Clinical Specialties Advancing - AOPA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Volume 1 / Issue 2 / December 2016 DISCOVER THE ORTHOTIC &
www.aopa.org.au
THE AOPA PROSTHETIC PROFESSION
Advancing Case Studies & How you can promote
Clinical Specialties P&O Practical Guides Prosthetics and Orthotics
NEW
RESOURCE:
SUPPORTING PRIVATE
PRACTICE
THE AOPA REVIEW
Welcome
After the success of the first edition of your new-look
Review, the Editorial Committee, National Office and
AOPA Board are thrilled to present the December edition.
The theme for this edition is ‘Clinical Specialties in
Prosthetics and Orthotics’. Inside you’ll find the new
AOPA Clinical Specialty Resource that promotes the
amazing diversity of roles orthotist/prosthetists perform,
as well as feature articles that provide an insight into
the vital work AOPA members conduct each day. Read
more about how you can use this new range of tools to
promote the profession and advance P&O on page 7.
Discover more about a range of clinical topics including
Cheneau bracing, plantar fasciitis management and
developmental dysplasia of the hip in a range of case
studies, clinical notes and research articles. Then find
out how to start-up your own private practice with
the release of the AOPA Private Practice Resource that
provides practical and easy-to-follow points to consider
when developing a new business. Read about how you
can support your clients with a new range of tools, from
Limbs 4 Life, available for those living with limb-loss.
Catch up on P&O education with an introduction to
We encourage you to submit articles or content by
the University of Sunshine Coast program and hear
contacting any member of the Editorial Committee
more about the Rio 2016 Paralympics from a team of
or the National Office. We also encourage you to
Australian P&O’s. Finally, read about the workshops and
suggest ideas or tell us what you’d like to see published
presentations that you may have missed at the 2016
in upcoming editions. This is your member magazine
AOPA Congress.
and we want to provide high quality content that is
We want to hear from you! valuable to you.
Help us make The AOPA Review become the leading Guidelines for submitting articles are available on the
source of information relating to the orthotic/prosthetic AOPA website: http://www.aopa.org.au/publications/
profession in Australia. Help us showcase the valuable the-aopa-review
contribution our profession makes to the Australian
healthcare system and highlight the unique skill sets of Earn extra CPD points
our practitioners. Get in touch if you’d like to submit an You can now gain some extra CPD points just by reading
article for publication. Suggested articles include: The Review. A brief online quiz will be available to
• Feature articles on clinical topics complete for each edition. Make sure you keep an eye
• Case studies out for one of our upcoming member emails which will
contain details of how to complete this quiz. Simply
• Research articles
follow the links and correctly answer the quiz questions
• Exploration of issues that impact our profession in to earn valuable CPD points!
Australia
• Introductions to new orthotic/prosthetic technologies Thank you to each of our contributors to the second
• Member reviews of new technologies edition of The Review. We hope you enjoy reading it and
find each of the articles as interesting and informative as
• Overviews of education events
we did!
• Contributions from other allied health professionals
and related disciplines The AOPA Editorial Committee
For further information on items in this Review
THE AOPA
please contact:
Editor, AOPA Office,
The AOPA Review is produced in June and December PO Box 1219, Greythorn VIC 3104
and is sent out to all AOPA members. Please contact
the editor if you would like any information regarding Ph: 1300 668 194 / (03) 9816 4620
advertising rates. The inclusion of advertising in no Fax: (03) 9816 4305
way implies endorsement by the Association. E-Mail: admin@aopa.org.au
CHAIR’S REPORT
Since the mid-year and the first publication of our the outstanding and tireless work she has performed
new review magazine, much activity has occurred. over the past years. Our association and profession
In line with our strategic plans and evolution over the would not be as well placed without Jackie’s quality
past 5 years, our association continues its transition contribution.
from a focus on internal infrastructure development,
to external directed activities. Our aim to engage We hope you enjoy the second edition of the Review.
with end-users and external policy agencies continues The AOPA board and office team have received
to gather momentum and deliver outcomes. In line numerous positive comments from members in response
with our strategic plan, we continue to work on to the first edition, following the change to the
internal projects and the past 6-months has seen us regularity, quality, format and size of the publication.
strengthen our self-regulation platform. We are delighted to deliver our second edition, focusing
on Clinical Specialties in Orthotics and Prosthetics.
Our office team continue to foster cooperation The Review will continue to represent a central and
and work diligently with consumer groups, along foundational vehicle in our aim to communicate,
with external government and funding agencies, educate & inform. We hope the publication meets
to improve end user access to our services. We the memberships needs following our member survey
have been making solid progress and our aim is performed early in 2016.
to have the opportunity to deliver the appropriate
Every 4 years sees the running of the Paralympic games,
and required services to those members of the
and we have recently seen the completion of the 2016
Australian community requiring prosthetic & orthotic
event in Brazil. The increasing visibility of the Paralympic
intervention. Those services are to be outcome
games continues to build awareness of the orthotic &
focused and evidence based, and deliver value to
prosthetic profession in Australia. Outstanding results
consumer and funder alike. Work continues with the
achieved by many of our athlete’s, and the media’s
private health insurance association, Medicare, NDIS,
desire to highlight athlete’s remarkable journeys, have
and multiple state-based agencies. In particular, our
provided many opportunities for the public to greater
office team continue to work closely with senior NDIS
understand the contribution our members make.
to support the roll-out of the program.
It has been a big year for our profession, and we are
We have just concluded our sixth and most successful
seeing major shifts in regulatory and funding platforms
Congress. The Congress saw in excess of 340
across the country. We continue to aim to support and
delegates in attendance, exceeding our prior record
guide the progression of our profession and the quality
attendance of just under 300. Sarah Anderson and
and accessibility of our services. On behalf of the board,
her dedicated and hard-working convening team,
I wish our membership a safe festive season, and look
delivered an outstanding three days of learning and
forward to a further year of
social activities, ably supported by our AOPA office
progress in 2017.
group. Our Congress continues to grow in quality
and scale, and it has now established itself as THE
event in the Australian P&O calendar for orthotist/ Yours respectfully,
prosthetists and our medical and allied health peers.
The number of international delegates, exhibitors,
presenters and keynote speakers continues to grow,
and we look forward to further progress next year
by proudly announcing the 2017 Congress will be
heading to the Melbourne tennis center.
The transformation of our governance platform
continues, and we are delighted to welcome Harvey Blackney
Melanie Dooley to the board. Melanie brings an Chair, AOPA Board
outstanding and much needed financial capability of Directors
to the board and our association, and will play a
vital role in planning and overseeing our financial
activities. We now have a full complement of board
members with three “non-industry” or independent
directors, and seven directors who are members of
the P&O profession. We also welcome Luke Rycken
to the office team, who is assuming the roles of
Jackie O’Connor in the advocacy portfolio, and Ella
Nicholson in the communications portfolio. Whilst
Ella will return next year following maternity leave,
we say farewell to Jackie and thank her sincerely for
4 / December 2016 / Volume 1 - Issue 2 / The AOPA Review
THOUGHTS FROM THE NATIONAL OFFICE
Hello members,
I hope you are enjoying the final moments of 2016 specialties and we encourage you to join us on
which I know has been a highly successful year for the social media via Facebook, Twitter and LinkedIn to
Association, the profession and individual members. disseminate the message as widely as possible.
This year seems to have disappeared quicker than
normal, which possibly indicates how busy the National As a membership association one of the
Office has been. The Office spends many months important measures of our growth and success is
focused on the National Congress, supporting the membership numbers and external engagement.
convener and convening committee and developing The increased engagement with students,
workshops, forums and resources for launch. The technicians and consumers at the AOPA congress
2016 Congress was our most successful event yet with is pleasing and indicates that people find
record numbers of delegates, sponsors and exhibitors connecting with the Association valuable. Our
and additional events. Of note was the highly success total membership numbers are also telling and
Best Business Practice in your Practice workshop and at the end of the 2016 renewal period, we are
the Leveraging Clinical Capacity Forum. These events pleased to report total member numbers of 446
were developed by the National Office team and aimed which has increased from 420 in April 2016. We
to challenge our thinking and support the growth welcome many new members and students to
and development of private practice in Australia. the Association and encourage you to contact the
Coinciding with these events was the launch of the National Office for assistance or support to access
AOPA Private Practice Resource Guide. This is now resources at any time.
available for members to download from the website In November, the National Board met to review
and offers extensive support for small and large private strategic progress against the 2015-17 Strategic
practices in areas such as insurance, establishing Plan. It has been a highly successful year for
referral networks and promoting your business. Please the Association with achievements in numerous
do not hesitate to provide feedback on this resource areas including: membership growth, delivery
and we hope that you find it valuable. of education events, development of member
I am also pleased to announce the beginning of AOPA’s resources, advocacy and engagement with state
first public promotion activity. For the last few years and federal funding agencies, roll out of regulatory
there has been significant time spent strengthening the processes including course accreditation and
Association’s regulatory role such as the development assessment of competence and the development
of competency standards, implementation of English of key relationships with external stakeholders. I
language and recency of practice requirements and hope our members are experiencing an increase in
the launch of course accreditation. The Association benefits and representation and welcome feedback
is now able to confidently represent the membership on areas of importance to you.
and make clear statements about the certification Thank you for your support in 2016. Best wishes to
process and standards to which our members are held. you and your family for Christmas and the holiday
Therefore, it is now time to begin a campaign to raise season and I look forward to delivering further
awareness of the depth and breadth of clinical services outcomes in 2017.
delivered to the Australian community by the O&P
profession. AOPA has developed a suite of fact sheets
depicting several the clinical specialty areas for the
profession. These are available on the AOPA website
and we encourage you to download and print them
for your facilities, placing your clinic details in the space Leigh Clarke
provided on the second page. Executive Officer, AOPA
We expect there will be a total of 20 fact sheets
available for your use and accessible to the public. To
support the release of these and our public education
agenda we have also launched the AOPA Facebook
page. AOPA is now pleased to provide a public social
media resource where we share information on the
profession for the public. This represents a substantial
step for the Association, demonstrating that our
regulatory development work is largely complete and
our future ability to have proactive, public messages
to deliver on behalf of our membership. This edition
of The Review provides a snap shot of the clinical
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 5

CLINICAL SPECIALTIES
AOPA launches new promotional resource:
Clinical Specialty
p y Fact Sheets
AOPA is incredibly excited to launch the first series of provided on each fact sheet to affix practice details and
clinical specialty fact sheets. The fact sheets are a new information is provided to enable consumers to easily
set of resources and tools to increase the recognition locate a certified orthotist/prosthetist. A full-size fact
of orthotist/prosthetists amongst the community and sheet can be found over the page.
promote the extensive range of clinical services provided
by the profession. AOPA has worked with experts in each specialty area to
examine available evidence and current practices. The fact
The fact sheets highlight specific areas of clinical practice sheets explain this information in language appropriate
and illustrate the expertise of orthotist/prosthetists in for potential orthotic and prosthetic consumers and
clear language that is both easy to understand and provides a small summary with key points.
share amongst the community.
Every fact sheet explains what an orthotist/prosthetist
AOPA encourages members to share each of the fact is and their role in supporting clients. Emphasis has
sheets with your personal and professional networks, been placed on ensuring that orthotist/prosthetists are
to spread the word about the amazing and vital work correctly portrayed as highly-trained professionals that
that you perform every day, as well as the work of your are the primary experts in managing each condition.
fellow P&O’s.
What are the Fact Sheets?
“Every fact sheet explains what an
The fact sheets are double-sided information leaflets
that provide practical information on specific areas orthotist/prosthetist is and their role
of interest to consumers. Each fact sheet provides an
overview of a specific condition and clearly illustrates in supporting clients.”
the service provided by orthotist/ prosthetists. Space is
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 7
CLINICAL SPECIALTIES
How can I use these to promote P&O?
AOPA encourages you to share, display and distribute
the fact sheets amongst your personal and professional
networks. Suggestions to do this include:
• Provide printed copies in your practice and to clients
that may find the information useful.
• Add the fact sheets to your practice website and social
media accounts, including Facebook, Twitter and
LinkedIn.
• Share the fact sheets on your personal Facebook
accounts, to increase awareness of the orthotic/
prosthetic profession amongst the community.
• Distribute the fact sheets to colleagues as a useful
reference for a particular area of practice.
“increase the profile of orthotist/
prosthetists by joining in the
conversation and contributing to
the promotion of P&O.”
Current Clinical Specialties
The first seven clinical specialty areas were selected
in conjunction with AOPA members to exemplify the
support Orthotist/Prosthetists provide to the Australian
community. The first seven fact sheets include:
• Scoliosis and Kyphosis
• Diabetes Related Foot Disease
• Sports and Recreational Prostheses
• Paediatric Orthotic Management
• Foot Orthoses
• Upper Limb Prostheses
• Plagiocepahly
Future Fact Sheets
AOPA is currently working with a range of experts to
develop the next series of fact sheets, which will be
published on the AOPA website. If you would like to
help develop further fact sheets, please contact the
AOPA Office. AOPA is in particular need of high-
resolution images that can be used in future fact
sheets. If you are able to provide images, please get in
touch.
Factt sheets in development include:
AOPA is proud of the thorough and consultative
method of developing the Clinical Specialty Fact • Acute Spinal Injury
Sheets and would like to sincerely thank all of the • Burns Management
members that provided advice, resources and content. • Management of Neuromuscular Conditions
AOPA members have been fundamental in developing
• Sports Injury
these resources, that would not have been produced
without their invaluable support. Thank you to • Post-amputation Rehabilitation
everyone involved. • Osseointegration
8 / December 2016 / Volume 1 - Issue 2 / The AOPA Review
Clinical specialties in orthotics and prosthetics Image Courtesy of Orthokids
Orthoses in paediatrics: supporting development and
therapeutic intervention in babies, children and young people
What is an orthosis? Cranial orthoses for babies with
An orthosis (pl. orthoses) is an externally applied device that is positional plagiocephaly and
designed and fitted to the body. Orthoses (historically known
as splints or braces) are described by the body part they brachycephaly
encompass. An orthosis may be used to correct body alignment, What is positional plagiocephaly and
support function, minimise discomfort or pain, protect a body part
after injury or surgery, re-distribute pressure, correct deformity or brachycephaly?
assist in rehabilitation. Positional (or deformational) plagiocephaly (pron. play-gee-o-kef-
a-lee) and brachycephaly (pron. brak-ee-kef-a-lee) are types of
Orthoses in paediatrics – who needs them? cranial deformity – meaning a misshapen head. Plagiocephaly
Orthoses play an important role in supporting development occurs when there is flattening on one side of the head, causing
and therapeutic intervention across a range of pathologies in asymmetry. Brachycephaly occurs when there is flattening of the
the paediatric population – from hip orthoses to encourage hip back of the head. Plagiocephaly and brachycephaly are common
development in newborn babies, to spinal orthoses to reduce cranio-facial conditions that occur most often when babies spend
abnormal spinal curves in adolescents with scoliosis or kyphosis. prolonged periods lying with their head in the same position.
How do cranial orthoses help?
Hip orthoses for babies with
Cranial orthoses are a
developmental dysplasia of the hip (DDH) treatment option for babies
What is DDH? with more severe deformity,
where counter positioning
Developmental dysplasia (or dislocation) of the hip (DDH) is an is not possible or has not
abnormal development of the hip joint. The ball at the top of the improved head shape, and
thighbone (the femoral head) is not stable within the socket (the who also have good head
Image Courtesy of Orthokids
acetabulum). The ligaments which hold the joint together may also control. A cranial orthosis
be stretched and loose. DDH can occur in one or both hip joints. is a custom-made helmet
fabricated with a hard plastic
How do hip orthoses help? shell and foam lining. An
Babies with DDH can be successfully treated with hip abduction orthotist designs the helmet to
orthoses. There are different types of hip abduction orthoses – a redirect skull growth by fitting Cranial Remodelling Helmet
pavlik harness, a ‘Denis Browne’ brace, a ‘Rhino’ brace. Though closely to the head but leaving
varied in design, these hip orthoses all hold the hip joint in the room for growth in the flattened area. Refer to the Plagiocephaly
most stable position – with the thigh ‘up and out’ - so that the and Brachycephaly Clinical Specialty Fact Sheet for further
ligaments tighten and the hip joint develops normally. An orthotist information.
works with a multidisciplinary team and the family to determine
the hip abduction orthosis design that best meets the hip position
requirements of the individual baby.
Foot abduction orthoses for children
with Congenital Talipes Equinovarus
What is Congenital Talipes Equinovarus?
Congenital Talipes Equinovarus (or CTEV or congenital clubfoot)
is the most common congenital deformity affecting 1 in 1000
Denis Browne Brace live births. In CTEV, the foot is twisted, pointing inward and
Image Courtesy of Orthokids downward.
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 9
Orthotists – supporting the Australian community
How do foot How do spinal orthoses
abduction orthoses help?
help? Spinal orthoses provide
Image Courtesy of Orthokids
The foot abduction corrective forces on the spine
orthosis is also known to promote symmetrical spinal
alignment in adolescents who
Image Courtesy of Orthokids
as ‘boots and bar’.
It is part of the gold have moderate structural curves
standard treatment for (scoliosis 25-45° or kyphosis 55-
treating CTEV as part of Boots 80°) and who are still growing.
Spinal orthoses effectively
the Ponseti method. This method begins with manipulation and
prevent curve progression in AIS
casting to stretch the foot into a corrected position, then often a
and reduce kyphotic curves in Boston Brace
small operation is performed to lengthen the Achilles tendon (a
people with Scheurmann’s disease.
tenotomy), and finally, wearing of special boots, connected by a
Orthotists combine knowledge of complex anatomy and
bar (the foot abduction orthosis) to keep the feet in their corrected biomechanics to design and fabricate an orthosis (made out of
position and avoid relapse. An orthotist works as part of a rigid plastic) that incorporates the necessary forces to correct
multidisciplinary team in the selection and fitting of foot abduction spinal alignment. Refer to the Spinal Clinical Specialty Fact Sheet
orthoses to support therapy and surgical interventions. for further detail.
Ankle-foot orthoses for children with Who provides orthoses?
cerebral palsy An orthotist (pron. or-tho-tist) is a tertiary qualified Allied Health
What is cerebral palsy? Practitioner who is trained to assess and treat the physical and
functional limitations of people, using orthoses. Orthotists are
Cerebral palsy (or CP) is a neurological disorder caused by a responsible for paediatric orthotic management including DDH,
non-progressive brain injury or malformation that occurs while plagiocephaly, CTEV, cerebral palsy, scoliosis and kyphosis.
the child’s brain is still developing — before birth, during birth, Orthotists combine clinical and biomechanical expertise with
or immediately after birth. Cerebral Palsy primarily affects body their knowledge of current evidence, materials and product
movement and muscle coordination. Cerebral palsy is the most developments to support children with developmental and mobility
common childhood physical disability in Australia. impairments to meet their personal goals.
How do ankle-foot orthoses help?
How do I access an orthotist?
The most common
If your child requires orthotic management for one of these – or
type of orthosis used
any other – condition, your GP or medical specialist will refer you
to help children with
to an orthotist. Certified Orthotist/Prosthetists ‘cOP-AOPA’
cerebral palsy is the
can also be located using the ‘Find a practitioner’ search function
ankle-foot-orthosis
Image Courtesy of Orthokids
on the AOPA website (www.aopa.org.au).
(or AFO). AFOs are
custom-made and
encompass the foot, Orthotic management in paediatrics:
ankle and lower s -ANY BABIES CHILDREN AND YOUNG PEOPLE BENElT FROM
leg. The design and orthotic intervention – including those with Developmental
purpose of the AFO is AFO Dysplasia of the Hip (DDH), deformational plagiocephaly,
different according to each person’s unique needs and goals, Congenital Talipes Equionovarus (CTEV or clubfoot), cerebral
which often includes supporting or correcting abnormal limb palsy, scoliosis and kyphosis
positioning, preventing deformity, providing a stable base for s /RTHOSES HELP TO REDUCE DEFORMITY CORRECT BODY ALIGNMENT
sitting and standing, and facilitating a safer and more efficient and support functional goals such as sitting, standing and
walking pattern. AFOs are also used by children who have walking
other conditions such as spina bifida, developmental delay or
s /RTHOTISTS ARE !LLIED (EALTH 0ROFESSIONALS WHO SUPPORT BABIES
CTEV. Orthotists work with the client, family and members of the
children and young people by providing comprehensive and
multidisciplinary team to determine the most appropriate AFO to evidence based orthotic care and interventions
help each child meet their personal goals.
Spinal orthoses for adolescents with
scoliosis and kyphosis
What is spinal deformity?
Spinal deformity is an abnormal curvature of the vertebral column.
Two common spinal deformities are Adolescent Idiopathic
Scoliosis (AIS) - a sideway curvature of the spine with rotation
resulting in a rib hump; and Scheurman’s kyphosis – an
increased forward curve of the thoracic (upper) spine presenting Disclaimer – This fact sheet does not replace clinical advice. If you require orthotic services AOPA recommend
speaking to your practitioner. This fact sheet was developed based on interpretation of current evidence as of
as rounded shoulder. August 2016. References available on request.
10 / December 2016 / Volume 1 - Issue 2 / The AOPA ReviewPROMOTING THE PROFESSION
AOPA Joins Facebook
To support and promote the profession AOPA has developed an association
Facebook page: www.facebook.com/AOPAnews/
AOPA is incredibly excited to launch an association Throughout 2017 AOPA will also be utilising Facebook
Facebook page to engage with the community and to promote the profession by featuring a particular
promote the profession. Whilst AOPA has maintained clinical specialty every two weeks. In doing this, AOPA
a presence on both LinkedIn and Twitter, Facebook hopes to promote the services orthotist/prosthetists
is the most effective platform to communicate with provide that may be less well-known or commonly
the community and increase the profile of orthotist/ associated with other professions. To support this, AOPA
prosthetists nationally. would be incredibly grateful if you could share, post and
like each promotional post on the AOPA Facebook page.
To achieve this, AOPA will be promoting resources that
concern the community and sharing articles and links Every AOPA member has the potential to increase
when the profession is featured in the media. Recently, the profile of orthotist/ prosthetists by joining in the
AOPA engaged with companies on Facebook after they conversation and contributing to the promotion of P&O.
featured orthoses in advertisements, and shared and Each time you write a personal post or share an AOPA
promoted an article regarding changes to prosthetic post on Facebook you expose the orthotic/prosthetic
funding in South Australia. In continuing to do this, the profession to hundreds of additional consumers and
profession can raise the profile of orthotist/prosthetists people in the community. Join the AOPA Facebook
and ensure that we are clearly linked to the services page today to begin supporting the future of P&O in
we provide. Every time the profession is featured in the Australia.
media presents an opportunity to further engage with
the community and increase the awareness of orthotic Find AOPA on Facebook here:
and prosthetic services. www.facebook.com/AOPAnews/
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 11INTERNATIONAL P&O PERSPECTIVES
An International P&O Career
Wes Pryor recently spoke at the AOPA and Ottobock Student Event. AOPA are pleased to
provide his perspective on prosthetics and orthotics internationally.
Wesley Pryor
Senior Technical Adviser at the Nossal Institute for
Global Health
Thanks to AOPA and its members for their
extraordinary commitment to strengthening P&O in
Australia. It's a real privilege to share some thoughts
about the international dimension of our sector.
Healthcare and technology are changing quickly.
As P&O professionals, we must think of ourselves
as being critical parts of that puzzle. I am always a
bit embarrassed to be talking to P&Os about their
profession, but am very glad to be able to continue
learn from them and imagine how we might work
together. I always wanted to be a P&O, plaster on-shoes,
carbon fibre, ovens, all of it. But I never got around to it.
With that in mind, AOPA has asked me to share a few
thoughts about my career.
I am at least the proudest P&O there is, but I haven't
had a typical career. Most of the time, I'm at a desk. strengthen rehabilitation and to address the unmet
Sometimes that desk is in other countries, but it’s a desk need for assistive products, which for many people
anyway. I started out at 15, compelled by the landmine are essential determinants of equitable participation in
legacy. Conflict in Cambodia for the most part had development.
ended, but the landmine legacy was still in the news.
Somehow that news made it to Western Victoria. So Still, I truly envy those who get to work with people
I studied P&O and completed a clinical placement in every day. As Australian P&Os we have peers working
Cambodia. around the world in extremely complex scenarios,
making a massive difference in peoples’ lives. I think
I wound up doing an evaluation of an aid project after they demonstrate the idea of P&O in international
the 2001 earthquake in western India and then ended health much more than my work.
up completing short term evaluation work in Iraqi
Kurdistan. It opened my eyes to the changing policy Improving access to services and basic rights for all
environment, and the daily challenges of people living is obviously a complex challenge and rehabilitation
in and around conflict. I applied for a few other jobs and allied health are not always a neat fit. But, the
in health agencies, thinking there might be something situation is getting better. Decent rehab is absolutely
for a P&O to do. I failed miserably in these attempts, on the development agenda. Your work, as a P&O, is
but some of the people on those panels are now great highly valued and P&O's are rightly seen as essential
mentors and have helped bring assistive technology and professionals with unique skills that are necessary if the
allied health into discussions about inclusion, rights and need for assistive technology is to be met. Advocating
development. for what we do is still important, but we must now
capture good evidence and practice detailing what
In 2007 I began advising on P&O for Handicap works in improving access to services, and seek to
International, who work across disability in development strengthen them further. For me, the challenge is still
and emergency, in partnership with local agencies rather mostly about connecting people to services that already
than providing services directly. In that role I lead teams, exist, and to ensure those services are appropriate, fair,
evaluated what works, and designed new programs. I and meet the needs of the ever-growing number of
did this for nearly 10 years, in about 15 countries. I now consumers. These goals are exactly what AOPA and its
work in rehabilitation in global health. I have awesome members are all about. The next phase of strengthening
colleagues, all with the same key things in mind: and extending rehabilitation in general and P&O
equity in health, and rights for people with disabilities. specifically will involve industry, educators, researchers
This means working with people with disabilities and and consumers working together. Professional
policy makers to ensure disability inclusion is taken associations are situated better than anyone to make
seriously in development practice. We also work to those connections.
12 / December 2016 / Volume 1 - Issue 2 / The AOPA ReviewCASE STUDY
A comparison of a Boston TLSO and a Cheneau
TLSO with Rigo principles in a patient with
Adolescent Idiopathic Scoliosis
Felicity Williams (cOP-AOPA) X was a diligent brace wearer who would only allow
& Wayne Borgelt (cOP-AOPA) her Dad to fasten the brace as Mum couldn’t fasten
Sydney Children’s Hospital the straps tight enough for her liking. Despite her
diligence, a radiograph in March 2014 showed that
Patient X, a 10.5 year old female presented to our the lumbar curve had progressed to 30˚ in brace. A
department in February 2013 for treatment of her cast was taken and a new custom Boston-style TLSO
scoliosis. X-rays showed a 25˚ right thoracic curve and a was fit in April 2014. Although multiple modifications
35˚ left lumbar curve at initial presentation (figure 1a). were made at the time of fitting the best in-brace
A cast was taken and she was fit with a custom made correction obtainable was only 24˚ (31% correction).
Boston-style TLSO in March 2013 (figure 1b). As per our At this time it was decided to recast and fabricate a
standard procedure a standing AP radiograph was taken Cheneau TLSO with Rigo principles in an attempt to
six weeks after the initial fitting. This showed good gain better correction of the lumbar curve.
correction of the thoracic (25˚ to 12˚, 50% correction)
and lumbar curves (35˚ to 20˚, 42% correction). The Cheneau TLSO utilises a system of very specific
Additional loading pads were applied at this time in an and detailed criteria to classify curves that directly
attempt to increase correction in the lumbar curve but relates to brace manufacture. There are both clinical
additional x-rays were not taken. and radiological criteria used to classify the curve
pattern with four main classifications and nine
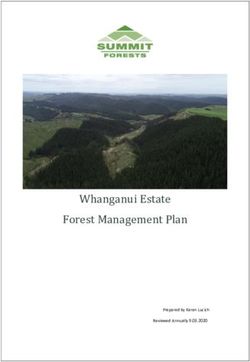
Figure 1. a) Pre-treatment x-ray, December 2012. b) Initial substyles. Each of these provides a unique brace
in-brace x-ray, May 2013. c) Curve progression in first brace, specific ‘blueprint’. A table showing these criteria can
March 2014. be found in Table 1.
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 13CASE STUDY
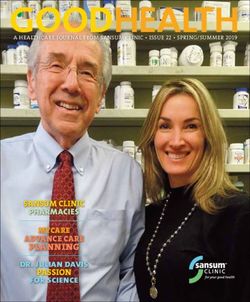
Figure 2. a) Out of brace x-ray April 2014 showing the transition point and central sacral line b) Radiological criteria for an E2 type
brace c) E2 brace ‘blueprint’ (Adapted from Rigo, Villagrasa & Gallo, 2010).
Therefore, when we decided to make X a Cheneau style X-rays in her E2 Cheneau TLSO showed excellent in-
TLSO, we obtained an out of brace x-ray so she could be brace correction of the lumbar curve (down to 8˚, 77%
radiologically classified (figure 2a). Radiologically X was correction) and a negligible thoracic curve (figure 3a). A
borderline between B2 and E2 types, however clinically new Cheneau E2 was fit in December 2015 with excellent
she met the E2 criteria as there was no rotation present correction once again obtained (10˚, 71% correction).
in a forward bend test indicating that the thoracic curve
had become a compensatory postural curve (rotation In July 2016 bracing was discontinued as a bone age
was present in the thoracic curve on initial presentation). x-ray showed that X was skeletally mature. An out of
Where there are discrepancies between clinical and brace x-ray performed at this time showed that the
radiological criteria the clinical classification tends to lumbar curve was 23˚ (figure 3b).
take precedence. Therefore, an E2 type TLSO was
It has been reported that patients with good compliance
fabricated and fit in May 2014.
and greater than 40% correction are likely to have
a stable reduction in Cobb angle at skeletal maturity
(Landauer, Wimmer and Behensky, 2003). Although X
initially had good correction of her lumbar curve (42%)
in the Boston brace, at a 12 month follow up her curve
had progressed in brace. If we had continued in the
Boston brace her outcome was likely to have been
poor. By changing to the Cheneau brace we achieved
over 70% correction and a stable curve at skeletal
maturity of 23˚ equating to a 12˚ reduction of her initial
Cobb angle. With the primary aim of bracing being to
simply prevent curve progression (Negrini et al. 2011), a
reduction of Cobb angle at the end of treatment was an
excellent outcome.
REFERENCES
Landauer, F; Wimmer, C; Behensky, H. (2003). Estimating the final outcome of brace treatment for idiopathic
thoracic scoliosis at 6-month follow-up. Ped Rehab, 6(3-4), pp. 201-207.
Rigo, M; Villagrasa, M; Gallo, D. (2010). A specific scoliosis classification correlating with brace treatment:
description and reliability. Scoliosis 5:1.
Figure 3. a) X-ray in Cheneau TLSO May 2015. b) X-ray at end Negrini et al. (2012). 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic
of treatment July 2016. scoliosis during growth. Scoliosis 7:3.
14 / December 2016 / Volume 1 - Issue 2 / The AOPA ReviewCASE STUDY
Table 1 – Cheneau Classifications. Adapted from Rigo, Villagrasa and Gallo, 2010.
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 15BOARD INTRODUCTION
Introducing a Consumer Advocate
AOPA would like to introduce Tricia Malowney, AOPA Board member, disability and
equality advocate, and P&O consumer.
Tricia Malowney
Consultant and AOPA External Director
Tricia Malowney contracted polio at four months,
using callipers until she was 16, at which time her
surgeon told her that they were no longer required,
a decision she now considers totally inappropriate. At
age 36, Tricia developed post-polio syndrome, and at
46 retired from a management position as a policy
and research officer, and educator with Victoria Police.
Tricia now uses a stance control KAFO and crutches
as mobility aids, and is always keen to espouse the
benefits of good quality orthoses and the work of
prosthetist/orthotists.
A key focus of Tricia's work is centred around
improving access to services for people with
disabilities, with an emphasis on access to justice and
health as well as ending violence against women with
disabilities. Tricia now works as a consultant, which
enables her to contribute to inclusive practices through
policy review, facilitation and development and by
providing advice to the disability and mainstream
sectors, including AOPA.
Tricia is a past President of the Victorian Disability
Services Board and has roles on a range of disability
and mainstream boards and committees, in addition
to AOPA, including the Chair of Independent Disability
Services Board and Director at Scope. Tricia is also
a member of the Coroner's Systemic Review of
Family Violence Deaths Reference Group and the
Eastern Region Family Violence Partnership Executive
Committee.
Tricia has previously been Deputy Chair of the
Victorian Disability Advisory Council and was the
inaugural chair of Women with Disabilities Victoria
and the Royal Women’s Hospital Disability Reference
Group, inaugural Co-chair of the Victorian Equal
services such as health, justice and employment, and
Opportunity and Human Rights Commission Disability
bring the learnings back to the Victorian State Disability
Reference Group and had a ministerial appointment
Plan and the National Disability Strategy.
as the community representative on the Road Based
Public Transport Advisory Council. She has served Tricia's is passionate about the NDIS and was a
on both the Board of Women's Health Victoria and campaigner for its introduction, and now campaigns for
the Board of Women's Health East. Tricia was also its implementation. However, she also believes that we
the recipient of the inaugural Brenda Gabe Award also need to implement the National Disability Strategy
by Women with Disabilities Victoria in November and the State Disability Plan and the Information
2013, that included a scholarship to attend the Pacific Linkages and Capacity Building component of the
Rim Disability Conference in Hawaii and present a NDIS, previously ‘Tier 2’. Recognising the compounding
paper on disability and leadership. An Ethel Temby nature of disadvantage, Tricia is committed to ensuring
research grant further enabled her to travel to Ireland that a disability lens is applied to the development of
in 2015 and look at their national disability strategy, mainstream policies and procedures, and that a gender
particularly as it pertains to access to mainstream lens is applied to the disability sector.
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 17CLINICAL TOPICS
Lower Limb Prostheses Through the Years:
An Experience
Barry Leech (cOP-AOPA)
In February 1964, I was seeking employment as an
apprentice electrician at the Royal Alexandria Hospital
for Children in Camperdown NSW. By misadventure I
chose a traineeship as a Surgical Appliance Technician
within the ‘Splint’ Department - and thus began my 52-
year (and counting) career in orthotics and prosthetics.
So what has changed in lower limb prostheses? When
I started out as a prosthetist, you were expected
to complete every job you were given from start
to finish. Unlike today, much of the componentry
was made within the facility. The skills required to
manufacture a limb included metalwork, woodwork,
plastics manipulation, welding, fitting and machining,
leatherwork and technical drawing. Records were kept
only to document time and date of appointment and
the components that were used. In fact, the client
would commonly collect their prosthesis from the office
counter and only return if there were problems.
Wooden prostheses required the prosthetist to take
measurements and templates as a guide to carve a
socket from a wooden block. The shaft milling machine
(that we still use today) was fitted with an exposed
cutting blade which would hollow out the socket to a
wall thickness of around 5mm. Aluminium prostheses
required high-level panel beating skills and competence some clients. We have access to an amazing range of
in using specialist machines to shape the prosthesis. prosthetic componentry (almost too many choices) and
Leather work skills were also required to mould and the possible outcomes for each client are far greater.
stitch the socket interface and mechanical skills to The mechanical and biomechanical efficiency, cosmetic
affix the ankle and knee joints. Aligning the prostheses options and comfort far exceeds that which was once
consumed a lot of time and the use of cumbersome available.
jigs. 30 hours of labour was not uncommon from
start to finish with an additional 6 hours of sanding
and painting often required. It was very dirty, labour “We have access to an amazing
intensive work and required proficiency in hand skills.
Ultimately, these prostheses were works of art and range of prosthetic componentry and
occasionally you didn't want to hand them over to the
client to be worn! the possible outcomes for each client
Today, orthotist/prosthetists begin their careers by are far greater.”
completing university studies and then practice as allied
health professionals in an evidence-based system. We Osseointegration also provides significant opportunities.
have extensive procedures and guidelines to ensure Regardless of componentry prescribed, osseointegration
all recommendations are followed and the best client
reduces interface issues, eliminates socket fitting
outcomes are achieved. We must also utilise continuing
problems and may provide improvements in gait
education to stay abreast of advancing technologies and
symmetry, proprioception, sensory feedback and client
evidence.
satisfaction. When asked if any of our osseointegration
For the majority, we utilise materials that technology clients would go back to a socket interface, the answer
has made available to us including carbon fibre, is always a resounding no! Osseointegration comes
plastics and laminates. However, we still provide the with a greater risk of infection and currently no real
occasional wooden prosthesis as it still has its place for understanding of implant sustainability. Alignment and
18 / December 2016 / Volume 1 - Issue 2 / The AOPA ReviewCLINICAL TOPICS
componentry selection are crucial to the success of level of fit, comfort and performance we should all
osseointegration for shock absorption, torsional force aspire to. These are the very same people who bridged
and terminal impact. the gap between orthotists and prosthetists which
eventually formed AOPA.
Through the evolving years in lower limb prostheses,
the one thing that has remained unchanged is the
responsibility of a prosthetist to provide the most
appropriate limb for the client as an individual.
“…the one thing that has remained
unchanged is the responsibility of
a prosthetist to provide the most
appropriate limb for the client”
So have lower-limb prostheses changed dramatically
over the years considering the first prosthesis was a
‘peg-leg?’ No…they have just become better!
I would like to acknowledge and thank the limb and
splint makers of the past. The limbless, returned
serviceman unendowed with the academic learning, nor
the technology available to us today. They set in place
the qualities of care and desire to achieve the highest
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 19CLINICAL NOTE
Custom Foot Orthosis Technique for Plantar
Fasciitis
Paul Retschko B.P.O. (Hons.) cOP-AOPA has been made to reduce heel strike transients, control
hind foot mechanics or support the MLA, let alone all at
Introduction once. Following is an explanation of how our practice
Plantar Fasciitis is a painful foot condition with a prescribes, designs and manufactures foot orthoses for
reported incidence of 10% of the population1 of whom the plantar fasciitis afflicted foot.
80% will experience resolution of symptoms within 1
year irrespective of the chosen therapy2. The reported
Biomechanical Assessment and Casting
risk factors for plantar fasciitis are broad, spanning the Full patient assessment is performed with attention
sedentary, obese patients to active athletes; the pes paid to defining the degree of varus or valgus hind
cavus foot to the hypermobile pes planovalgus foot.3 foot posting. This aids in achieving ‘stabilisation of the
hindfoot’. Put simply, this is the magnitude of the skive,
Recently nomenclature has been expanded to plantar wedge or post applied to the heel in order to balance
fasciosis, including a degenerative fascial disease the plantar weight bearing surface of the calcaneum in
as opposed to a sole inflammatory focus. Despite subtalar neutral. (Figure 1). The easiest way to de-stress
this, the recommended treatments remain heel cord the plantar fascia is to invert the hind foot and plantar
stretching exercises with soft heel inserts, physical flex the first ray.4
therapy, cortisone injection (despite links with increased
incidence of rupture7), extra corporeal shockwave At this stage, the magnitude of any gastrocnemius
therapy (ESWT), night splints, intrinsic toe flexor contracture() is recorded. A heel raise is often required
strengthening exercises and in-shoe orthoses and as gastrocnemius contracture creates internal rotation of
inserts.3 For recalcitrant cases that fail conservative the mid foot at mid to late stance phase which increases
management, endoscopic release of the plantar fascial tension. In a small number of cases, especially
fascia may be performed, often with gastrocnemius with cavoid posture, forefoot alignment may reveal that
lengthening. Published studies on the results of the a valgus forefoot post may be necessary. This can relieve
aforementioned treatments vary greatly, however the tension in the lateral portion of the fascia or can be used
objectives remain to reduce patient pain, increase to counterbalance the varus hind foot post if lateral
functional capacity and reduce disease duration. stability is problematic.5
A study by Walther et al (2013) into the efficacy of A foam box impression is used for casting. Prior to
3 simple orthoses demonstrated significant benefits embedding the foot, transfer paint is applied along the
in pain scores with customised versions of the tested course of the prominent portions of the plantar fascia
orthoses. The desirable properties of the orthoses were and used to define the margins of the pain around the
to reduce maximum pressure at heel strike, stabilisation insertion of the fascia onto the calcaneal tuberosity.
of the hind foot and support of the medial longitudinal Orthotic pressure along the medial slip of an inflamed
arch (MLA) to decrease plantar fascia strain.2 fascia is a classic cause of patient-orthotic intolerance;
devices have often had the MLA lowered extensively
Examining the array of foot orthoses provided by when all that was required was a fascial groove. Loss of
other clinicians (including all allied health disciplines) the MLA height then compromises heel decompression,
demonstrates little change in the orthotic technique mechanical control and a reduction in tension of the
used for other foot conditions. Often little or no attempt fascia. The foot is embedded whilst the patient is
Figure 1. Manipulation of the cast to create varus or valgus stabilisation of the hind foot. Source Kirby, K.A.
20 / December 2016 / Volume 1 - Issue 2 / The AOPA ReviewCLINICAL NOTE
Figure 2 Left: Posterior view displaying hind foot
to forefoot relationship and PF insertional relief
modification, (ideally a more rounded heel cup
would be included-modified for demonstration),
Right: Plantar view demonstrating metatarsal
build up, medial slip modification, MLA profile
and insertion of PF build up.
70kg person a layer of 6mm 300 then 6mm
of 400 density is used ensuring heel raises
are incorporated. These devices are typically
bulky; the heel raise and aggressive MLA
support dictate this.
Patients are encouraged to break the
devices in by using for two hours twice daily
for 3-4 days and then expand as tolerated.
Typically, patients are in sufficient discomfort
such that deep shoes such as runners or
lace up walkers are tolerated for the healing
period. An initial period of 3 months of
full time use is described, depending on
seated, thereby allowing the position and posture of the recovery rates, this can be prolonged.
foot to be manipulated. Through use of the windlass
mechanism, subtalar neutral should be achieved Review and Adjust
during casting. Full weight bearing impressions result Reviews are performed two weeks’ post fitting to
in maximum flattening of the MLA and compromised alleviate common orthotic issues, then at six weeks
results as the fascia is lengthened. Maintenance of a to monitor pain and functional capacity. Notes are
rounded heel and cupping of the subcalcaneal fat pad compared from pre and post fitting reviews and walking
also improves shock absorption at heel strike.6 standing tolerance durations compared.
Modifications Common problems experienced in the initial orthotic
When modifying the positive casts, I add 5mm to the period are excessive lateral longitudinal arch and or mid
metatarsal head region as this creates universal loading foot height, excessive bulk of device and incongruity
of the MLA tissues by the orthosis. Consequentially, care between location of pain and orthotic relief. These
must be taken to ensure that the lateral longitudinal problems are readily adjusted for. It may be necessary to
arch is not excessive in height. The marked areas re-mark the most sensitive areas of the foot and have
of the plantar fascia and insertion are built up by the patient stand on the device to double check that
approximately 6 mm. (Figure 2) The heel section should offloading occurs. Modification to the depth and with
maintain approximately 60% contact with the foot, this of the heel relief and or channel is often required. I will
is necessary for the hind foot posting to be effective and again review the patient two and six weeks’ post fitting.
for patient comfort. Should insufficient progress be made the program
may be augmented with a course of ESWT, review of
The MLA profile is levelled horizontal to the ground gastrocnemius stretching exercises and on occasion use
from the base of the plantar fascia. This allows of a night splint.
the profile of the finished orthotic to be accurately
manipulated in small increments where a curved surface I hope this enhances your management of a common
is difficult to alter. It also helps reduce some of the bulk and painful foot condition.
of the device.
BIBLIOGRAPHY
Manufacture 1. Grecco, M.V., Brech, G.C., Greve, J.M.D. One-year treatment follow-up of plantar fasciitis: radial
shockwaves vs. conventional physiotherapy. Clinics. 2013;68(8): 1089-1095.
The objective of the orthosis is to decompress the sensitive 2. Walther, M., Kratschmer, B., Verschl, J., Volkering, C., Altenberger, S., Kriegelstein, S., Hilgers, M. Effect
regions of the foot and create a soft landing for these of different orthotic concepts as first line treatment of plantar fasciitis. Foot and Ankle surgery 2013;
19:103-107
regions if loaded. Areas of the foot capable of tolerating 3. Schwartz, E.N., Su, J. Plantar fasciitis: A concise review. The Permanente Journal 2014 Winter 18(1)
pressure are used to control frontal plane motion and e105-e107
4. Kirby, K.A., Foot and Lower Extremity Biomechanics: A ten year collection of precision intricast
redistribute force from those sensitive areas. A 2mm layer newsletters. 1997;Precision Intricast Inc. Payton Arizona
of 200-250 density material is vacuum formed over the 5. Hunter, S., Dolan, M.G., Davis, J.M. Foot Orthotics in therapy and sport. 1995; Human Kinetics,
Champaign IL
cast. 2-3 mm thick super soft material is then adhered 6. Retschko, P.H., Wood, M. and Bach,T.M. The effect of casting technique on shock absorption foot
over the heel and fascia relief. The fill density is judged orthoses. Prosthetics Orthotics Australia 1995 Dec. 38-44.
7. Rolf. C., Guntner, P., Ericsater, J., Turan., I. Plantar fascia Rupture: Diagnosis and treatment. The Journal of
on patient weight and perceived activity level; i.e. for a Foot and Ankle Surgery 1997; 36(2): 112-114
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 21RESEARCH NOTE
Comparison of the Pavlik Harness and Von
Rosen Splint for the Orthotic Management of
Neonatal Developmental Dysplasia of the Hip
Claire Skewes Incidence & Classification
Orthotic and Prosthetic Student, La Trobe University The reported incidence of developmental DDH ranges
Introduction from 0.5 to 35 per 1000 live births (De Hundt et al.,
2012). Age at diagnosis contributes to this variation,
Developmental dysplasia of the hip (DDH) is the given that it can drop from 5.5 to 0.5 per 1000 live
abnormal development or dislocation of the hip at births in the same cohort after just two weeks of age
birth, comprising a spectrum of abnormalities ranging (Alsaleem et al., 2014). This is due to the majority
from slightly dysplastic to completely dislocated hips of newborn DDH cases spontaneously normalising
(Agarwal & Gupta, 2012). Risk factors include female within the first two months of life (Agarwal & Gupta,
gender, being firstborn, a positive family history of DDH, 2012). Although no universal classification system
oligohydramnios, and breech position (De Hundt et al., exists (Bin et al., 2014), the most commonly used is
2012). Untreated DDH is responsible for chronic pain, Graf’s classification system which relies on the use
gait abnormalities, abnormal joint development, and of ultrasound and measurements of hip angles to
juvenile osteoarthritis (Alsaleem et al., 2014). These determine normality of development (Graf, 1984).
consequences of DDH account for 30% of all total Diagnosis
hip replacements in people under the age of 60 years
Delayed diagnosis and subsequent intervention are
(Agarwal & Gupta, 2012).
synonymous with worsened outcomes and increased
need for surgery (Aiello, 1989). It is well documented
that an early diagnosis within the first 2 weeks of
“Untreated DDH is responsible for life, and prompt conservative treatment before three
chronic pain, gait abnormalities, months of age, are crucial to a good functional outcome
(Agarwal & Gupta, 2012). A number of screening and
abnormal joint development, and diagnostic methods exist (Paton & Choudry, 2016),
however ultrasound and the Ortolani and Barlow
juvenile osteoarthritis.” manoeuvres are of greatest relevance to the orthotic
management of DDH.
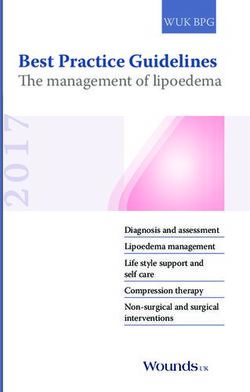
Figure 1. Flexion and abduction used in the Ortolani test to relocate a posteriorly dislocated hip at birth (Gelfer & Kennedy, 2008)
Figure 2. Flexion and adduction applied in the Barlow manoeuvre to dislocate an unstable hip (Gelfer & Kennedy, 2008)
The AOPA Review / Volume 1 - Issue 2 / December 2016 / 23You can also read