COVID-19 & CO-INFECTIONS - NCIC JOURNAL CLUB 23 SEPTEMBER 2020 SHIO YEN TIO PHD CANDIDATE NCIC, PETER MACCALLUM CANCER CENTRE - NATIONAL CENTRE ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NCIC JOURNAL CLUB
23 SEPTEMBER 2020
COVID-19 & CO-INFECTIONS
Shio Yen Tio
PhD Candidate
NCIC, Peter MacCallum Cancer Centre
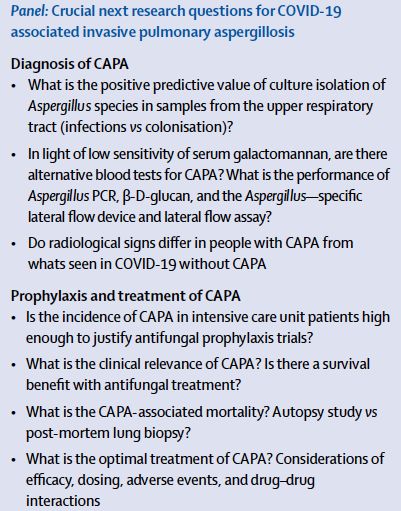
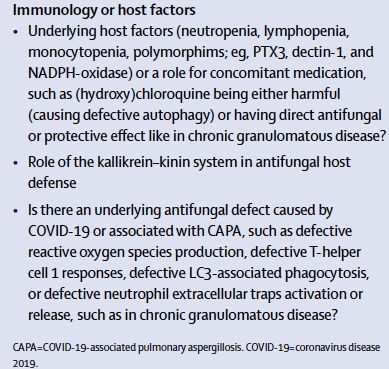
INTRODUCTION/ BACKGROUND
• Reports of co-infections with COVID-19: viral, bacterial and fungal
• Fungal co-infections: invasive pulmonary aspergillosis (IPA) è
strong association in patients with severe influenza
• Pathophysiology: damage to lung epithelial cells and/ or immune
dysregulation è pulmonary damage è create inflammatory
environment predisposes to fungal infections
Lansbury et al. J Infect. 2020;81(2):266
Schauwvlieghe et al. Lancet Respir Med. 2018; 6(10): 782
van de Veerdonk et al. Am J Respir Crit Care Med. 2017; 196(4): 524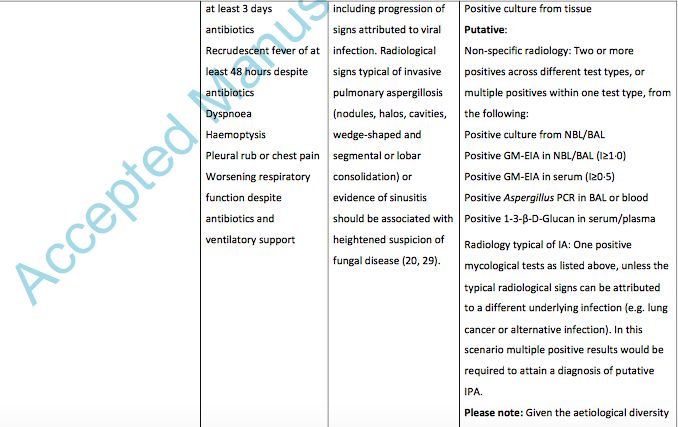
BACKGROUND
• Diagnostic challenges of IPA in COVID-19:
Ø Most patients do not fulfill host factors/ criteria based on
EORTC/ MSG definitions
Ø Restricted role of bronchoscopy procedures
Ø Sensitivity of serum galactomannan (GM) è 25-30% (as
opposed to positive serum GM in 65% of patients with influenza-
associated pulmonary aspergillosis)
Ø GM not validated for upper respiratory tract samples
Ø Aspergillus spp in sputum/ tracheal aspirate è ? Colonisation
Ø Non-specific radiological findings
Verweij et al. Lancet Microbe 2020, 1, e53
Bartoletti et al. Clin Infect Dis. 2020
Koehler et al. Mycoses. 2020; 63(6): 528
Van Arkel et al. Am J Respir Crit Care Med. 2020; 202(1): 132
Alanio et al. Lancet Respir Med. 2020;8(6): e48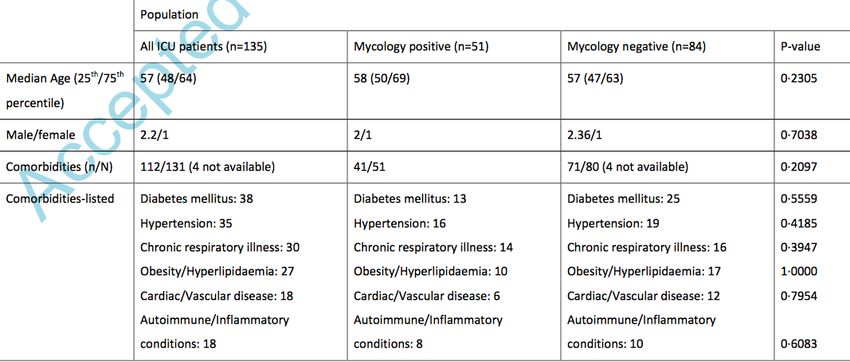
CHALLENGES
Verweij et al. Lancet Microbe 2020, 1, e53
White et al. Clinical Infectious Diseases. 2020.
OBJECTIVES/ AIM
To determine incidence, impact & risk factors
for COVID-19 associated pulmonary
aspergillosis
Testing strategy to diagnose IFD in critically-ill
COVID-19 patients across Wales
METHODS
• National prospective, consecutive cohort study
• Involved all ICU in Wales
• Enhanced mycological testing in ICU patients 1 week post COVID
diagnosis – to detect yeast and mould
Detection of yeast Blood culture + 1, 3 beta-D-glucan
• GM: ≥0.5 (serum); ≥1.0 (deep respiratory samples –
NBL/ BAL)
Combined with
• Aspergillus PCR: on serum/ plasma & NBL/ BAL molecular, GM and
• NBL/ BAL culture culture of respiratory
• BDG (Fungitell assay): +ve threshold of 80pg/ml samples
(tested in duplicate to get a mean value)
• BC and CT chest/ CTPA Detection of moulds
DIFFERENT DEFINITIONS TO DEFINE INCIDENCE OF IPA
Blot et al. Am J Respir Crit Care Med. 2012;186(1):56Verweij et al. Intensive Care Med. 2020; 46(8): 1524
STATISTICAL ANALYSIS
• Descriptive analysis
• Positive rate for each test was determined for both the specimens and
patients
• Associations between clinical factors were determined for combined
IFD, and IPA and candidosis individually.RESULTS
• Over the study period (first 7 weeks of service), 257 patients admitted to ICU
with COVID-19:
• 135 (53%) screened for IFD
• 123 patients had BC and BDG testing
• 60 had NBL test
• 48 patients had all testsRESULTS
135/ 257 (53%) patients screened
51/135 (37.8%) with at least 1 positive
mycological tests (culture, BDG, GM or PCR)
17/51 invasive 30/51 with positive 4/51 with unspecified
yeast infections Aspergillus results IFD, but +ve BDG
multiple times
93.8% Candida 14 with single 16 with ≥2 +ve
spp +ve Aspergillus Aspergillus
result resultsRESULTS
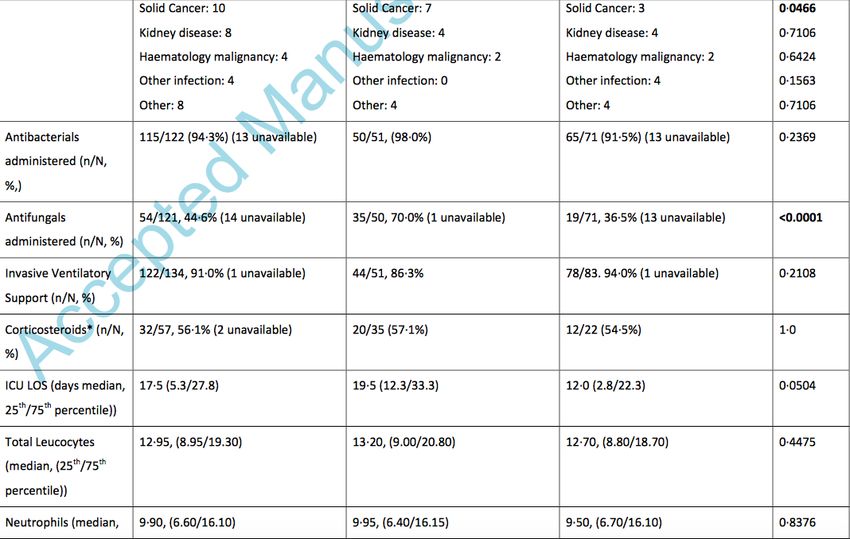
• Strong association between:
• Patients with multiple Aspergillus/BDG (≥2) positive results and high-dose
systemic corticosteroids (13/15 patients, Odds ratio 7.9, 95% CI: 1.6-39.3, p=
0·007)
• Patients with an underlying chronic respiratory condition to have multiple positive
Aspergillus/BDG tests (7/16) (OR: 3·15, 95% CI: 1·06-9.34, p=0·05)
• Median time to positive Aspergillus results = 8 days post ICU admissions (0-35
days); 6.5 days post positive COVID-19 PCR
• Median time to yeast infections = 9 days post ICU (0-38 days) & 10 days post
positive COVID-19 PCR (1-38 days)
• 7/16 patients with multiple positive Aspergillus results had non-specific CT
chest findings
• CT chest findings with typical IPA features: sensitivity 56.3% (95% CI: 33.2-
76.9) and specificity 98·0% (95% CI: 93·1-99·5)DEFINING IPA IN ICU COVID-19 PATIENTS
• Using AspICU, IAPA and novel CAPA definitions, incidence of IPA:
• 5.9% (8/135) for AspICU definition
• 14.8% (20/135) for IAPA definition
• 14.1% (19/135) for novel CAPA definition
IAPA definition Novel CAPA definition
Mortality rate: 45% Mortality rate: 58%
42.9% died despite antifungal; 50% 46.7% died despite antifungal; 100%
died if no antifungal initiated è died if no antifungal initiated
?under-estimated/ misclassified
patients with true IPA
• ROC analysis of GM in NBL + novel CAPA definition:
• GM >1.2 è 97.4% specificity of diagnosing IPA
• GM >4.5 è99% specificity of diagnosing IPAPATIENTS’ PROGNOSIS
• Overall mortality rate for COVID-19 patients in ICU: 38%
• Mortality for patients with CAPA: 57.9% (95% CI: 36.3-76.9),
ranging from 46.7% in patients with appropriate antifungal
therapy to 100% who did not receive antifungal
• Mortality for patients with yeast infections: 47.1% (95% CI:
26·2-69·0), ranging from 27.3% in patients with appropriate
antifungal therapy to 83.3% who did not receive antifungal
• Combined IFD (CAPA & yeast infection): 52.8% (95% CI:
37.0-68.0)DISCUSSION
• Structured IFD testing in COVID-19 patients admitted to ICU is urgently
needed
• Availability of 1,3-beta-D glucan test; lower sensitivity of serum GM
• The role of NBL versus BAL
• Using different definitions to define incidence:
• AspICU – low sensitivity, slow turn-around time
• IAPA – similar incidence rate as CAPA definition, but considerable
discordance
• CAPA – enhances specificity
• Significant incidence of yeast infections (13%) – documented cases
even after 5 weeks post ICU admissionSTRENGTHS AND LIMITATIONS
• Strengths:
• Prospective cohort study
• Proposed different tests or test combinations
• Used different definitions to determine incidence of IPA, including
novel CAPA definitions
• Included not only IPA, but invasive yeast infections as well
• Limitations:
• Not all patients were screened (about 50%) è potentially
underestimated the incidence
• May not be applicable to our local settings: NBL and BAL not
performed, only tracheal aspirates; no BDG testing in Victoria/
AustraliaCONCLUSIONS
• Poor outcome in patients with COVID-19 and IFD
• Structured IFD testing in COVID-19 patients admitted to ICU is
urgently needed
• Radiology when typical of IA, is highly specific for CAPA (98%)
• Multiple positive mycology results are also indicative of IFD
• Steroids and underlying chronic respiratory condition è increase the
likelihood of CAPA, ?benefit from prophylactic antifungalBartoletti et al. Clin Infect Dis. 2020
METHODOLOGY:
• Prospective, multi-centre cohort study in 3 ICUs in Italy, from 22
February to 20 April 2020
• Only involved patients requiring mechanical ventilation for ARDS
• Screening protocol:
• BAL on ICU admission and at day 7 (clinical disease progression),
samples tested for GM (and if positive for Aspergillus PCR) and fungal
culture
• Serum GM
• Different aspergillosis case definition to determine incidence and
outcome of COVID-19 associated pulmonary aspergillosis
• AspICU & IAPA definitionsMAIN FINDINGS
• 108 patients included in the study è 189 BAL samples
• IAPA definition – probable aspergillosis in 30/108 (27.7%), after median
of 4 days (2-8) from intubation, 14 days (11-22) from COVID-19
symptom onset
• Compared to patients without aspergillosis, main risk factor = steroid
use
• AspICU definition – putative IPA in 19/108 (17.6%) patientsCOVID-19 & CO-INFECTIONS
Lansbury et al. J Infect. 2020 Aug;81(2):266COVID-19 & CO-INFECTIONS
• Widespread use of empiric antibiotics in patients with SARS-CoV-2
?justified its use
• Influenza associated bacterial infections è 30% of CAP cases; no co-
infections in patients with MERS-CoV; and only rarely in patients with
SARS-CoV-1.
• Altogether 30 studies included:
• 23 from China, 3 from USA, 2 from Spain, 1 from Thailand and 1 from
Singapore
• 29 observational study; 1 RCT
• 3834 patients
• 27 studies on data for hospitalised patients (6 included patients in ICU); 2
studies on deceased patients; 1 on non-hospitalised patients
• Mainly adult studies; median age 69
• 17 studies reported antibiotic use; >90% of patients received empiric
antibiotics in 10 studiesBACTERIAL CO-INFECTIONS
• Lab-confirmed bacterial co-infections:
• 7% (95% CI 3-12) for hospitalised patients, N = 2183 patients from 18
studies
• 14% (95%CI 5-26) for subgroup analysis of ICU patients, N=204 patients
• 17 studies specified co-infecting pathogensBACTERIAL CO-INFECTIONS
• Limitations:
• Only 1 study defined secondary bacterial co-infections
• Mycoplasma pneumoniae were serologically diagnosed (PCR
negative)
• Those with gram negative organisms - ?result of ICU-HAP rather than
specific for COVID-19
• Compared to influenza infections, bacterial co-infections seemed less
prevalent in COVID-19 patients
• 2009 influenza pandemic: 1 in 4 severe or fatal cases of influenza
A(H1N1) pdm09 had a bacterial infection, with an apparent association
with morbidity and mortality
• Streptococcus pneumoniae, Staphylococcus aureus, and
Streptococcus pyogenes most commonVIRAL CO-INFECTIONS
• Estimated that 3% of patients had viral co-infections (95% CI 1-6%; N=1014 patients, 16
studies)
• No significant difference if patients were admitted to ICU
• One study included outpatients/ presentation to ED only – 23/115 patients had viral co-
infections (20%) è depends on the season?OTHER RESULTS
• Fungal co-infections – in 3 studies (search ended 17 April 2020)
• Pooled analysis – those with co-infections had higher odds of death
(pooled OR 5.82, 95% CI 3.4 – 9.9, N = 733, 4 studies)
• However unclear if it’s due to viral/ bacterial/ fungal co-infections
• Limitations:
• Search ended 17 April 2020
• Most studies were from China during winter months
• Resource constraint in many countries + most COVID-19 patients were
outpatients è under-estimation of co-infections
• Significant heterogeneity amongst studies
• A lot of studies were not clear in their definitions• Main aim: to identify common bacterial/ fungal co-infections
• Secondary analysis: antimicrobial prescribing
• Review of 9 studies: rates of bacterial/ fungal co-infections 8% (62/806 patients)
• Mainly respiratory infections (VAP) and bacteremia (line associated)
• Low rates of co-infections, but high rates of antimicrobial prescribing
• 1450/2010 (72%) patients received antibiotics
• Mostly broad spectrum: quinolones, cephalosporins and carbapenems
Rawson et al. Clinical Infectious Diseases. 2020.REFERENCES
• Lansbury L, Lim B, Baskaran V, Lim WS. Co-infections in people with COVID-19: a systematic review and meta-analysis.
J Infect. 2020 Aug;81(2):266-275.
• Schauwvlieghe AFAD, Rijnders BJA, Philips N, et al. Invasive aspergillosis in patients admitted to the intensive care unit
with severe influenza: a retrospective cohort study. Lancet Respir Med. 2018; 6(10): 782-792.
• van de Veerdonk FL, Kolwijck E, Lestrade PP, Hodiamont CJ, Rijnders BJ, van Paassen J, et al. Influenza-Associated
Aspergillosis in Critically Ill Patients. Am J Respir Crit Care Med. 2017; 196(4): 524-7.
• Verweij PE, Gangneux JP, Bassetti M, Brüggemann RJM, Cornely OA, Koehler P, Lass-Flörl C, van de Veerdonk FL,
Chakrabarti A, Hoenigl M; European Confederation of Medical Mycology; International Society for Human and Animal
Mycology; European Society for Clinical Microbiology and Infectious Diseases Fungal Infection Study Group; ESCMID
Study Group for Infections in Critically Ill Patients. Diagnosing COVID-19-associated pulmonary aspergillosis. Lancet
Microbe. 2020 Jun;1(2):e53-e55.
• Bartoletti M, Pascale R, Cricca M, Rinaldi M, Maccaro A, Bussini L, et al. Epidemiology of invasive pulmonary
aspergillosis among COVID-19 intubated patients: a prospective study. Clin Infect Dis. 2020.
• Koehler P, Cornely OA, Bottiger BW, Dusse F, Eichenauer DA, Fuchs F, et al. COVID-19 associated pulmonary
aspergillosis. Mycoses. 2020; 63(6): 528-34.
• van Arkel ALE, Rijpstra TA, Belderbos HNA, van Wijngaarden P, Verweij PE, Bentvelsen RG. COVID-19-associated
Pulmonary Aspergillosis. Am J Respir Crit Care Med. 2020; 202(1): 132-135.
• Alanio A, Delliere S, Fodil S, Bretagne S, Megarbane B. Prevalence of putative invasive pulmonary aspergillosis in
critically ill patients with COVID-19. Lancet Respir Med. 2020;8(6): e48-e9.
• White PL, Dhillon R, Cordey A, Hughes H, Faggian F, Soni S, et al. A national strategy to diagnose COVID-19 associated
invasive fungal disease in the ICU. Clinical Infectious Diseases. 2020.
• Blot SI, Taccone FS, Van den Abeele AM, Bulpa P, Meersseman W, Brusselaers N, et al. A clinical algorithm to diagnose
invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med. 2012;186(1):56-64.
• Verweij PE, Rijnders BJA, Bruggemann RJM, Azoulay E, Bassetti M, Blot S, et al. Review of influenza-associated
pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med. 2020;
46(8): 1524-35.
• Rawson TM, Moore LSP, Zhu N, Ranganathan N, Skolimowska K, Gilchrist M, et al. Bacterial and Fungal Coinfection in
Individuals With Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clinical Infectious
Diseases. 2020.THANK YOU!
You can also read

















































