002 ; 10 : 689-93. .
a retrospective series of 15 cases. Eur Ann Otorhinolaryngol
Head Neck Dis 2012; 129:179–84.
[5] Abir B, Abouchadi A, Hamama J, Oukabli M, Nassih M,
Rzin A. Aspergillose invasive du sinus maxillaire chez un How to cite this article
patient immunocompétent. Rev Stomatol Chir Maxillofac
AB Thiam, M Mbaye, M Thioub, LF Barry, SB Kinata-
2012;113: 127–30.
Bambino, EHC Ndiaye Sy et al. Sphenoidal aspergillosis, rare
[6] Palacios E, Valvassori G, D’Antonio M. Aggressive
invasive fungal sinusitis. Ear Nose Throat J 2000; 79:842. cause of pseudo-tumor of the sellar region: case report. Jaccr
[7] Petrick M, Honegger J, Daschner F, Feuerhake F, Zentner Africa 2020; 4(2): 227-231
J. Fungal granuloma of the sphenoid sinus and clivus in a
patient presenting with cranial nerve III paresis: Case report
and review of the literature. Neurosurgery 2003;52:955-9.
[8] Barry B, Bouchaud O, Vittecoq D, Minoz- zi C, Coulaud
JP, Gehanno P. Sinusites aspergillaires invasives chez les
patients infectés par le virus de l’immunodéficience humaine.
Ann Otolaryngol Chir Cervicofac 1999;116:237-41.
[9] Haegelen C, Godey B, Riffaud L, Le Gall F, Le Page E,
Morandi X. Syndrome du si- nus caverneux par aspergillose
isolée du sinus sphénoïdal. Rev Neurol (Paris) 2003; 2,209-11.
[10] Haidara A, Broalet E, Zunon-Kypre y, Ba Zeze V.
L’aspergillose de la loge sellaire stimulant une tumeur
hypophysaire : à propos d’un cas. Rev. Col. Odonto-Stomatol.
Afr. Chir. Maxillo-fac., 2008 ; 15 : 53-6.
[11] Barry B, Topeza M, Géhanno P. Rôle de l’environnement
dans la survenue d’une aspergillose naso-sinusienne. Ann
Otolayngol Chir Cervicofac 2002;119:170-3.
[12] Dubey A, Patwardhan RV, Sampth S, Santosh V, Kolluri
S, Nanda A. Intracra- nial fungal granuloma: analysis of
40 patients and review of the literature. Surg Neurol 2005;
63:254-60.
[13] I Kamaoui, H Jerguigue, K Znati, R Latib, A El Quessar,
N Chakir et al. Aspergillose sphénoïdale révélée par des
signes neuro-ophtalmologiques : à propos d’un cas. J Radiol
2007;88:901-3.
[14] Ishibashi T, Kikuchi S. Mucocele-like lesions of the
sphenoid sinus with hypo- intense foci on T2-weighted
magnetic resonance imaging. Neuroradiology 2001; 43: 1108-
11.
[15] Klossek JM, Peloquin L, Fourcroy PJ, Ferrie JC, Fontanel
JP. Aspergillomas of the sphenoid sinus: A series of 10 cases
treated by endoscopic sinus surgery. Rhinology 1996;34:179-
Jaccr Africa 2020, Vol 4, Num 2 www.jaccrafrica.comYou can also read